1. Introduction
Urinary tract infections (UTIs) are a common public health issue in both community and nosocomial settings, affecting ~150 million people worldwide each year [
1]. UTIs are caused by a wide range of pathogens, both Gram-negative and Gram-positive bacteria, as well as by certain fungi, but usually by uropathogenic
Escherichia coli [
2,
3]. UTI is among one of the most common bacterial infections, occurring particularly in women [
4].
The development of the antimicrobial agents, which started with the discovery of penicillin by Sir Alexander Fleming in 1928, is a cardinal step in the history of medicine, allowing to prevent millions of deaths due to infectious diseases [
5]. Unfortunately, shortly after their discovery, antibiotic resistance emerged, nowadays representing a significant burden to global public health [
6].
Integrative approach of UTI has an important role in improving prognosis, implying that in most cases antimicrobial therapy has to be prescribed empirically. In order to provide suitable empirical therapy, it is essential to know the main bacteria typically involved in the urinary tract infection, as well as their antimicrobial resistance pattern. This approach allows limiting antimicrobial resistance and the spread of multidrug-resistant bacterial strains [
7].
Numerous international experts came together through a joint initiative by the European Centre for Disease Prevention and Control (ECDC) and the United States Centers for Disease Control and Prevention (CDC), to create a standardized international definition for the description of acquired resistance profiles, as follows:
MDR (Multidrug Resistance) is defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories;
XDR (Extensive Drug Resistance) as non-susceptibility to at least one agent in all but two or fewer antimicrobial categories (i.e., bacterial isolates remain susceptible to only one or two categories);
PDR (Pandrug-resistance)—non-susceptibility to all agents in all antimicrobial categories [
8].
Furthermore, McDonnell et al. [
9] added to this list by proposing the notion of UDR: Usual Drug Resistance, to describe isolates that are not fully susceptible wild-type strains but that can nonetheless be readily treated with standard therapies.
More recently, Kadri et al. [
10] proposed the expression of DTR: Difficult to Treat Resistance. Their point of departure is the idea that the MDR-XDR-PDR definitions make no distinction between strengths and weaknesses of the individual antibiotics: agents with higher efficacy and lower toxicity are considered in the same way as agents with lower efficacy and higher toxicity. Therefore, they define DTR as intermediate or resistant to all of the typical first-line, lower toxicity agents, defined as the beta-lactams (including carbapenems and combinations with beta-lactamase inhibitors) and the fluoroquinolones. To determine the DTR status, the susceptibility testing of at least one carbapenem, one extended-spectrum cephalosporin, and one fluoroquinolone is required.
The latest CDC report provided definitions for two other antimicrobial resistance patterns [
11]:
ESC (Extended-spectrum cephalosporin-resistant)—Any E. coli, Klebsiella oxytoca or Klebsiella pneumoniae that has tested Intermediate (I) or Resistant (R) to at least 1 of the following: cefepime, ceftriaxone, cefotaxime, ceftazidime, ceftolozane/tazobactam or ceftazidime/avibactam;
CRE (Carbapenem-resistant Enterobacterales)—Any E. coli, Klebsiella aerogenes, Klebsiella oxytoca, Klebsiella pneumoniae, or Enterobacter spp. that has tested Resistant (R) to at least 1 of the following: imipenem, meropenem, doripenem, ertapenem, meropenem/vaborbactam, or imipenem/relebactam.
The impact of multidrug-resistant Gram-negative bacteria (MDR-GNB) infections can be determined by assessing the clinical outcomes, such as length of stay in the hospital or mortality rates. Although most of the studies found significant correlations between MDR-GNB and mortality risk, other authors failed to demonstrate such an association, therefore the topic remains controversial a fertile ground for further research [
12,
13,
14,
15].
This research is a sequel of our previous observations, which focused on the characterization of UTIs caused by K. pneumoniae, motivated by the necessity of determining the resistance patterns for all Enterobacterales against common antibiotic classes in treating UTIs.
Therefore, the aim of this study was to assess the antibiotic susceptibility rates and epidemiology of UTIs caused by Enterobacterales. Moreover, by using the novel resistance patterns, we aim to introduce them in the clinical practice, as a useful and more accurate tool for the characterization of antibiotic resistance in UTIs, especially for the clinicians.
2. Materials and Methods
A retrospective cohort study was conducted from 30 June 2019, to 30 December 2019, at “St. Parascheva” Clinical Hospital of Infectious Diseases from Iasi, a 300 beds university setting, as it is the largest tertiary center for Infectious Diseases from North-Eastern Romania, a region with approximately 4 million inhabitants.
2.1. Study Population
In this study, we enrolled all hospitalized patients presenting a confirmed UTI, both community-acquired and hospital-acquired (i.e., >48 h after admission), with the following inclusion criteria: (i) suggestive clinical syndrome (dysuria, pollakiuria or non-specific symptoms for catheterized patients, such as fever or chills); (ii) pyuria [≥10 white blood cell count (WBC)/mm3]; (iii) isolation of GNB Enterobacterales, including E. coli, K. pneumoniae, and Enterobacter spp., Proteus spp., Serratia spp., Providencia spp. or Morganella spp. in urine culture [≥105 colony forming units (CFU)/mL)]. We included only one isolate per patient (except for the isolates with different antibiotic susceptibility, which were considered as different isolates) and excluded those with GNB Enterobacterales colonization or with a urinary CFU count <105/mL.
A total of 354 clinical specimens were analyzed during the study period. Bacterial identification was automated, using phenotypical characters. Based on the antibiotic resistance pattern, we classified the isolates as susceptible to all tested antibiotics (S), MDR, XDR, and PDR. We also further divided the strains according to the novel resistance pattern such as UDR, DTR, CRE, or ESC.
2.2. Data Collection
Patient information was collected from the medical records, including age, gender, type of bacteria (E. coli, K. pneumoniae, Enterobacter spp. Proteus spp., Serratia spp., Providencia spp., or Morganella spp.), resistance pattern for each isolate, previous hospitalizations (within the past 3 months) or use of antibiotics within the past 30 days, urinary catheterization, presence of comorbid conditions (such as kidney disease, or diabetes mellitus), treatment regimen, and clinical outcome.
2.3. Microbiological Procedures
Antimicrobial susceptibility testing was performed by the Kirby Bauer disk diffusion method, using the following antimicrobial discs: ampicillin, amoxicillin/clavulanic acid, piperacillin/tazobactam, cefixime, cefuroxime, ceftazidime, ceftriaxone, cefotaxime, cefoxitine, cefepime, imipenem, meropenem, ertapenem, amikacin, gentamicin, tobramycin, ciprofloxacin, norfloxacin, moxifloxacin, ofloxacin, trimethoprim/sulfamethoxazole, and nitrofurantoin. We used EUCAST clinical breakpoint table v9.0 for the interpretation of the minimal inhibitory concentrations (MIC) and zone diameters.
2.4. Carbapenemase Detection
For isolates resistant to carbapenems, NG-Test Carba 5 multiplex lateral flow immunoassay was used for the phenotypic detection and differentiation of five common carbapenemase families: Klebsiella pneumoniae carbapenemase (KPC), oxacillinase (OXA-48-like), Verona integron encoded metallo-β-lactamase (VIM), imipenemase (IMP), and New Delhi metallo-β-lactamase (NDM). The test was performed according to the manufacturer’s instructions.
2.5. Statistical Analysis
We used Kolmogorov–Smirnov test to assess the normal distribution of parameters in the study population, normally distributed variables being presented as means ± standard deviation. Categorical variables are presented as absolute numbers or percentages. The differences between various subgroups were assessed using independent t-test or one-way ANOVA, as appropriate. For certain significant differences objectified within subgroups following the ANOVA analysis, we performed a post hoc Dunnett’s test. The correlation analysis between two or more variables was performed using either Pearson’s (for continuous variables) or Spearman’s (for categorical variables) rank (r) coefficients.
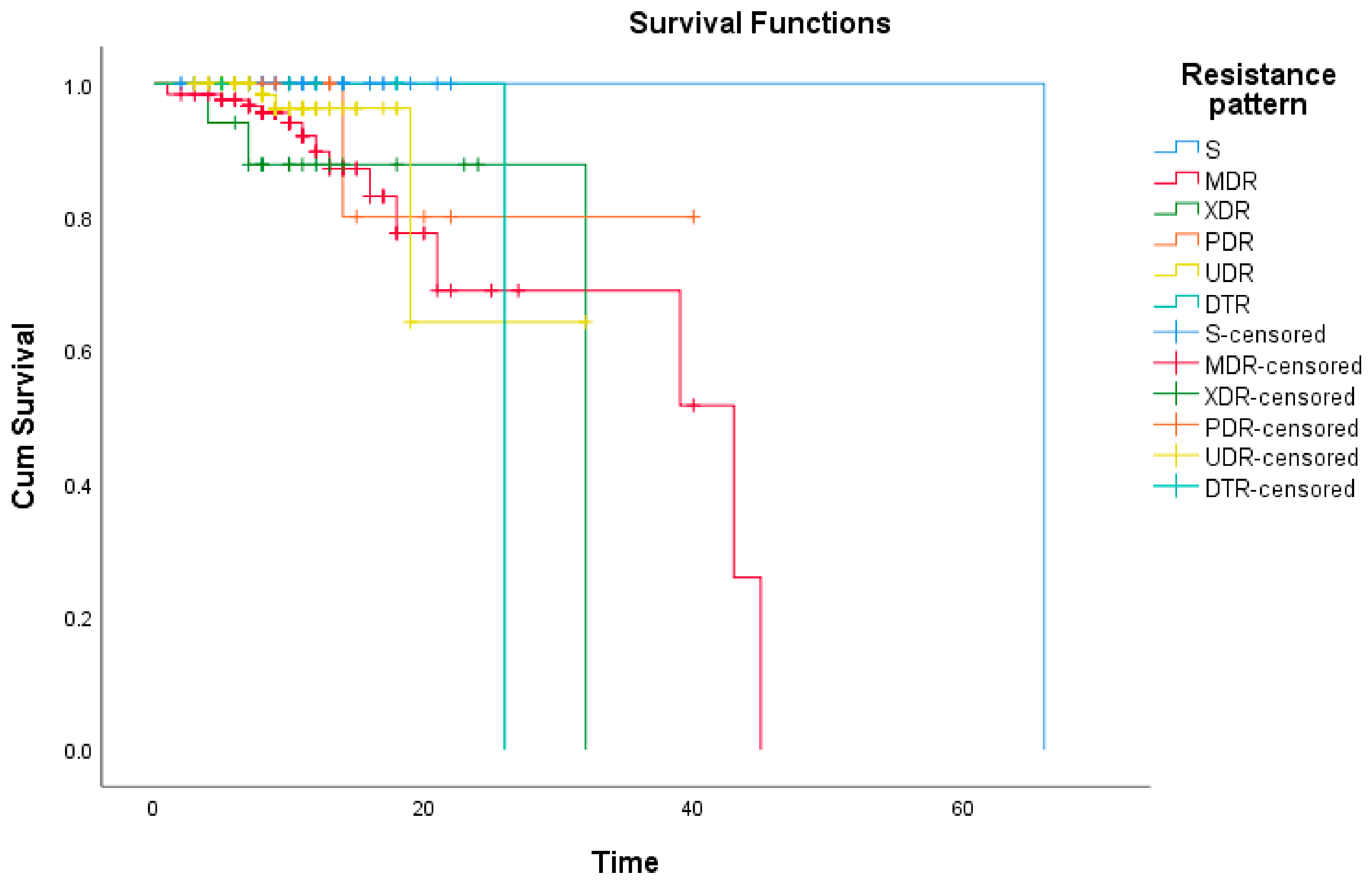
To compare the survival distribution within the resistance pattern subgroups we used the log-rank test, while Kaplan–Meier method was used for the estimation of the survival curves.
A multivariate logistic regression was also performed to identify a specific model comprising multiple risk factors as predictors associated with multidrug resistance (dependent variable), with Hosmer–Lemeshow goodness-of-fit test indicating that the model adequately describes the analyzed data.
A p-value of 0.05 was considered statistically significant. For the initial data collection, we used Microsoft Excel 2013 version (Microsoft Corporation, Redmond, WA, USA), while the data analysis was performed with SPSS version 23 (IBM, Armonk, VA, USA).
4. Discussions
This study focused on the widespread prevalence of various drug-resistance patterns among Enterobacterales UTIs in North-Eastern Romania and their impact on the patients’ outcome. This is one of the first studies that specifically addressed DTR as a novel resistance pattern in UTIs, the other currently available data referring mainly to bloodstream infections.
As expected, the most commonly identified uropathogen was
E. coli, responsible for almost two-thirds of the recorded cases of UTI. This finding is in accordance with multiple recent studies [
16,
17,
18,
19], which found it to be the main etiological agent in up to 95% of the UTIs. The second most isolated bacteria were
Klebsiella spp., encountered in 76 cases (21.4%), of which
K. pneumoniae was by far the most common species, an aspect in accordance with the results reported by several recent studies [
4,
17,
18,
20], even though a recent study conducted in another region of Romania reported
K. pneumoniae as the leading etiology in some settings [
21].
Regarding the antibiotic resistance pattern, we identified that 43.5% of isolates were resistant to multiple antibiotic classes. Of those, the majority was MDR (35.5%), followed by XDR (4.8%) and PDR (3.1%). The identification of PDR strains represents a major concern; multiple studies that analyzed the resistance profile of Gram-negative pathogens have failed to identify such a pattern [
13,
22], while others have reported negligible amounts [
23,
24].
Another goal of the study was to turn the spotlight on the novel resistance classification, aiming to outline a local epidemiological profile, since Romania constantly top ranks in terms of antibiotic resistance [
25]. The DTR pattern can be described as a subcategory within MDR/XDR/PDR strains, being resistant to all first-line agents: entire range of β-lactams (including carbapenems), various combinations with β-lactamase inhibitors, as well as to fluoroquinolones. A plethora of studies has tried so far to assess the prognostic utility of this novel resistance pattern, but were focusing mainly on blood stream infections. Benkő et al. analyzed the prevalence of DTR strains among the ESKAPE pathogens and found only 23 isolates (0.46%), mostly
Acinetobacter baumannii and
Pseudomonas aeruginosa, with only one
Klebsiella spp. and one
Proteus spp. [
26]. Similarly, Gianella et al. conducted a research in the region of Emilia-Romagna, Italy, and identified higher numbers of DTR patterns, representing 11% of all isolates, with
K. pneumoniae accounting for all but one strains [
23], while reports from France [
27], Hungary [
28] or United States [
10] highlighted a much lower prevalence of DTR, constantly reported as maximum 1%. Interestingly, there is a wide spectrum of DTR variance among bacterial species, the highest shares of DTR being found among UTIs caused by
A. baumannii [
10]. In our study, we found that out of the 25 DTR strains (7% of all cases, of which two were MDR, 12 were XDR, and 11 were PDR), most of the isolates were
K. pneumoniae, followed by
Enterobacter spp.,
Providencia spp.,
Proteus spp. and
Serratia spp.
The already established risk factors for the acquisition of an UTI caused by a drug-resistant pathogen, as reported in numerous studies conducted worldwide [
29,
30,
31] are age, male gender, previous hospitalizations, previous antibiotic use, and urinary catheterization, all of them being also significantly higher among patients with resistant isolates from our study, especially in the PDR and DTR groups. Furthermore, Faine et al. identified some other risk factors, such as chronic hemodialysis and nursing home residence [
32], while Ben Ayed et al. found a correlation between the presence of diabetes mellitus or a history of urinary tract surgery in the last 12 months, with the acquisition of a MDR community-acquired UTI [
33].
Moreover, Tenney et al. [
34] performed a systematic review including more than 30.000 patients, aiming to stratify the risk factors for MDR UTIs, according to their prevalence; in this regard, they classified the risk factors as probable (urinary catheterization, previous hospitalization, or antibiotic intake and nursing home residence), possible (age, history of UTI and male gender) and unlikely/supplementary research needed (diabetes mellitus, recent travel, ethnicity, immunosuppression, and female gender). This classification is consistent with our findings; all the noteworthy risk factors we identified fit in the “probable” and “possible” categories, while those categorized as “unlikely” did not reach the statistical significance; worth mentioning, female gender was a protective factor, being strongly associated with S isolates and, consequently, with a favorable outcome.
When assessing individual antibiotic susceptibility, we identified a great rate of isolates resistant to all aminopenicillins (+/−IBL) and fluoroquinolones, given the fact that these antibiotics usually represent the empiric treatment for UTIs in the north east region of Romania. We also identified a high resistance rate to aminoglycosides, particularly to gentamicin and tobramycin, while amikacin remains active for most isolates of E. coli and Proteus spp. Carbapenems continue to be a viable option for most Gram-negative UTIs, even though we identified a total of 25 strains, mostly K. pneumoniae, resistant to carbapenems (of which 19 were carbapenemase-producers).
Our results are more dramatic than those reported in most of the studies [
35,
36,
37,
38], even though we have found some others with higher resistance rates [
19,
24,
39]. For example, Kot et al. identified all
E. coli and
P. mirabilis isolates as susceptible to carbapenems (vs. 99.1% and 91.1%, respectively, in our study), and an 84.4% susceptibility for
K. pneumoniae isolates (vs. 68.4% sensitivity to ertapenem in ours) [
17]. Even though
Proteus spp. is usually associated with hospital-acquired UTIs [
21], with higher resistance rates to carbapenems [
40,
41], we identified up to 97% susceptibility to meropenem, similar to other Romanian research [
16]; however, we must interpret these results with caution, due to the relatively small number of
Proteus spp. isolates. Interestingly, a recent study that included isolates from other regions of Romania, reported a significantly lower resistance rates for both
E. coli and
K. pneumoniae UTIs in females, with 85.3% of
E. coli and 73.9% of
K. pneumoniae isolates being susceptible to amoxicillin-clavulanic acid (vs. 65% and 32.8%, respectively, in our study), 91.2% and 81.8% presenting sensitivity to ceftazidime (vs. 80.7% and 48.6% in ours), 96% and 88.4% to amikacin (vs. 71.1% and 44.7%) and 98.16% and 93.9% sensitivity to Imipenem (vs. 100% and 82.8%) [
42]. However, Sokhn et al., while investigating the resistance pattern of Gram-negative uropathogens in Lebanon, found similar or even lower sensitivity to some of the antibiotics tested; they reported only 42.4% and 35.8% sensitivity to amoxicillin-clavulanic acid for
E. coli and
K. pneumoniae, respectively, 69.4% and 65.7% to ciprofloxacin (vs. 71.1% and 44.7% in our study), 77.6% and 77.8% to amikacin, while 100% of their isolates were susceptible to all tested carbapenems (imipenem and meropenem) [
19].
Those regional differences in terms of antibiotic resistance can be based also on the socioeconomic status of the countries where the studies were conducted. Although the resistance mechanisms are triggered by certain microbiological and molecular particularities, those phenomena may be enhanced by specific socioeconomic and behavioral factors. There is a growing body of evidence that antibiotic resistance is positively correlated with a poor economic status, with higher rates of resistance found in less developed countries [
43,
44,
45]. Some socio-governmental determinants that may induce the selection of resistant strain are the limited acknowledge of the standardized protocols concerning the antibiotic prescription by the medical staff, the non-judicious use of broad-spectrum antibiotics in several medical departments, or even the abusive prescriptions by general practitioner irrespective of the involved germ or local epidemiology recommendations. Of course, at individual level, a poor educational status can be the source for frequent, empirical antibiotic self-administration or, conversely, for incomplete adherence to a prescribed antibiotic regimen, resulting in an increased antibiotic resistance [
46], as confirmed by the results of our study. Last but not least, an impaired socioeconomic status can be the trigger for various comorbidities that can alter the natural immunity against infections or can even be associated with some precarious housing issues vastly incriminated in the apparition of UTIs (e.g., lack of running water or indoor sanitation facilities) [
47]. The region of Romania where this study was conducted can be considered a borderline region, exhibiting characteristics from both the developed and the developing countries, therefore the reported resistance profiles from this area could emerge as relevant epidemiological benchmarks.
The prognosis of patients with UTIs may be significantly influenced by the resistance pattern. Therefore, we noted that the overall in-hospital mortality in our study was 6.7%, ranging from 1% in the S group to 24% in CRE and DTR groups. Risk factors strongly associated with a negative outcome were urinary catheterization, previous recent antibiotic treatment or hospitalizations within the past 3 months, respiratory comorbidities, obesity, longer hospital stay, and inappropriate empirical therapy. Clearly, multiple associated pathologies, as well as older age, all summed in the CCI, have a negative impact on the survival rate. A CCI value ≥3 was positively correlated with a higher mortality risk in our study, a similar cut-off value being reported also by Hoxha et al. [
48], while Hussein et al. [
49] claimed that a value ≥5 is more appropriate in the mortality risk assessment in patients with carbapenem-resistant
K. pneumoniae infections. We also observed that a high inflammatory state was correlated with increased risk of death. Even if this biomarker is not specific for UTIs, the baseline and dynamics of CRP’s serum levels represent an adequate tool for risk stratification and prognosis assessment of every admitted patient, regardless the etiology of infection or the resistance pattern [
50].


 ,
, 




{kind=link}
{kind=link}