
High Cefuroxime Concentrations and Long Elimination in an Orthopaedic Surgical Deadspace—A Microdialysis Porcine Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Comparison of Weight Groups
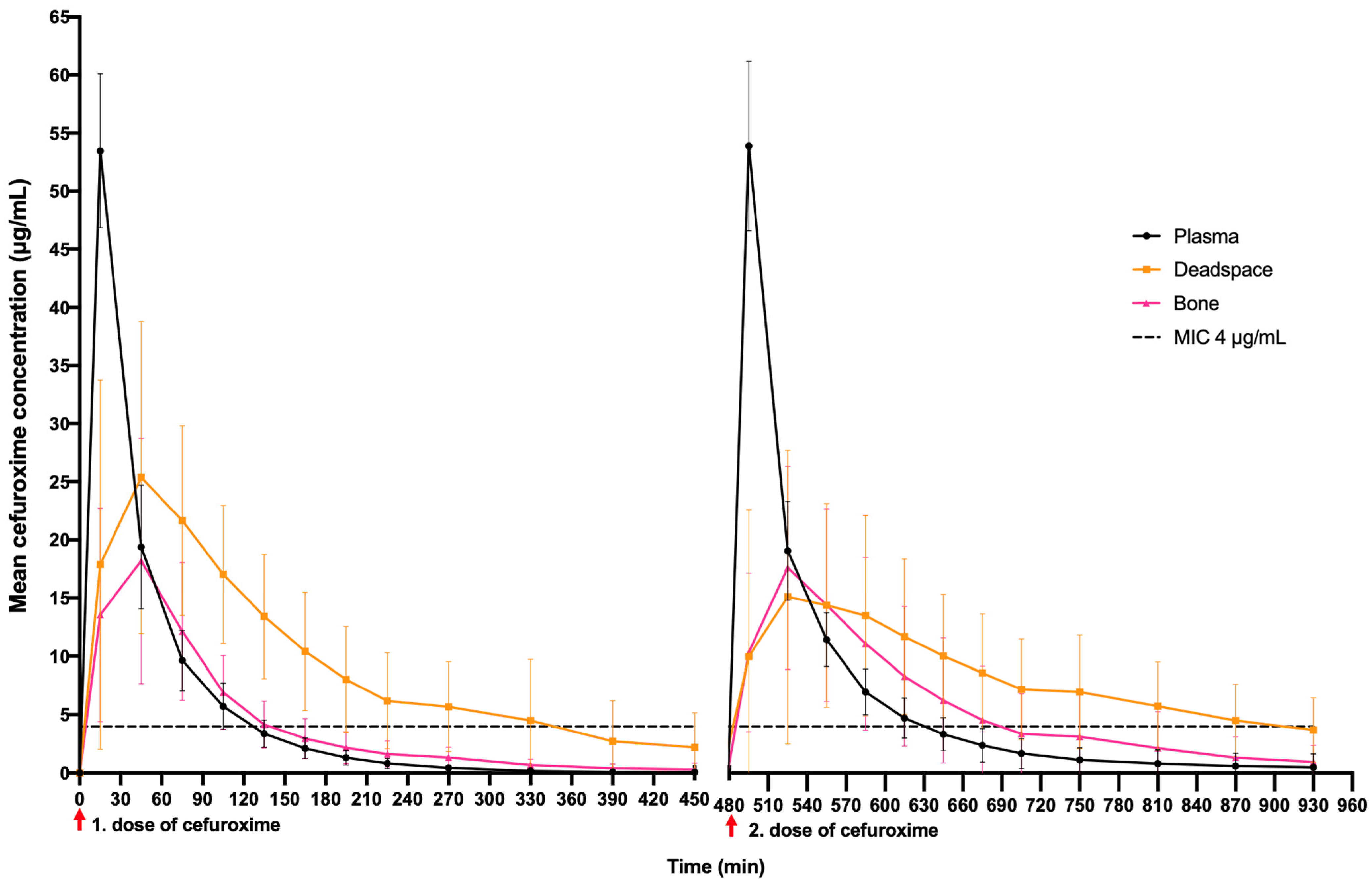
2.2. fT > MIC (4 μg/mL) and Time to Reach A Mean Concentration of 4 μg/mL
2.3. Pharmacokinetic Parameters
3. Discussion
- (1)
- Deadspace fT > MIC (4 µg/mL) was longer than that of both bone and plasma, especially in the second dosing interval.
- (2)
- Plasma Cmax was twice as high as deadspace Cmax, but deadspace AUC was significantly higher than plasma AUC.
- (3)
- Deadspace penetration was higher than that of bone in both dosing intervals.
- (4)
- In the second dosing interval, deadspace penetration was significantly delayed compared to the first dosing interval, and a lower mean concentration was found.
- (5)
- Deadspace elimination was significantly longer in the second dosing interval compared with first dosing interval, and more than twice that of plasma and bone in both dosing intervals.
4. Materials and Methods
4.1. Study Design and Anaesthetic
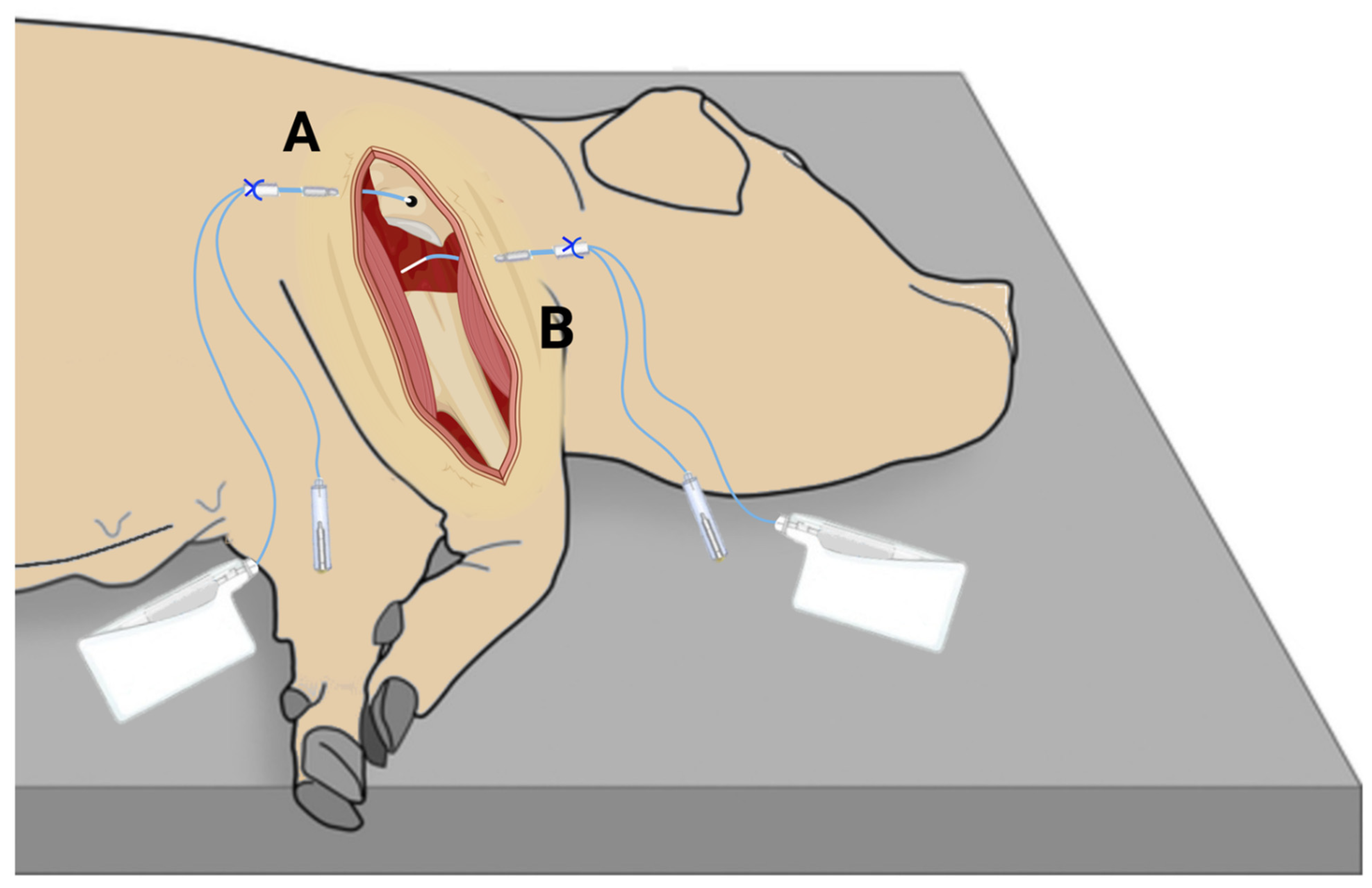
4.2. Surgical Procedure

4.3. Cefuroxime Administration, Sampling and Handling of Samples
4.4. Microdialysis
4.5. Liquid Chromatography Tandem Mass Spectrometry (LC-MS/MS)
4.6. Pharmacokinetic Analysis and Statistical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singhal, K.; Rammohan, R. Going forward with reverse shoulder arthroplasty. J. Clin. Orthop. Trauma 2018, 9, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, J.H.; Manring, M.M. Adult osteomyelitis. Infect. Dis. Clin. North Am. 2005, 19, 65–86. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Fragomen, A.T.; Moriarty, T.F.; Morgenstern, M.; Egol, K.; Zalavras, C.; Obremskey, W.T.; Raschke, M.; McNally, M.A. Evidence-Based Recommendations for Local Antimicrobial Strategies and Dead Space Management in Fracture-Related Infection. J. Orthop. Trauma 2020, 34, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Oliver, R.A.; Lovric, V.; Yu, Y.; Christou, C.; Aiken, S.S.; Cooper, J.J.; Walsh, W.R. Development of a Novel Model for the Assessment of Dead-Space Management in Soft Tissue. PLoS ONE 2015, 10, e0136514. [Google Scholar] [CrossRef] [PubMed]
- Darouiche, R.O. Treatment of infections associated with surgical implants. N. Engl. J. Med. 2004, 350, 1422–1429. [Google Scholar] [CrossRef]
- Gage, M.J.; Yoon, R.S.; Gaines, R.J.; Dunbar, R.P.; Egol, E.A.; Liporace, F.A. Dead Space Management after Orthopaedic Trauma: Tips, Tricks, and Pitfalls. J. Orthop. Trauma 2016, 30, 64–70. [Google Scholar] [CrossRef]
- Whiteside, L.A. Prophylactic peri-operative local antibiotic irrigation. Bone Jt. J. 2016, 98-b, 23–26. [Google Scholar] [CrossRef] [Green Version]
- Tong, S.Y.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G., Jr. Staphylococcus aureus infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 2015, 28, 603–661. [Google Scholar] [CrossRef] [Green Version]
- Campoccia, D.; Montanaro, L.; Arciola, C.R. The significance of infection related to orthopedic devices and issues of antibiotic resistance. Biomaterials 2006, 27, 2331–2339. [Google Scholar] [CrossRef]
- Peel, T.N.; Cheng, A.C.; Buising, K.L.; Choong, P.F.M. Microbiological aetiology, epidemiology, and clinical profile of prosthetic joint infections: Are current antibiotic prophylaxis guidelines effective? Antimicrob. Agents Chemother. 2012, 56, 2386–2391. [Google Scholar] [CrossRef] [Green Version]
- Nowakowska, J.; Landmann, R.; Khanna, N. Foreign Body Infection Models to Study Host-Pathogen Response and Antimicrobial Tolerance of Bacterial Biofilm. Antibiotics 2014, 3, 378–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, W.; Waldvogel, F.A.; Vaudaux, P.; Nydegger, U.E. Pathogenesis of foreign body infection: Description and characteristics of an animal model. J. Infect. Dis. 1982, 146, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Bendtsen, M.A.F.; Bue, M.; Hanberg, P.; Slater, J.; Thomassen, M.B.; Hansen, J.; Søballe, K.; Öbrink-Hansen, K.; Stilling, M. Flucloxacillin bone and soft tissue concentrations assessed by microdialysis in pigs after intravenous and oral administration. Bone Jt. Res. 2021, 10, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Bue, M.; Tøttrup, M.; Hanberg, P.; Langhoff, O.; Birke-Sørensen, H.; Thillemann, T.M.; Andersson, T.L.; Søballe, K. Bone and subcutaneous adipose tissue pharmacokinetics of vancomycin in total knee replacement patients. Acta Orthop. 2018, 89, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Slater, J.; Stilling, M.; Hanberg, P.; Bendtsen, M.A.F.; Jørgensen, A.R.; Søballe, K.; Jørgensen, N.P.; Bue, M. Moxifloxacin Concentrations in the Knee Joint, Tibial Bone, and Soft Tissue When Combined with Rifampicin: A Randomized Porcine Microdialysis Study. J.Bone Jt. Surg. Am. 2022, 104, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for Prevention of Surgical Site Infection. Am. J. Infect. Control 1999, 27, 97–132. [Google Scholar] [CrossRef]
- McKinnon, P.S.; Paladino, J.A.; Schentag, J.J. Evaluation of area under the inhibitory curve (AUIC) and time above the minimum inhibitory concentration (T>MIC) as predictors of outcome for cefepime and ceftazidime in serious bacterial infections. Int. J. Antimicrob. Agents 2008, 31, 345–351. [Google Scholar] [CrossRef]
- Eucast. Antimicrobial Wild Type Distributions of Microorganisms. 2020. Available online: https://mic.eucast.org/Eucast2/SearchController/search.jsp?action=init (accessed on 25 September 2020).
- Tøttrup, M.; Bue, M.; Koch, J.; Jensen, L.K.; Hanberg, P.; Aalbæk, B.; Fuursted, K.; Jensen, H.E.; Søballe, K. Effects of Implant-Associated Osteomyelitis on Cefuroxime Bone Pharmacokinetics: Assessment in a Porcine Model. J. Bone Jt. Surg. Am. 2016, 98, 363–369. [Google Scholar] [CrossRef]
- Hanberg, P.; Bue, M.; Kabel, J.; Jørgensen, A.R.; Jessen, C.; Søballe, K.; Stilling, M. Effects of tourniquet inflation on peri- and postoperative cefuroxime concentrations in bone and tissue. Acta Orthop. 2021, 92, 1–7. [Google Scholar] [CrossRef]
- Prokuski, L. Prophylactic antibiotics in orthopaedic surgery. J. Am. Acad. Orthop. Surg. 2008, 16, 283–293. [Google Scholar] [CrossRef]
- Tøttrup, M.; Søballe, K.; Bibby, B.M.; Hardlei, T.F.; Hansen, P.; Fuursted, K.; Birke-Sørensen, H.; Bue, M. Bone, subcutaneous tissue and plasma pharmacokinetics of cefuroxime in total knee replacement patients—A randomized controlled trial comparing continuous and short-term Infusion. APMIS 2019, 127, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Engesaeter, L.B.; Lie, S.A.; Espehaug, B.; Furnes, O.; Vollset, S.E.; Havelin, L. Antibiotic prophylaxis in total hip arthroplasty: Effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0–14 years in the Norwegian Arthroplasty Register. Acta Orthop. Scand 2003, 74, 644–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veltman, E.S.; Lenguerrand, E.; Moojen, D.J.F.; Whitehouse, M.; Nelissen, R.G.H.H.; Blom, A.W.; Poolman, R.W. Similar risk of complete revision for infection with single-dose versus multiple-dose antibiotic prophylaxis in primary arthroplasty of the hip and knee: Results of an observational cohort study in the Dutch Arthroplasty Register in 242,179 patients. Acta Orthop. 2020, 91, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Bitar, D.; Parvizi, J. Biological response to prosthetic debris. World J. Orthop. 2015, 6, 172–189. [Google Scholar] [CrossRef] [PubMed]
- Southwood, R.T.; Rice, J.L.; McDonald, P.J.; Hakendorf, P.H.; Rozenbilds, M.A. Infection in experimental hip arthroplasties. J. Bone Jt. Surg. Br. 1985, 67, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Cordero, J.; Munuera, L.; Folgueira, M.D. Influence of bacterial strains on bone infection. J. Orthop. Res. 1996, 14, 663–667. [Google Scholar] [CrossRef]
- Lauderdale, K.J.; Malone, C.L.; Boles, B.R.; Morcuende, J.; Horswill, A.R. Biofilm dispersal of community-associated methicillin-resistant Staphylococcus aureus on orthopedic implant material. J. Orthop. Res. 2010, 28, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Nunes, S.; Carneiro, C.; Bexiga, R.; Bernardo, F.; Vilela, C. Time course of biofilm formation by Staphylococcus aureus and Staphylococcus epidermidis mastitis isolates. Vet. Microbiol. 2007, 124, 187–191. [Google Scholar] [CrossRef]
- Gristina, A.G. Implant failure and the immuno-incompetent fibro-inflammatory zone. Clin. Orthop. Relat. Res. 1994, 298, 106–118. [Google Scholar] [CrossRef]
- Mihailescu, R.; Tafin, U.F.; Corvec, S.; Oliva, A.; Betrisey, B.; Borens, O.; Trampuz, A. High activity of Fosfomycin and Rifampin against methicillin-resistant staphylococcus aureus biofilm in vitro and in an experimental foreign-body infection model. Antimicrob. Agents Chemother. 2014, 58, 2547–2553. [Google Scholar] [CrossRef] [Green Version]
- Jaruratanasirikul, S.; Sriwiriyajan, S. Stability of meropenem in normal saline solution after storage at room temperature. Southeast Asian J. Trop. Med. Public Health 2003, 34, 627–629. [Google Scholar] [PubMed]
- Carlier, M.; Stove, V.; Verstraete, A.; De Waele, J.J. Stability of generic brands of meropenem reconstituted in isotonic saline. Minerva Anestesiol. 2015, 81, 283–287. [Google Scholar] [PubMed]
- Swindle, M.M.; Makin, A.; Herron, A.J.; Clubb, F.J., Jr.; Frazier, K.S. Swine as models in biomedical research and toxicology testing. Vet. Pathol. 2012, 49, 344–356. [Google Scholar] [CrossRef] [PubMed]
- Hanberg, P.; Bue, M.; Öbrink-Hansen, K.; Thomassen, M.; Søballe, K.; Stilling, M. Timing of Antimicrobial Prophylaxis and Tourniquet Inflation: A Randomized Controlled Microdialysis Study. J. Bone Jt. Surg. Am. 2020, 102, 1857–1864. [Google Scholar] [CrossRef]
- Flecknell, P. Replacement, reduction and refinement. ALTEX 2002, 19, 73–78. [Google Scholar]
- Tøstesen, S.K.; Hanberg, P.; Bue, M.; Thillemann, T.M.; Falstie-Jensen, T.; Tøttrup, M.; Knudsen, M.B.; Schmedes, A.V.; Stilling, M. Weight-based cefuroxime dosing provides comparable orthopedic target tissue concentrations between weight groups—A microdialysis porcine study. APMIS 2021, 130, 111–118. [Google Scholar] [CrossRef]
- Hanberg, P.; Szekely, G.; Blanc, R. Simultaneous Retrodialysis by Drug for Cefuroxime Using Meropenem as an Internal Standard-A Microdialysis Validation Study. J. Pharm. Sci. 2020, 109, 1373–1379. [Google Scholar] [CrossRef]
- Krcah, M.; SzÈkely, G.B.; Blanc, R. Fully automatic and fast segmentation of the femur bone from 3D-CT images with no shape prior. In Proceedings of the 2011 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Chicago, IL, USA, 30 March–2 April 2011; pp. 2087–2090. [Google Scholar]
- De Raedt, S.; Mechlenburg, I.; Stilling, M.; Rømer, L.; Søballe, K.; de Bruijne, M. Automated measurement of diagnostic angles for hip dysplasia. In Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 9 February 2013; SPIE: Bellingham, DC, USA, 2013; Volume 8670. [Google Scholar]
- Boykov, Y.; Funka-Lea, G. Graph Cuts and Efficient N-D Image Segmentation. Int. J. Comput. Vis. 2006, 70, 109–131. [Google Scholar] [CrossRef] [Green Version]
- BioRender. Available online: https://biorender.com/. (accessed on 20 December 2021).
- Knudsen, M.; Bue, M.; Pontoppidan, L.L.; Hvistendahl, M.A.; Søballe, K.; Stilling, M.; Hanberg, P. Evaluation of Benzylpenicillin as an Internal Standard for Measurement of Piperacillin Bone Concentrations via Microdialysis. J. Pharm Sci. 2021, 110, 3500–3506. [Google Scholar] [CrossRef]
- Olsen Kipp, J.; Hanberg, P.; Slater, J.; Nielsen, L.M.; Jakobsen, S.S.; Stilling, M.; Bue, M. Vancomycin bone and tissue concentrations following tibial intraosseous administration—Evaluated in a porcine model. J. Bone Jt. Infect. 2021, 6, 99–106. [Google Scholar] [CrossRef]
- Hanberg, P.; Bue, M.; Jørgensen, A.R.; Thomassen, M.; Öbrink-Hansen, K.; Søballe, K.; Stilling, M. Pharmacokinetics of double-dose cefuroxime in porcine intervertebral disc and vertebral cancellous bone-a randomized microdialysis study. Spine J. 2020, 20, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Joukhadar, C.; Müller, M. Microdialysis: Current applications in clinical pharmacokinetic studies and its potential role in the future. Clin. Pharmacokinet. 2005, 44, 895–913. [Google Scholar] [CrossRef] [PubMed]
- Bøgehøj, M.F.; Emmeluth, C.; Overgaard, S. Microdialysis in the femoral head of the minipig and in a blood cloth of human blood. Acta Orthop. 2011, 82, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Stolle, L.B.; Arpi, M.; Jørgensen, P.; Riegels-Nielsen, P.; Keller, J. In situ gentamicin concentrations in cortical bone: An experimental study using microdialysis in bone. Acta Orthop. Scand 2003, 74, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Tøttrup, M.; Hardlei, T.F.; Bendtsen, M.; Bue, M.; Brock, B.; Fuursted, K.; Søballe, K.; Birke-Sørensen, H. Pharmacokinetics of cefuroxime in porcine cortical and cancellous bone determined by microdialysis. Antimicrob. Agents Chemother. 2014, 58, 3200–3205. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Comparison of Weight groups | Group 1 53–57 kg | Group 2 73–77 kg | Group 3 93–97 kg |
|---|---|---|---|
| Humeral head size: Volume, mm3 (95% CI) | 14,413 (10,941–17,885) | 17,971 (14,499–21,443) | 22,361 (18,889–25,833) |
| Deadspace fT > MIC, min (95% CI): First dosing interval | 333 (241–424) | 255 (163–346) | 245 (148–341) |
| Deadspace fT > MIC, min (95% CI): Second dosing interval | 321 (230–412) | 378 (287–469) | 315 (219–412) |
| AUCdeadspace/AUCplasma (95% CI): First dosing interval | 1.87 (1.38–2.35) | 1.77 (1.29–2.25) | 1.27 (0.79–1.76) |
| AUCdeadspace/AUCplasma (95% CI): Second dosing interval | 1.13 (0.65–1.61) | 1.70 (1.22–2.19) | 1.19 (0.68–1.71) |
| fT > MIC | First Dosing Interval | Second Dosing Interval | Total | p-Values 1st and 2nd Dosing Interval | p-Values Compartments |
|---|---|---|---|---|---|
| Plasma fT > MIC, min (95% CI) | 124 (72–177) | 160 (107–212) | 284 (232–337) | 0.206 * | <0.000 ** |
| % fT > MIC (95% CI) | 28 (16–39) | 36 (24–47) | 32 (26–37) | ||
| Deadspace fT > MIC, min (95% CI) | 277 (224–331) | 338 (284–391) | 605 (552–658) | 0.039 * | <0.000 *** |
| % fT > MIC (95% CI) | 62 (50–74) | 75 (63–87) | 67 (61–73) | ||
| Bone fT > MIC, min (95% CI) | 130 (77–182) | 205 (152–257) | 334 (282–387) | 0.008 * | 0.076 **** |
| % fT > MIC (95% CI) | 29 (17–40) | 56 (34–57) | 37 (31–43) |
| TT4 μg/mL | First Dosing Interval | Second Dosing Interval | p-Values |
|---|---|---|---|
| Plasma: TT4, min (SD) | 1 (0) | 1 (0) | 0.995 * |
| Deadspace: TT4, min (SD) | 8 (8) | 21 (23) | 0.003 * |
| Bone: TT4, min (SD) | 10 (16) | 9 (9) | 0.777 * |
| Parameter | First Dosing Interval | Second Dosing Interval | p-Values 1st vs. 2nd Dosing Interval |
|---|---|---|---|
| Plasma AUC, min µg/mL (95% CI) | 2521 (1843–3201) | 2868 (2190–3547) | 0.404 |
| Deadspace AUC, min µg/mL (95% CI) | 4147 (3468–4826) ab | 3787 (3092–4482) ab | 0.394 |
| Bone AUC, min µg/mL (95% CI) | 1886 (1207–2565) | 2621 (1942–3300) | 0.079 |
| Plasma Cmax, µg/mL (95% CI) | 53 (49–58) | 54 (49–59) | 0.890 |
| Deadspace Cmax, µg/mL (95% CI) | 27 (22–32) ab | 19 (14–24) a | 0.011 |
| Bone Cmax, µg/mL (95% CI) | 18 (14–23) | 18 (14–23) | 0.976 |
| Plasma Tmax, min (SD) | 15 (0) | 15 (0) | 1.000 |
| Deadspace Tmax, min (SD) | 57 (29) a | 89 (48) ab | <0.000 |
| Bone Tmax, min (SD) | 48 (14) | 50 (15) | 0.830 |
| Plasma T½, min (SD) | 46 (3) | 97 (50) | 0.338 |
| Deadspace T½, min (SD) | 151 (117) | 407 (455) ab | <0.000 |
| Bone T½, min (SD) | 74 (30) | 149 (103) | 0.169 |
| Deadspace AUCdeadspace/AUCplasma (95% CI) | 1.64 (1.36–1.92) b | 1.34 (1.05–1.62) b | 0.062 |
| Bone AUCbone/AUCplasma (95% CI) | 0.75 (0.48– 1.03) | 0.90 (0.62–1.18) | 0.347 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tøstesen, S.K.; Stilling, M.; Hanberg, P.; Thillemann, T.M.; Falstie-Jensen, T.; Tøttrup, M.; Knudsen, M.; Petersen, E.T.; Bue, M. High Cefuroxime Concentrations and Long Elimination in an Orthopaedic Surgical Deadspace—A Microdialysis Porcine Study. Antibiotics 2022, 11, 208. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11020208
Tøstesen SK, Stilling M, Hanberg P, Thillemann TM, Falstie-Jensen T, Tøttrup M, Knudsen M, Petersen ET, Bue M. High Cefuroxime Concentrations and Long Elimination in an Orthopaedic Surgical Deadspace—A Microdialysis Porcine Study. Antibiotics. 2022; 11(2):208. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11020208
Chicago/Turabian StyleTøstesen, Sara Kousgaard, Maiken Stilling, Pelle Hanberg, Theis Muncholm Thillemann, Thomas Falstie-Jensen, Mikkel Tøttrup, Martin Knudsen, Emil Toft Petersen, and Mats Bue. 2022. "High Cefuroxime Concentrations and Long Elimination in an Orthopaedic Surgical Deadspace—A Microdialysis Porcine Study" Antibiotics 11, no. 2: 208. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11020208