
Effects of Allogeneic Mesenchymal Stem Cell Transplantation in Dogs with Inflammatory Bowel Disease Treated with and without Corticosteroids


 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Groups
- −
- MSC group: Animals without any treatment at least 21 days before MSC administration.
- −
- P-MSC group: Animals treated with prednisone at the time of MSC administration (all other immunosuppressant drugs except prednisone were withdrawn at least 21 days before the MSC administration). The starting dose of prednisone in dogs in this group was between 0.75 and 2 mg/kg per day. In addition, the prednisone dosage was assessed and reduced at the different time points post-treatment if CIBDAI and CCECAI scores dropped more than 30% of the previous value. If not, the dosage was maintained.
2.3. Initial Tests
2.4. Isolation and In Vitro Expansion of Adipose-Derived Mesenchymal Stem Cells
2.5. Adipose-Derived Mesenchymal Stem Cell Administration
2.6. Study Procedure
2.7. Statistical Study
3. Results
3.1. Animals and Groups
3.2. Symptomatology
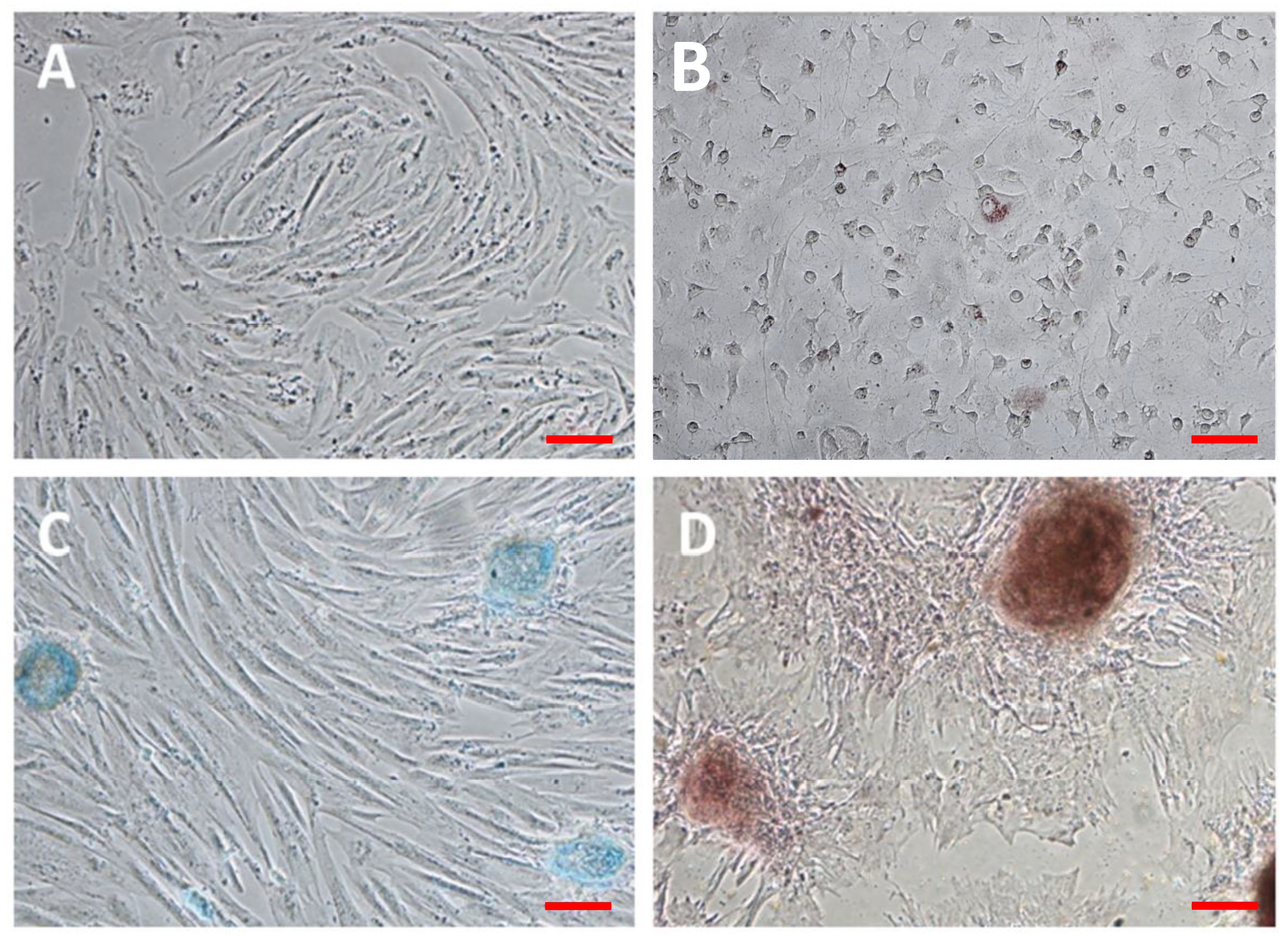
3.3. Characterization of Adipose-Derived Mesenchymal Stem Cells
3.4. Results of the Parameters Studied
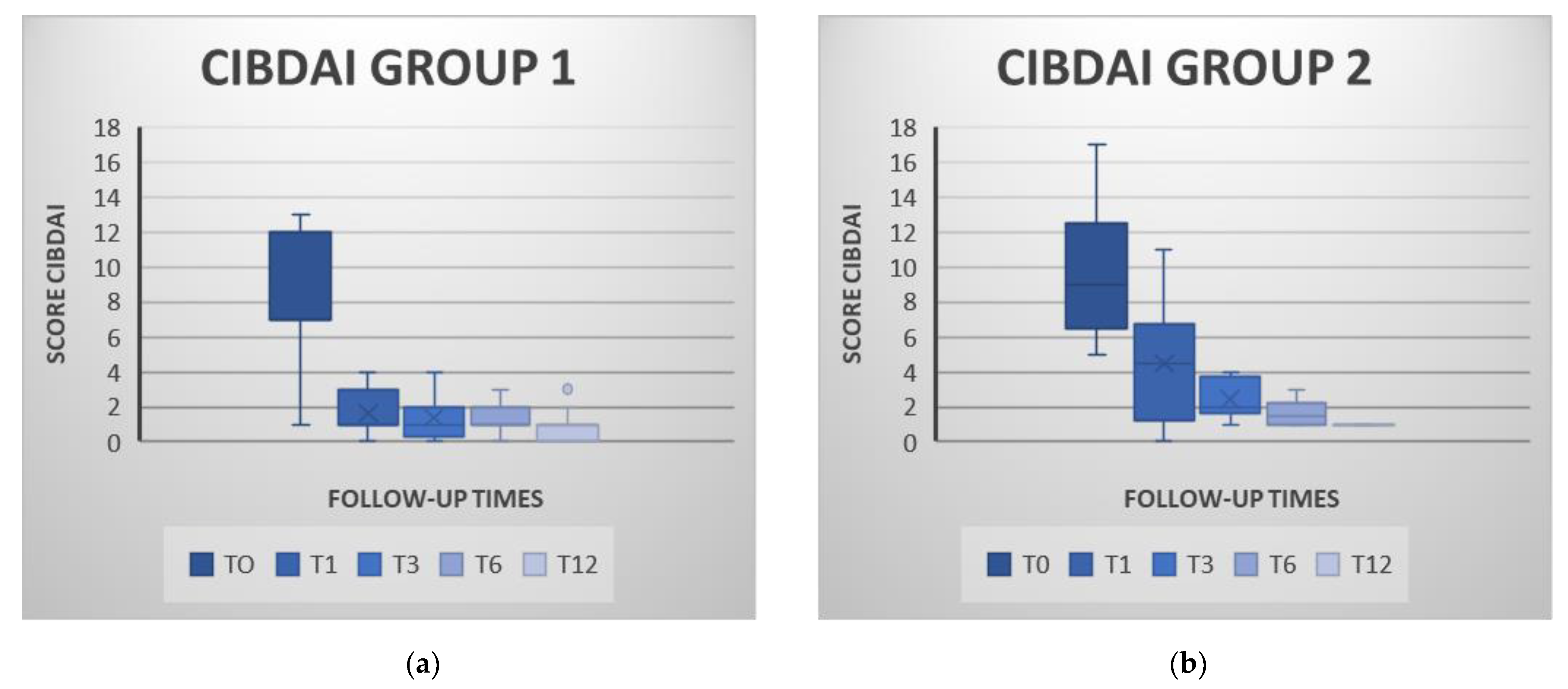
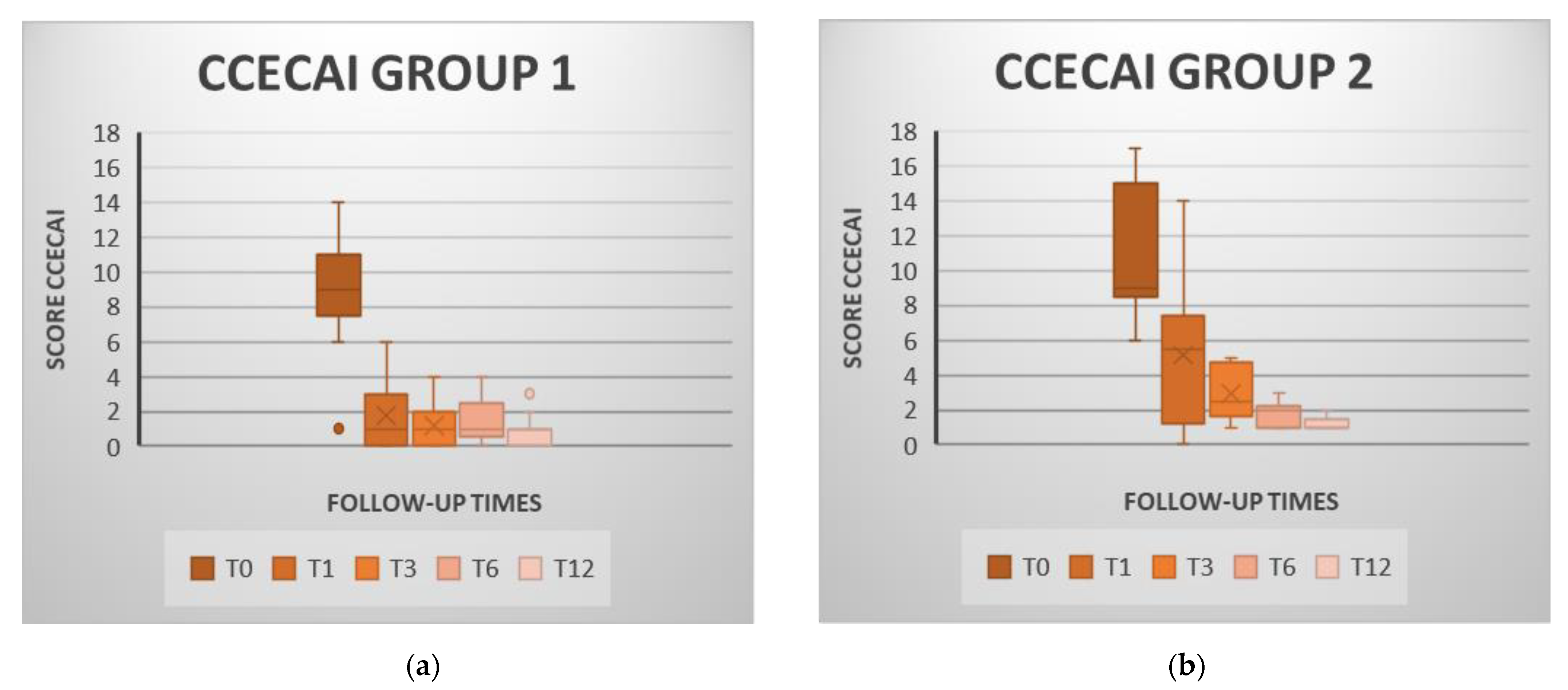
3.4.1. Clinical Activity Indices
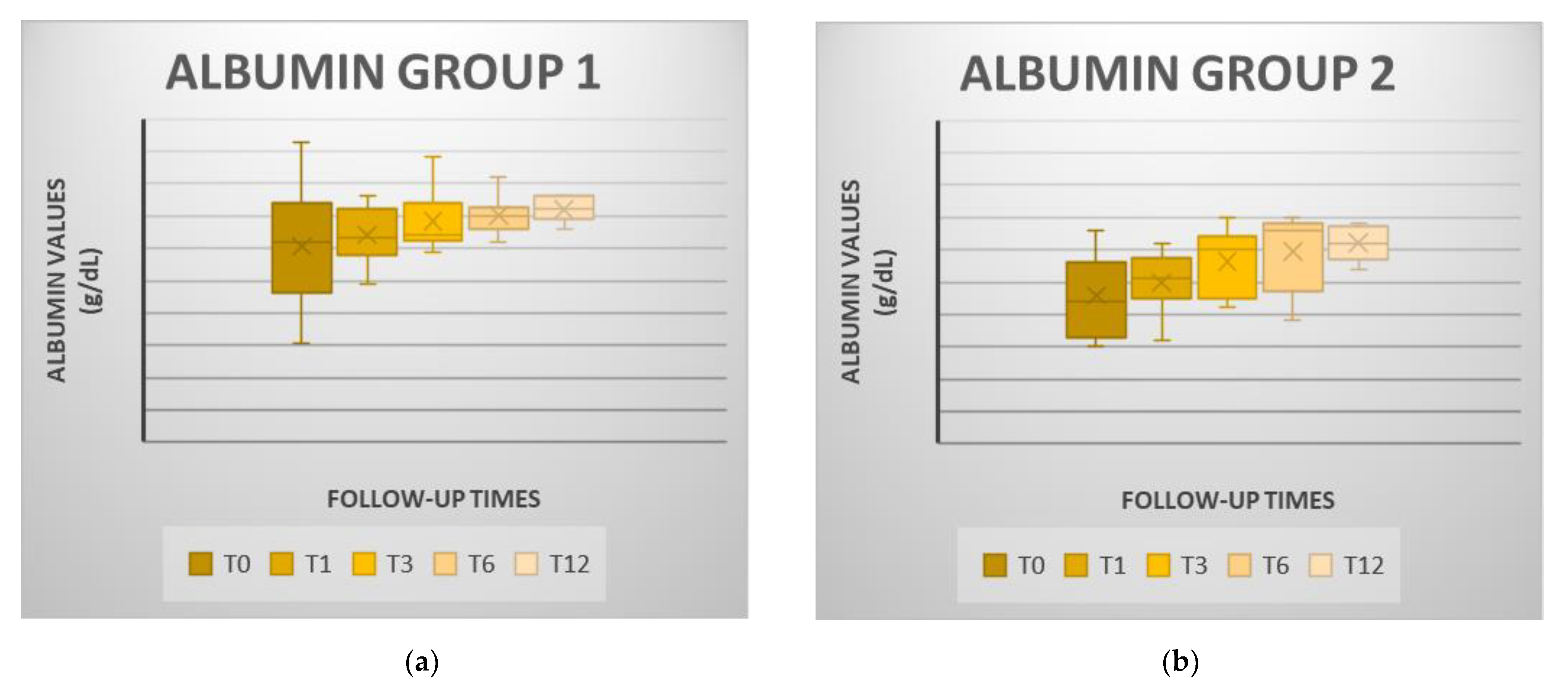
3.4.2. Albumin
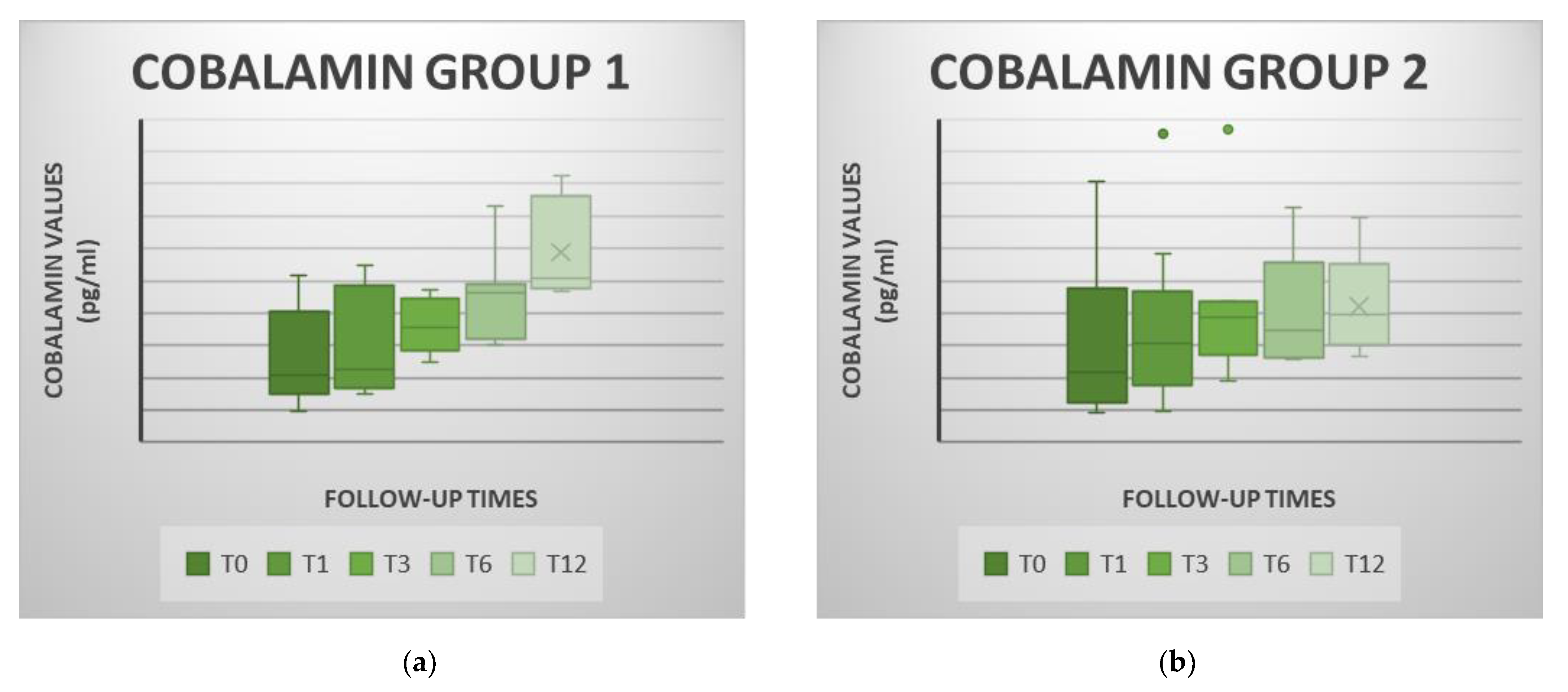
3.4.3. Cobalamin
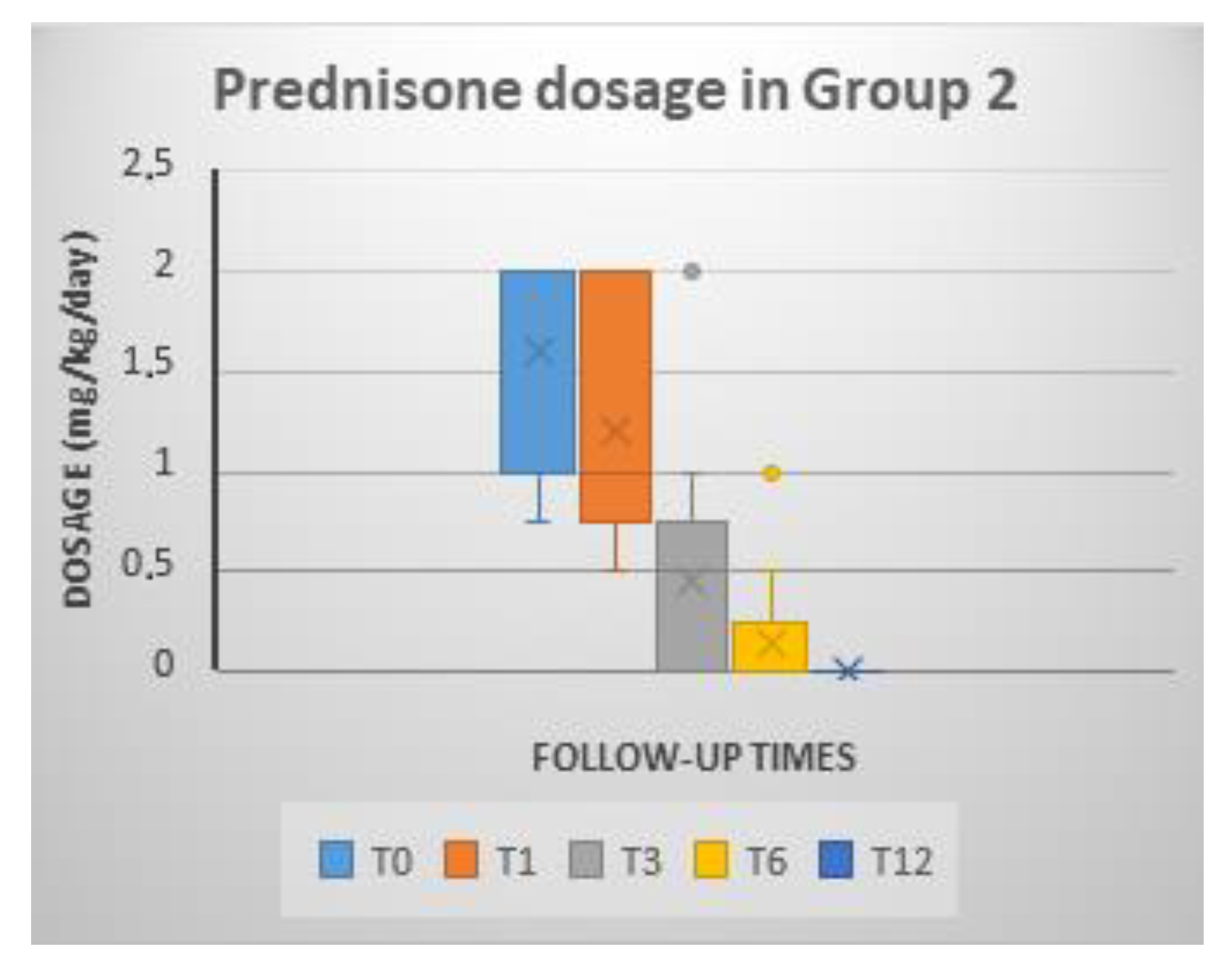
3.4.4. Prednisone Dosage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Simpson, K.W.A.; Jergens, A.E. Pitfalls and progress in the diagnosis and management of canine inflammatory bowel disease. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 381–398. [Google Scholar] [CrossRef]
- Cerquetella, M.; Spaterna, A.; Laus, F.; Tesei, B.; Rossi, G.; Antonelli, E.; Villanacci, V.; Bassotti, G. Inflammatory bowel disease in the dog: Differences and similarities with humans. World J. Gastroenterol. 2010, 16, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Allenspach, K. Clinical immunology and immunopathology of the canine and feline intestine. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Jergens, A.E.; Simpson, K.W. Inflammatory bowel disease in veterinary medicine. Front. Biosci. 2012, 4, 1404–1419. [Google Scholar] [CrossRef]
- Ricart, E.; Jauregui-Amezaga, A.; Ordás, I.; Pinó, S.; Ramírez, A.M. Cell therapies for IBD: What works? Curr. Drug Targets 2013, 14, 1453–1459. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, S.; Ding, X.; Guo, J.; Tian, Z. Potential methods for improving the efficacy of mesenchymal stem cells in the treatment of inflammatory bowel diseases. Scand. J. Immunol. 2020, 92, e12897. [Google Scholar] [CrossRef] [PubMed]
- Dias, I.E.; Pinto, P.O.; Barros, L.C.; Viegas, C.A.; Dias, I.R.; Carvalho, P.P. Mesenchymal stem cells therapy in companion animals: Useful for immune-mediated diseases? BMC Vet. Res. 2019, 15, 358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, T.L.; Webb, C.B. Stem cell therapy in cats with chronic enteropathy: A proof-of-concept study. J. Feline Med. Surg. 2015, 17, 901–908. [Google Scholar] [CrossRef]
- Pérez-Merino, E.M.; Usón-Casaús, J.M.; Zaragoza-Bayle, C.; Duque-Carrasco, J.; Mariñas-Pardo, L.; Hermida-Prieto, M.; Barrera-Chacón, R.; Gualtieri, M. Safety and efficacy of allogeneic adipose tissue-derived mesenchymal stem cells for treatment of dogs with inflammatory bowel disease: Clinical and laboratory outcomes. Vet. J. 2015, 206, 385–390. [Google Scholar] [CrossRef]
- Duijyestein, M.; Vos, A.C.; Roelofs, H.; Wildenberg, M.E.; Wendrich, B.B.; Verspaget, H.W.; Kooy-Winkelaar, E.M.C.; Koning, F.; Zwaginga, J.J.; Fidder, H.H.; et al. Autologous bone marrow-derived mesenchymal stromal cell treatment for refractory luminal Crohn’s disease: Results of a phase I study. Gut 2010, 59, 1662–1669. [Google Scholar] [CrossRef]
- Zhang, J.; Lv, S.; Liu, X.; Song, B.; Shi, L. Umbilical Cord Mesenchymal Stem Cell Treatment for Crohn’s Disease: A Randomized Controlled Clinical Trial. Gut Liver 2018, 12, 73–78. [Google Scholar] [CrossRef]
- Liang, J.; Zhang, H.; Wang, D.; Feng, X.; Wang, H.; Hua, B.; Liu, B.; Sun, L. Allogeneic mesenchymal stem cell transplantation in seven patients with refractory inflammatory bowel disease. Gut 2012, 61, 468–469. [Google Scholar] [CrossRef] [PubMed]
- Jergens, A.E.; Schreiner, C.A.; Frank, D.E.; Niyo, Y.; Ahrens, F.E.; Eckersall, P.D.; Benson, T.J.; Evans, R. A scoring index for disease activity in canine inflammatory bowel disease. J. Vet. Intern. Med. 2003, 17, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Allenspach, K.; Wieland, B.; Grone, A.; Gaschen, F. Chronic enteropathies in dogs: Evaluation of risk factors for negative outcome. J. Vet. Intern. Med. 2007, 21, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.G.; Gomez-Mauricio, G.; Alvarez, V.; Mijares, J.; Tarazona, R.; Bernad, A.; Sanchez-Margallo, F. Comparative phenotypic and molecular characterization of porcine mesenchymal stem cells from different sources for translational studies in a large animal model. Vet. Immunol. Immunopathol. 2012, 147, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.M.; Dow, S.W. Concise Review: Stem Cell Trials Using Companion Animal Disease Models. Stem Cells. 2016, 34, 1709–1729. [Google Scholar] [CrossRef]
- Schneider, N.; Gonçalves, F.C.; Pinto, F.O.; Lopez, P.L.D.C.; Araújo, A.B.; Pfaffenseller, B.; Passos, E.P.; Cirne-Lima, E.O.; Meurer, L.; Lamers, M.L.; et al. Dexamethasone and azathioprine promote cytoskeletal changes and affect mesenchymal stem cell migratory behavior. PLoS ONE 2015, 10, e0120538. [Google Scholar] [CrossRef]
- Peroni, J.F.; Borjesson, D.L. Anti-inflammatory and immunomodulatory activities of stem cells. Vet. Clin. N. Am.—Equine Pract. 2011, 27, 351–362. [Google Scholar] [CrossRef]
- Dandrieux, J.R.S. Inflammatory bowel disease versus chronic enteropathy in dogs: Are they one and the same? J. Small Anim. Pract. 2016, 57, 589–599. [Google Scholar] [CrossRef]
- Khan, N.; Patel, D.; Shah, Y.; Trivedi, C.; Yang, Y.-X. Albumin as a prognostic marker for ulcerative colitis. World J. Gastroenterol. 2017, 23, 8008–8016. [Google Scholar] [CrossRef]
- Craven, M.; Simpson, J.W.; Ridyard, A.E.; Chandler, M.L. Canine inflammatory bowel disease: Retrospective analysis of diagnosis and outcome in 80 cases (1995–2002). J. Small Anim. Pract. 2004, 45, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Kather, S.; Grützner, N.; Kook, P.H.; Dengler, F.; Heilmann, R.M. Review of cobalamin status and disorders of cobalamin metabolism in dogs. J. Vet. Intern. Med. 2020, 34, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Toresson, L.; Steiner, J.M.; Suchodolski, J.S.; Spillmann, T. Oral Cobalamin Supplementation in Dogs with Chronic Enteropathies and Hypocobalaminemia. J. Vet. Intern. Med. 2016, 30, 101–107. [Google Scholar] [CrossRef]
- Sémont, A.; Mouiseddine, M.; François, A.; Demarquay, C.; Mathieu, N.; Chapel, A.; Saché, A.; Thierry, D.; Laloi, P.; Gourmelon, P. Mesenchymal stem cells improve small intestinal integrity through regulation of endogenous epithelial cell homeostasis. Cell Death Differ. 2010, 17, 952–961. [Google Scholar] [CrossRef] [Green Version]
- Misselwitz, B.; Juillerat, P.; Sulz, M.C.; Siegmund, B.; Brand, S. Swiss IBDnet, an official working group of the Swiss Society of Gastroenterology. Emerging Treatment Options in Inflammatory Bowel Disease: Janus Kinases, Stem Cells, and More. Digestion 2020, 101 (Suppl. 1), 69–82. [Google Scholar] [CrossRef] [PubMed]
- Allenspach, K.; Culverwell, C.; Chan, D. Long-term outcome in dogs with chronic enteropathies: 203 cases. Vet. Rec. 2016, 178, 368. [Google Scholar] [CrossRef] [Green Version]
- Hosseini-Asl, S.K.; Mehrabani, D.; Karimi-Busheri, F. Therapeutic Effect of Mesenchymal Stem Cells in Ulcerative Colitis: A Review on Achievements and Challenges. J. Clin. Med. 2020, 9, 3922. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MSC | P-MSC | |
|---|---|---|
| Animals | 19 | 13 |
| Age | 4.18 (1–14) | 5.84 (1–11) |
| Sex (Male/Female) | 12/7 | 7/6 |
| Weight | 13.3 (3–41) | 13.8 (2.2–26.2) |
| MSC GROUP | P-MSC GROUP | p-Value | |
|---|---|---|---|
| CIBDAI | |||
| T0 | 8.21 ± 2.97 | 9.54 ± 3.87 | p = 0.280 |
| T1 | 1.63 ± 1.44 | 4.46 ± 3.24 | p = 0.006 |
| T3 | 1.38 ± 1.31 | 2.44 ± 1.12 | p = 0.035 |
| T6 | 1.38 ± 0.86 | 1.67 ± 0.82 | p = 0.542 |
| T12 | 0.85 ± 0.89 | 1.00 ± 0.00 | p = 0.426 |
| CCECAI | |||
| T0 | 8.90 ± 2.90 | 11.12 ± 3.79 | p = 0.142 |
| T1 | 1.77 ± 1.78 | 5.13 ± 3.92 | p = 0.007 |
| T3 | 1.18 ± 1.33 | 2.94 ± 1.57 | p = 0.017 |
| T6 | 1.56 ± 1.33 | 1.83 ± 0.75 | p = 0.540 |
| T12 | 0.83 ± 0.94 | 1.20 ± 0.45 | p = 0.246 |
| ALBUMIN (g/dL) | |||
| T0 | 3.03 ± 0.81 | 2.29 ± 0.62 | p = 0.010 |
| T1 | 3.21 ± 0.41 | 2.49 ± 0.45 | p < 0.001 |
| T3 | 3.42 ± 0.43 | 2.81 ± 0.51 | p = 0.008 |
| T6 | 3.51 ± 0.27 | 2.98 ± 0.61 | p = 0.024 |
| T12 | 3.60 ± 0.20 | 3.10 ± 0.27 | p = 0.007 |
| COBALAMIN (pg/mL) | |||
| T0 | 271.46 ± 136.72 | 322.86 ± 250.83 | p = 0.954 |
| T1 | 308.76 ± 153.57 | 350.93 ± 250.51 | p = 1.000 |
| T3 | 365.26 ± 83.33 | 424.00 ± 253.56 | p = 0.832 |
| T6 | 446.10 ± 132.42 | 396.68 ± 191.78 | p = 0.286 |
| T12 | 587.84 ± 149.42 | 420.78 ± 163.54 | p = 0.033 |
| PREDNISONE DOSAGE (MG/KG/DAY) | |||
| T0 | 1.60 ± 0.54 | ||
| T1 | 1.19 ± 0.60 | ||
| T3 | 0.46 ± 0.59 | ||
| T6 | 0.15 ± 0.31 | ||
| T12 | 0.00 ± 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristóbal, J.I.; Duque, F.J.; Usón-Casaús, J.M.; Ruiz, P.; Nieto, E.L.; Pérez-Merino, E.M. Effects of Allogeneic Mesenchymal Stem Cell Transplantation in Dogs with Inflammatory Bowel Disease Treated with and without Corticosteroids. Animals 2021, 11, 2061. https://0-doi-org.brum.beds.ac.uk/10.3390/ani11072061
Cristóbal JI, Duque FJ, Usón-Casaús JM, Ruiz P, Nieto EL, Pérez-Merino EM. Effects of Allogeneic Mesenchymal Stem Cell Transplantation in Dogs with Inflammatory Bowel Disease Treated with and without Corticosteroids. Animals. 2021; 11(7):2061. https://0-doi-org.brum.beds.ac.uk/10.3390/ani11072061
Chicago/Turabian StyleCristóbal, José Ignacio, Francisco Javier Duque, Jesús María Usón-Casaús, Patricia Ruiz, Esther López Nieto, and Eva María Pérez-Merino. 2021. "Effects of Allogeneic Mesenchymal Stem Cell Transplantation in Dogs with Inflammatory Bowel Disease Treated with and without Corticosteroids" Animals 11, no. 7: 2061. https://0-doi-org.brum.beds.ac.uk/10.3390/ani11072061