
The General Population’s Inappropriate Behaviors and Misunderstanding of Antibiotic Use in China: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
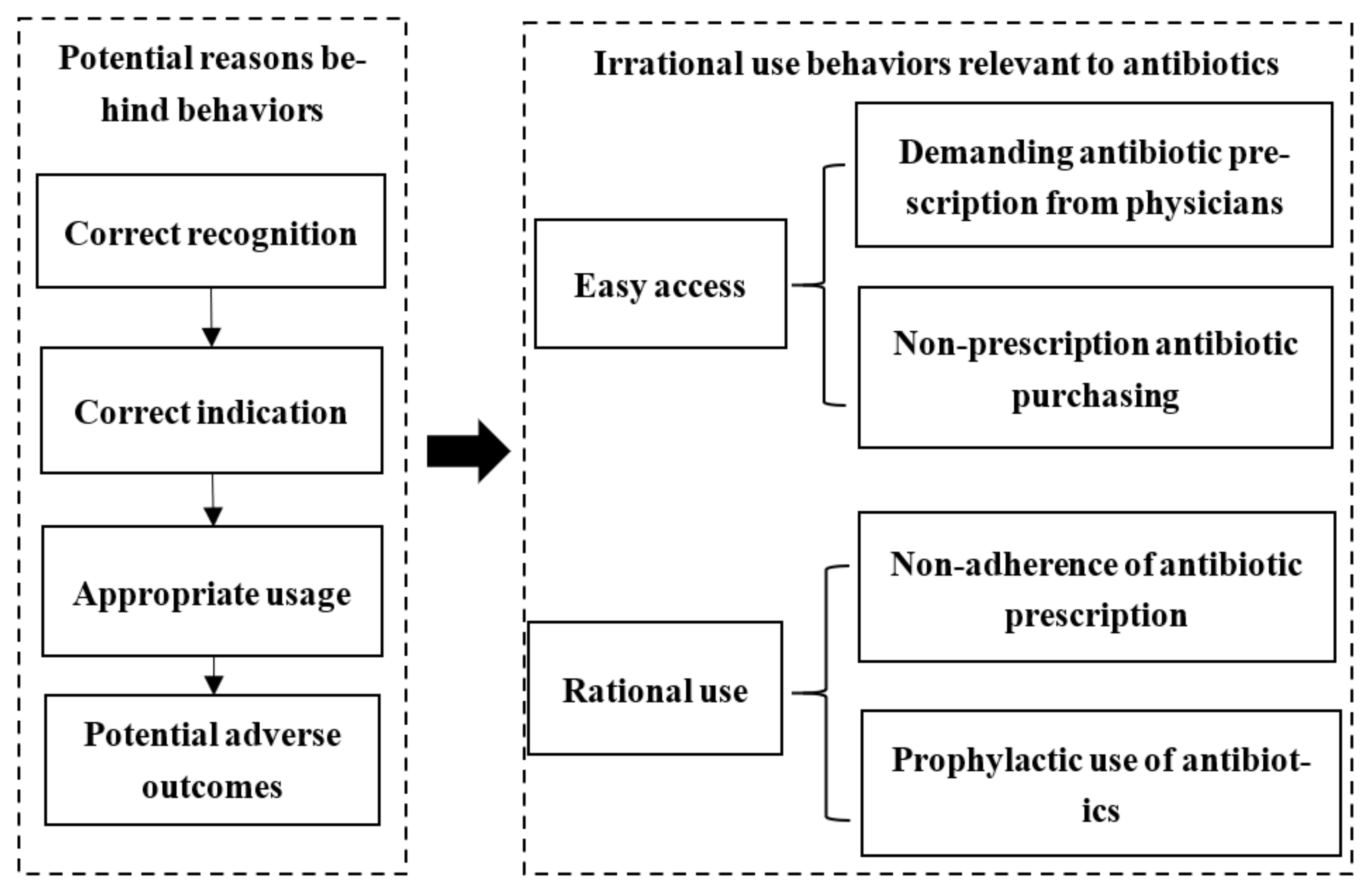
2.1. Review Framework
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Quality Assessment
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
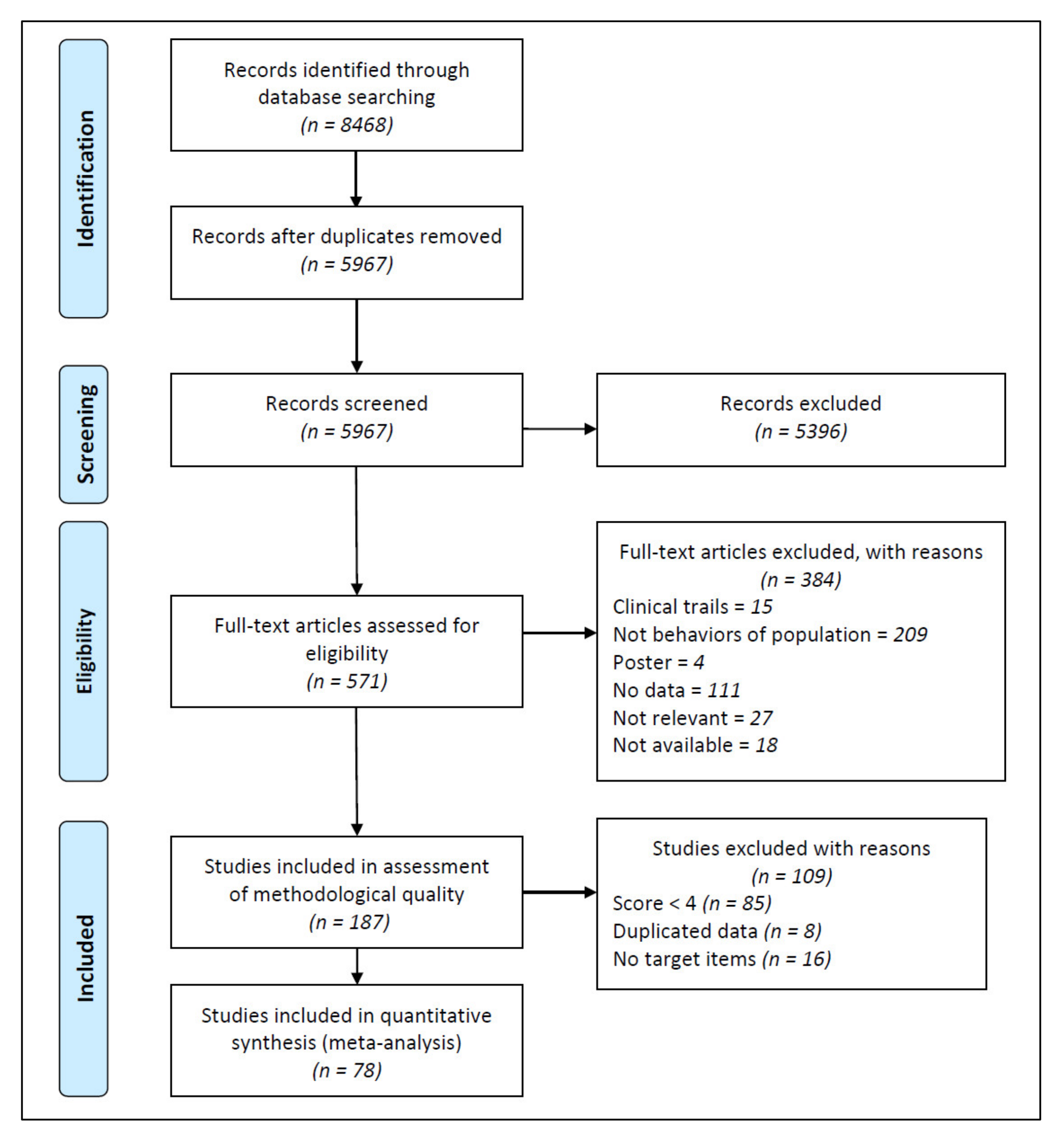
3.1. Study Selection and Characteristics
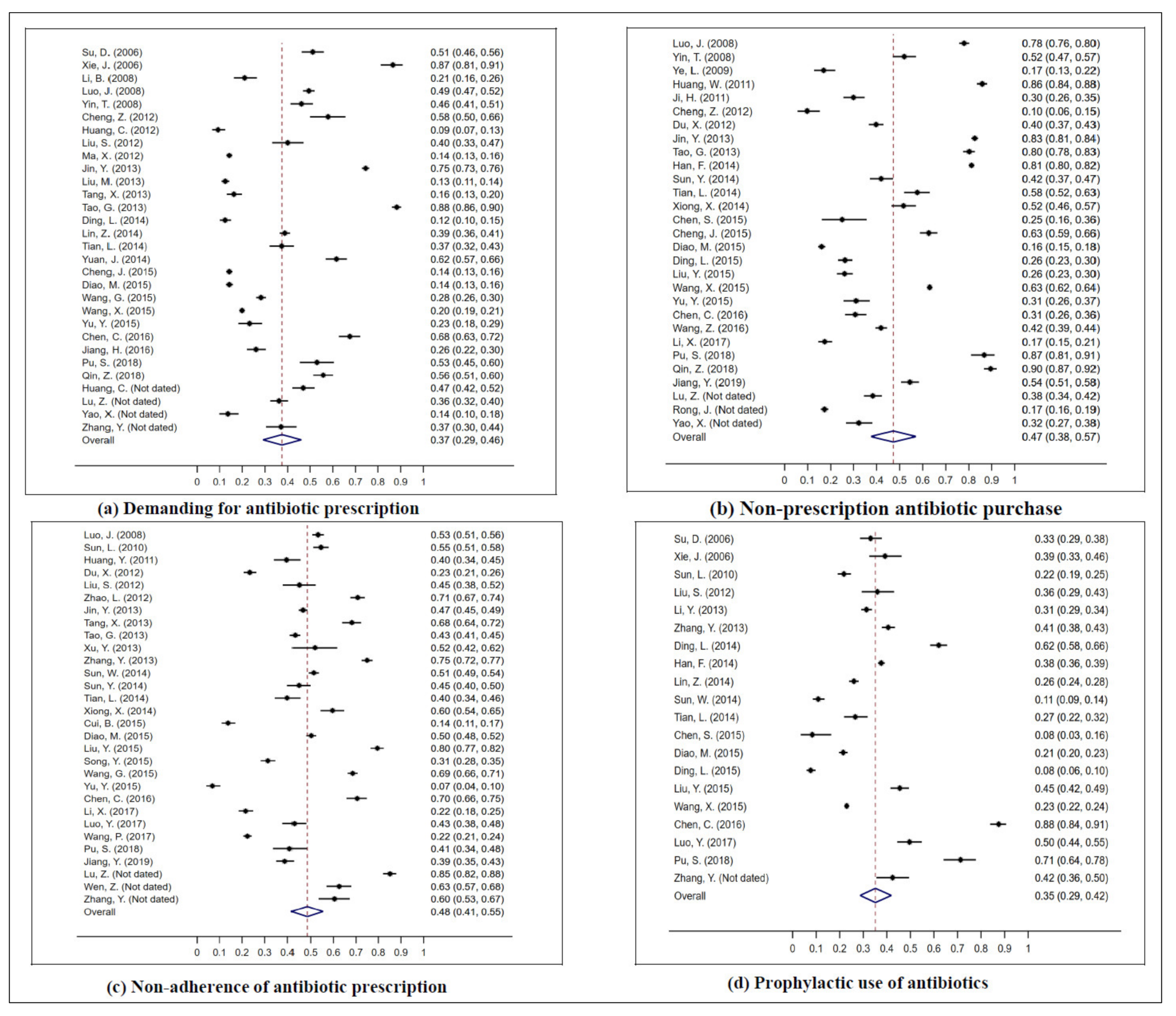
3.2. The Prevalence of Irrational Use Behaviors of the General Population
3.2.1. Demanding Antibiotic Prescription
3.2.2. Non–Prescription Antibiotic Purchasing
3.2.3. Non–Adherence to Antibiotic Prescription
3.2.4. Prophylactic Use of Antibiotics
3.2.5. Sensitivity Analysis
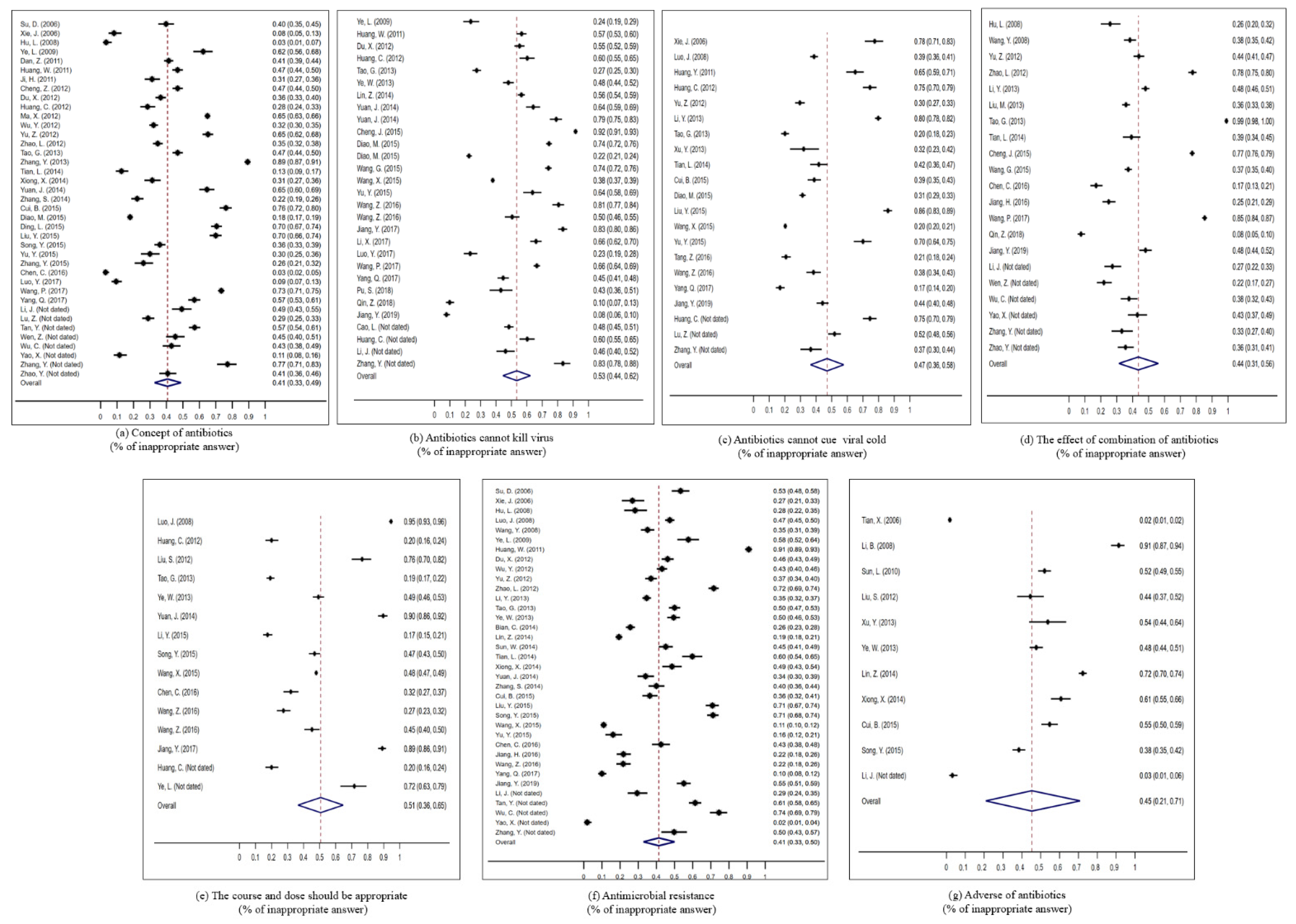
3.3. Prevalence of Potential Reasons of the General Population’s Irrational Use of Antibiotics
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Comparison with Existing Studies
4.4. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. JBI Critical Appraisal Checklist for Studies Reporting Prevalence Data
| Heading | Yes | No | Unclear | Not Applicable |
| 1. Was the sample frame appropriate to address the target population? | ? | ? | ? | ? |
| 2. Were study participants sampled in an appropriate way? | ? | ? | ? | ? |
| 3. Was the sample size adequate? | ? | ? | ? | ? |
| 4. Were the study subjects and the setting described in detail? | ? | ? | ? | ? |
| 5. Was the data analysis conducted with sufficient coverage of the identified sample? | ? | ? | ? | ? |
| 6. Were valid methods used for the identification of the condition? | ? | ? | ? | ? |
| 7. Was the condition measured in a standard, reliable way for all participants? | ? | ? | ? | ? |
| 8. Was there appropriate statistical analysis? | ? | ? | ? | ? |
| 9. Was the response rate adequate, and if not, was the low response rate managed appropriately? | ? | ? | ? | ? |
- Was the sample frame appropriate to address the target population? The sampling frame should match with the purpose of the study, and can obtain the target population of the study;
- Were study participants sampled in an appropriate way? It is necessary to describe in detail what sampling method was used and how to gradually obtain our target population. For cluster and stratified sampling, you should describe the characteristics according to which participants are stratified and grouped. Non–probability sampling is not considered an appropriate survey research method;
- Was the sample size adequate? In addition to a comprehensive census, a detailed and reasonable sample size calculation process is required for sample surveys;
- Were the study subjects and the setting described in detail? The characteristics of the participants need to be described in detail, and demographic information, research time and research location need to be included at the same time;
- Was the data analysis conducted with sufficient coverage of the identified sample? It is necessary to describe whether the samples can adequately cover the structure of each subgroup;
- Were valid methods used for the identification of the condition? While using a self–made questionnaire as measurement tool, the reliability and validity test results of the questionnaire need to be provided; if a certain established standard or definition is applied in the research, its standard and source should be introduced in detail;
- Was the condition measured in a standard, reliable way for all participants? Introduce whether the questionnaire surveyor has been uniformly trained, and introduce the content of the uniform training, or describe in detail the distribution and quality control process of the questionnaire in the data collection process;
- Was there appropriate statistical analysis? The rate index should give the numerator, denominator, and rate with confidence interval;
- Was the response rate adequate, and if not, was the low response rate managed appropriately? The response rate of the research needs to be given. Generally, the response rate is >70%. If the response rate is less than 70%, the response rate is too low. The research needs to provide solutions for the response rate.
Appendix B. Data Extraction Form for Prevalence Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation Details | ||||||
|---|---|---|---|---|---|---|
| Author | Title | Journal | Year | Issue | Volume | Pages |
| Generic Study Details | ||||||
| Study Design | Country | Setting/Context | Year/Timeframe for Data Collection | Participants Characteristic (Study Inclusion/Exclusion Information) | Condition and Measurement | Description of Main Result (n/N) |
References
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Watkins, R.R.; Bonomo, R.A. Overview: Global and Local Impact of Antibiotic Resistance. Infect. Dis. Clin. N. Am. 2016, 30, 313–322. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance Global Report on Surveillance: 2014 Summary; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- O’neill, J. Review on Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; HM Government: London, UK, 2016. [Google Scholar]
- Zhen, X.; Lundborg, C.S.; Sun, X.; Hu, X.; Dong, H. The Clinical and Economic Impact of Antibiotic Resistance in China: A Systematic Review and Meta–Analysis. Antibiotics 2019, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhen, X.; Stålsby Lundborg, C.; Sun, X.; Zhu, N.; Gu, S.; Dong, H. Economic burden of antibiotic resistance in China: A national level estimate for inpatients. Antimicrob. Resist. Infect. Control 2021, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- The Role of Antimicrobial Use in the Epidemiology of Resistant Pneumococci: A 10–Year Follow Up. Microb. Drug Resist. 2006, 12, 169–176. [CrossRef]
- Bronzwaer, S.L.; Cars, O.; Buchholz, U.; Mölstad, S.; Goettsch, W.; Veldhuijzen, I.K.; Kool, J.L.; Sprenger, M.J.; Degener, J.E. A European study on the relationship between antimicrobial use and antimicrobial resistance. Emerg. Infect. Dis. 2002, 8, 278–282. [Google Scholar] [CrossRef]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: A cross–national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, X.; Tucker, J.D.; Little, P.; Moore, M.; Fukuda, K.; Zhou, X. Knowledge, Attitude, and Practice with Respect to Antibiotic Use among Chinese Medical Students: A Multicentre Cross–Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1165. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Lin, L.; Xuan, Z.; Li, L.; Zhou, X. Keeping Antibiotics at Home Promotes Self–Medication with Antibiotics among Chinese University Students. Int. J. Environ. Res. Public Health 2018, 15, 687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljayyousi, G.F.; Abdel–Rahman, M.E.; El–Heneidy, A.; Kurdi, R.; Faisal, E. Public practices on antibiotic use: A cross–sectional study among Qatar University students and their family members. PLoS ONE 2019, 14, e0225499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigoryan, L.; Burgerhof, J.G.; Haaijer–Ruskamp, F.M.; Degener, J.E.; Deschepper, R.; Monnet, D.L.; Di Matteo, A.; Scicluna, E.A.; Bara, A.C.; Lundborg, C.S.; et al. Is self–medication with antibiotics in Europe driven by prescribed use? J. Antimicrob. Chemother. 2007, 59, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Lv, B.; Zhou, Z.; Xu, G.; Yang, D.; Wu, L.; Shen, Q.; Jiang, M.; Wang, X.; Zhao, G.; Yang, S.; et al. Knowledge, attitudes and practices concerning self–medication with antibiotics among university students in western China. Trop. Med. Int. Health Tm Ih 2014, 19, 769–779. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance. Available online: https://www.who.int/news–room/fact–sheets/detail/antibiotic–resistance (accessed on 23 February 2021).
- Macfarlane, J.; Holmes, W.; Macfarlane, R.; Britten, N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: Questionnaire study. BMJ 1997, 315, 1211–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, J.G.; Cohen, D.; DiCicco–Bloom, B.; Orzano, A.J.; Jaen, C.R.; Crabtree, B.F. Antibiotic use in acute respiratory infections and the ways patients pressure physicians for a prescription. J. Fam. Pract. 2001, 50, 853–858. [Google Scholar]
- Liu, C.; Liu, C.; Wang, D.; Deng, Z.; Tang, Y.; Zhang, X. Determinants of antibiotic prescribing behaviors of primary care physicians in Hubei of China: A structural equation model based on the theory of planned behavior. Antimicrob. Resist. Infect. Control 2019, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Mangione–Smith, R.; McGlynn, E.A.; Elliott, M.N.; Krogstad, P.; Brook, R.H. The relationship between perceived parental expectations and pediatrician antimicrobial prescribing behavior. Pediatrics 1999, 103, 711–718. [Google Scholar] [CrossRef]
- Francois Watkins, L.K.; Sanchez, G.V.; Albert, A.P.; Roberts, R.M.; Hicks, L.A. Knowledge and Attitudes Regarding Antibiotic Use Among Adult Consumers, Adult Hispanic Consumers, and Health Care Providers—United States, 2012–2013. Morb. Mortal. Wkly. Rep. 2015, 64, 767–770. [Google Scholar] [CrossRef] [Green Version]
- Dyar, O.J.; Zhang, T.; Peng, Y.; Sun, M.; Sun, C.; Yin, J.; Ding, L.; Sun, C.; Wang, Y.; Sun, Q.; et al. Knowledge, attitudes and practices relating to antibiotic use and antibiotic resistance among backyard pig farmers in rural Shandong province, China. Prev. Vet. Med. 2020, 175, 104858. [Google Scholar] [CrossRef]
- Wang, J.; Sheng, Y.; Ni, J.; Zhu, J.; Zhou, Z.; Liu, T.; Zhang, X.; Zhao, Q. Shanghai Parents’ Perception And Attitude Towards The Use Of Antibiotics On Children: A Cross–Sectional Study. Infect. Drug Resist. 2019, 12, 3259–3267. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Hu, Y.; Zou, G.; Lin, M.; Zeng, J.; Deng, S.; Zachariah, R.; Walley, J.; Tucker, J.D.; Wei, X. Antibiotic prescribing for upper respiratory infections among children in rural China: A cross–sectional study of outpatient prescriptions. Glob. Health Action 2017, 10, 1287334. [Google Scholar] [CrossRef] [Green Version]
- Nepal, G.; Bhatta, S. Self–medication with Antibiotics in WHO Southeast Asian Region: A Systematic Review. Cureus 2018, 10, e2428. [Google Scholar] [CrossRef] [Green Version]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu–Aguye, S.N.; Adeloye, D.; Strickland–Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta–analysis. J. Infect 2019, 78, 8–18. [Google Scholar] [CrossRef]
- Kianmehr, H.; Sabounchi, N.S.; Seyedzadeh Sabounchi, S.; Cosler, L.E. Patient expectation trends on receiving antibiotic prescriptions for respiratory tract infections: A systematic review and meta–regression analysis. Int. J. Clin. Pract. 2019, 73, e13360. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.; Nichols, T.; French, D.P.; Joshi, P.; Butler, C.C. Expectations for consultations and antibiotics for respiratory tract infection in primary care: The RTI clinical iceberg. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2013, 63, e429–e436. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Wei, L.; Li, H.; Zhang, M.; Cao, B.; Bian, J.; Zhan, S. Appropriateness of antibiotic prescriptions in ambulatory care in China: A nationwide descriptive database study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Wang, X.; Peng, D.; Wang, W.; Xu, Y.; Zhou, X.; Hesketh, T. Massive misuse of antibiotics by university students in all regions of China: Implications for national policy. Int. J. Antimicrob. Agents 2017, 50, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Xuan, Z.; Storella, T.H.; Zhou, X. Determinants of non–prescription antibiotic dispensing in Chinese community pharmacies from socio–ecological and health system perspectives. Soc. Sci. Med. 2020, 256, 113035. [Google Scholar] [CrossRef]
- Lin, L.; Sun, R.; Yao, T.; Zhou, X.; Harbarth, S. Factors influencing inappropriate use of antibiotics in outpatient and community settings in China: A mixed–methods systematic review. BMJ Glob. Health 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Systematic reviews of prevalence and incidence. Joanna Briggs Inst. Rev. Man. 2017, 5, 177–217. [Google Scholar]
- Xu, Y.; Lu, J.; Sun, C.; Wang, X.; Hu, Y.J.; Zhou, X. A cross–sectional study of antibiotic misuse among Chinese children in developed and less developed provinces. J. Infect. Dev. Ctries. 2020, 14, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Monnier, A.A.; Eisenstein, B.I.; Hulscher, M.E.; Gyssens, I.C. Towards a global definition of responsible antibiotic use: Results of an international multidisciplinary consensus procedure. J. Antimicrob. Chemother. 2018, 73, vi3–vi16. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Behzadifar, M.; Heydarvand, S.; Behzadifar, M.; Bragazzi, N.L. Prevalence of Hepatitis C Virus in Tuberculosis Patients: A Systematic Review and Meta–Analysis. Ethiop. J. Health Sci. 2019, 29, 945–956. [Google Scholar] [CrossRef]
- Tian, X.; Tang, X.; Li, J. Cognition status about side effect antibiotics among staff members and students in one college. Chin. Sch. Health 2010, 31, 216–217. (In Chinese) [Google Scholar] [CrossRef]
- Su, D.; Zhang, X.; Wang, L. Evaluation of the pilot effect of health education on the control of antibiotic abuse in rural communities in Zhejiang. Chin. Rural Health Serv. Manag. 2010, 30, 296–298. (In Chinese) [Google Scholar]
- Xie, J.; Yang, T.; He, Y. Evaluation on the effectiveness of antimicrobial abuse publicity interventions among residents in Xiacheng District, Hangzhou. Zhejiang Prev. Med. 2009, 3. (In Chinese) [Google Scholar] [CrossRef]
- Luo, J. Study on self–medication behaviors and influencing factors of antimicrobial drugs among pharmacies customers. Master’s Thesis, Central South University, Changsha, China, 2009. (In Chinese). [Google Scholar]
- Yin, T. Social epidemiological study on the use of antibiotics among community residents in Changsha. Ph.D. Thesis, Central South University, Changsha, China, 2010. (In Chinese). [Google Scholar]
- Hu, L. Study on anitbiotic use in urban population in Ningbo city. China Health Educ. 2010, 26, 127–128. (In Chinese) [Google Scholar] [CrossRef]
- Wang, Y.; Zou, D. Analysis of cognitive behaviors of community residents toward the antimicrobial use. J. Pharmacoepidemiol. 2010, 19, 498–500. (In Chinese) [Google Scholar]
- Li, B.; Wen, Q.; Deng, L.; Chen, Z. Investigation and analysis of antibiotic–related knowledge of parents of children with children in the pediatric infusion room. J. Yangtze Univ. (Self Sci. Ed.) Med. Vol. 2009, 6, 323–325. (In Chinese) [Google Scholar] [CrossRef]
- Ye, L.; Hu, Z. A survey of the cognition and use of antibiotics in patients in the Department of Infectious Diseases. Chin. J. Mod. Nurs. 2010, 33, 4028–4029. (In Chinese) [Google Scholar]
- Sun, L.; Peng, L.; Cai, F. Cognition of antibiotic and its intervention among staff and students in a vocational college. Chin. Sch. Dr. 2011, 25, 576–577. (In Chinese) [Google Scholar]
- Huang, W.; Liao, J.; He, J. A survey of Lanzhou uppperrespiratory tract infectious patients’ knoledge on antibiotics and its usage out hospital. Gansu Med. 2013, 32, 9–12. (In Chinese) [Google Scholar] [CrossRef]
- Huang, Y.; Zhang, H.; Qian, K. Investigation on the awareness and use of antibiotics among community residents. Community Med. J. 2013, 11, 52–54. (In Chinese) [Google Scholar]
- Ji, H.; Li, D.; Li, P. Suevey on drug use related knowledge and behaviors among Xianyang City of Shaanxi Province in 2011. China Health Educ. 2014, 30, 694–697. (In Chinese) [Google Scholar] [CrossRef]
- Shan, H.; Fan, M.; Mao, F. Investigation on the status quo of antibacterial drug use in outpatients. Pharm. Clin. Res. 2013, 21, 90–93. (In Chinese) [Google Scholar] [CrossRef]
- Huang, C.; Jin, Y. Survey of the knowledge and behavior for rational use of antibiotics in Huating Town, Jiading district, Shanhai. Shanghai Med. 2013, 4, 33–35. (In Chinese) [Google Scholar]
- Cheng, S.; Shi, L.; Luo, X. Investigation and analysis of rational use of antibiotics in the community residents of Beijing. China Pharm. 2013, 24, 3758–3760. (In Chinese) [Google Scholar] [CrossRef]
- Zhao, L.; Sun, Q.; Li, C. Antibiotcs in rural Shandong province: User cognition and behavior. China Health Policy Res. 2013, 6, 43–47. (In Chinese) [Google Scholar] [CrossRef]
- Wu, Y.; Nan, H.; Tie, Y. Analysis on rational use of drugs situation among urban and rural residents in Shaanxi Province. China Health Educ. 2015, 31, 289–292. (In Chinese) [Google Scholar] [CrossRef]
- Ma, X.; Yin, W.; Wei, Y. Investigation and analysis of current situation of the cognition of residents and use of antibacterials in Shandong Province under National Essential Drug System. China Pharm. 2014, 25, 1066–1069. (In Chinese) [Google Scholar] [CrossRef]
- Yu, M. Utilization of Antibiotics and the Influencing Factors in Rural Areas of Jiangxi Province. Master’s Thesis, Fudan University, Shanghai, China, 2013. (In Chinese). [Google Scholar]
- Liu, S.; Gu, W.; Shen, Q. The survey of the resident’s knowledge attitudes and practice for antimicrobial medicaiton in Minhang District of Shanghai. Community Med. J. 2016, 14, 7–10. (In Chinese) [Google Scholar]
- Du, X.; Sun, Y.; Kang, M. A survey of College Students’ awareness of antibacterial drugs. Chin. Prim. Med. 2014, 21, 650–652. (In Chinese) [Google Scholar]
- Tao, G. Investigation and analysis of effect of health education intervention on the knowledge–belief–behavior level of the rational use of antibiotics by community residents. China Pharm. 2015, 26, 3751–3754. (In Chinese) [Google Scholar] [CrossRef]
- Li, Y. Investigation on cognition and judgment of present applicantion situation antibiotics in the medical students. J. Qiqihar Med. Coll. 2016, 37, 3944–3946. (In Chinese) [Google Scholar]
- Jin, Y.; Lu, Y.; Lu, P. Influence of demographic characteristics on antibiotics use among middle aged and elderly people. Chin. Public Health 2014, 30, 1140–1143. (In Chinese) [Google Scholar] [CrossRef]
- Ye, W.; Xuan, R.; Ye, P. An empirical study on the assessment and influencing factors of the status quo of cognition and medication behavior of antibacterial drugs among residents in Dongguan. China Pract. Med. 2014, 9, 195–196. (In Chinese) [Google Scholar] [CrossRef]
- Tang, X.; Zhang, Y. Investigation on the knowledge, belief and practice of the rational use of antibacterial drugs in outpatients. Jiangsu Prev. Med. 2015, 26, 122–123. (In Chinese) [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, Q. A survey on the cognition of antibacterial drugs among college students. Chin. J. Drug Abus. Prev. Treat. 2014, 20, 215–216. (In Chinese) [Google Scholar] [CrossRef]
- Xu, Y.; Lu, S.; Zou, X. Investigation and analysis of the cognition and use of antibacterial drugs among residents in a certain community in Shanghai. Community Med. J. 2013, 111, 80–82. (In Chinese) [Google Scholar]
- Liu, M.; Zhang, X.; Gao, X. Investigation and analysis of 1046 children’s parents on antibacterial drugs–related cognition and behavior. China Healthc. Nutr. 2016, 26, 7–8. (In Chinese) [Google Scholar] [CrossRef]
- Sun, W. The impact evaluation of health promotion on improving rational use of antibiotics among rural children caregiver. Master’s Thesis, Shandong University, Jinan, China, 2015. (In Chinese). [Google Scholar]
- Ding, L.; Sun, W.; Li, Y. Knowledge, attitude and practice about antibiotic use among caregivers of rural preschool children. Chin. Public Health 2015, 31, 1109–1112. (In Chinese) [Google Scholar] [CrossRef]
- Tian, L.; Peng, L. Evaluation on the intervention effect of antibiotics in Dongli District of Tianjin. China Urban Rural Enterp. Health 2017, 32, 13–15. (In Chinese) [Google Scholar] [CrossRef]
- Han, F. Survey on the Present Knowledge and Use of Antibiotic of Suzhou Secondary Vocaitonal Students. Master’s Thesis, Anhui Medical University, Hefei, China, 2015. (In Chinese). [Google Scholar]
- Yuan, J. Knowledge, Attitude and Practice towards Antibiotcs Usage—A Cross Sectional Survey Amnog the Genernal Public in Luquan County, Yunnan Province. Master’s Thesis, Kunming Medical University, Kunming, China, 2016. (In Chinese). [Google Scholar]
- Bian, C.; Wang, H.; Wu, J. Analysis of influencing factors on the awareness of antimicrobial resistance and preference in outpatients among second–tier hospitals in Anhui Province. Chin. J. Dis. Control 2015, 19, 847–848. (In Chinese) [Google Scholar] [CrossRef]
- Zhang, S.; Shao, C.; Wu, H. Investigation and analysis on the cognition and safe use of antibiotics among residents in Henan Province. Sci. Technol. Econ. Trib. 2015, 16, 125–126. (In Chinese) [Google Scholar]
- Xiong, X.; Xiao, X.; Fan, Y. Investigation of congnition and utilization situation of antibiotics among residents inWeifang. Community Med. J. 2015, 13, 1–4. (In Chinese) [Google Scholar]
- Lin, W.; Jin, H.; Wu, L. Cognition and attitude of community residents on anitbiotics and its usage status. Chin. Gen. Pract. 2015, 18, 3491–3495. (In Chinese) [Google Scholar] [CrossRef]
- Sun, Y.; Zhu, X.; Fang, C. The cognition of college students on oral antibiotics. Front. Med. 2015, 5, 31–32. (In Chinese) [Google Scholar]
- Liu, Y. The research on the evauation about effect of intervention to promote the irrationla use of antibiotics of rural residents inShandong province. Master’s Thesis, Shandong University, Jinan, China, 2018. (In Chinese). [Google Scholar]
- Diao, M. Analysis of Antibacterial Drug Use by Rural Residents in Anhui Province. J. Nanjing Med Univ. (Soc. Sci. Ed.) 2017, 17, 462–466. (In Chinese) [Google Scholar] [CrossRef]
- Chen, S.; Zhao, G.; Xia, B. Investigation for the knowledge of drug use among and medication habits of teachers in a senior high school in Beijing. China Pharm. 2016, 27, 4187–4190. (In Chinese) [Google Scholar] [CrossRef]
- Wang, X. Antibiotic related knowledge and behaviors:A cross–sectional study and Ron campaign among Chinese university students. Ph.D. Thesis, Zhejiang University, Hangzhou, China, 2018. (In Chinese). [Google Scholar]
- Cheng, J. Antibiotics Use in Rural Areas and Piloting Intervention for Rational antibiotics use based on Plannede Behavior Theory. Ph.D. Thesis, Anhui Medical University, Hefei, China, 2017. (In Chinese). [Google Scholar]
- Zhang, Y.; Lin, S.; Li, G. Congnition and usage of antibiotics in caregivers of 0–6 years old children in rural area of Weinan, 2015. Pract. Prev. Med. 2017, 24, 196–198. (In Chinese) [Google Scholar] [CrossRef]
- Song, Y. Analysis of unreasonable use of antibacterial drugs for college students and countermeasures. J. Clin. Ration. Use Drugs 2016, 9, 86–87. [Google Scholar] [CrossRef]
- Cui, B. Investigation on congnition status of antibacterial agents among freshmen in a university. Chin. Sch. Dr. 2018, 32, 561–563. (In Chinese) [Google Scholar]
- Ding, L. A Study on Rural Residents’ baseline knowledge, attitudes, and practice of antibiotics–a case from a county in Shandong province. Master’s Thesis, Shandong University, Jinan, China, 2016. (In Chinese). [Google Scholar]
- Wang, G.; Gao, H.; Yan, J. Knowledge and behavior about antibiotics use in adult community residents in Tianjin between 20 and 69 years old. Chin. Public Health 2017, 33, 407–411. (In Chinese) [Google Scholar] [CrossRef]
- Yu, Y.; Zhao, Y.; Wang, X. Cognition status quo of residents toward antibiotics in community in Tianjin city and analysis of its influencing factors. Nurs. Res. 2016, 30, 3403–3406. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2016&filename=SXHZ201627029&v=ufUEvZiz8f1%25mmd2BvxdnLEbH2R3UhcGlK7SWaFUfv02NvQsQ8tm5lZ5u2wcbZS%25mmd2FvpOSt (accessed on 22 April 2021). (In Chinese). [CrossRef]
- Lei, Z.; Xu, Y.; Guo, Q. An investigation of antibacterial medicine use in the communities of Changsha. Guangdong Chem. Ind. 2016, 43, 20–21. (In Chinese) [Google Scholar]
- Chen, C.; Wang, G.; Gao, H. Knowledge and behaviors of antibiotic and its influencing factors among civil servants in Tianjin (In Chinese). Occup. Health 2018, 34, 622–626. [Google Scholar] [CrossRef]
- Tang, Z.; Tang, J.; Su, Q. Investigation and Analysis on Cognition Degree of the Children Patients’ Parents on Common Cold and Its Medication Safety. China Pharm. 2018, 27, 78–81. (In Chinese) [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; Huang, X. Relationship between cognition on and attitudes towards antibiotic use among citizens in Hangzhou city. Chin. Public Health 2018, 34, 882–886. (In Chinese) [Google Scholar] [CrossRef]
- Jiang, H.; Jin, Y.; Ye, J. An analysis on knowledge, attitude and practice regarding antibiotics use among community residents in Hangzhou. Prev. Med. 2017, 29, 978–982. (In Chinese) [Google Scholar] [CrossRef]
- Wang, Q.; Wang, X.; Kang, C. Investigation on Use of Antibacterial Drugs among College Students in the City of Chengdu. Chin. Pharmacovigil. 2017, 14, 493–497. (In Chinese) [Google Scholar]
- Jiang, Y.; Zhang, F.; Yan, H. Congnition of antibiotics and its influence factors among residens in Xuzhou after the implementation of antimicrobial agents use. Prev. Med. Forum 2018, 24, 483–486. (In Chinese) [Google Scholar] [CrossRef]
- Luo, Y.; Li, H.; Deng, R. Antibiotic use knowledge, attitude and behavior of nursing students with different academic levels. Guangxi Med. 2019, 41, 141–145. (In Chinese) [Google Scholar] [CrossRef]
- Yang, Q. A Study on the Rational Use of Antibiotics and Its Influential Factors in Children’s Parents in Xiacheng District. Master’s Thesis, Zhejiang University, Hangzhou, China, 2018. (In Chinese). [Google Scholar]
- Wang, P.; Li, Y.; Bai, J. Cognition, use and education demand of antibiotics among college students in 5 universities in China. Pract. Prev. Med. 2020, 27, 919–922. (In Chinese) [Google Scholar] [CrossRef]
- Li, X.; Wang, Y.; Song, Y. Analysis of knowledge, belief and behavior regarding rational antibiotic use of some students in Dongcheng district, Beijing. China Health Educ. 2020, 36, 723–728. (In Chinese) [Google Scholar] [CrossRef]
- Piao, S. Investigation and analysis on the cognition and use of antibiotics among residents in a community in Dalian. China New Commun. 2019, 21, 221–222. (In Chinese) [Google Scholar]
- Qin, Z.; Li, H.; Tian, F. Investigation and analysis of drug behavior risk KAP of residents in Sichuan Province. J. Clin. Drug Ther. 2019, 17, 73–77. (In Chinese) [Google Scholar] [CrossRef]
- Jiang, Y.; Yang, Y.; Cheng, J. Investigation of Cognition and Self–medication Behavior of Antibiotics among Urban and Rural Residents in Lu’an City. China Pharm. 2021, 32, 98–103. (In Chinese) [Google Scholar] [CrossRef]
- Cao, L.; Yuan, Y.; Sun, Y. The effect of parental knowledge survey on preventing antibiotic abuse—An investigation on antibiotic knowledge of 1080 children’s parents. Chin. Med. J. 2004, 2, 35–37. (In Chinese) [Google Scholar]
- Tan, Y.; Tang, H.; Zhang, X. A survey on the cognition and use of antibiotics by residents in villages and towns in northeastern Sichuan. Beifang Pharm. 2014, 11, 126–127. (In Chinese) [Google Scholar]
- Ye, L. Evaluation of Health Education Effect on Undergraduates’ Antibiotic Application Cognition and Behavior. Chin. Sch. Health 2004, 2, 196. (In Chinese) [Google Scholar]
- Yao, X.; Liu, S. Investigation on the cognition, usage habits and application attitude of antibacterial drugs among college students. Health Vocat. Educ. 2018, 36, 123–125. (In Chinese) [Google Scholar]
- Zhao, Y.; Jiang, Y.; Wu, Y. Investigation on Knowledge, Attitude and Practice on Antibiotics among Undergraduates of Sichuan University. China Pharm. Aff. 2017, 31, 1522–1526. (In Chinese) [Google Scholar] [CrossRef]
- Li, J.; Li, Y.; Wei, Y. Analysis on the Antibiotic Status of Rural Residents in Ethnic Autonomous Regions and Its Influencing Factors—Take Pingluo County for Example. China Health Ind. 2018, 15, 173–178. (In Chinese) [Google Scholar] [CrossRef]
- Huang, C.; Jin, Y. Effect Evaluation on Health Education Prevention for Reasonable Use of Antibiotics in Huating Town of Shanghai. Health Educ. Health Promot. 2014, 9, 439–441. (In Chinese) [Google Scholar] [CrossRef]
- Wu, C.; Guan, S. Intervention effect evaluation antibiotics among boarding students in Wenzhou. Chin. Sch. Health 2012, 33, 531–532. (In Chinese) [Google Scholar] [CrossRef]
- Wen, W. Investigation on Antibacterial Drug Knowledge and Drug Use Behavior of Residents in Yingze District. J. Shanxi Med. Coll. Staff Work. 2018, 28, 82–84. (In Chinese) [Google Scholar]
- Lu, T.; Li, X. Research on the Knowledge, Attitudes and Behaviors of Antibiotic Use among College Students from 5 Universities in Nanjing. J. Nanjing Med Univ. (Soc. Sci. Ed.) 2016, 16, 274–280. (In Chinese) [Google Scholar] [CrossRef]
- Rong, J.; Gao, J.; Zhang, L. Investigation and analysis on the cognitive situation of rational use of antibiotics in Shanghai. Health Educ. Health Promot. 2013, 8, 208–210. (In Chinese) [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J.; Li, P. A survey of knowledge, attitude and practice about antibiotic use among caregivers and health knowledge among school–aged children. In Proceedings of the Chinese Pharmaceutical Association Pharmaceutical Management Professional Committee Annual Meeting and Academic Symposium, Jinan, Shandong, China, 24 August 2018. (In Chinese). [Google Scholar]
- The Medicine and Society. Guide for Authors. Available online: http://yxysh.hust.edu.cn/info/1008/1036.htm (accessed on 16 April 2021).
- The Chinese Health Service Management. Guide for Authors. Available online: http://www.zgwssygl.cn/html/list–10–1.html (accessed on 16 April 2021).
- Larson, E.; Lin, S.X.; Gomez–Duarte, C. Antibiotic use in Hispanic households, New York city. Emerg. Infect. Dis. 2003, 9, 1096–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigoryan, L.; Germanos, G.; Zoorob, R.; Juneja, S.; Raphael, J.L.; Paasche–Orlow, M.K.; Trautner, B.W. Use of Antibiotics Without a Prescription in the U.S. Population: A Scoping Review. Ann. Intern. Med. 2019, 171, 257–263. [Google Scholar] [CrossRef]
- Mainous, A.G., 3rd; Cheng, A.Y.; Garr, R.C.; Tilley, B.C.; Everett, C.J.; McKee, M.D. Nonprescribed antimicrobial drugs in Latino community, South Carolina. Emerg. Infect. Dis. 2005, 11, 883–888. [Google Scholar] [CrossRef]
- Zoorob, R.; Grigoryan, L.; Nash, S.; Trautner, B.W. Nonprescription Antimicrobial Use in a Primary Care Population in the United States. Antimicrob. Agents Chemother. 2016, 60, 5527–5532. [Google Scholar] [CrossRef] [Green Version]
- Saradamma, R.D.; Higginbotham, N.; Nichter, M. Social factors influencing the acquisition of antibiotics without prescription in Kerala State, south India. Social Sci. Med. 2000, 50, 891–903. [Google Scholar] [CrossRef]
- Measures for the Administration of Clinical Application of Antibacterial Drugs. Available online: http://www.nhc.gov.cn/fzs/s3576/201808/f5d983fb5b6e4f1ebdf0b7c32c37a368.shtml (accessed on 22 March 2021).
- About the General Office of the State Council Opinions on Improving the National Essential Drug System. Available online: http://www.gov.cn/zhengce/content/2018–09/19/content_5323459.htm (accessed on 22 March 2021).
- The 13th Five–Year Plan for Deepening the Reform of the Medical and Health System. Available online: http://www.gov.cn/zhengce/content/2017–01/09/content_5158053.htm (accessed on 22 March 2021).
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross–Degnan, D. Assessment of non–prescription antibiotic dispensing at community pharmacies in China with simulated clients: A mixed cross–sectional and longitudinal study. Lancet Infect. Dis. 2019, 19, 1345–1354. [Google Scholar] [CrossRef]
- Gong, Y.; Jiang, N.; Chen, Z.; Wang, J.; Zhang, J.; Feng, J.; Lu, Z.; Yin, X. Over–the–counter antibiotic sales in community and online pharmacies, China. Bull. World Health Organ. 2020, 98, 449–457. [Google Scholar] [CrossRef]
- Kalungia, A.; Godman, B. Implications of non–prescription antibiotic sales in China. Lancet Infect. Dis. 2019, 19, 1272–1273. [Google Scholar] [CrossRef] [Green Version]
- Covvey, J.R.; Johnson, B.F.; Elliott, V.; Malcolm, W.; Mullen, A.B. An association between socioeconomic deprivation and primary care antibiotic prescribing in Scotland. J. Antimicrob. Chemother. 2014, 69, 835–841. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. Don’t wear me out––the public’s knowledge of and attitudes to antibiotic use. J. Antimicrob. Chemother. 2007, 59, 727–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pechère, J.C.; Hughes, D.; Kardas, P.; Cornaglia, G. Non–compliance with antibiotic therapy for acute community infections: A global survey. Int. J. Antimicrob. Agents 2007, 29, 245–253. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S.; Ferranti, R.; Mistretta, A. Pattern of antibiotic use in the community: Νon–adherence and self–prescription rates in an Italian urban population. Mol. Med. Rep. 2012, 5, 1305–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demoré, B.; Mangin, L.; Tebano, G.; Pulcini, C.; Thilly, N. Public knowledge and behaviours concerning antibiotic use and resistance in France: A cross–sectional survey. Infection 2017, 45, 513–520. [Google Scholar] [CrossRef]
- Fernandes, M.; Leite, A.; Basto, M.; Nobre, M.A.; Vieira, N.; Fernandes, R.; Nogueira, P.; Nicola, P.J. Non–adherence to antibiotic therapy in patients visiting community pharmacies. Int. J. Clin. Pharm. 2014, 36, 86–91. [Google Scholar] [CrossRef]
- Horne, R.; Chapman, S.C.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding patients’ adherence–related beliefs about medicines prescribed for long–term conditions: A meta–analytic review of the Necessity–Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Champman, S.; Li, X.; Li, X.; Li, S.; Chen, R.; Bo, N.; Chater, A.; Horne, R. Beliefs about medicines and non–adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: A cross–sectional study in China. BMJ Open 2017, 7, e017293. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance: Multi–country Public Awareness Survey; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- NHS UK. Antibiotic Uses. Available online: https://www.nhs.uk/conditions/antibiotics/uses/ (accessed on 15 April 2021).
- Sun, C.; Hu, Y.J.; Wang, X.; Lu, J.; Lin, L.; Zhou, X. Influence of leftover antibiotics on self–medication with antibiotics for children: A cross–sectional study from three Chinese provinces. BMJ Open 2019, 9, e033679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualano, M.R.; Gili, R.; Scaioli, G.; Bert, F.; Siliquini, R. General population’s knowledge and attitudes about antibiotics: A systematic review and meta–analysis. Pharmacoepidemiol. Drug Saf. 2015, 24, 2–10. [Google Scholar] [CrossRef] [PubMed]
- National Action Plan for Containing Antimicrobial Resistance (2016–2020). Available online: https://www.who.int/publications/m/item/china–national–action–plan–to–contain–antimicrobial–resistance–(2016–2020).
- Huttner, B.; Goossens, H.; Verheij, T.; Harbarth, S. Characteristics and outcomes of public campaigns aimed at improving the use of antibiotics in outpatients in high–income countries. Lancet Infect. Dis. 2010, 10, 17–31. [Google Scholar] [CrossRef]
- Cross, E.L.; Tolfree, R.; Kipping, R. Systematic review of public–targeted communication interventions to improve antibiotic use. J. Antimicrob. Chemother. 2017, 72, 975–987. [Google Scholar] [CrossRef] [Green Version]
- Make Prescription Medication No Longer Difficult! Trial Operation of the Province’s First Electronic Prescription Circulation Supervision Service Platform. Available online: https://baijiahao.baidu.com/s?id=1685403808329340175&wfr=spider&for=pc (accessed on 7 December 2020).
- Chen, J.; Wang, Y.; Chen, X.; Hesketh, T. Widespread illegal sales of antibiotics in Chinese pharmacies–a nationwide cross–sectional study. Antimicrob. Resist. Infect. Control 2020, 9, 12. [Google Scholar] [CrossRef]
- Kotwani, A.; Wattal, C.; Joshi, P.C.; Holloway, K. Irrational use of antibiotics and role of the pharmacist: An insight from a qualitative study in New Delhi, India. J. Clin. Pharm. Ther. 2012, 37, 308–312. [Google Scholar] [CrossRef]
- Khan, T.M.; Ibrahim, Y. A qualitative exploration of the non–prescription sale of drugs and incidence of adverse events in community pharmacy settings in the Eastern Province of the Kingdom of Saudi Arabia. Eur. J. Hosp. Pharm. Sci. Pract. 2013, 20, 26. [Google Scholar] [CrossRef]
- Parsons, S.; Morrow, S.; Underwood, M. Did local enhancement of a national campaign to reduce high antibiotic prescribing affect public attitudes and prescribing rates? Eur. J. Gen. Pract. 2004, 10, 18–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.M.; Singh, S.R.; Duong, M.C.; Legido–Quigley, H.; Hsu, L.Y.; Tam, C.C. Impact of national interventions to promote responsible antibiotic use: A systematic review. J. Antimicrob. Chemother. 2020, 75, 14–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| # | Searches |
|---|---|
| 1 | (antibacterial * or antibiotics * or antimicrobial *).af. |
| 2 | (application * or management * or use * or storage * or non-prescri * or self-medication * or irrational * or abuse * or behavior * or status quo *).af. |
| 3 | (determinants * or knowledge * or attitude * or belief * or expectation * or medical advice * or compliance *).af. |
| 4 | (residents * or population * or general population * or public * or respiratory infection patients * or middle-aged and elderly * or students * or outpatients *).af. |
| 5 | 1 and 2 and 3 and 4 |
| First Author | Year | Region | Study Design | Type of Participants | Sample Size | Quality Assessment |
|---|---|---|---|---|---|---|
| Tian, X. [37] | 2006 | East | Cross-sectional | Students | 4980 | 4 |
| Su, D. [38] | 2006 | East | Quasi-experimental | Rural residents | 420 | 5 |
| Xie, J. [39] | 2006 | East | Quasi-experimental | Urban residents | 209 | 4 |
| Luo, J. [40] | 2008 | Central | Cross-sectional | Pharmacy customers | 1490 | 7 |
| Yin, T. [41] | 2008 | Central | Cross-sectional | Pharmacy customers | 396 | 7 |
| Hu, L. [42] | 2008 | East | Cross-sectional | Urban residents | 209 | 5 |
| Wang, Y. [43] | 2008 | East | Cross-sectional | Urban residents | 658 | 4 |
| Li, B. [44] | 2008 | Central | Cross-sectional | Children’s parents | 266 | 4 |
| Ye, L. [45] | 2009 | Central | Cross-sectional | Outpatients | 276 | 4 |
| Sun, L. [46] | 2010 | East | Cross-sectional | Students | 853 | 4 |
| Huang, W. [47] | 2011 | West | Cross-sectional | Outpatients | 956 | 5 |
| Huang, Y. [48] | 2011 | East | Cross-sectional | Urban residents | 298 | 4 |
| Ji, H. [49] | 2011 | West | Cross-sectional | Urban residents | 400 | 5 |
| Shan, H. [50] | 2011 | East | Cross-sectional | Outpatients | 1236 | 4 |
| Huang, C. [51] | 2012 | East | Cross-sectional | Rural residents | 400 | 5 |
| Cheng, S. [52] | 2012 | East | Cross-sectional | Urban residents | 164 | 5 |
| Zhao, L. [53] | 2012 | East | Cross-sectional | Rural residents | 1014 | 6 |
| Wu, Y. [54] | 2012 | West | Cross-sectional | Urban and rural residents | 1200 | 5 |
| Ma, X. [55] | 2012 | East | Cross-sectional | Urban residents | 4183 | 4 |
| Yu, M. [56] | 2012 | Central | Cross-sectional | Children’s parents | 854 | 5 |
| Liu, S. [57] | 2012 | East | Cross-sectional | Urban residents | 200 | 4 |
| Du, X. [58] | 2012 | Central | Cross-sectional | Students | 905 | 4 |
| Tao, G. [59] | 2013 | West | Quasi-experimental | Urban residents | 1000 | 6 |
| Li, Y. [60] | 2013 | East | Cross-sectional | Rural residents | 1589 | 5 |
| Jin, Y. [61] | 2013 | West | Cross-sectional | Urban residents | 2556 | 5 |
| Ye, W. [62] | 2013 | East | Cross-sectional | Rural residents | 800 | 4 |
| Tang, X. [63] | 2013 | East | Cross-sectional | Outpatients | 496 | 4 |
| Zhang, Y. [64] | 2013 | East | Cross-sectional | Students | 1180 | 4 |
| Xu, Y. [65] | 2013 | East | Cross-sectional | Urban residents | 106 | 5 |
| Liu, M. [66] | 2013 | East | Cross-sectional | Children’s parents | 1046 | 7 |
| Sun, W. [67] | 2014 | East | Quasi-experimental | Children’s parents | 593 | 6 |
| Ding, L. [68] | 2014 | East | Cross-sectional | Children’s parents | 722 | 5 |
| Tian, L. [69] | 2014 | East | Cross-sectional | Urban residents | 316 | 5 |
| Han, F. [70] | 2014 | Central | Cross-sectional | Students | 4462 | 5 |
| Yuan, J. [71] | 2014 | West | Cross-sectional | Rural residents | 435 | 6 |
| Bian, C. [72] | 2014 | Central | Cross-sectional | Outpatients | 1214 | 4 |
| Zhang, S. [73] | 2014 | Central | Cross-sectional | Urban residents | 500 | 5 |
| Xiong, X. [74] | 2014 | East | Cross-sectional | Urban residents | 354 | 4 |
| Lin, W. [75] | 2014 | East | Cross-sectional | Urban residents | 1784 | 5 |
| Sun, Y. [76] | 2014 | Central | Cross-sectional | Students | 388 | 4 |
| Liu, Y. [77] | 2015 | East | Quasi-experimental | Rural residents | 639 | 7 |
| Diao, M. [78] | 2015 | Central | Cross-sectional | Rural residents | 2047 | 5 |
| Chen, S. [79] | 2015 | East | Cross-sectional | Teachers | 84 | 8 |
| Wang, X. [80] | 2015 | Central | Cross-sectional | Students | 11,192 | 5 |
| Li, Y. [60] | 2015 | Central | Cross-sectional | Students | 692 | 5 |
| Cheng, J. [81] | 2015 | Central | Cross-sectional | Rural residents | 2611 | 6 |
| Zhang, Y. [82] | 2015 | East | Cross-sectional | Children’s parents | 250 | 6 |
| Song, Y. [83] | 2015 | East | Cross-sectional | Students | 812 | 4 |
| Cui, B. [84] | 2015 | East | Cross-sectional | Students | 528 | 4 |
| Ding, L. [85] | 2015 | East | Cross-sectional | Rural residents | 769 | 6 |
| Wang, G. [86] | 2015 | East | Cross-sectional | Urban residents | 1718 | 5 |
| Yu, Y. [87] | 2015 | East | Cross-sectional | Urban residents | 267 | 5 |
| Lei, Z. [88] | 2015 | Central | Cross-sectional | Pharmacy customers | 282 | 4 |
| Chen, C. [89] | 2016 | East | Cross-sectional | Civil servants | 400 | 5 |
| Tang, Z. [90] | 2016 | West | Cross-sectional | Children’s parents | 766 | 5 |
| Wang, Z. [91] | 2016 | East | Cross-sectional | Urban and rural residents | 438 | 5 |
| Jiang, H. [92] | 2016 | East | Cross-sectional | Urban residents | 449 | 6 |
| Wang, Q. [93] | 2016 | West | Cross-sectional | Students | 1584 | 4 |
| Jiang, Y. [94] | 2017 | East | Cross-sectional | Urban and rural residents | 651 | 4 |
| Luo, Y. [95] | 2017 | West | Cross-sectional | Students | 368 | 5 |
| Yang, Q. [96] | 2017 | East | Cross-sectional | Children’s parents | 713 | 4 |
| Wang, P. [97] | 2017 | East | Cross-sectional | Students | 1957 | 4 |
| Li, X. [98] | 2017 | East | Cross-sectional | Children’s parents | 658 | 4 |
| Piao, S. [99] | 2018 | East | Cross-sectional | Urban residents | 181 | 4 |
| Qin, Z. [100] | 2018 | West | Cross-sectional | Urban residents | 518 | 4 |
| Jiang, Y. [101] | 2019 | Central | Cross-sectional | Urban and rural residents | 657 | 6 |
| Cao, L. [102] | NA | East | Cross-sectional | Children’s parents | 1080 | 4 |
| Tan, Y. [103] | NA | West | Cross-sectional | Rural residents | 800 | 4 |
| Ye, L. [104] | NA | East | Cross-sectional | Students | 152 | 6 |
| Yao, X. [105] | NA | East | Cross-sectional | Students | 270 | 6 |
| Zhao, Y. [106] | NA | West | Cross-sectional | Students | 363 | 4 |
| Li, J. [107] | NA | West | Cross-sectional | Rural residents | 286 | 4 |
| Huang, C. [108] | NA | East | Quasi-experimental | Urban residents | 400 | 4 |
| Wu, C. [109] | NA | East | Quasi-experimental | Students | 337 | 4 |
| Wen, W. [110] | NA | Central | Cross-sectional | Urban residents | 315 | 4 |
| Lu, Z. [111] | NA | East | Cross-sectional | Students | 600 | 5 |
| Rong, J. [112] | NA | East | Cross-sectional | Urban residents | 2000 | 4 |
| Zhang, Y. [113] | NA | West | Cross-sectional | Children’s parents | 205 | 4 |
| Subgroup | Demanding Antibiotic Prescription | Non-Prescription Antibiotic Purchasing | Non-Adherence to Antibiotic Prescription | Prophylactic Use of Antibiotics |
|---|---|---|---|---|
| Geographical region | ||||
| Eastern China | 34 (26–43) | 34 (25–44) | 49 (39–60) | 35 (25–46) |
| Central China | 26 (17–37) | 51 (36–65) | 45 (35–56) | 27 (18–37) |
| Western China | 65 (50–78) | 70 (51–86) | 47 (43–52) | 47 (43–51) |
| Study period | ||||
| <2010 | 51 (35–67) | 49 (15–83) | 53 (51–56) | 35 (31–39) |
| 2010–2015 | 37 (20–56) | 57 (43–70) | 51 (43–59)) | 32 (24–40) |
| ≥2015 | 32 (24–41) | 44 (31–58) | 40 (27–53) | 38 (24–53) |
| NA | 33 (20–47) | 29 (15–45) | 70 (51–86) | 42 (36–50) |
| Type of participant | ||||
| Rural residents | 28 (13–45) | 32 (15–52) | 67 (48–84) | 27 (16–39) |
| Urban residents | 48 (33–64) | 54 (32–76) | 45 (36–55) | 39 (26–54) |
| Students | 23 (13–34) | 49 (35–62) | 43 (27–61) | 34 (25–44) |
| Pharmacy’s customer | 49 (47–51) | 73 (71–75) | – | – |
| Children’s parents | 20 (12–29) | 17 (15–21) | 22 (18–25) | – |
| Urban and rural residents | – | 54 (51–58) | 39 (35–43) | – |
| Others | 38 (35–41) | 40 (7–80) | 61 (53–68) | 41 (12–74) |
| Quality score | ||||
| 4–6 | 38 (29–47) | 48 (37–58) | 47 (40–54) | 36 (29–43) |
| 7–9 | 35 (10–64) | 45 (18–75) | 63 (61–65) | 40 (3–44) |
| Study size | ||||
| <400 | 41 (28–55) | 40 (27–53) | 44 (34–55) | 38 (26–51) |
| 400–800 | 37 (24–51) | 42 (26–58) | 54 (31–76) | 40 (16–67) |
| 800–1200 | 88 (86–90) | 70 (41–93) | 51 (30–72) | 32 (30–34) |
| ≥1200 | 28 (16–42) | 54 (34–74) | 48 (37–58) | 28 (21–34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duan, L.; Liu, C.; Wang, D. The General Population’s Inappropriate Behaviors and Misunderstanding of Antibiotic Use in China: A Systematic Review and Meta-Analysis. Antibiotics 2021, 10, 497. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050497
Duan L, Liu C, Wang D. The General Population’s Inappropriate Behaviors and Misunderstanding of Antibiotic Use in China: A Systematic Review and Meta-Analysis. Antibiotics. 2021; 10(5):497. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050497
Chicago/Turabian StyleDuan, Lixia, Chenxi Liu, and Dan Wang. 2021. "The General Population’s Inappropriate Behaviors and Misunderstanding of Antibiotic Use in China: A Systematic Review and Meta-Analysis" Antibiotics 10, no. 5: 497. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050497