
An Adaptive Neuro-Fuzzy Control of Pneumatic Mechanical Ventilator

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Related Works
3. Design of the Mechanical Ventilator
3.1. Requirements of the Mechanical Ventilator
- Possibility of pressure control ventilation (PCV).
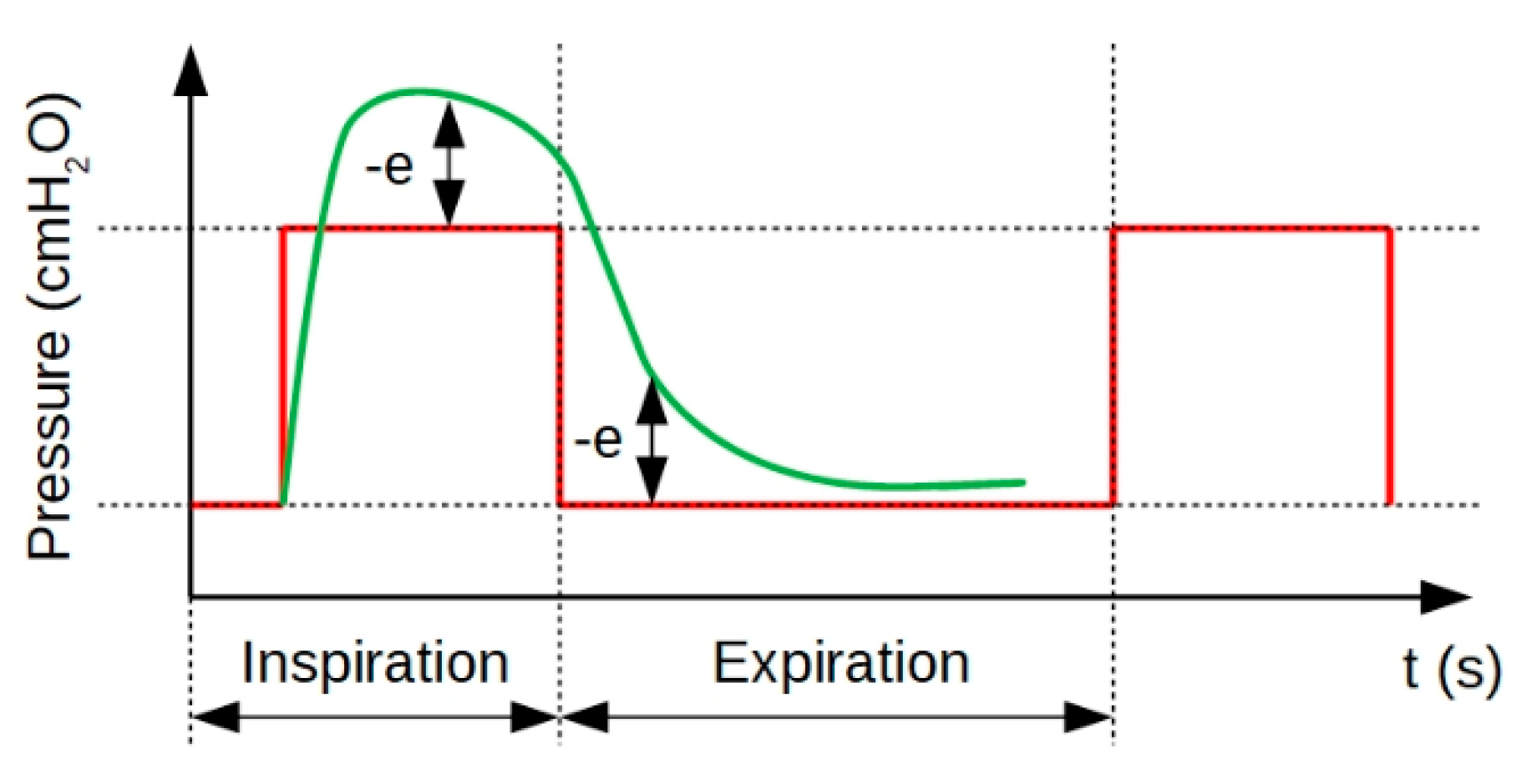
- Peak pressure should be no more than 2 cmH2O greater than plateau pressure.
- PEEP (Positive end-expiratory pressure) must be maintained during expiration.
- For the ratio of inspiration phase/expiration phase, the ventilator must provide a ratio in the range 1:1–1:3.
- The ventilator must provide a range of 10–30 breaths per minute.
- The volume of gas flowing into the lungs during one inspiratory cycle must be at least 400 mL.
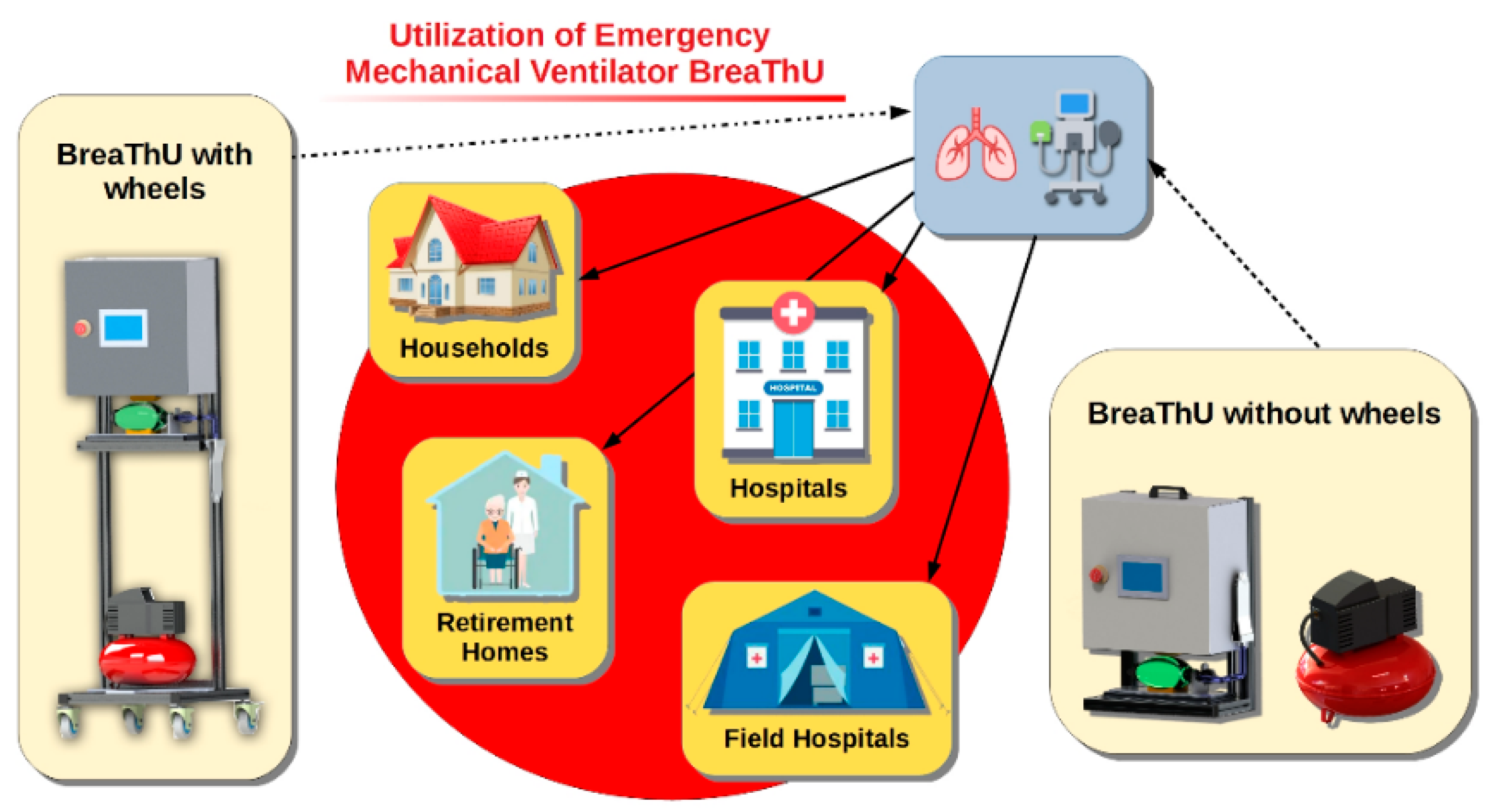
- Portability—A mechanical design should offer an option to use a mechanical ventilator in hospitals or in households. Hence, the portability is an important property. A ventilator should be easily displaced from one to the next required place. In the case of need, the developed ventilator should also have the potential to be used in outdoor applications. For this reason, the ventilator BreaThU can be used as a version with wheels as well as without wheels, with consideration of manual transmission.
- Simplicity—Considering today’s situation, the simplicity of the ventilator is one of the key elements. The ventilator consists of components which can be very easily replaceable. Some of the used components are printed by a three-dimensional (3D) printer and some of them are conventional industrial components which are commercially available. The simplicity of the ventilator ensures fast production of many other ventilators for the cases of unmanageable pandemic situations, when there may be a shortage of professional ventilators in the hospitals.
- Fast reproducibility—Since one of the main aims of the ventilator BreaThU is utilization in very critical situations, the ventilator was designed to be quickly reproducible. For this reason, a mechanical and electrical design was adapted for this point.
- Robustness—Mechanical robustness of the ventilator is an important point especially for outdoor applications, such as field hospitals.
- Hospital, field hospitals and household utilization—As well as hospital utilization of the ventilator BreaThU, it also has potential to be applied in field hospitals and in households, especially for seniors.
- IoT—The next important requirement for the ventilator was internet access ability. In this way, the data collected during the ventilation process can be collected and saved to a database. Subsequently, necessary statistics and analyses of the ventilation process of patients can be performed. There is also the possibility to set required ventilation parameters remotely.
3.2. Mechanical Design
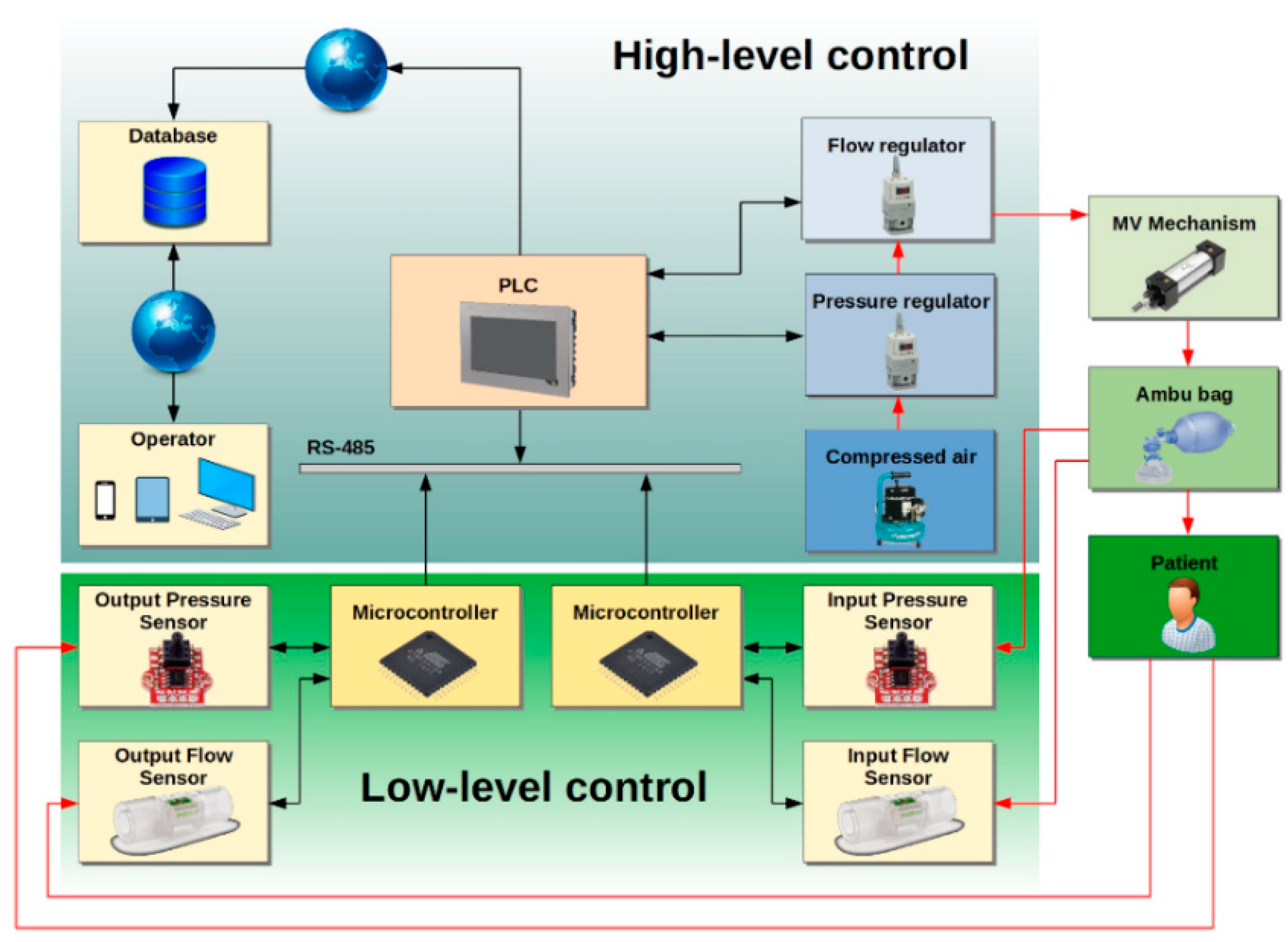
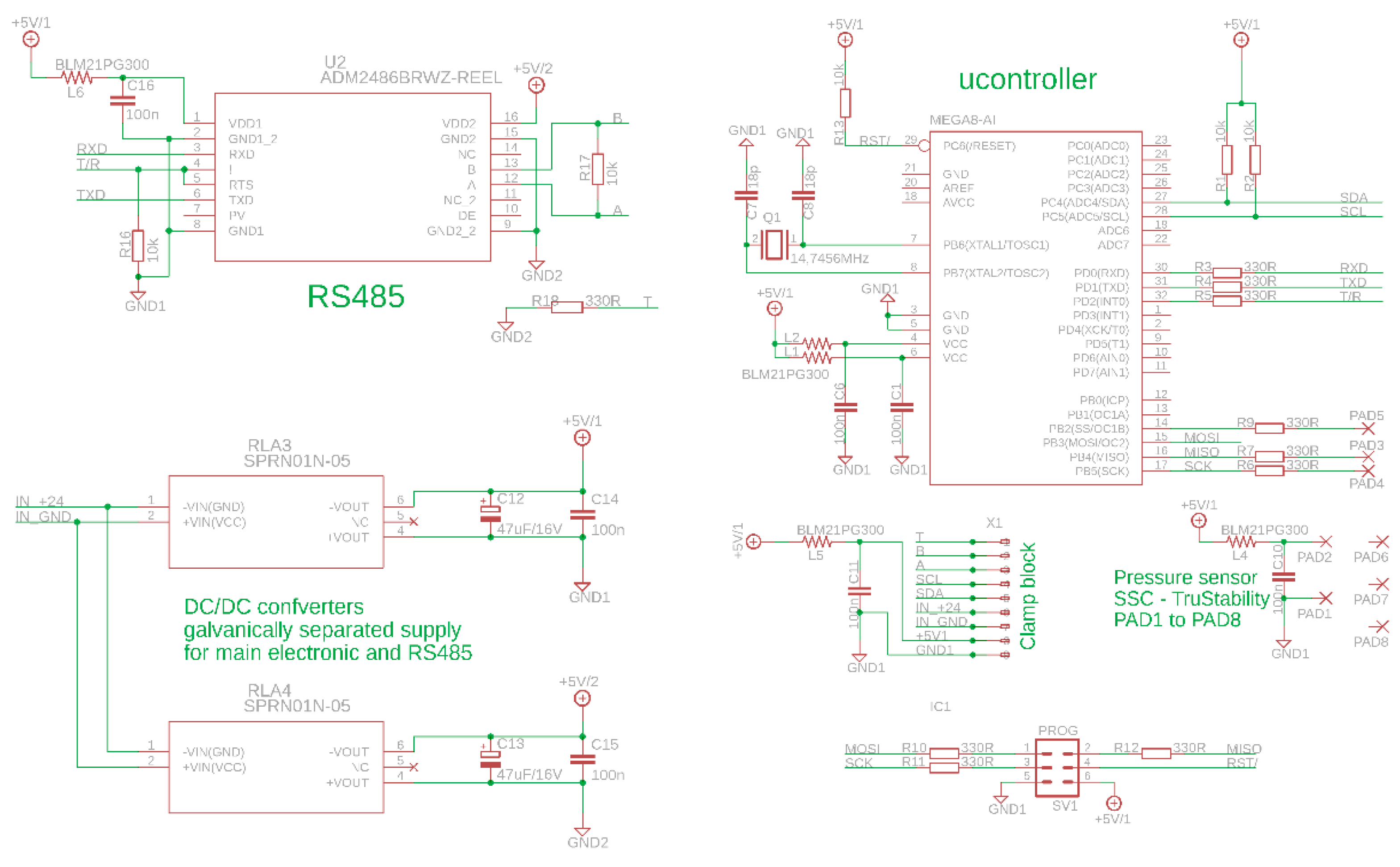
3.3. Hardware Design
3.4. Control Modes of the Ventilator
4. Design of Control System
4.1. Problem Formulation
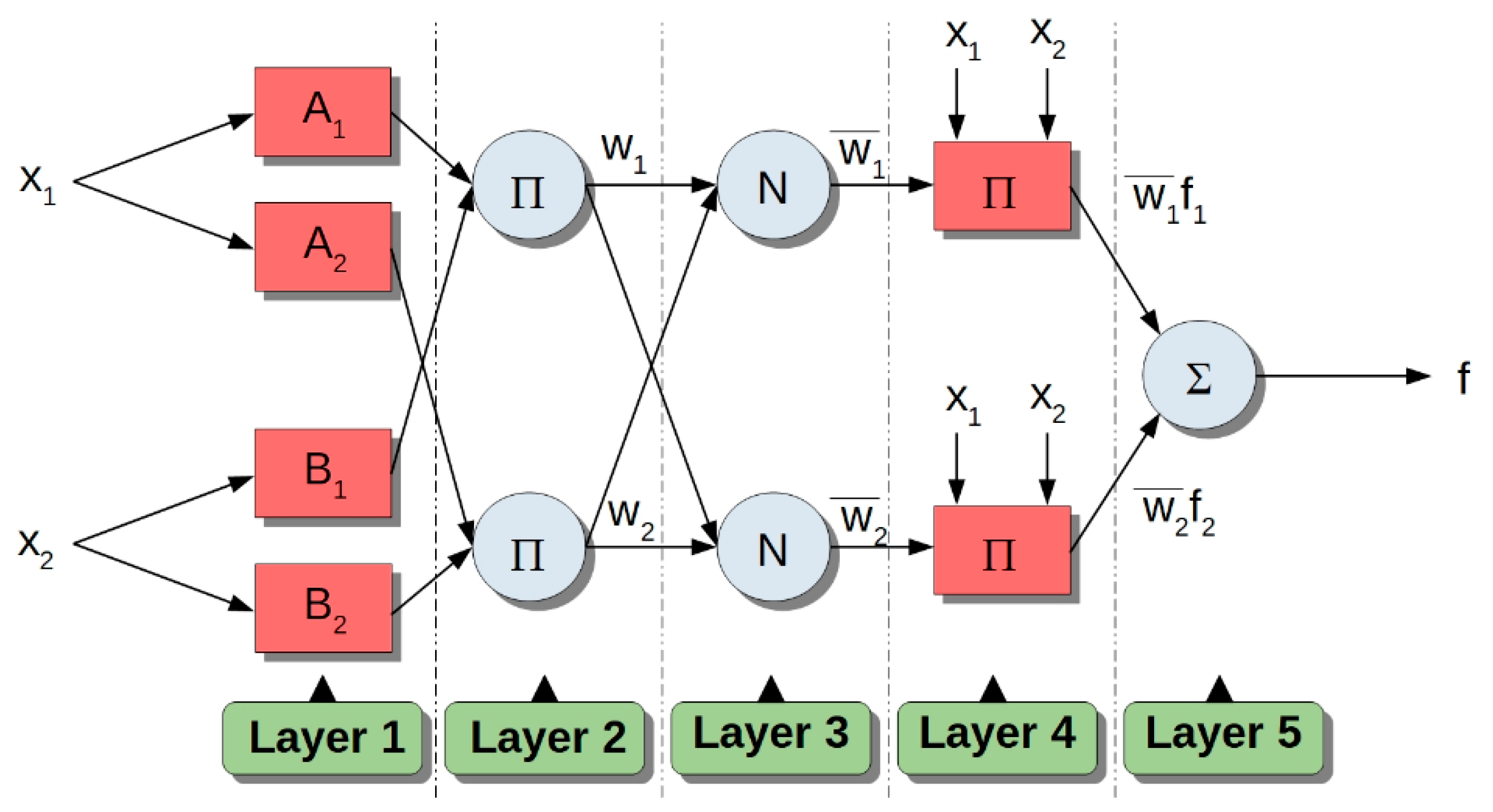
4.2. Adaptive Neuro-Fuzzy Inference System
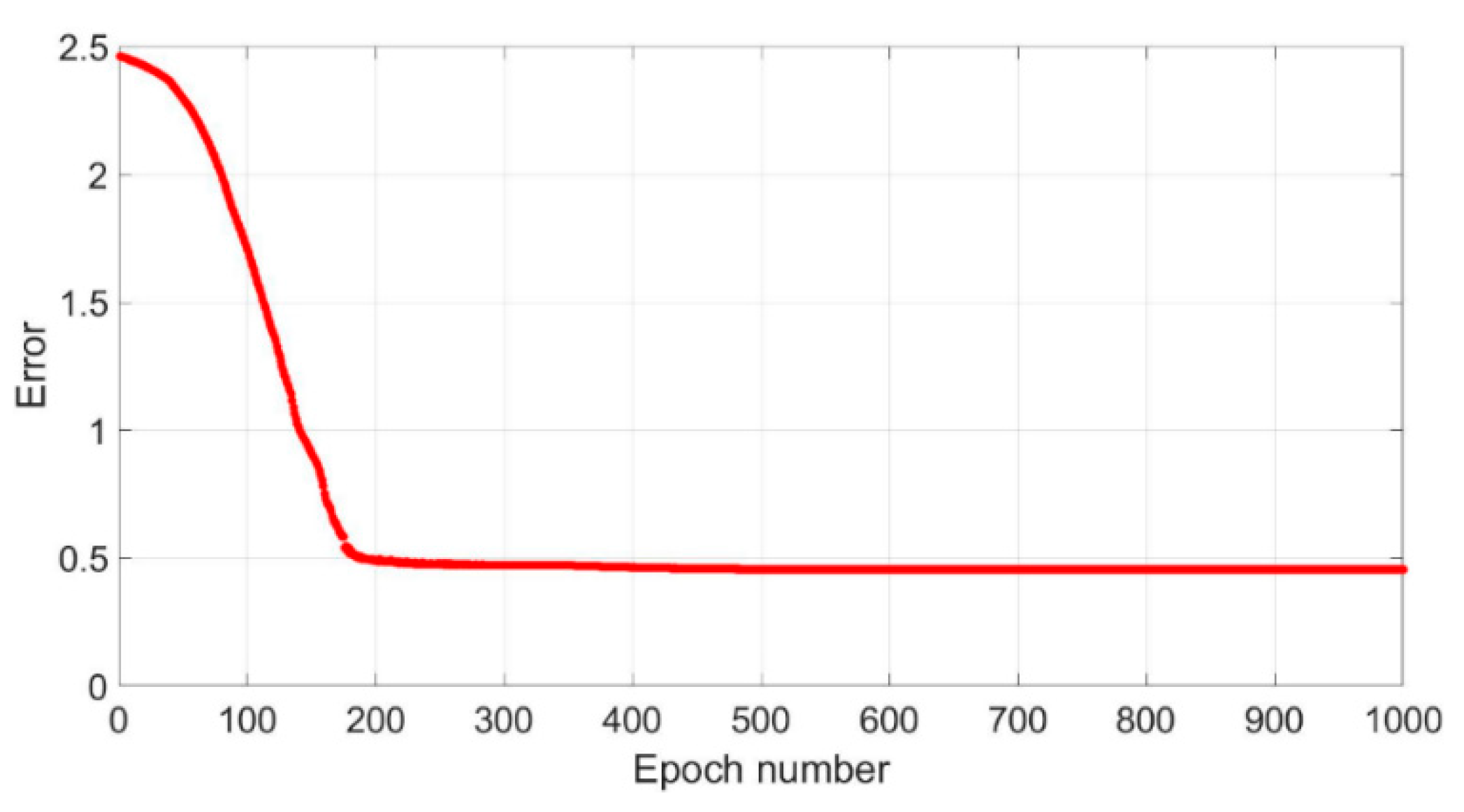
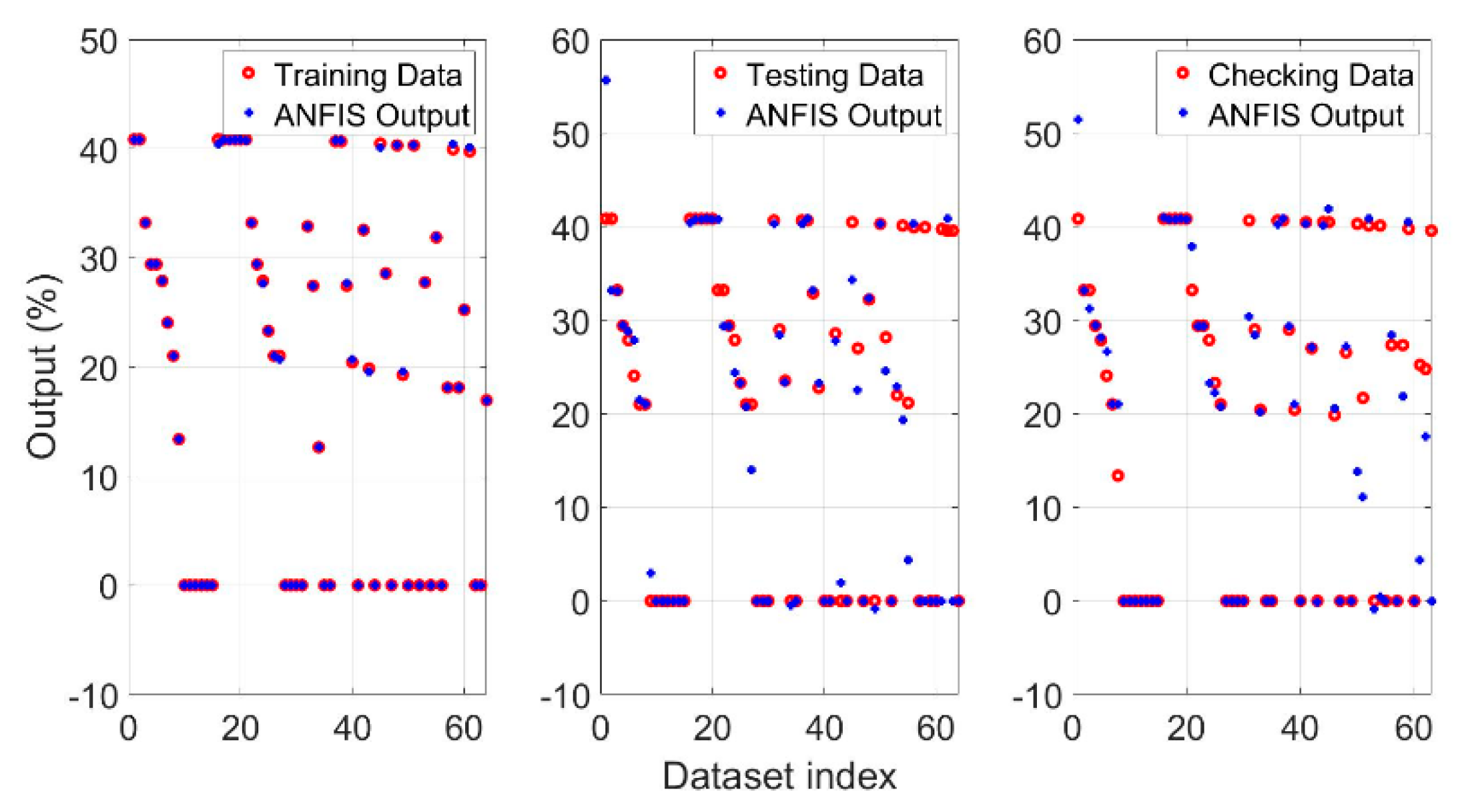
4.3. Collecting Data and Training Process
| Algorithm 1: Data Collecting. |
| 1: Setting of initial parameters of ventilation 2: WHILE (collecting Process is Alive = true) 3: Measuring of control error and speed error 4: IF 5: set the output control 6: …. 7: ELSEIF 8: set the output control 9: END_IF 10: IF 11: decrease 12: ELSE 13: increase 14: END_IF 15: 16: END_WHILE |
| Algorithm 2: Fuzzy rules. |
| 1: WHILE (ventilationProcess==isAlive) 2: Resetting previous states, order = 0 3: Determination of input variables: e, de, pref 4: Fuzzification 5: FOR er=1:14 6: FOR se=1:7 7: FOR rp=1:2 8: order = order + 1 9: IF e==eMF[er] AND de==seMF[se] AND pref==rpMF[rp] 10: output = outputMF[order] 11: END_IF 12: END_FOR 13: END_FOR 14: END_FOR 15: END_WHILE |
5. Simulations and Experiments
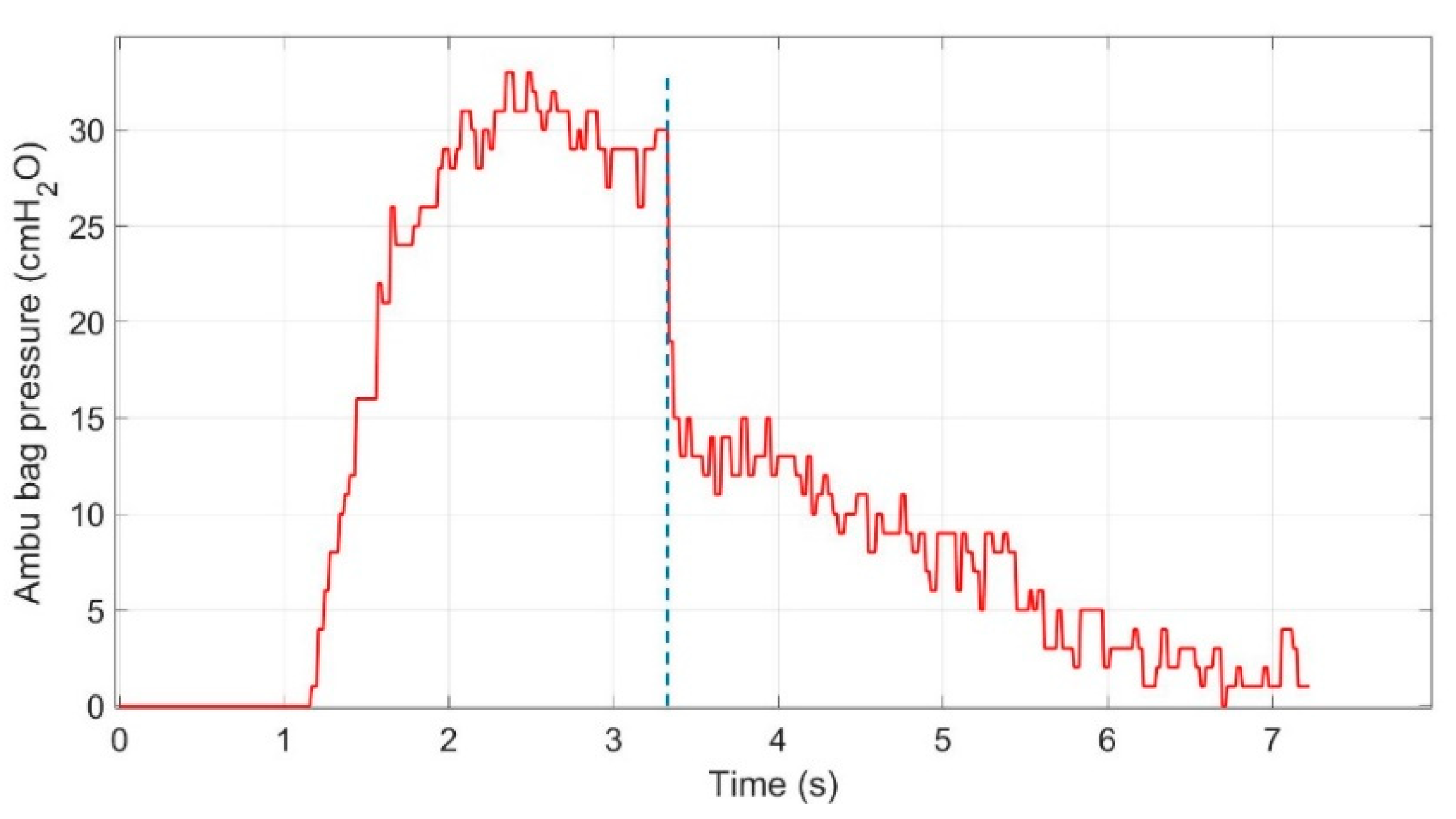
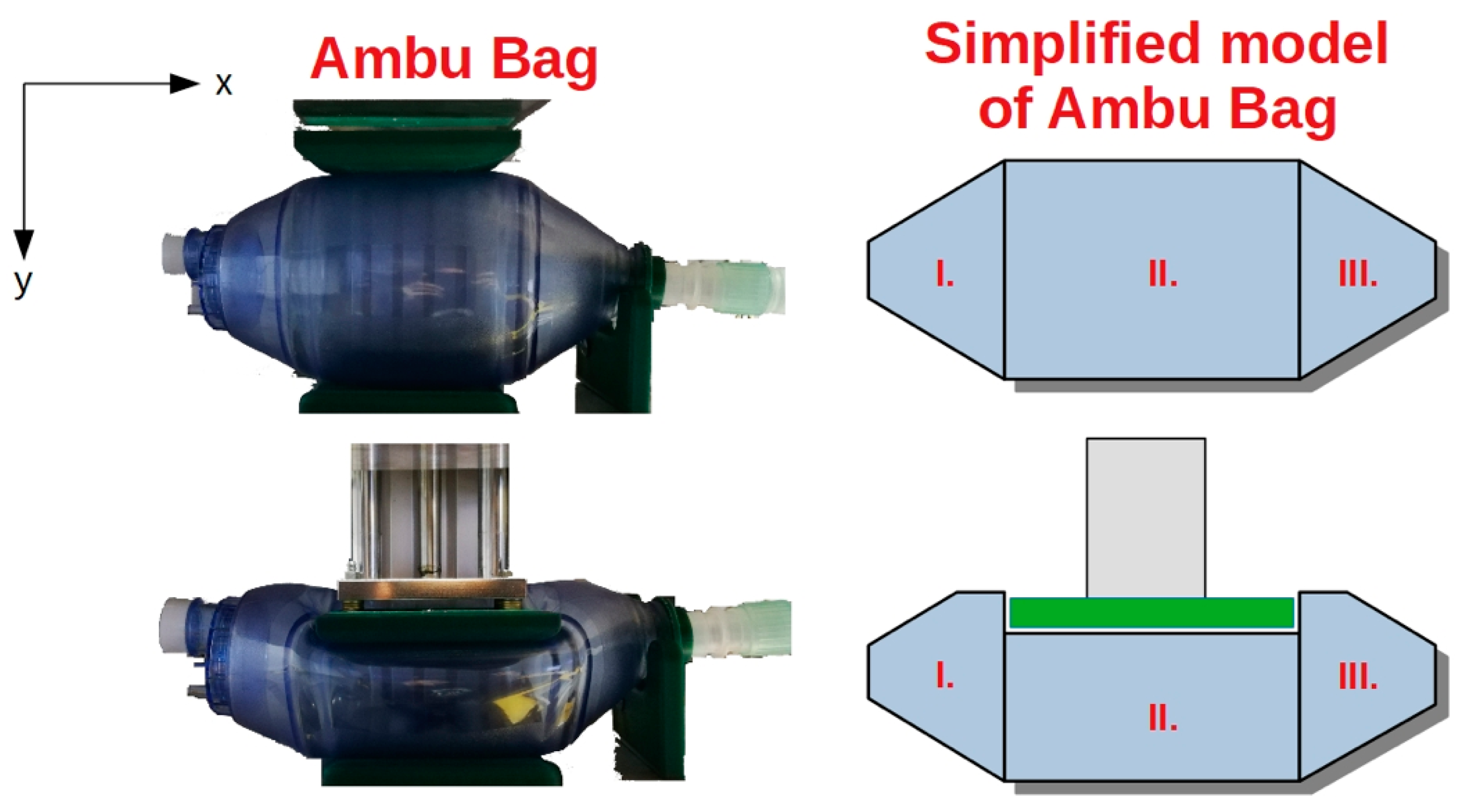
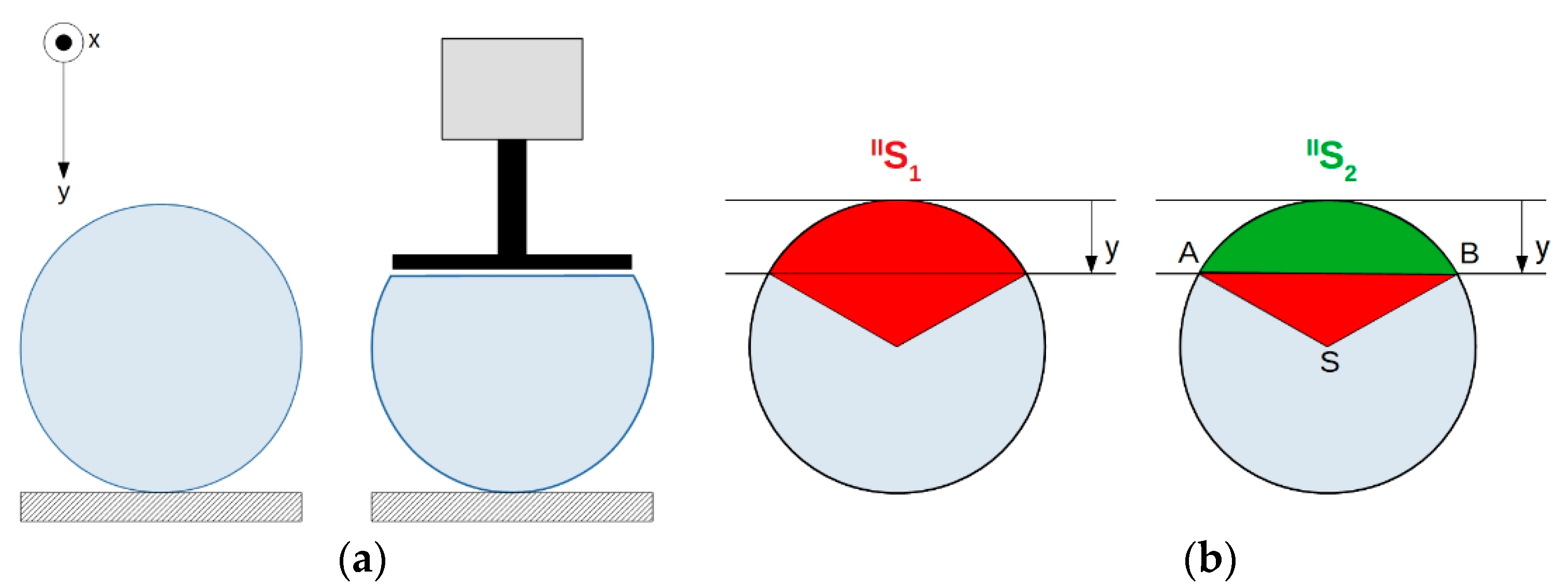
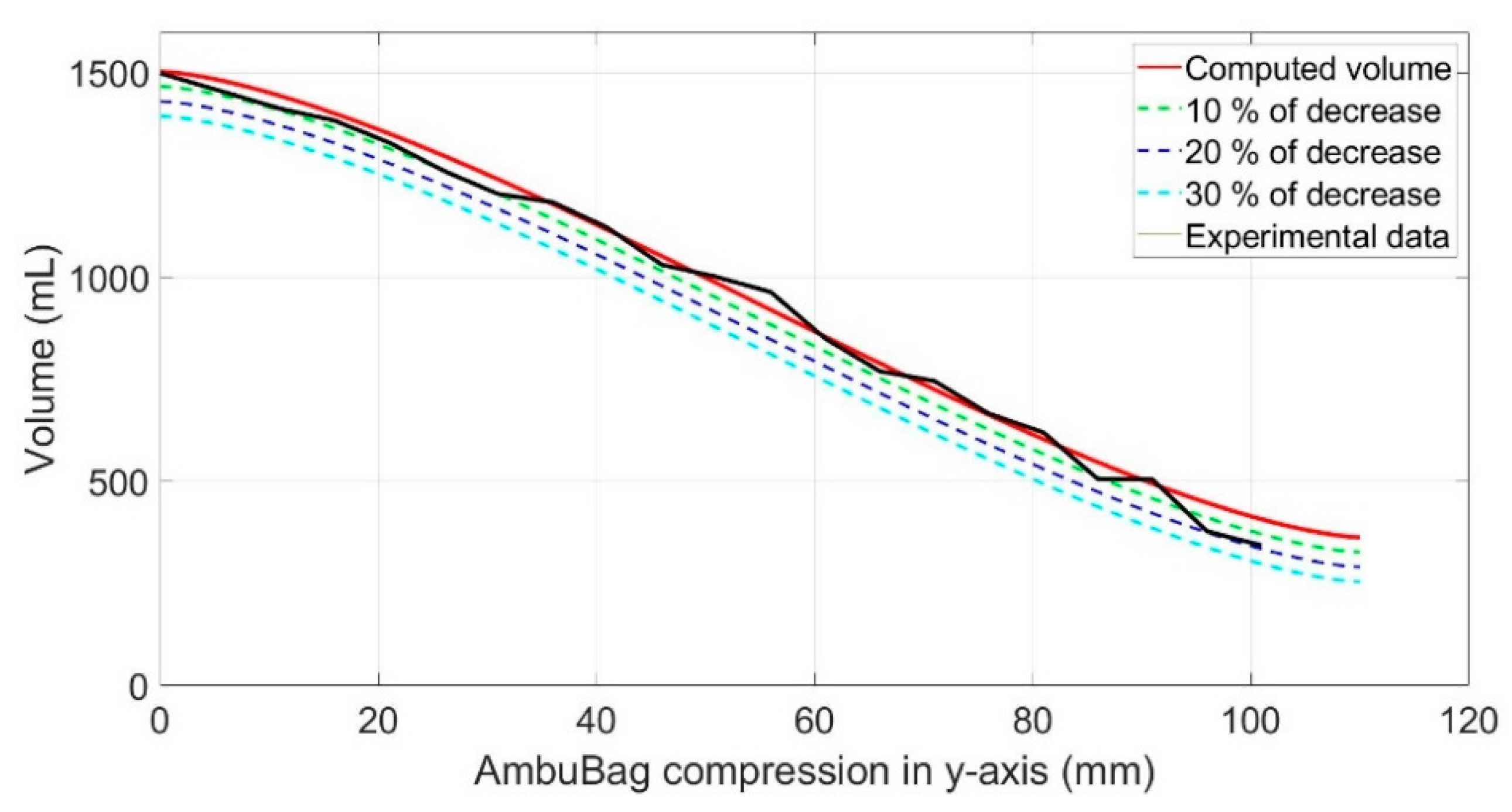
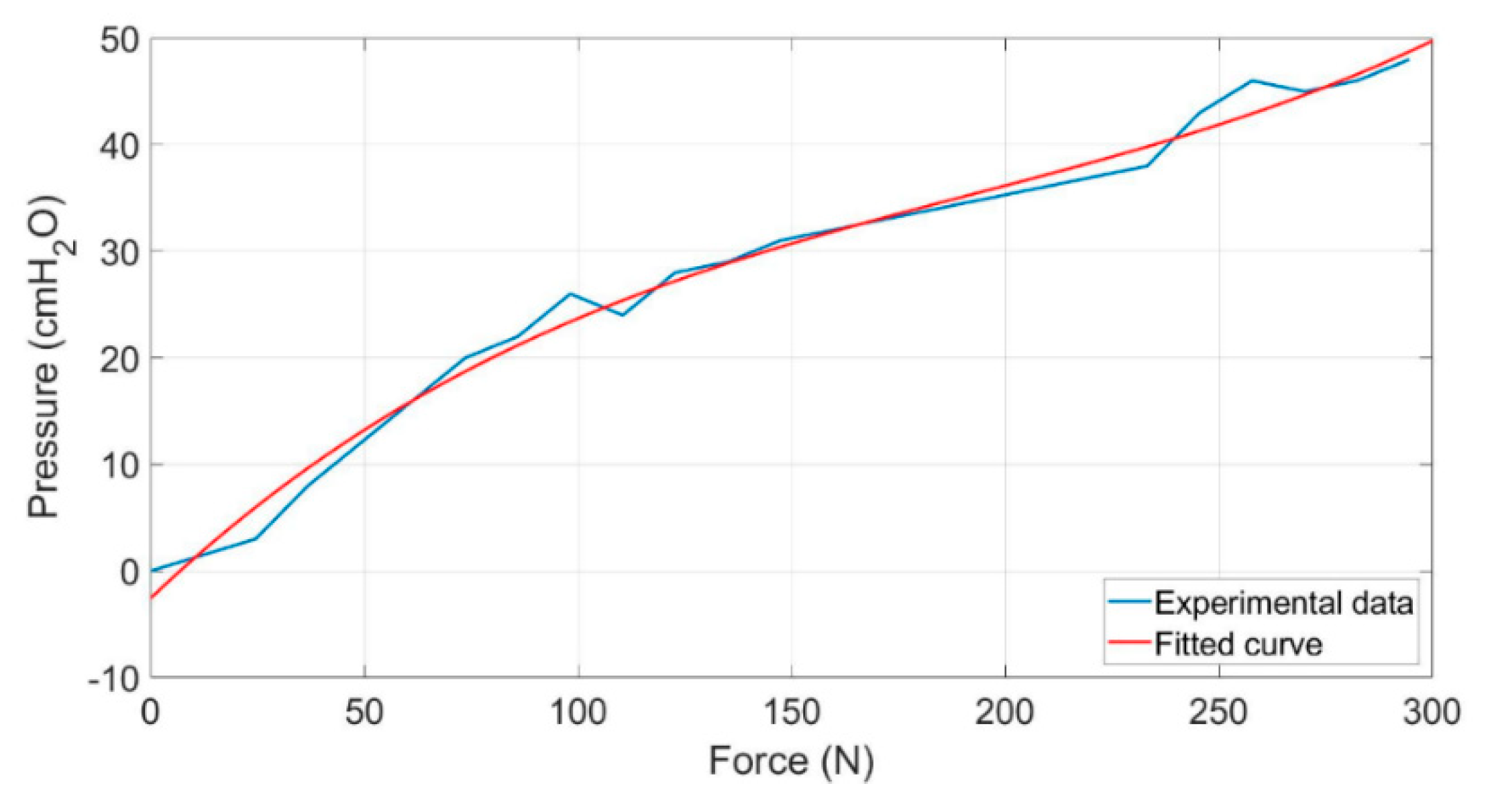
5.1. Mathematical Description and Experimental Analysis of AmbuBag
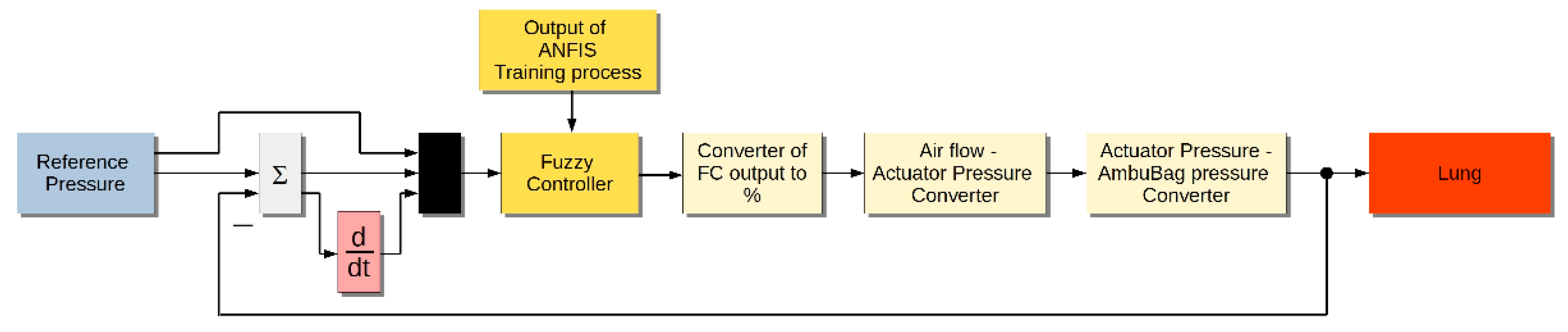
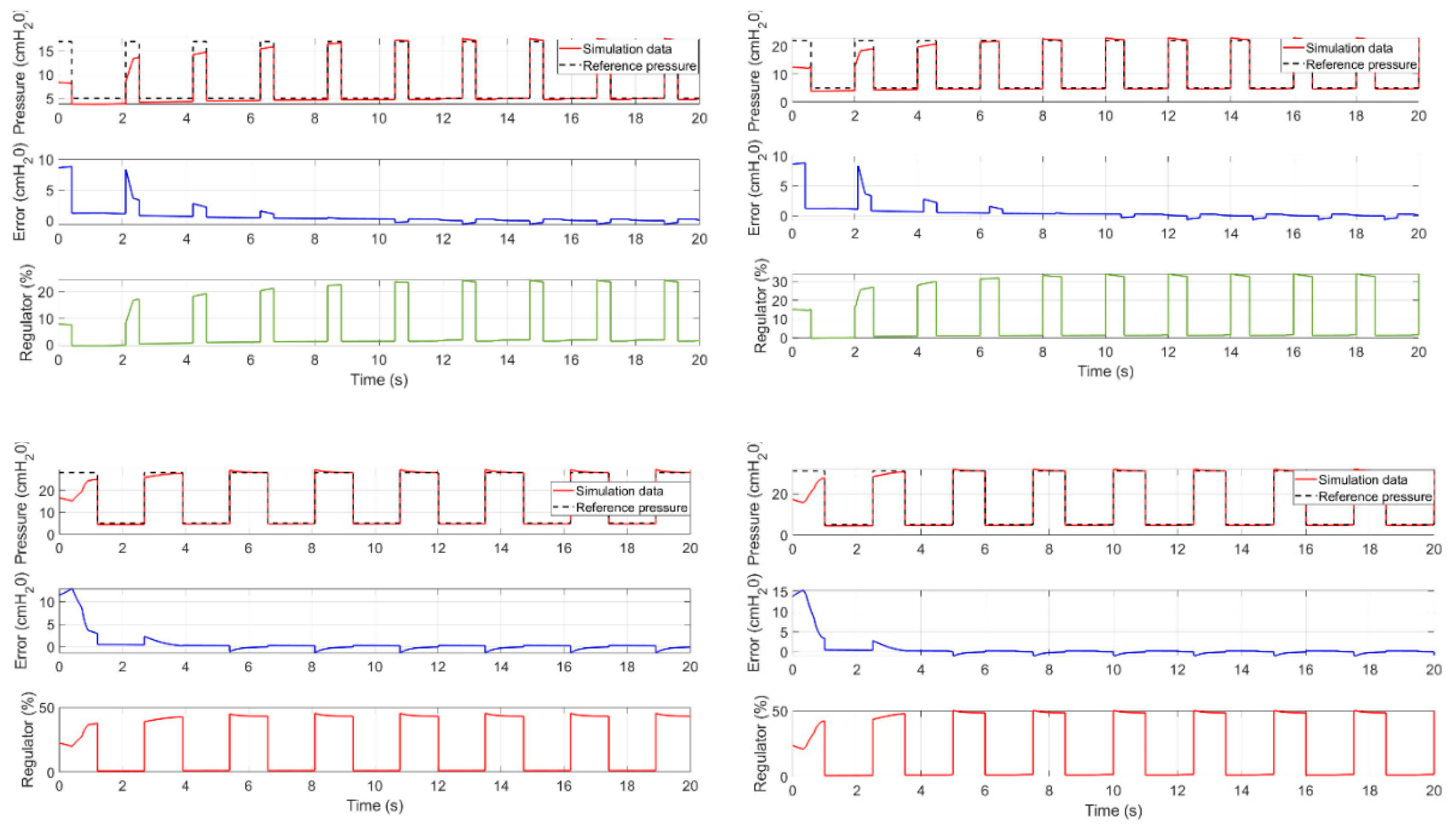
5.2. Simulation Model
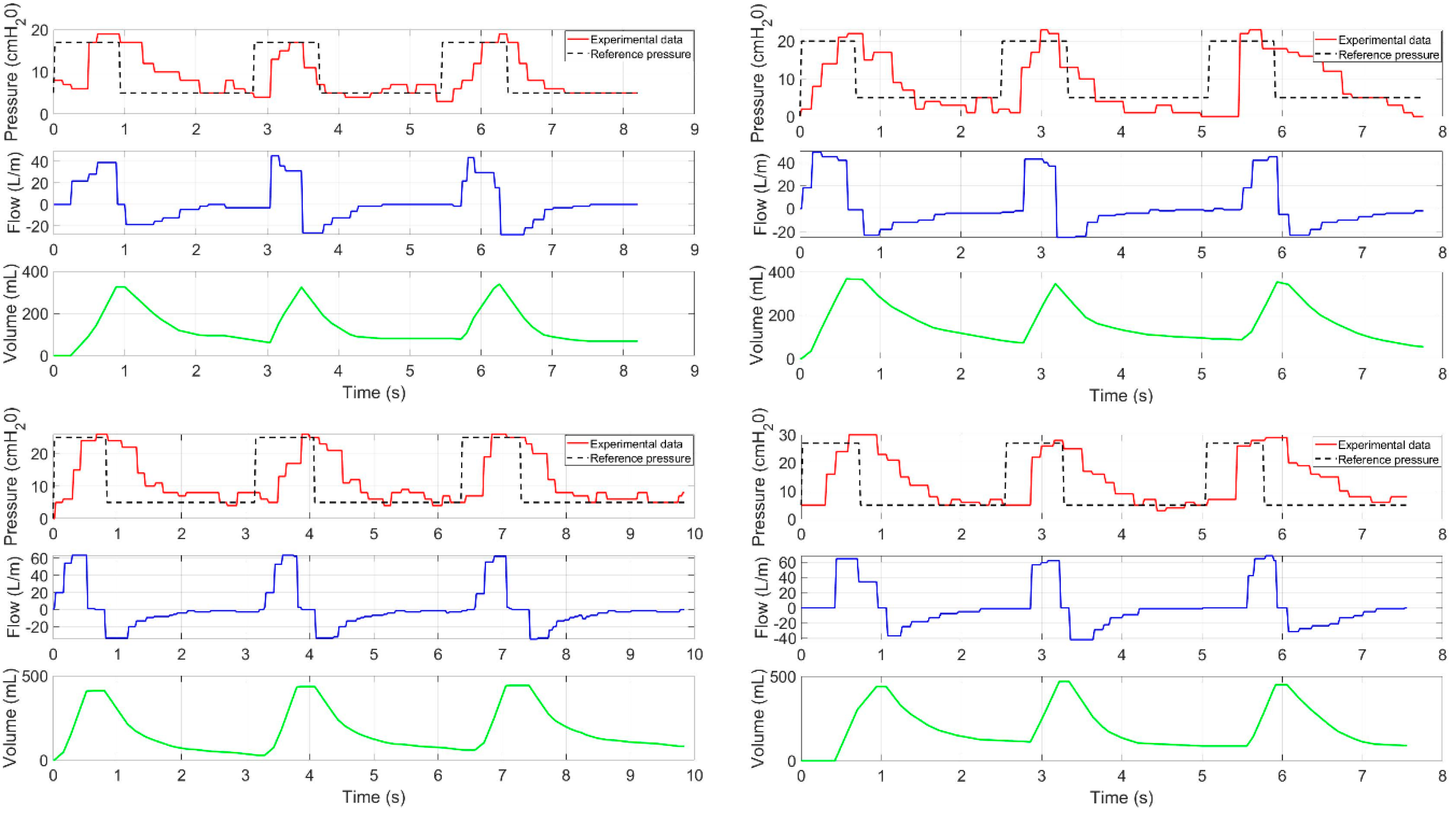
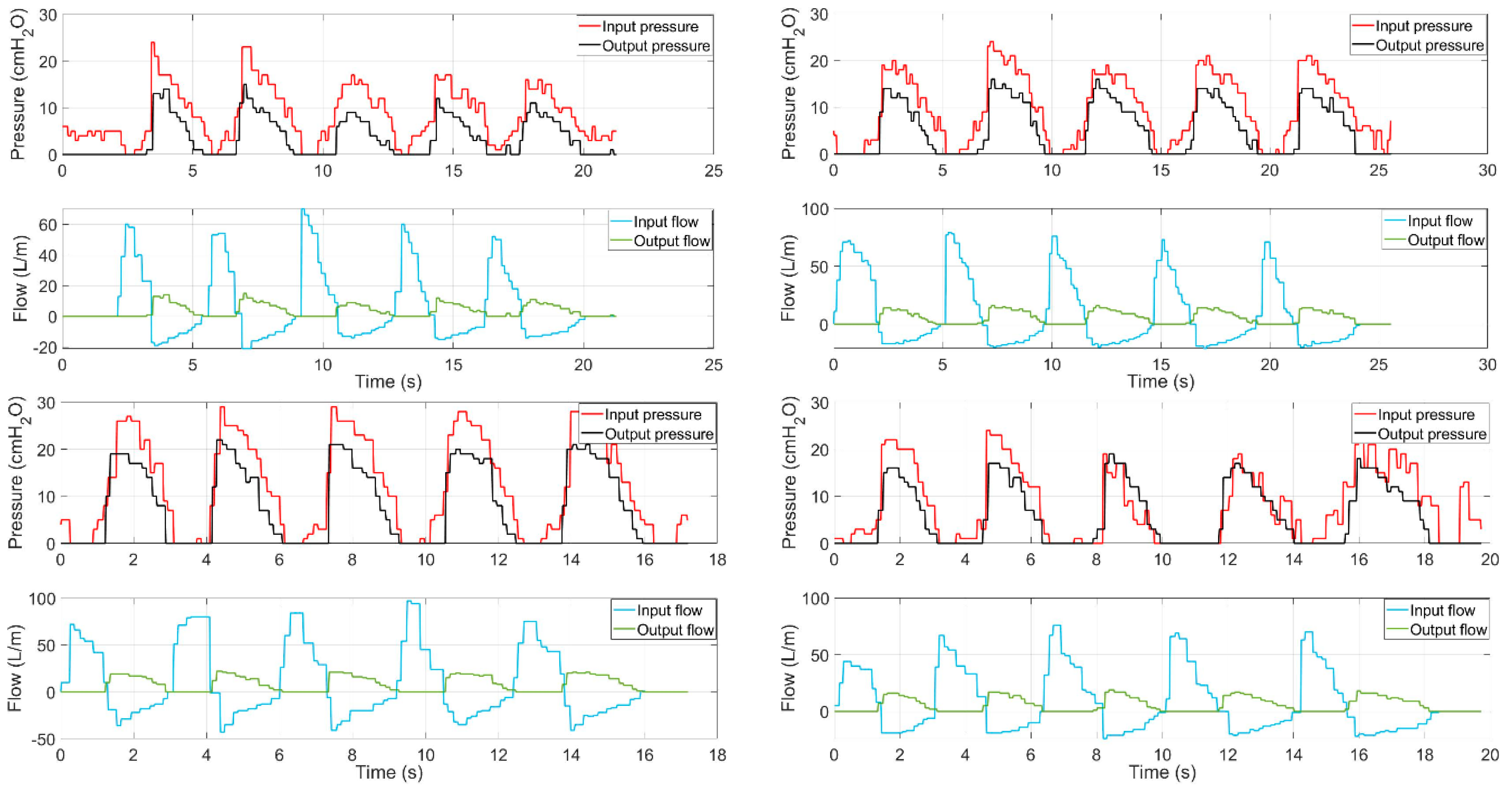
5.3. Experiments
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

References
- Hoehl, S.; Rabenau, H.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; Behrens, P.; Böddinghaus, B.; Götsch, U.; Naujoks, F.; et al. Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China. N. Engl. J. Med. 2020, 382, 1278–1280. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 29 April 2019).
- Wang, D.; Zhou, M.; Nie, X.; Qiu, W.; Yang, M.; Wang, X.; Xu, T.; Ye, Z.; Feng, X.; Xiao, Y.; et al. Epidemiological characteristics and transmission model of Corona Virus Disease 2019 in China. J. Infect. 2020, 80, e25–e27. [Google Scholar] [CrossRef]
- Lipinski, T.; Ahmad, D.; Serey, N.; Jouhara, H. Review of ventilation strategies to reduce the risk of disease transmissionin high occupancy buildings. Int. J. Thermofluids 2020, 7. [Google Scholar] [CrossRef]
- Carter, C.; Osborn, M. COVID-19 disease: Invasive ventilation. Clin. Integr. Care 2020, 1. [Google Scholar] [CrossRef]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung Recruitment in Patients with the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2006, 354, 1775–1786. [Google Scholar] [CrossRef] [PubMed]
- Dostál, P. Základy Umělé Plicní Ventilace; Maxdorf s.r.o.: Prague, Czech Republic, 2004; ISBN 80-7345-059-3. [Google Scholar]
- Das, A.; Menon, P.P.; Hardman, J.G.; Bates, D.G. Optimization of Mechanical Ventilator Settings for Pulmonary Disease States. IEEE Trans. Biomed. Eng. 2013, 60, 1599–1607. [Google Scholar] [CrossRef]
- Esteban, A.; Anzueto, A.; Frutos, F.; Alía, I.; Brochard, L.; Stewart, T.E.; Benito, S.; Epstein, S.K.; Apezteguía, C.; Nightingale, P.; et al. Characteristics and Outcomes in Adult Patients Receiving Mechanical VentilationA 28-Day International Study. JAMA 2002, 287, 345–355. [Google Scholar] [CrossRef]
- Esteban, A.; Ferguson, N.D.; Meade, M.O.; Frutos-Vivar, F.; Apezteguia, C.; Brochard, L.; Raymondos, K.; Nin, N.; Hurtado, J.; Tomicic, V.; et al. Evolution of Mechanical Ventilation in Response to Clinical Research. Am. J. Respir. Crit. Care Med. 2008, 177, 170–177. [Google Scholar] [CrossRef]
- Islam, R.; Ahmad, M.; Hossain, S.; Islam, M.M.; Ahmed, S.F.U. Designing an Electro-Mechanical Ventilator Based on Double CAM Integration Mechanism. In Proceedings of the 2019 1st International Conference on Advances in Science, Dhaka, Bangladesh, 3–5 May 2019; pp. 1–6. [Google Scholar]
- Acho, L.; Vargas, A.N.; Pujol-V´azquez, G. Low-Cost, Open-Source Mechanical Ventilator with Pulmonary Monitoring for COVID-19 Patients. Actuators 2020, 9, 84. [Google Scholar] [CrossRef]
- Al Husseini, A.M.; Lee, H.J.; Negrete, J.; Powelson, S.; Servi, A.T.; Slocum, A.H.; Saukkonen, J. Design and Prototyping of a Low-Cost Portable Mechanical Ventilator. J. Med. Devices 2010, 4, 027514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Camus, E.; Ornik, J.; Mach, C.; Hernandez-Cardoso, G.; Savalia, B.; Taiber, J.; Ruiz-Marquez, A.; Kesper, K.; Konde, S.; Sommer, C.; et al. Simple Ventilators for Emergency Use Based on Bag-Valve Pressing Systems: Lessons Learned and Future Steps. Appl. Sci. 2020, 10, 7229. [Google Scholar] [CrossRef]
- Petsiuk, A.; Tanikella, N.G.; Dertinger, S.; Pringle, A.; Oberloier, S.; Pearce, J.M. Partially RepRapable automated open source bag valve mask-based ventilator. HardwareX 2020, 8, e00131. [Google Scholar] [CrossRef] [PubMed]
- MIT E-Vent. MIT emergency ventilator project. Available online: https://e-vent.mit.edu/ (accessed on 25 June 2020).
- AndalucíaRespira. Available online: https://www.andaluciarespira.com/en/andalucia-respira-en/ (accessed on 5 February 2021).
- Medicines and Healthcare products Regulatory Agency, Rapidly Manufactured Ventilator System. Available online: https://assets.publishing.service.gov.uk/government/uploads/ (accessed on 17 June 2020).
- Kelemen, M.; Kelemenová, T.; Virgala, I.; Miková, Ľ.; Lipták, T. Rapid Control Prototyping of Embedded Systems Based on Microcontroller. Procedia Eng. 2014, 96, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Virgala, I.; Kelemen, M.; Prada, E.; Lipták, T. Positioning of Pneumatic Actuator Using Open-Loop System. Appl. Mech. Mater. 2015, 816, 160–164. [Google Scholar] [CrossRef]
- Prada, E.; Virgala, I.; Granosik, G.; Gmiterko, A. Mrkva, Štefan Simulation Analysis of Pneumatic Rubber Bellows for Segment of Hyper-Redundant Robotic Mechanism. Appl. Mech. Mater. 2014, 611, 10–21. [Google Scholar] [CrossRef]
- Jang, J.-S.R. ANFIS: Adaptive Network-Based Fuzzy Inference System. IEEE Trans. Syst. Man Cybern. 1993, 23, 665. [Google Scholar] [CrossRef]
- Takagi, T.; Sugeno, M. Fuzzy Identification of Systems and Its Applications to Modeling and Control. Read. Fuzzy Sets Intell. Syst. 1993, 1, 387–403. [Google Scholar] [CrossRef]
- Rezaei, E.; Karami, A.; Yousefi, T.; Mahmoudinezhad, S. Modeling the free convection heat transfer in a partitioned cavity using ANFIS. Int. Commun. Heat Mass Transf. 2012, 39, 470–475. [Google Scholar] [CrossRef]
- Naadimuthu, G.; Liu, D.; Lee, E. Application of an adaptive neural fuzzy inference system to thermal comfort and group technology problems. Comput. Math. Appl. 2007, 54, 1395–1402. [Google Scholar] [CrossRef] [Green Version]
- Ishola, N.B.; Adeyemi, O.O.; Adesina, A.J.; Odude, V.O.; Oyetunde, O.O.; Okeleye, A.A.; Soji-Adekunle, A.R.; Betiku, E. Adaptive neuro-fuzzy inference system-genetic algorithm vs. response surface methodology: A case of optimization of ferric sulfate-catalyzed esterification of palm kernel oil. Process. Saf. Environ. Prot. 2017, 111, 211–220. [Google Scholar] [CrossRef]
- Jang, J.S.R.; Sun, C.T.; Mizutani, E. Neuro-Fuzzy and Soft Computing; Prentice Hall: Upper Saddle River, NJ, USA, 1997. [Google Scholar]
- Al-Hmouz, A.; Shen, J.; Al-Hmouz, R.; Yan, J. Modeling and Simulation of an Adaptive Neuro-Fuzzy Inference System (ANFIS) for Mobile Learning. IEEE Trans. Learn. Technol. 2011, 5, 226–237. [Google Scholar] [CrossRef]
- Premkumar, K.; Manikandan, B.V. Adaptive Neuro-Fuzzy Inference System based speed controller for brushless DC motor. Neurocomputing 2014, 138, 260–270. [Google Scholar] [CrossRef]

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
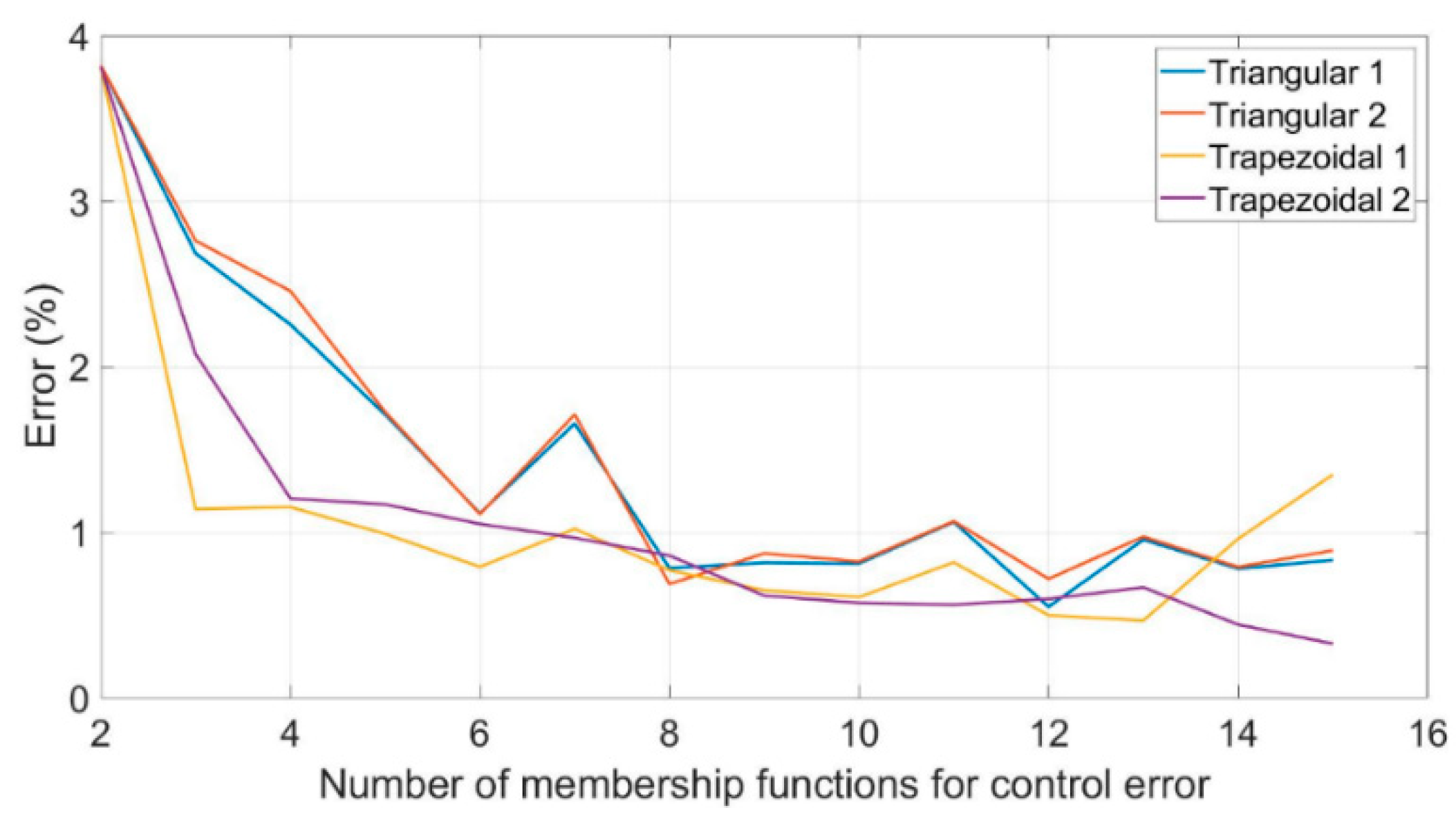
| Control Error (Number of MF) | Speed Error (Number of MF) | Reference. Pressure (Number of MF) | Triangular (%) | Trapezoidal (%) |
|---|---|---|---|---|
| 2 | 2 | 2 | 3.821 | 3.813 |
| 3 | 3 | 2 | 2.686 | 1.142 |
| 4 | 4 | 2 | 2.257 | 1.154 |
| 5 | 5 | 2 | 1.713 | 0.992 |
| 6 | 6 | 2 | 1.116 | 0.793 |
| 7 | 7 | 2 | 1.658 | 1.022 |
| 8 | 8 | 2 | 0.785 | 0.772 |
| 9 | 9 | 2 | 0.818 | 0.651 |
| 10 | 10 | 2 | 0.813 | 0.61 |
| 11 | 11 | 2 | 1.063 | 0.82 |
| 12 | 12 | 2 | 0.551 | 0.5 |
| 13 | 13 | 2 | 0.957 | 0.469 |
| 14 | 14 | 2 | 0.782 | 0.962 |
| 15 | 15 | 2 | 0.834 | 1.35 |
| Control Error (Number of MF) | Speed Error (Number of MF) | Reference Pressure (Number of MF) | Triangular (%) | Trapezoidal (%) |
|---|---|---|---|---|
| 2 | 2 | 2 | 3.821 | 3.813 |
| 3 | 2 | 2 | 2.763 | 2.078 |
| 4 | 2 | 2 | 2.459 | 1.206 |
| 5 | 3 | 2 | 1.728 | 1.17 |
| 6 | 3 | 2 | 1.111 | 1.052 |
| 7 | 4 | 2 | 1.713 | 0.968 |
| 8 | 4 | 2 | 0.689 | 0.861 |
| 9 | 5 | 2 | 0.874 | 0.619 |
| 10 | 5 | 2 | 0.825 | 0.575 |
| 11 | 6 | 2 | 1.068 | 0.564 |
| 12 | 6 | 2 | 0.72 | 0.599 |
| 13 | 7 | 2 | 0.975 | 0.669 |
| 14 | 7 | 2 | 0.792 | 0.444 |
| 15 | 8 | 2 | 0.892 | 0.329 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Živčák, J.; Kelemen, M.; Virgala, I.; Marcinko, P.; Tuleja, P.; Sukop, M.; Liguš, J.; Ligušová, J. An Adaptive Neuro-Fuzzy Control of Pneumatic Mechanical Ventilator. Actuators 2021, 10, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/act10030051
Živčák J, Kelemen M, Virgala I, Marcinko P, Tuleja P, Sukop M, Liguš J, Ligušová J. An Adaptive Neuro-Fuzzy Control of Pneumatic Mechanical Ventilator. Actuators. 2021; 10(3):51. https://0-doi-org.brum.beds.ac.uk/10.3390/act10030051
Chicago/Turabian StyleŽivčák, Jozef, Michal Kelemen, Ivan Virgala, Peter Marcinko, Peter Tuleja, Marek Sukop, Ján Liguš, and Jana Ligušová. 2021. "An Adaptive Neuro-Fuzzy Control of Pneumatic Mechanical Ventilator" Actuators 10, no. 3: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/act10030051