
Implant Removal in the Management of Prosthetic Joint Infection by Staphylococcus aureus: Outcome and Predictors of Failure in a Large Retrospective Multicenter Study


 , , , ,
, , , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Implant Removal as the Initial Surgical Strategy in the Cohort of Acute Prosthetic Joint Infection (PJI)
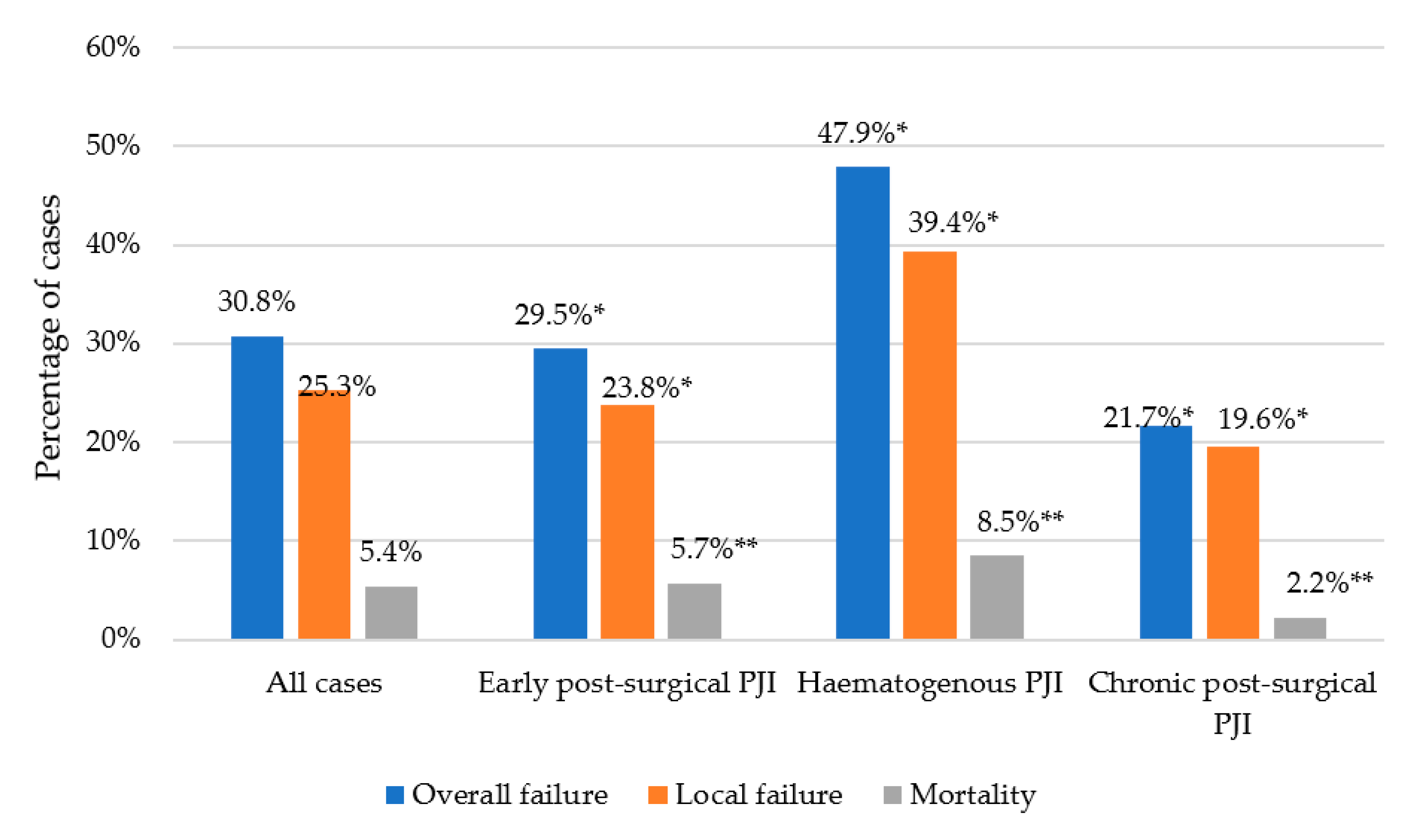
2.2. Cohort of All Cases Managed with Implant Removal (Initially or Salvage Therapy)
3. Discussion
4. Materials and Methods
4.1. Design, Setting, and Patients
4.2. Definitions
4.3. Clinical and Surgical Management
4.4. Outcomes and Follow-Up
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Pozo, J.L.; Patel, R. Clinical practice. Infection associated with prosthetic joints. N. Engl. J. Med. 2009, 361, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benito, N.; Franco, M.; Ribera, A.; Soriano, A.; Rodriguez-Pardo, D.; Sorli, L.; Fresco, G.; Fernandez-Sampedro, M.; Dolores Del Toro, M.; Guio, L.; et al. Time trends in the aetiology of prosthetic joint infections: A multicentre cohort study. Clin. Microbiol. Infect. 2016, 22, 732.e1–732.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-joint infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboltins, C.A.; Page, M.A.; Buising, K.L.; Jenney, A.W.; Daffy, J.R.; Choong, P.F.; Stanley, P.A. Treatment of staphylococcal prosthetic joint infections with debridement, prosthesis retention and oral rifampicin and fusidic acid. Clin. Microbiol. Infect. 2007, 13, 586–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, C.M.; Sistrunk, W.W.; Duffy, M.C.; Hanssen, A.D.; Steckelberg, J.M.; Ilstrup, D.M.; Osmon, D.R. Staphylococcus aureus prosthetic joint infection treated with debridement and prosthesis retention. Clin. Infect. Dis. 1997, 24, 914–919. [Google Scholar] [CrossRef] [Green Version]
- Byren, I.; Bejon, P.; Atkins, B.L.; Angus, B.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Berendt, A. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): Antibiotic duration and outcome. J. Antimicrob. Chemother. 2009, 63, 1264–1271. [Google Scholar] [CrossRef] [Green Version]
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sanchez-Somolinos, M.; Baraia-Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodriguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef] [Green Version]
- Marculescu, C.E.; Berbari, E.F.; Hanssen, A.D.; Steckelberg, J.M.; Harmsen, S.W.; Mandrekar, J.N.; Osmon, D.R. Outcome of prosthetic joint infections treated with debridement and retention of components. Clin. Infect. Dis. 2006, 42, 471–478. [Google Scholar] [CrossRef]
- Brandt, C.M.; Duffy, M.C.; Berbari, E.F.; Hanssen, A.D.; Steckelberg, J.M.; Osmon, D.R. Staphylococcus aureus prosthetic joint infection treated with prosthesis removal and delayed reimplantation arthroplasty. Mayo. Clin. Proc. 1999, 74, 553–558. [Google Scholar] [CrossRef]
- Senneville, E.; Joulie, D.; Legout, L.; Valette, M.; Dezeque, H.; Beltrand, E.; Rosele, B.; d’Escrivan, T.; Loiez, C.; Caillaux, M.; et al. Outcome and predictors of treatment failure in total hip/knee prosthetic joint infections due to Staphylococcus aureus. Clin. Infect. Dis. 2011, 53, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajgopal, A.; Panda, I.; Rao, A.; Dahiya, V.; Gupta, H. Does Prior Failed Debridement Compromise the Outcome of Subsequent Two- Stage Revision Done for Periprosthetic Joint Infection Following Total Knee Arthroplasty? J. Arthroplast. 2018, 33, 2588–2594. [Google Scholar] [CrossRef] [PubMed]
- Sherrell, J.C.; Fehring, T.K.; Odum, S.; Hansen, E.; Zmistowski, B.; Dennos, A.; Kalore, N. The Chitranjan Ranawat Award: Fate of two-stage reimplantation after failed irrigation and debridement for periprosthetic knee infection. Clin. Orthop. Relat. Res. 2011, 469, 18–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Widmer, A.F.; Blatter, M.; Frei, R.; Ochsner, P.E. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: A randomized controlled trial. Foreign-Body Infection (FBI) Study Group. Jama 1998, 279, 1537–1541. [Google Scholar] [CrossRef] [Green Version]
- McPherson, E.J.; Woodson, C.; Holtom, P.; Roidis, N.; Shufelt, C.; Patzakis, M. Periprosthetic total hip infection: Outcomes using a staging system. Clin. Orthop. Relat. Res. 2002, 403, 8–15. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Sebillotte, M.; Lomas, J.; Taylor, A.; Palomares, E.B.; Murillo, O.; Parvizi, J.; Shohat, N.; Reinoso, J.C.; Sanchez, R.E.; et al. Clinical outcome and risk factors for failure in late acute prosthetic joint infections treated with debridement and implant retention. J. Infect. 2019, 78, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Tornero, E.; Morata, L.; Martinez-Pastor, J.C.; Bori, G.; Climent, C.; Garcia-Velez, D.M.; Garcia-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin. Microbiol. Infect. 2015, 21, 786.e9–786.e17. [Google Scholar] [CrossRef] [Green Version]
- Bryan, A.J.; Abdel, M.P.; Sanders, T.L.; Fitzgerald, S.F.; Hanssen, A.D.; Berry, D.J. Irrigation and Debridement with Component Retention for Acute Infection After Hip Arthroplasty: Improved Results with Contemporary Management. J. Bone Joint Surg. Am. 2017, 99, 2011–2018. [Google Scholar] [CrossRef]
- Wimmer, M.D.; Randau, T.M.; Friedrich, M.J.; Ploeger, M.M.; Schmolder, J.; Strauss, A.C.; Pennekamp, P.H.; Vavken, P.; Gravius, S. Outcome Predictors in Prosthetic Joint Infections--Validation of a risk stratification score for Prosthetic Joint Infections in 120 cases. Acta Orthop. Belg. 2016, 82, 143–148. [Google Scholar]
- Amanatullah, D.; Dennis, D.; Oltra, E.G.; Marcelino Gomes, L.S.; Goodman, S.B.; Hamlin, B.; Hansen, E.; Hashemi-Nejad, A.; Holst, D.C.; Komnos, G.; et al. Hip and Knee Section, Diagnosis, Definitions: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S329–S337. [Google Scholar] [CrossRef]
- Gomez-Junyent, J.; Murillo, O.; Grau, I.; Benavent, E.; Ribera, A.; Cabo, X.; Tubau, F.; Ariza, J.; Pallares, R. Analysis of mortality in a cohort of 650 cases of bacteremic osteoarticular infections. Semin. Arthritis Rheum. 2018, 48, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Euba, G.; Ribera, A.; Murillo, O.; Pedrero, S.; Garcia-Somoza, D.; Pujol, M.; Cabo, X.; Ariza, J. Infected hip hemiarthroplasties and total hip arthroplasties: Differential findings and prognosis. J. Infect. 2013, 67, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.C.; Son, M.S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are We Winning or Losing the Battle With Periprosthetic Joint Infection: Trends in Periprosthetic Joint Infection and Mortality Risk for the Medicare Population. J. Arthroplast. 2018, 33, 3238–3245. [Google Scholar] [CrossRef] [PubMed]
- Hart, W.J.; Jones, R.S. Two-stage revision of infected total knee replacements using articulating cement spacers and short-term antibiotic therapy. J. Bone Joint Surg. Br. 2006, 88, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Tibrewal, S.; Malagelada, F.; Jeyaseelan, L.; Posch, F.; Scott, G. Single-stage revision for the infected total knee replacement: Results from a single centre. Bone Joint J. 2014, 96, 759–764. [Google Scholar] [CrossRef]
- Tsukayama, D.T.; Estrada, R.; Gustilo, R.B. Infection after total hip arthroplasty. A study of the treatment of one hundred and six infections. J. Bone Joint Surg. Am. 1996, 78, 512–523. [Google Scholar] [CrossRef]
- Murray, P.R.; Jo Baron, E.; Jorgensen, J.H.; Landry, M.I.; Pfaller, M.A. Manual of Clinical Microbiology, 9th ed.; ASM Press: Washington, DC, USA, 2007. [Google Scholar]
- Chotanaphuti, T.; Courtney, P.M.; Fram, B.; In den Kleef, N.J.; Kim, T.K.; Kuo, F.C.; Lustig, S.; Moojen, D.J.; Nijhof, M.; Oliashirazi, A.; et al. Hip and Knee Section, Treatment, Algorithm: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S393–S397. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Orthopedic Implant-Associated Infections. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier: Philadelphia, PA, USA, 2015; Volume I, pp. 1328–1340. [Google Scholar]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Acute PJI Managed with DAIR (n = 311) | Acute PJI Managed with Implant Removal (n = 89) | p Value | Adjusted OR of Implant Removal (95% CI) * | p Value |
|---|---|---|---|---|---|
| PATIENT CHARACTERISTICS | |||||
| Female sex | 184 (59.2) | 59 (66.3) | 0.225 | ||
| Age (years) 1 | 72 (64–78) | 74 (68–78) | 0.168 | 1.01 (0.99–1.04) | 0.294 |
| Two or more comorbidities 2 | 60 (19.3) | 17 (19.1) | 0.968 | ||
| Chronic kidney disease | 16 (5.1) | 8 (9.0) | 0.178 | ||
| PROSTHESIS CHARACTERISTICS | |||||
| Total hip arthroplasty | 109 (35.1) | 27 (30.3) | 0.408 | ||
| Total knee arthroplasty | 174 (56.0) | 45 (50.6) | 0.368 | ||
| Hemiarthroplasty | 24 (7.7) | 14 (15.7) | 0.023 | 3.73 (1.60–8.68) | 0.003 |
| Revision prosthesis | 53 (17.0) | 14 (15.7) | 0.770 | ||
| CLINICAL AND ANALYTICAL DATA | |||||
| Hematogenous PJI | 49 (15.8) | 26 (29.2) | 0.004 | 3.34 (1.72–6.46) | <0.001 |
| Leukocytosis 3 | 157 (50.5) | 52 (58.4) | 0.186 | ||
| CRP (mg/L) | 109 (28–120) | 100 (30–107) | 0.415 | ||
| Abnormal radiography 4 | 27 (8.7) | 26 (29.2) | <0.001 | 3.70 (1.85–7.43) | <0.001 |
| Duration of symptoms > 21 days | 33 (10.6) | 37 (41.6) | <0.001 | 7.69 (4.03–14.68) | <0.001 |
| Poor condition of soft tissues | 37 (11.9) | 19 (21.4) | 0.023 | 1.50 (0.72–3.12) | 0.282 |
| Infection by MRSA | 75 (24.1) | 34 (38.2) | 0.008 | 1.42 (0.95–3.19) | 0.074 |
| Bacteremia | 57 (18.3) | 17 (19.1) | 0.868 | ||
| Polymicrobial infection | 58 (18.7) | 19 (21.4) | 0.569 | ||
| OUTCOME 5 | |||||
| Overall failure | 107 (35.7) | 20 (23.3) | 0.031 | ||
| Local failure | 94 (31.3) | 9 (10.5) | <0.001 | ||
| Mortality <60 days | 13 (4.3) | 11 (12.8) | 0.004 |
| Acute PJI (Early Post-Surgical and Hematogenous) | Chronic Post-Surgical PJI | |||||
|---|---|---|---|---|---|---|
| Characteristic | IRm as Initial Strategy (n = 89) | IRm as Salvage Therapy (n = 78) | p Value * | IRm as Initial Strategy (n = 72) | IRm as Salvage Therapy (n = 10) | p Value ** |
| Female sex | 59 (66.3) | 52 (66.7) | 0.959 | 46 (63.9) | 7 (70.0) | 0.705 |
| Age (years) | 74 (68–78) | 72 (60–79) | 0.470 | 74 (64–79) | 68 (57–76) | 0.082 |
| Two or more comorbidities 1 | 17 (19.1) | 16 (20.5) | 0.819 | 13 (18.1) | 4 (40.0) | 0.109 |
| Chronic kidney disease | 8 (9.0) | 6 (7.7) | 0.763 | 8 (11.1) | 0 | 0.267 |
| Hemiarthroplasty | 14 (15.7) | 3 (3.9) | 0.011 | 3 (4.2) | 0 | 0.511 |
| Revision prosthesis | 14 (15.7) | 18 (23.1) | 0.229 | 15 (20.8) | 5 (50.0) | 0.044 |
| Infection by MRSA | 34 (38.2) | 16 (20.5) | 0.013 | 12 (16.7) | 3 (30.0) | 0.307 |
| Bacteremia | 9 (10.1) | 4 (5.1) | 0.230 | 1 (1.4) | 0 | 0.708 |
| Polymicrobial infection | 19 (21.4) | 20 (25.6) | 0.513 | 20 (27.8) | 2 (20.0) | 0.603 |
| OUTCOME 2 | ||||||
| Overall failure | 20 (23.3) | 9 (12.0) | 0.064 | 6 (9.0) | 2 (22.2) | 0.223 |
| Local failure | 9 (10.5) | 7 (9.3) | 0.811 | 4 (6.0) | 2 (22.2) | 0.090 |
| Mortality < 60 days | 11 (12.8) | 2 (2.7) | 0.019 | 2 (3.0) | 0 | 0.599 |
| Characteristic | Failed/Total (%) | Crude HR (95%CI) | p Value | Adjusted HR (95% CI) | p Value | |
|---|---|---|---|---|---|---|
| Age | <75 years | 15/127 (11.8) | 1 | 1 | ||
| ≥75 years | 7/110 (6.4) | 0.59 (0.24–1.44) | 0.234 | 0.59 (0.24–1.44) | 0.231 | |
| Sex | Male | 9/80 (11.3) | 1 | |||
| Female | 13/157 (8.3) | 0.67 (0.29–1.57) | 0.364 | |||
| Two or more comorbidities 1 | No | 15/192 (7.8) | 1 | 1 | ||
| Yes | 7/45 (15.6) | 2.44 (0.99–5.99) | 0.051 | 2.46 (1.00–6.09) | 0.051 | |
| Hemiarthroplasty | No | 21/218 (9.6) | 1 | |||
| Yes | 1/19 (5.3) | 0.87 (0.12–6.50) | 0.891 | |||
| Revision prosthesis | No | 15/185 (8.1) | 1 | |||
| Yes | 7/52 (13.5) | 1.77 (0.72–4.37) | 0.232 | |||
| Hematogenous PJI | No | 18/193 (9.3) | 1 | |||
| Yes | 4/44 (9.1) | 0.93 (0.31–2.75) | 0.891 | |||
| Infection by MRSA | No | 18/179 (10.1) | 1 | |||
| Yes | 4/58 (6.9) | 0.87 (0.29–2.57) | 0.798 | |||
| Bacteremia | No | 21/223 (9.4) | 1 | |||
| Yes | 1/14 (7.1) | 1.76 (0.23–13.32) | 0.613 | |||
| Polymicrobial infection | No | 19/178 (10.7) | 1 | |||
| Yes | 3/59 (5.1) | 0.51 (0.15–1.71) | 0.236 | |||
| Initially managed with DAIR | No | 13/153 (8.5) | 1 | 1 | ||
| Yes | 9/84 (10.7) | 1.06 (0.45–2.49) | 0.886 | 0.94 (0.40–2.23) | 0.897 | |
| Surgical management | One-stage exchange | 2/16 (12.5) | 1 | |||
| Two-stage exchange | 16/182 (8.8) | 0.60 (0.14–2.62) | ||||
| Hip resection arthroplasty | 4/39 (10.3) | 0.84 (0.15–4.61) | 0.720 | |||
| Rifampin 2 | No | 7/96 (7.3) | 1 | |||
| Yes | 12/119 (10.1) | 1.01 (0.37–2.73) | 0.989 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Junyent, J.; Lora-Tamayo, J.; Baraia-Etxaburu, J.; Sánchez-Somolinos, M.; Iribarren, J.A.; Rodriguez-Pardo, D.; Praena-Segovia, J.; Sorlí, L.; Bahamonde, A.; Riera, M.; et al. Implant Removal in the Management of Prosthetic Joint Infection by Staphylococcus aureus: Outcome and Predictors of Failure in a Large Retrospective Multicenter Study. Antibiotics 2021, 10, 118. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020118
Gómez-Junyent J, Lora-Tamayo J, Baraia-Etxaburu J, Sánchez-Somolinos M, Iribarren JA, Rodriguez-Pardo D, Praena-Segovia J, Sorlí L, Bahamonde A, Riera M, et al. Implant Removal in the Management of Prosthetic Joint Infection by Staphylococcus aureus: Outcome and Predictors of Failure in a Large Retrospective Multicenter Study. Antibiotics. 2021; 10(2):118. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020118
Chicago/Turabian StyleGómez-Junyent, Joan, Jaime Lora-Tamayo, Josu Baraia-Etxaburu, Mar Sánchez-Somolinos, Jose Antonio Iribarren, Dolors Rodriguez-Pardo, Julia Praena-Segovia, Luisa Sorlí, Alberto Bahamonde, Melchor Riera, and et al. 2021. "Implant Removal in the Management of Prosthetic Joint Infection by Staphylococcus aureus: Outcome and Predictors of Failure in a Large Retrospective Multicenter Study" Antibiotics 10, no. 2: 118. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10020118