A Clinical Perspective on the Antimicrobial Resistance Spectrum of Uropathogens in a Romanian Male Population

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
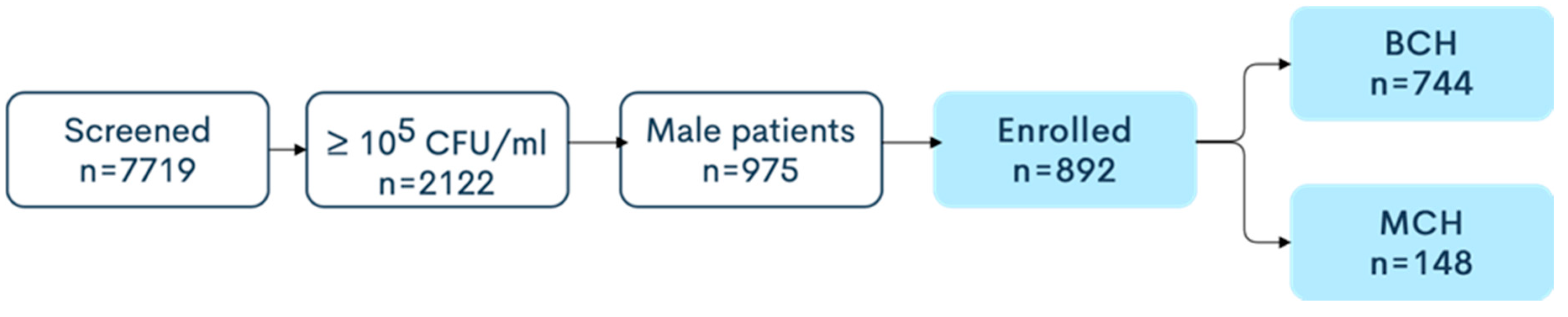
2.1. Study Design and Sample Population
- Positive uroculture ≥ 105 CFU/mL;
- Single bacteria strain on uroculture;
- Age ≥ 18 years;
- Male patients.
- Uroculture < 105 CFU/mL;
- Presence of a urological catheter;
- Multiple bacteria strains on uroculture.
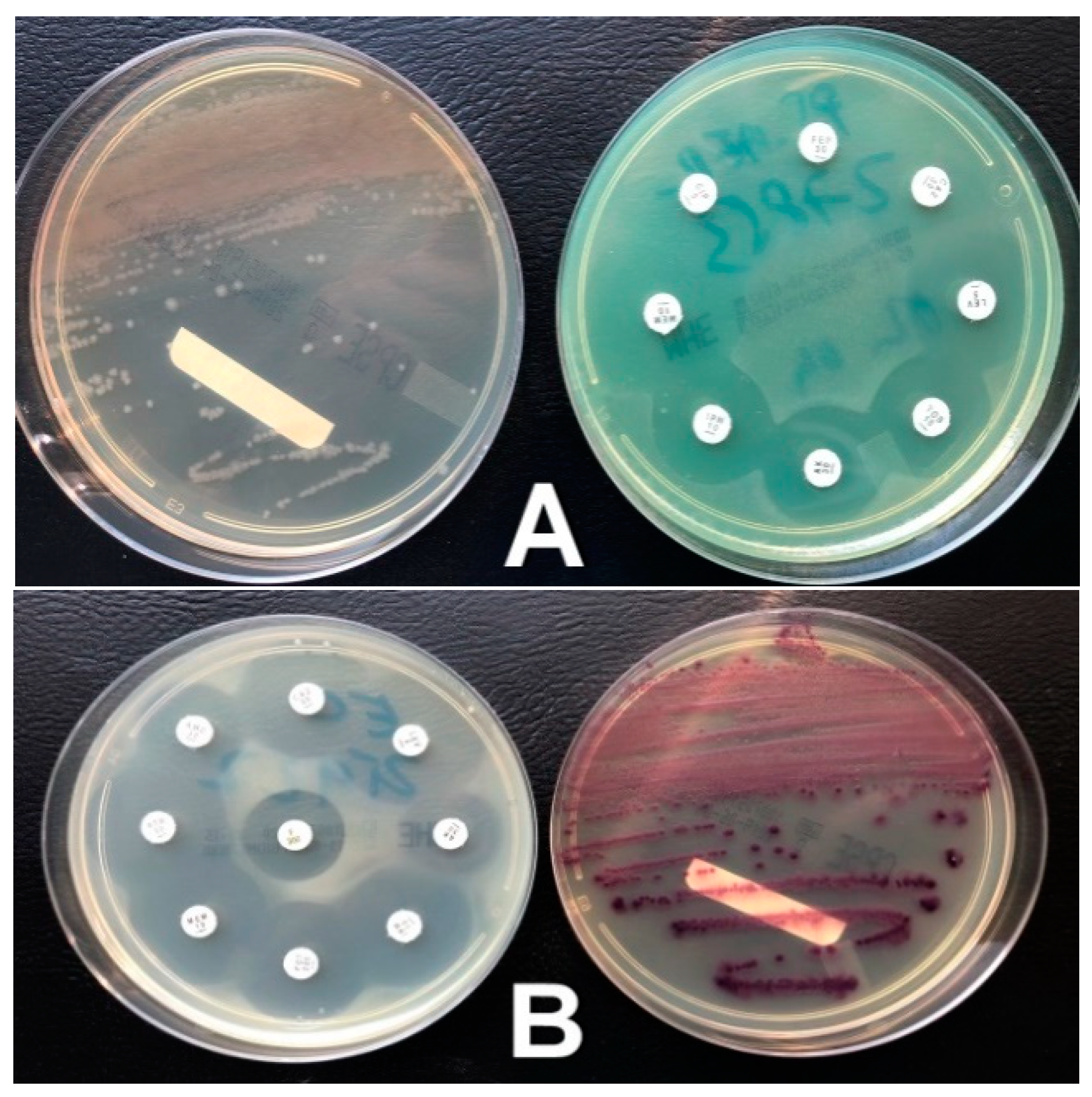
2.2. Sample Collection and Processing
2.3. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nicolle, L.E. Epidemiology of urinary tract infection. Infect. Med. 2001, 18, 153–162. [Google Scholar] [CrossRef]
- Asadi, S.; Kargar, M.; Solhjoo, K.; Najafi, A.; Ghorbani-Dalini, S. The association of virulence determinants of uropathogenic Escherichia coli with antibiotic resistance. Jundishapur J. Microbiol. 2014, 7, e9936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenlehner, F.M.; Naber, K.G.; Weidner, W. Rational antibiotic therapy of urinary tract infections. Med. Monatsschr. Pharm. 2008, 31, 385–390. [Google Scholar] [PubMed]
- Omoregie, R.; Erebor, J.O.; Ahonkhai, I.; Isibor, J.O.; Ogefere, H.O. Observed changes in the prevalence of uropathogens in Benin City, Nigeria. N. Z. J. Med. Lab. Sci. 2008, 62, 29–33. [Google Scholar]
- Gruneberg, R.N. Antibiotic sensitivities of urinary pathogens 1971–1978. J. Clin. Pathol. 1980, 33, 853–856. [Google Scholar] [CrossRef] [Green Version]
- Millan, Y.; Hernandez, E.; Millan, B.; Araque, M. Distribution of phylogenetic groups and virulence factors in CTX-M-15 beta-lactamase-producing uropathogenic Escherichia coli strains isolated from patients in the community of Merida, Venezuela. Rev. Argent. Microbiol. 2014, 46, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am. J. Med. 2002, 113 (Suppl. 1A), 5–13. [Google Scholar] [CrossRef]
- Nicolle, L.E. Urinary tract infections in the elderly. Clin. Geriatr. Med. 2009, 25, 423–436. [Google Scholar] [CrossRef]
- Petca, R.C.; Salaheddin, Y.; Petca, A.; Popescu, R.I.; Mehedintu, C.; Maru, N.; Jinga, V. Could chemical composition of stone influence percutaneous nephrolithotomy in the management of staghorn calculi? Rev. Chim. 2019, 70, 3872–3877. [Google Scholar] [CrossRef]
- Griebling, T.L. Urologic diseases in america project: Trends in resource use for urinary tract infections in men. J. Urol. 2005, 173, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Caljouw, M.A.; den Elzen, W.P.; Cools, H.J.; Gussekloo, J. Predictive factors of urinary tract infections among the oldest old in the general population: A population-based prospective follow-up study. BMC Med. 2011, 9, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saffar, M.J.; Enayti, A.A.; Abdolla, I.A.; Razai, M.S.; Saffar, H. Antibacterial susceptibility of uropathogens in 3 hospitals, Sari, Iran, 2002–2003. East. Mediterr. Health J. 2008, 14, 556–563. [Google Scholar] [PubMed]
- Gales, C.A.; Jones, R.N.; Gordon, K.A.; Sader, S.H.; Wilke, W.W.; Beach, M.L.; Pfaller, M.A.; Doern, G.V.; the SENTRY Study Group Latin America. Activity and spectrum of 22 antimicrobial agents tested against urinary tract infections pathogens in hospitalized patients in Latin America: Report from the second year of the SENTRY Antimicrobial Surveillance Programme (1998). J. Antimicrob. Chemother. 2000, 45, 295–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blix, H.S.; Røed, J.; Sti, M.O. Large variation in antibacterial use among Norwegian nursing homes. Scand. J. Infect. Dis. 2007, 39, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Warren, J.W.; Abrutyn, E.; Hebel, J.R.; Johnson, J.R.; Schaeffer, A.J.; Stamm, W.E. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America (IDSA). Clin. Infect. Dis. 1999, 29, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R. Antibiotic treatment and susceptibility testing. J. Clin. Pathol. 2005, 58, 786–787. [Google Scholar] [CrossRef] [Green Version]
- Petca, R.C.; Popescu, R.I.; Mares, C.; Petca, A.; Mehedintu, C.; Sandu, I.; Măru, N. Antibiotic resistance profile of common uropathogens implicated in urinary tract infections in Romania. Farmacia 2019, 67, 994–1004. [Google Scholar] [CrossRef]
- Johnson, J.R.; Johnston, B.; Kuskowski, M.A.; Colodner, R.; Raz, R. Spontaneous conversion to quinolone and fluoroquinolone resistance among wild-type Escherichia coli isolates in relation to phylogenetic background and virulence genotype. Antimicrob. Agents Chemother. 2005, 49, 4739–4744. [Google Scholar] [CrossRef] [Green Version]
- Kamenski, G.; Wagner, G.; Zehetmayer, S.; Fink, W.; Spiegel, W.; Hoffmann, K. Antibacterial resistances in uncomplicated urinary tract infections in women: ECO.SENS II data from primary health care in Austria. BMC Infect. Dis. 2012, 12, 222. [Google Scholar] [CrossRef] [Green Version]
- Cullen, I.M.; Manecksha, R.P.; McCullagh, E.; Ahmad, S.; O’Kelly, F.; Flynn, R.J.; Murphy, P.; Fennell, J.; McDermott, T.; Grainger, R.; et al. The changing pattern of antimicrobial resistance within 42,033 Escherichia coli isolates from nosocomial, community and urology patient-specific urinary tract infections, Dublin, 1999–2009. BJU Int. 2012, 109, 1198–1206. [Google Scholar] [CrossRef] [Green Version]
- Lautenbach, E.; Patel, J.B.; Bilker, W.B.; Edelstein, P.H.; Fishman, N.O. Extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: Risk factors for infection and impact of resistance on outcomes. Clin. Infect. Dis. 2001, 32, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Petca, R.C.; Mares, C.; Popescu, R.; Petca, A.; Diaconescu, D.; Braticevici, B.; Jinga, V. Antibiotic resistance profile of uropathogens strains implicated in the etiology of the urinarytract infections. Eur. Urol. Suppl. 2019, 18, e2397. [Google Scholar] [CrossRef]
- Abubakar, E.M. Antimicrobial susceptibility pattern of pathogenic bacteria causing urinary tract infections at the Specialist Hospital, Yola, Adamawa State, Nigeria. J. Clin. Med. Res. 2009, 1, 1–8. [Google Scholar]
- Oluremi, B.B.; Idowu, A.O.; Olaniyi, J.F. Antibiotic susceptibility of common bacterial pathogens in urinary tract infections in a Teaching hospital in Southwestern Nigeria. Afr. J. Microbiol. Res. 2011, 5, 3658–3663. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/antimicrobial-resistance (accessed on 4 May 2020).
- Aluculesei, B.C. Antibiotic resistance in Romania: An economic and medical challenge. Jr. Sci. Res. 2017, 3, 1–8. [Google Scholar]
- Benea, E.O.; Gavriliu, L.C.; Popescu, C.; Popescu, G.A. Ghidul Angelescu. Terapie Antimicrobiana 2018, 3rd ed.; Editura Bucuresti: Bucharest, Romania, 2018; pp. 181–192. [Google Scholar]
- Bonkat, G.; Pickard, R.; Bartoletti, R.; Cai, T.; Bruyere, F.; Geerlings, S.E.; Köves, B.; Wagenlehner, F. EAU Guidelines on Urological Infections; European Association of Urology: Arnhem, The Netherlands, 2018. [Google Scholar]
- World Health Organization. Guidelines for the Collection of Clinical Specimens during Field Investigation of Outbreaks; World Health Organization: Geneva, Switzerland, 2000; pp. 1–51. [Google Scholar]
- Pincus, D.H. Microbial Identification Using the Biomérieux Vitek® 2 System. Available online: https://store.pda.org/tableofcontents/ermm_v2_ch01.pdf (accessed on 12 March 2020).
- Lee, P.S. Quantification of microorganisms. In Practical Handbook of Microbiology, 2nd ed.; Goldman, E., Green, L.H., Eds.; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2009; pp. 11–30. [Google Scholar]
- The Clinical & Laboratory Standards Institute (CLSI). Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 10 March 2020).
- Rowe, T.A.; Juthani-Mehta, M. Diagnosis and management of urinary tract infection in older adults. Infect. Dis. Clin. N. Am. 2014, 28, 75–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popescu, G.C.; Ion, A.R. On the economics of climate change and health: An overwiew. In The Impact of Climate Change on Our Life. The Questions of Sustainability; Omran, A., Schwarz-Herion, O., Eds.; Springer: Singapore, 2018; pp. 79–96. [Google Scholar]
- Schvoerer, E.; Massue, J.P.; Gut, J.P.; Stoll-Keller, F. Climate change: Impact on viral disease. Open Epidemiol. J. 2008, 1, 53–56. [Google Scholar] [CrossRef] [Green Version]
- Koeijers, J.J.; Verbon, A.; Kessels, A.G.H.; Bartelds, A.; Donkers, G.; Nys, S.; Stobberingh, E.E. Urinary tract infection in male general practice patients: Uropathogens and antibiotic susceptibility. Urology 2010, 76, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Rocha, J.L.; Tuon, F.F.; Johnson, J.R. Sex, drugs, bugs, and age: Rational selection of empirical therapy for outpatient urinary tract infection in an era of extensive antimicrobial resistance. Braz. J. Infect. Dis. 2012, 16, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Bonadio, M.; Meini, M.; Spetaleri, P.; Gilgi, C. Current microbiological and clinical aspects of urinary tract infections. Eur. Urol. 2001, 40, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Grude, N.; Tveten, Y.; Kristiansen, B.E. Urinary tract infections in Norway: Bacterial aetiology and susceptibility. A retrospective study of clinical isolates. Clin. Microbiol. Infect. 2001, 7, 543–547. [Google Scholar] [CrossRef]
- Leibovici, L.; Pitlik, S.D.; Konisberger, H.; Drucker, M. Bloodstream infections in patients older than eighty years. Age Ageing 1993, 22, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B.; Klemstine, K.L.; Brown, P.D. Acute pyelonephritis in US hospitals in 1997: Hospitalization and in-hospital mortality. Ann. Epidemiol. 2003, 13, 144–150. [Google Scholar] [CrossRef]
- Smithson, A.; Ramos, J.; Niño, E.; Culla, A.; Pertierra, U.; Friscia, M.; Bastida, M.T. Characteristics of febrile urinary tract infections in older male adults. BMC Geriatr. 2019, 19, 334. [Google Scholar] [CrossRef] [PubMed]
- Bitew, A.; Molalign, T.; Chanie, M. Species distribution and antibiotic susceptibility profile of bacterial uropathogens among patients complaining urinary tract infections. BMC Infect. Dis. 2017, 17, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.N.; Kugler, K.C.; Pfaller, M.A.; Winokur, P.L. Characteristics of pathogens causing urinary tract infections in hospitals in North America: Results from the SENTRY Antimicrobial Surveillance Program, 1997. Diagn. Microbiol. Infect. Dis. 1999, 35, 55–63. [Google Scholar] [CrossRef]
- Gardiner, B.J.; Stewardson, A.J.; Abbott, I.J.; Peleg, A.Y. Nitrofurantoin and fosfomycin for resistant urinary tract infections: Old drugs for emerging problems. Aust. Prescr. 2019, 42, 14–19. [Google Scholar] [CrossRef]
- Zhang, H.; Kong, H.; Yu, Y.; Wu, A.; Duan, Q.; Jiang, X.; Zhang, S.; Sun, Z.; Ni, Y.; Wang, W.; et al. Carbapenem susceptibilities of Gram-negative pathogens in intra-abdominal and urinary tract infections: Updated report of SMART 2015 in China. BMC Infect. Dis. 2018, 18, 493. [Google Scholar] [CrossRef]
- Winstanley, T.G.; Limb, D.I.; Eggington, R.; Hancock, F. A 10-year survey of the antimicrobial susceptibility of urinary isolates in the UK: The Microbe Base Project. J. Antimicrob. Chemother. 1997, 40, 591–594. [Google Scholar] [CrossRef] [Green Version]
- Caneiras, C.; Lito, L.; Melo-Cristino, J.; Duarte, A. Community- and hospital-acquired Klebsiella pneumonia urinary tract infections in Portugal: Virulence and antibiotic resistance. Microorganisms 2019, 7, 138. [Google Scholar] [CrossRef] [Green Version]
- Bonkat, G.; Pilatz, A.; Wagenlehner, F. Time to adapt our practice? The European Commission has restricted the use of Fluoroquinolones since March 2019. Eur. Urol. 2019, 76, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, F.E.; Mushtaq, A.; Irshad, M.; Rauf, H.; Afzal, N.; Rasheed, A. Current efficacy of antibiotics against Klebsiella isolates from urine samples - a multi-centric experience in Karachi. Pak. J. Pharm. Sci. 2013, 26, 11–15. [Google Scholar] [PubMed]
- Lin, W.P.; Wang, J.T.; Chang, S.C.; Chang, F.Y.; Fung, C.P.; Chuang, Y.C.; Chen, Y.S.; Shiau, Y.R.; Tan, M.C.; Wang, H.Y.; et al. The antimicrobial susceptibility of Klebsiella pneumoniae from community settings in Taiwan, a trend analysis. Sci. Rep. 2016, 6, 36280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haller, M.; Brandis, M.; Berner, R. Antibiotic resistance of urinary tract pathogens and rationale for empirical intravenous therapy. Pediatr. Nephrol. 2004, 19, 982–986. [Google Scholar] [CrossRef]
- Sharifi, Y.; Hasani, A.; Ghotaslou, R.; Naghili, B.; Aghazadeh, M.; Milani, M.; Bazmany, A. Virulence and antimicrobial resistance in enterococci isolated from urinary tract infections. Adv. Pharm. Bull. 2013, 3, 197–201. [Google Scholar] [CrossRef] [Green Version]
- Zanichelli, V.; Hutnner, A.; Harbarth, S.; Kronenberg, A.; Huttner, B.; The Swiss Centre for Antibiotic Resistance (ANRESIS). Antimicrobial resistance trends in Escherichia coli, Klebsiella pneumoniae and Proteus mirabilis urinary isolates from Switzerland: Retrospective analysis of data from a national surveillance network over an 8-year period (2009–2016). Swiss Med. Wkly. 2019, 149, w20110. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Trecarichi, E.M.; Fiori, B.; Losito, A.R.; D’Inzeo, T.; Campana, L.; Ruggeri, A.; Di Meco, E.; Liberto, E.; Fadda, G.; et al. Multidrug-resistant Proteus mirabilis bloodstream infections: Risk factors and outcomes. Antimicrob. Agents Chemother. 2012, 56, 3224–3231. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isolated Bacteria | BCH | MCH | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Gram Negative | 542 | 72.84 | 124 | 83.78 | 666 | 74.66 |
| E. coli | 248 | 33.33 | 73 | 49.32 | 321 | 35.98 |
| Klebsiella spp. | 177 | 23.79 | 28 | 18.91 | 205 | 22.98 |
| Pseudomonas aeruginosa | 51 | 6.85 | 14 | 9.45 | 65 | 7.28 |
| Proteus spp. | 66 | 8.87 | 9 | 6.08 | 75 | 8.40 |
| Gram Positive | 202 | 27.15 | 24 | 16.21 | 226 | 25.33 |
| Enterococcus spp. | 156 | 32.70 | 20 | 13.51 | 177 | 19.73 |
| Staphylococcus spp. | 46 | 6.18 | 4 | 2.70 | 50 | 5.60 |
| Isolated Bacteria | BCH | MCH | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <31 | 31–50 | 51–70 | >70 | <31 | 31–50 | 51–70 | >70 | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| E. coli | 1 | 0.13 | 18 | 2.41 | 123 | 16.53 | 106 | 14.24 | 6 | 4.05 | 8 | 5.4 | 29 | 19.59 | 30 | 20.27 |
| Klebsiella spp. | 0 | - | 11 | 1.47 | 67 | 9.00 | 99 | 13.30 | 3 | 2.02 | 4 | 2.7 | 13 | 8.78 | 8 | 5.40 |
| Pseudomonas aeruginosa | 1 | 0.13 | 12 | 1.61 | 81 | 10.88 | 63 | 8.46 | 2 | 1.35 | 4 | 2.7 | 8 | 5.4 | 6 | 4.05 |
| Proteus spp. | 1 | 0.13 | 2 | 0.26 | 20 | 2.68 | 43 | 5.77 | 2 | 1.35 | 1 | 0.67 | 2 | 1.35 | 4 | 2.7 |
| Enterococcus spp. | 0 | - | 5 | 0.67 | 19 | 2.55 | 26 | 3.49 | 2 | 2.35 | 1 | 0.67 | 5 | 3.37 | 6 | 4.05 |
| Staphylococcus spp. | 2 | 0.26 | 0 | - | 23 | 3.09 | 20 | 2.68 | 0 | - | 1 | 0.67 | 2 | 2.35 | 1 | 0.67 |
| Total | 5 | 0.67 | 48 | 6.45 | 333 | 44.75 | 357 | 47.98 | 15 | 10.13 | 19 | 12.83 | 59 | 39.86 | 55 | 37.16 |
| Antibiotics | Gram-Negative Organism Isolated | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Escherichia coli | Klebsiella spp. | Pseudomonas aeruginosa | Proteus spp. | |||||||||
| R·n/% | S·n/% | NA | R·n/% | S·n/% | NA | R·n/% | S·n/% | NA | R·n/% | S·n/% | NA | |
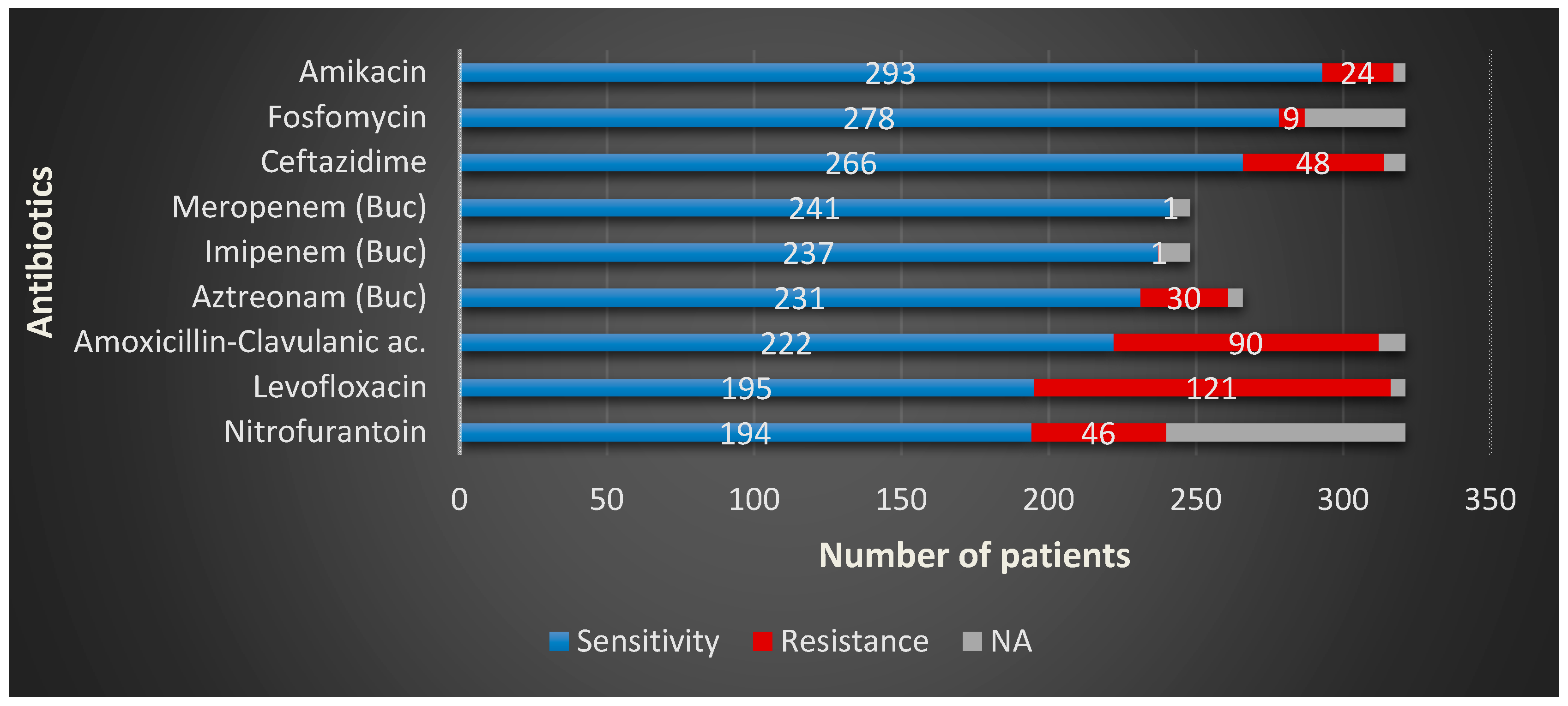
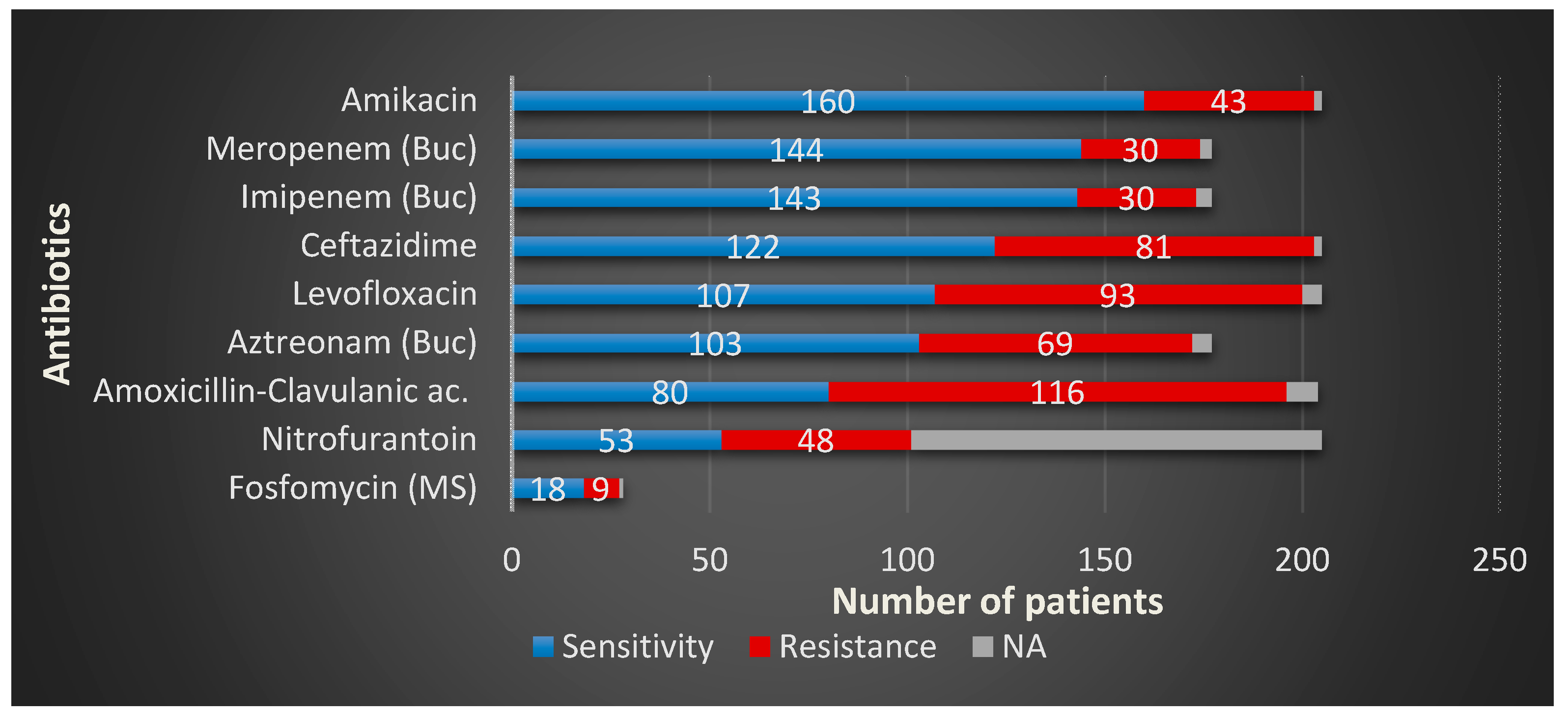
| Amikacin | 24/7.47 | 293/91.27 | - | 43/20.97 | 160/78.04 | - | 21/32.30 | 40/61.53 | - | 4/5.33 | 70/93.33 | |
| Amoxicillin-Clavulanic ac. | 90/28.03 | 222/69.15 | - | 116/65.58 | 80/39.02 | - | 4/28.57 | 5/35.71 | 51-BCH | 24/32.0 | 45/60.0 | |
| Aztreonam | 30/12.0 | 213/85.88 | 73- MCH | 69/38.98 | 103/58.19 | 28-MCH | 12/23.52 | 37/72.54 | 14-MCH | 5/7.57 | 59/89.39 | 9-MCH |
| Ceftazidime | 48/14.95 | 266/82.86 | - | 81/39.51 | 122/59.51 | - | 17/26.15 | 47/72.30 | - | 11/14.66 | 62/82.66 | |
| Fosfomycin | 9/2.80 | 278/86.60 | - | 9/32.14 | 18/64.28 | 177-BCH | 2/14.28 | 7/50 | 51/BCH | 6/66.66 | 2/22.22 | 66-BCH |
| Imipenem | 1/0.4 | 237/95.56 | 73-MCH | 30/1.69 | 143/80.79 | - | 13/25.49 | 38/74.5 | 14-MCH | 1/15.15 | 59/89.39 | 9-MCH |
| Levofloxacin | 121/37.69 | 195/60.74 | - | 93/45.36 | 107/52.19 | - | 29/44.61 | 35/53.84 | - | 18/24.00 | 53/70.66 | |
| Meropenem | 1/0.40 | 241/97.17 | 73-MCH | 30/1.69 | 144/81.35 | 28-MCH | 13/25.49 | 38/74.5 | 14-MCH | 0 | 62/93.93 | 9-MCH |
| Nitrofurantoin | 46/14.33 | 194/60.43 | - | 48/23.41 | 53/25.85 | - | 4/28.57 | 7/50 | 51-BCH | 3/33.33 | 4/44.44 | 66-BCH |
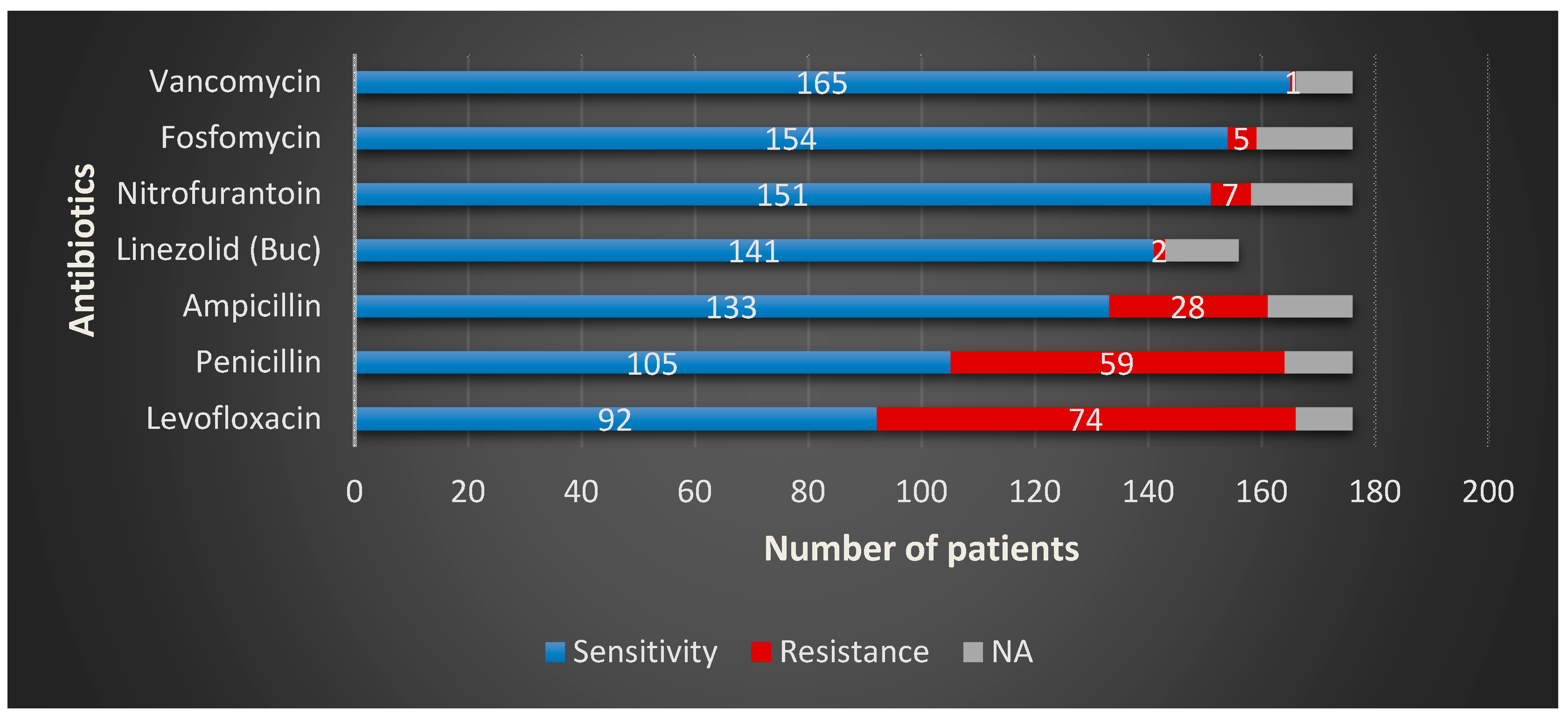
| Antibiotics | Gram-Positive Organism Isolated | ||||
|---|---|---|---|---|---|
| Enterococcus spp. | Staphylococcus spp. | ||||
| R·n/% | S·n/% | NA | R·n/% | S·n/% | |
| Amikacin | - | - | - | 2/4.0 | 46/92.0 |
| Ampicillin | 28/15.90 | 133/75.56 | - | - | - |
| Sumetrolim-Sulfamethoxazole | - | - | - | 18/36.0 | 26/52.0 |
| Ceftazidime | - | - | - | 9/18.0 | 35/70.0 |
| Fosfomycin | 5/2.84 | 154/87.5 | - | - | - |
| Levofloxacin | 74/42.04 | 92/52.27 | - | 27/54.0 | 21/42.0 |
| Linezolid | 2/1.28 | 141/90.38 | 20-MCH | - | - |
| Nitrofurantoin | 7/3.97 | 151/85.79 | - | - | 37/74.0 |
| Penicillin | 59/33.52 | 105/59.65 | - | 33/66.0 | 8/16.0 |
| Vancomycin | 1/0.56 | 165/93.75 | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chibelean, C.B.; Petca, R.-C.; Mareș, C.; Popescu, R.-I.; Enikő, B.; Mehedințu, C.; Petca, A. A Clinical Perspective on the Antimicrobial Resistance Spectrum of Uropathogens in a Romanian Male Population. Microorganisms 2020, 8, 848. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8060848
Chibelean CB, Petca R-C, Mareș C, Popescu R-I, Enikő B, Mehedințu C, Petca A. A Clinical Perspective on the Antimicrobial Resistance Spectrum of Uropathogens in a Romanian Male Population. Microorganisms. 2020; 8(6):848. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8060848
Chicago/Turabian StyleChibelean, Călin Bogdan, Răzvan-Cosmin Petca, Cristian Mareș, Răzvan-Ionuț Popescu, Barabás Enikő, Claudia Mehedințu, and Aida Petca. 2020. "A Clinical Perspective on the Antimicrobial Resistance Spectrum of Uropathogens in a Romanian Male Population" Microorganisms 8, no. 6: 848. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms8060848