


A Dual Perspective of Psycho-Social Barriers and Challenges Experienced by Drug-Resistant TB Patients and Their Caregivers through the Course of Diagnosis and Treatment: Findings from a Qualitative Study in Bengaluru and Hyderabad Districts of South India
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings
2.2. Study Population
2.3. Ethical Approval and Human Rights
2.4. Data Collection
2.5. Study Process
2.6. Data Analysis
3. Results
3.1. Demography
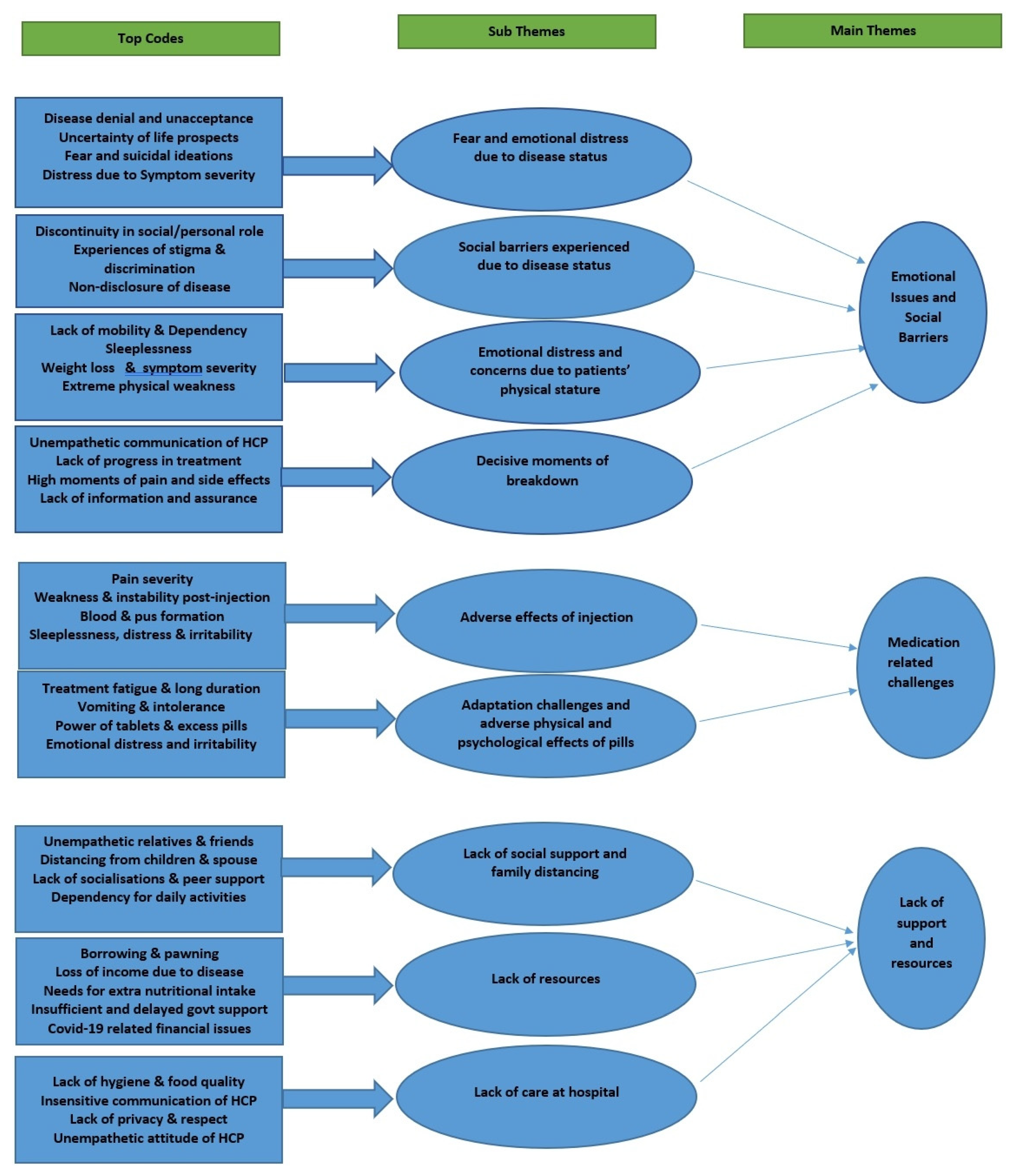
Main Themes and Sub-Themes Classification
3.2. Main Theme-1: Emotional Issues and Social Barriers (Table 2)
3.2.1. Sub-Theme-1: Fear and Emotional Distress Due to Disease Status
3.2.2. Sub-Theme-2: Social Barriers Experienced Due to Disease Status
3.2.3. Sub-Theme-3: Emotional Distress and Concerns Due to Patients’ Physical Stature
3.2.4. Sub-Theme-4: Decisive Moments of Breakdown
3.3. Main Theme-2: Medication-Related Challenges (Table 3)
3.3.1. Sub-Theme-1: Adverse Effects of Injection
3.3.2. Sub-Theme-2: Adaptation Challenges and Adverse Physical and Psychological Effects of Pills
3.4. Main Theme-3: Lack of Support and Resources (Table 4)
3.4.1. Sub-Theme-1: Lack of Social Support and Family Distancing
3.4.2. Sub-Theme-2: Lack of Resources
3.4.3. Sub-Theme-3: Lack of Care at the Hospital
4. Discussion
4.1. Acute Phases of Hopelessness and the Need for a Special Approach
4.2. Lack of Supportive Care and Social Support for Patients and Caregivers
4.3. Physical Appearance Driven Anxiety and Distress
4.4. Lack of Resources as a Major Barrier
4.5. Adverse Physical and Psychological effects of DR-TB Injections and Pills
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2017; Workplace Health and Safety; WHO: Geneva, Switzerland, 2017; Volume 63. [Google Scholar]
- Central TB Division. India TB Report 2018; Central TB Division, Directorate General of Health Services: New Delhi, India, 2018. [Google Scholar]
- Central TB Division. India TB Report 2020; Central TB Division, Directorate General of Health Services: New Delhi, India, 2020. [Google Scholar]
- Parmar, M.M.; Sachdeva, K.S.; Dewan, P.K.; Rade, K.; Nair, S.A.; Pant, R.; Khaparde, S.D. Unacceptable treatment outcomes and associated factors among India’s initial cohorts of multidrug-resistant tuberculosis (MDR-TB) patients under the revised national TB control programme (2007–2011): Evidence leading to policy enhancement. PLoS ONE 2018, 13, e0193903. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.E.; Shanmugam, P.; Malaisamy, M.; Ovung, S.; Suresh, C.; Subbaraman, R.; Adinarayanan, S.; Nagarajan, K. Psycho-socio-economic issues challenging multidrug resistant tuberculosis patients: A systematic review. PLoS ONE 2016, 11, e0147397. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Bakshi, H.; Prajapati, S.; Bhatt, G.; Mehta, R.; Rami, K.; Mehta, P.; Shah, T.; Dave, R.; Pirzada, A. A qualitative study of psycho social impact on multi drug resistant TB (MDRTB) cases: Experience from Ahmedabad City, India. Natl. J. Community Med. 2021, 12, 209–210. [Google Scholar] [CrossRef]
- Ahmad, N.; Javaid, A.; Syed Sulaiman, S.A.; Basit, A.; Afridi, A.K.; Jaber, A.A.; Khan, A.H. Effects of multidrug resistant tuberculosis treatment on patients’ health related quality of life: Results from a follow up study. PLoS ONE 2016, 11, e0159560. [Google Scholar] [CrossRef] [PubMed]
- Laxmeshwar, C.; Das, M.; Mathur, T.; Israni, T.; Jha, S.; Iyer, A.; Morales, M.; Decroo, T.; Gils, T.; Ferlazzo, G.; et al. Psychiatric comorbidities among patients with complex drug-resistant tuberculosis in Mumbai, India. PLoS ONE 2022, 17, e0263759. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.; Basu, R.; Sarkar, S.; Nath, S.; Biswas, D. Psychological profile of multi drug resistance TB patients: A qualitative study from a Tertiary care Centre of Kolkata. J. Fam. Med. Prim. Care 2021, 10, 392–397. [Google Scholar]
- Misra, S.; Misra, N.; Seepamore, B.; Holloway, K.; Singh, N.; Ngozo, J.; Dlamini, V.; Radebe, Z.; Ndjeka, N.O.; Furin, J. “I would watch her with awe as she swallowed the first handful”: A qualitative study of pediatric multidrug-resistant tuberculosis experiences in Durban, South Africa. PLoS ONE 2022, 17, e0274741. [Google Scholar] [CrossRef] [PubMed]
- Isaakidis, P.; Rangan, S.; Pradhan, A.; Ladomirska, J.; Reid, T.; Kielmann, K. ‘I cry every day’: Experiences of patients co-infected with HIV and multidrug-resistant tuberculosis. Trop. Med. Int. Health 2013, 18, 1128–1133. [Google Scholar] [CrossRef]
- Kohli, R.; Purohit, V.; Karve, L.; Bhalerao, V.; Karvande, S.; Rangan, S.; Reddy, S.; Paranjape, R.; Sahay, S. Caring for Caregivers of People Living with HIV in the Family: A Response to the HIV Pandemic from Two Urban Slum Communities in Pune, India. PLoS ONE 2012, 7, e44989. [Google Scholar] [CrossRef] [Green Version]
- Horter, S.; Stringer, B.; Greig, J.; Amangeldiev, A.; Tillashaikhov, M.N.; Parpieva, N.; Tigay, Z.; du Cros, P. Where there is hope: A qualitative study examining nuirtremainss’ adherence to multi-drug resistant tuberculosis treatment in Karakalpakstan, Uzbekistan. BMC Infect. Dis. 2016, 16, 362. [Google Scholar] [CrossRef] [Green Version]
- Daftary, A.; Mondal, S.; Zelnick, J.; Friedland, G.; Seepamore, B.; Boodhram, R.; Amico, K.R.; Padayatchi, N.; O’Donnell, M.R. Dynamic needs and challenges of people with drug-resistant tuberculosis and HIV in South Africa: A qualitative study. Lancet Glob. Health 2021, 9, e479–e488. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, B.A.; Seeley, K.; Davis, M.; Boone-Heinonen, J. Positive deviance in health and medical research on individual level outcomes—A review of methodology. Ann. Epidemiol. 2022, 69, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Babu, D.S.; John, K.R.; Babu, R. Profile of the tuberculosis patients enrolled in Nikshay portal (a web-based online portal) from Chittoor district: A monitoring tool for tuberculosis in India. DY Pat 2020, 13, 460. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology, Qualitative Research in Psychology. J. Chem. Inf. Model. 2008, 3, 77–101. [Google Scholar]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification Strategies for Establishing Reliability and Validity in Qualitative Research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Hatherall, B.; Newell, J.N.; Emmel, N.; Baral, S.C.; Khan, M.A. “Who Will Marry a Diseased Girl?” Marriage, Gender, and Tuberculosis Stigma in Asia. Qual. Health Res. 2019, 29, 1109–1119. [Google Scholar] [CrossRef] [Green Version]
- Obermeyer, C.M.; Baijal, P.; Pegurri, E. Facilitating HIV disclosure across diverse settings: A review. Am. J. Public Health 2011, 101, 1011–1023. [Google Scholar] [CrossRef]
- Zheng, Y.; Lei, F.; Liu, B. Cancer Diagnosis Disclosure and Quality of Life in Elderly Cancer Patients. Healthcare 2019, 7, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusheno, F.T.; Nguse, T.M.; Gebretekle, G.B. Assessment of Knowledge and Attitude of Tuberculosis Patients in Direct Observation Therapy Program towards Multidrug-Resistant Tuberculosis in Addis Ababa, Ethiopia: A Cross-Sectional Study. Tuberc. Res. Treat. 2020, 2020, 6475286. [Google Scholar] [CrossRef]
- Somma, D.; Thomas, B.E.; Karim, F.; Kemp, J.; Arias, N.; Auer, C.; Gosoniu, G.D.; Abouihia, A.; Weiss, M.G. Gender and socio-cultural determinants of TB-related stigma in Bangladesh, India, Malawi and Colombia. Int. J. Tuberc. Lung Dis. 2008, 12, 856–866. [Google Scholar] [PubMed]
- Muniyandi, M.; Rao, V.G.; Bhat, J.; Yadav, R.; Sharma, R.K.; Bhondeley, M.K. Health literacy on tuberculosis amongst vulnerable segment of population: Special reference to Saharia tribe in central India. Indian J. Med. Res. 2015, 141, 640–647. [Google Scholar] [CrossRef]
- Senthilingam, M.; Pietersen, E.; McNerney, R.; Te Riele, J.; Sedres, P.; Wilson, R.; Dheda, K. Lifestyle, attitudes and needs of uncured XDR-TB patients living in the communities of South Africa: A qualitative study. Trop. Med. Int. Health 2015, 20, 1155–1161. [Google Scholar] [CrossRef]
- de Jong, K.; Conijn, J.M.; Gallagher, R.A.; Reshetnikova, A.S.; Heij, M.; Lutz, M.C. Using progress feedback to improve outcomes and reduce drop-out, treatment duration, and deterioration: A multilevel meta-analysis. Clin. Psychol. Rev. 2021, 85, 102002. [Google Scholar] [CrossRef]
- Cancer Patients in Crisis Responding to Urgent Needs. Available online: https://www.rcr.ac.uk/system/files/publication/field_publication_files/Cancer_patients_crisis.pdf (accessed on 20 October 2022).
- Alexander, G.; Kanth, C.; Thomas, R. A Descriptive Study on the Users and Utility of HIV/AIDS Helpline in Karnataka, India. Indian J. Community Med. 2011, 36, 17–20. [Google Scholar] [CrossRef]
- Das, M.; Mathur, T.; Ravi, S.; Meneguim, A.C.; Iyer, A.; Mansoor, H.; Kalon, S.; Hossain, F.N.; Acharya, S.; Ferlazzo, G.; et al. Challenging drug-resistant TB treatment journey for children, adolescents and their care-givers: A qualitative study. PLoS ONE 2021, 16, e0248408. [Google Scholar] [CrossRef] [PubMed]
- Fana, T.E.; Sotana, L. Exploring the experiences of family caregivers with people with drug-resistant tuberculosis. Cogent Soc. Sci. 2021, 7, 1906494. [Google Scholar] [CrossRef]
- Frost, J.C. Support groups for medical caregivers of people with HIV diseases. Group 1994, 18, 141–153. [Google Scholar] [CrossRef]
- de Jong, R.K.; Snoek, H.; Staal, W.G.; Klip, H. The effect of patients’ feedback on treatment outcome in a child and adolescent psychiatric sample: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2019, 28, 819–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kundu, D.; Sharma, N.; Chadha, S.; Laokri, S.; Awungafac, G.; Jiang, L.; Asaria, M. Analysis of multi drug resistant tuberculosis (MDR-TB) financial protection policy: MDR-TB health insurance schemes, in Chhattisgarh state, India. Health Econ. Rev. 2018, 8, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajbhandary, S.S.; Marks, S.M.; Bock, N.N. Costs of patients hospitalized for multidrug-resistant tuberculosis. Physiol. Behav. 2004, 8, 1012–1016. [Google Scholar]
- TB Online. MDR-TB Treatment Costs 235% One’s Income: Study. Available online: https://www.tbonline.info/posts/2016/10/5/mdr-tb-treatment-costs-235-ones-income-study (accessed on 20 October 2022).
- Law, S.; Daftary, A.; O’Donnell, M.; Padayatchi, N.; Calzavara, L.; Menzies, D. Interventions to improve retention-in-care and treatment adherence among patients with drug-resistant tuberculosis: A systematic review. Eur. Respir. J. 2019, 53, 1801030. [Google Scholar] [CrossRef]
- Krska, J.; Morecroft, C.W.; Rowe, P.H.; Poole, H. Measuring the impact of long-term medicines use from the patient perspective. Int. J. Clin. Pharm. 2014, 36, 675–678. [Google Scholar] [CrossRef]
- Fredericks, J.E.; Bunting, R.F., Jr. Implementation of a patient-friendly medication schedule to improve patient safety within a healthcare system. J. Healthc. Risk Manag. 2010, 29, 22–27. [Google Scholar] [CrossRef]
- Mercurio, A. The evolving role of health educators in advancing patient safety: Forging partnerships and leading change. Health Promot. Pract. 2007, 8, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Snyman, L.; Venables, E.; Trivino Duran, L.; Mohr, E.; Azevedo, V.D.; Harmans, X.; Isaakidis, P. I didn’t know so many people cared about me: Support for patients who interrupt drug-resistant TB treatment. Int. J. Tuberc. Lung Dis. 2018, 22, 1023–1030. [Google Scholar] [CrossRef]
- Johnson, B.; Ford, D.; Abraham, M. Collaborating with patients and their families. J. Healthc. Risk Manag. 2010, 29, 15–21. [Google Scholar] [CrossRef]


{kind=link}
| Category | Characteristics | No | Average Age | Literacy | ||
|---|---|---|---|---|---|---|
| School | Illiterate | Graduate | ||||
| Patients | Male | 13 | 38 | 10 | 1 | 2 |
| Female | 7 | 34 | 5 | 1 | 1 | |
| Contacts | Male | 6 | 35 | 3 | 2 | 1 |
| Female | 14 | 50 | 8 | 3 | 3 | |
| 3.2. Main Theme-1 Emotional Issues and Social Barriers | |
|---|---|
| 3.2.1. Sub-theme-1: Fear and emotional distress due to disease status | |
| “When I was diagnosed with TB disease, I was extremely worried and fearful about my condition. I was worried and skeptical about overcoming the disease. I introspected and feared thinking, Will I be able to get through this (TB)? Will I be able to see my child once again?” | Patient (Male, aged 33 years) (Code B1) |
| “I am scared. We are going to give her to others (in terms of marriage). I wished her a speedy recovery from it (TB), as I was worried about her future. I was worried that if she could get married or not. I was scared that it might be a problem later in her life” | Caregiver (Female, 54 years, Housewife) (Code B10F) |
| 3.2.2. Sub-theme-2: Social barriers experienced due to disease status | |
| “No. I left the job soon after I was diagnosed with (TB). I was not going to work or outside because I had a severe cough and I was feeling weak and tired. Whenever I was coughing in front of them, they used to sarcastically and rudely tell, what is wrong with you? Why are you coughing so much? If you have health issues go to the hospital, don’t come here” | A patient (Male, 28 years) told (Code B5) |
| “They (people) were discussing amongst themselves; he is the pastor and his wife is suffering from this kind of disease. He has his own church and prays for so many people, but why this thing has happened to him and his family? That kind of word was hurting me and was painful”. | A female caregiver (30 years) (Code B2F) |
| 3.2.3. Sub-theme-3: Emotional distress and concerns due to patients’ physical stature | |
| “I lost weight a lot and turned pale. I was not able to go to work, I had no appetite. I use to sleep most of the time. I became very weak and lost interest in work. I lost weight from 40 to 30 kg and then to 28 kgs. During the initial stage itself, I was vomiting blood” | Patient (Female, 25 years) (Code B3) |
| “For six months, I had struggled a lot to take care of him. Then as it went on, we got used to it. Initially, for one month, he was like a bed patient, he used to feel tired and weak and always lying on the bed” | Caregiver (Female, 47 years, wife) (Code B9F) |
| 3.2.4. Sub-theme-4-: Decisive moments of breakdown | |
| “When I asked the reason, he told, I can only survive up to only 40 years. Your validity is 40 or 45 plus because of your disease condition. I went there with higher hopes but he pulled me down with no hopes left inside. I lost my mind there only…. And soon after reaching home, I decided to quit my life” | Patient (Male, 28 years) (Code B5) |
| “At that time after taking the injection, there will be a lot of difficulties sir. For two months I have to take injections daily even though it was on Sundays or holidays. For ten days I took an injection and stopped one day, again they said the injection will not work if I stopped for a day. They told me that again I have to take back all the ten days of injection. At that time my health was very weak so I lost my hope”. | Patient (Male, 28 years) (Code H5) |
| 3.3. Main Theme Medication-Related Challenges | |
|---|---|
| 3.3.1. Sub-theme-1: Adverse effects of injection | |
| “Yes, I had faced a lot of issues while taking the injections. I had severe pain, there were nodules formed at the injection site. I went through a terrible experience” | Patient (Female, 22 years) (Code B10) |
| “It was very painful to see her. I wonder how she used to take it every day as it was painful for her and even if I think about it, I used to be scared! The pain that she has undergone is unbearable. I used to cry just by looking at her injection site, and just imagine what she had gone through when she was getting it (injection) daily” | Caregiver (Female, 54 years, Mother) (Code B10F) |
| 3.3.2. Sub-theme-2: Adaptation challenges & adverse physical & psychological effects of pills | |
| “Yes, there were a lot of challenges; the most difficult and frustrating thing was consuming the tablets. Whenever I used to consume tablets, I used to vomit; the health staff had told me to consume them even after vomiting and I used to follow the same. Completing the treatment is a challenging task…. It will be 400 to 600 mg and it is difficult to swallow” … | Patient (Female, 24 years) (Code B7) |
| “It was very difficult for my husband to take those tablets because of the very high-power medicines. In those two years, he became very weak because of the tablet dosage” | Caregiver (Mother, 54 years) (Code H10F) |
| 3.4. Main Theme-3: Lack of Support and Resources | |
|---|---|
| 3.4.1. Sub-theme -1: Lack of social support and family distancing | |
| “I don’t know what to say. But in my mind, I was thinking about what has happened to me. What is there for me and why any of my friends are not coming to see me? And no one was calling me and asking how you are and what has happened to you and I use to cry at that time” | Patient (Male, 32 years) (Code H7) |
| “They came to the hospital. We told them about my condition. However, nobody helped us during our testing times. No one was bothered nor tried to help us in any way. It was very painful madam (emotional and started weeping). When I told my mother-in-law, she was least bothered” | Caregiver (Female, 47 years, Wife) (Code B9F) |
| 3.4.2. Sub-theme-2: Lack of resources | |
| “I was not able to work. I stayed at home for three months. I was managing financially by borrowing money from my dad; I also have a debt to pay back. I have requested so many times and I have borrowed approximately. Rs.1 lakh” | A patient (Male, 33 years) (Code B8) |
| “my in-law family has helped at that time. Sometimes they will give rice and sometimes they will give money to buy something like eggs and mutton. With their help only we have survived for one year, for they have helped us one complete year”. | A patient (Male, 20 years) (Code H5) |
| 3.4.3. Sub-theme-3:Lack of care at the hospital | |
| “No we did not face it. But what I think is, inviting the patients for the meetings and discussing the issues in-front of the crowd is kind of a demotivating them. Especially while conducting the survey. Once they called us for the survey saying: People who are infected with TB must come to the healthcare facility. But we did not like it, whatever it is, they are supposed to keep confidentiality and that was not the way right?” | Caregiver (Female, 23 years, living partner) (Code B5F) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagarajan, K.; Kumarsamy, K.; Begum, R.; Panibatla, V.; Reddy, R.; Adepu, R.; Munjattu, J.F.; Sellapan, S.; Arangba, S.; Goswami, A.; et al. A Dual Perspective of Psycho-Social Barriers and Challenges Experienced by Drug-Resistant TB Patients and Their Caregivers through the Course of Diagnosis and Treatment: Findings from a Qualitative Study in Bengaluru and Hyderabad Districts of South India. Antibiotics 2022, 11, 1586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111586
Nagarajan K, Kumarsamy K, Begum R, Panibatla V, Reddy R, Adepu R, Munjattu JF, Sellapan S, Arangba S, Goswami A, et al. A Dual Perspective of Psycho-Social Barriers and Challenges Experienced by Drug-Resistant TB Patients and Their Caregivers through the Course of Diagnosis and Treatment: Findings from a Qualitative Study in Bengaluru and Hyderabad Districts of South India. Antibiotics. 2022; 11(11):1586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111586
Chicago/Turabian StyleNagarajan, Karikalan, Karthikeyan Kumarsamy, Rehana Begum, Vikas Panibatla, Rameshchandra Reddy, Rajesham Adepu, Joseph Francis Munjattu, Senthil Sellapan, Stephen Arangba, Amrita Goswami, and et al. 2022. "A Dual Perspective of Psycho-Social Barriers and Challenges Experienced by Drug-Resistant TB Patients and Their Caregivers through the Course of Diagnosis and Treatment: Findings from a Qualitative Study in Bengaluru and Hyderabad Districts of South India" Antibiotics 11, no. 11: 1586. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111586