

In-Vitro and In-Vivo Antibacterial Effects of Frankincense Oil and Its Interaction with Some Antibiotics against Multidrug-Resistant Pathogens
 , , and
, , and
Abstract
:1. Introduction
2. Results
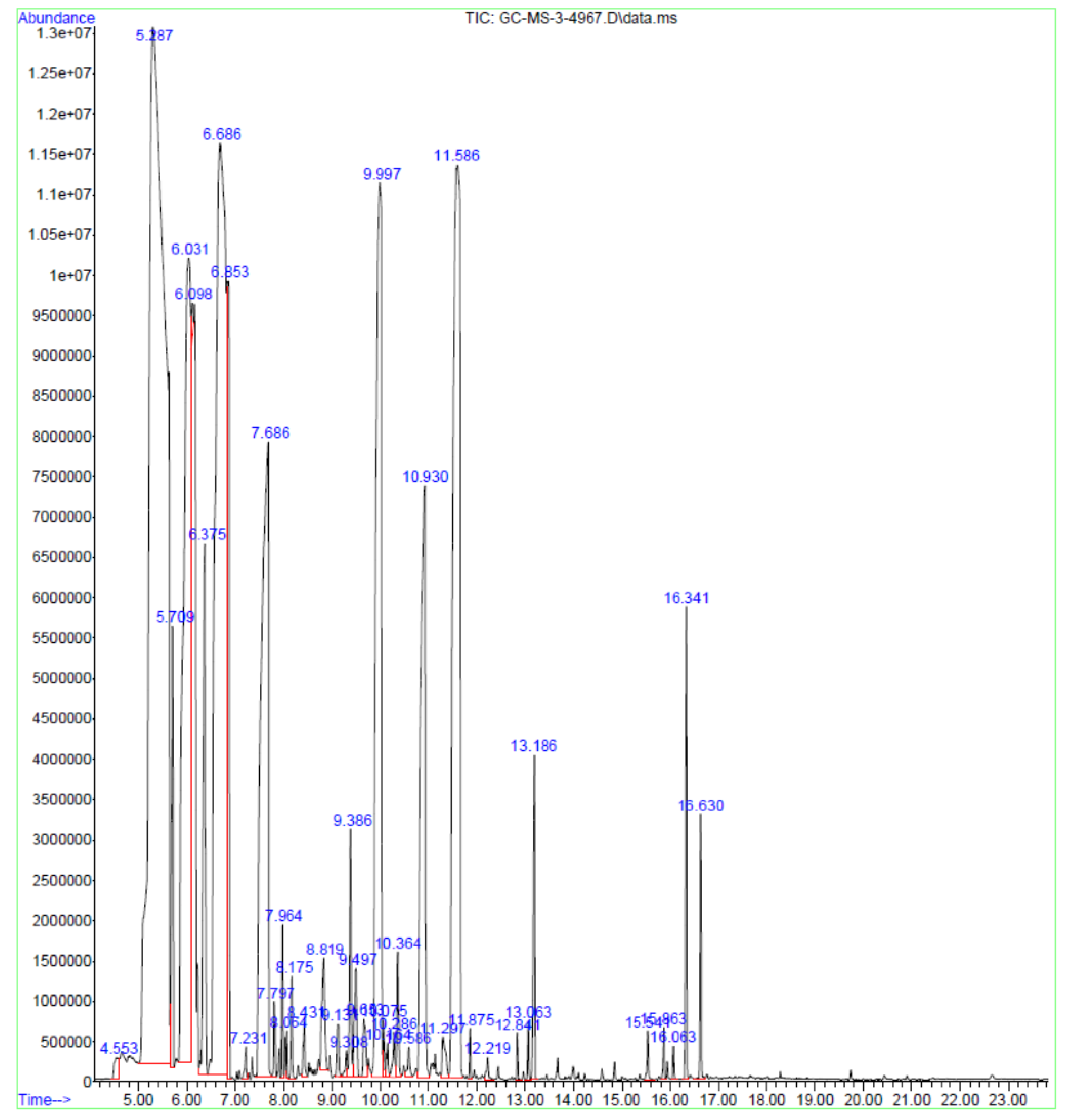
2.1. GC-MS Analysis of Frankincense Oil
2.2. Antibacterial Effect of Frankincense Oil
2.3. Interaction Study of Frankincense Oil with Antibiotics against MDR Strains
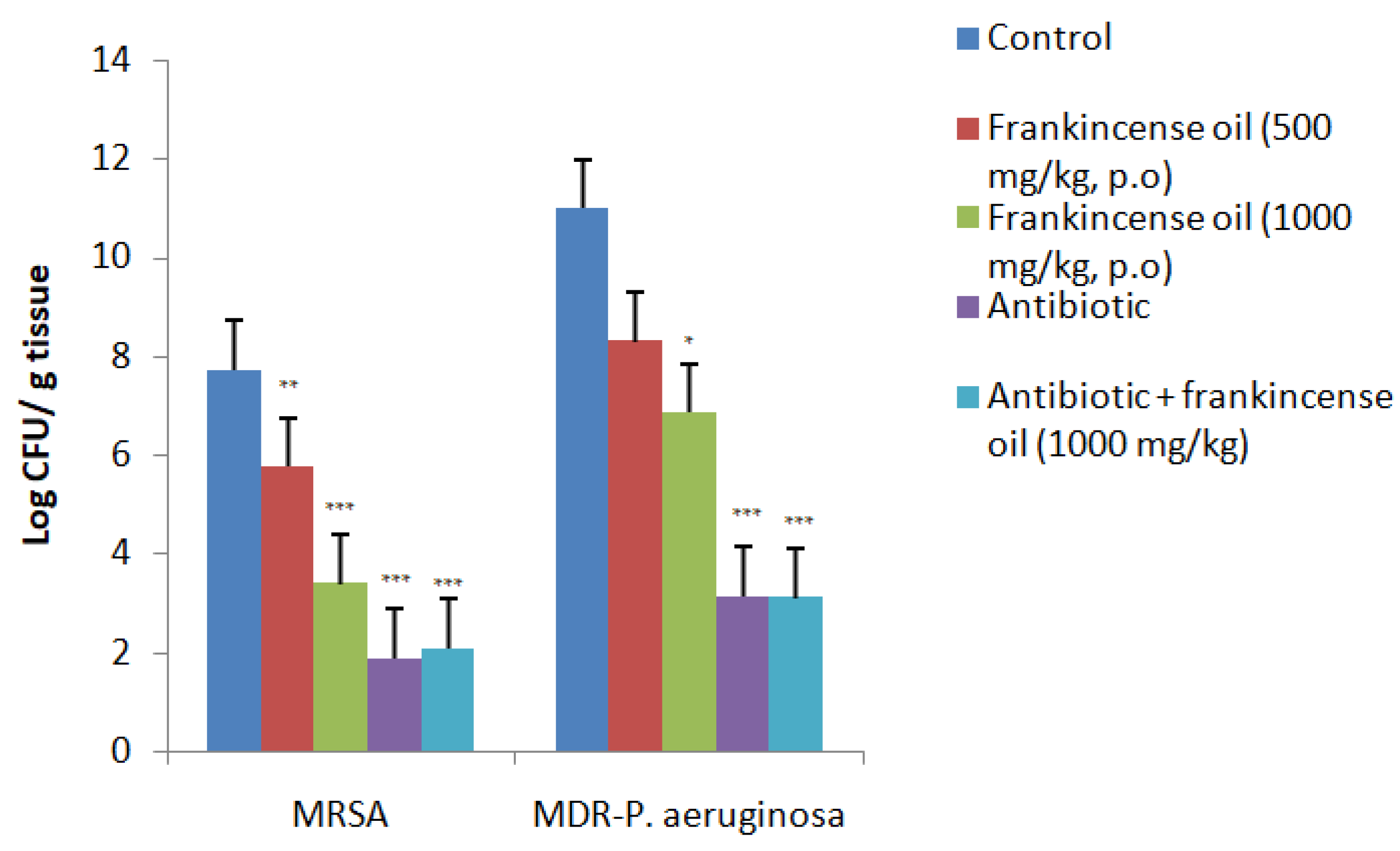
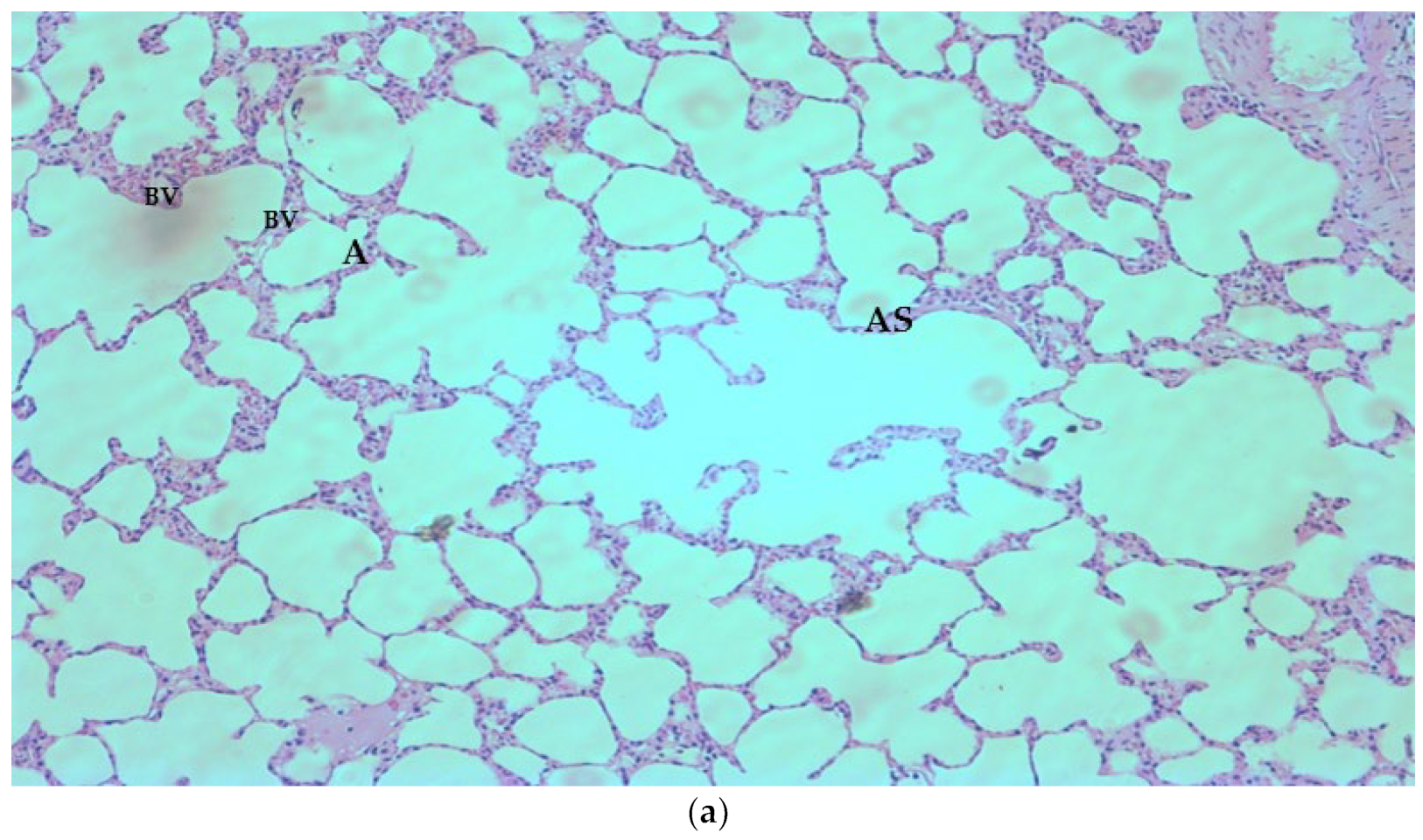
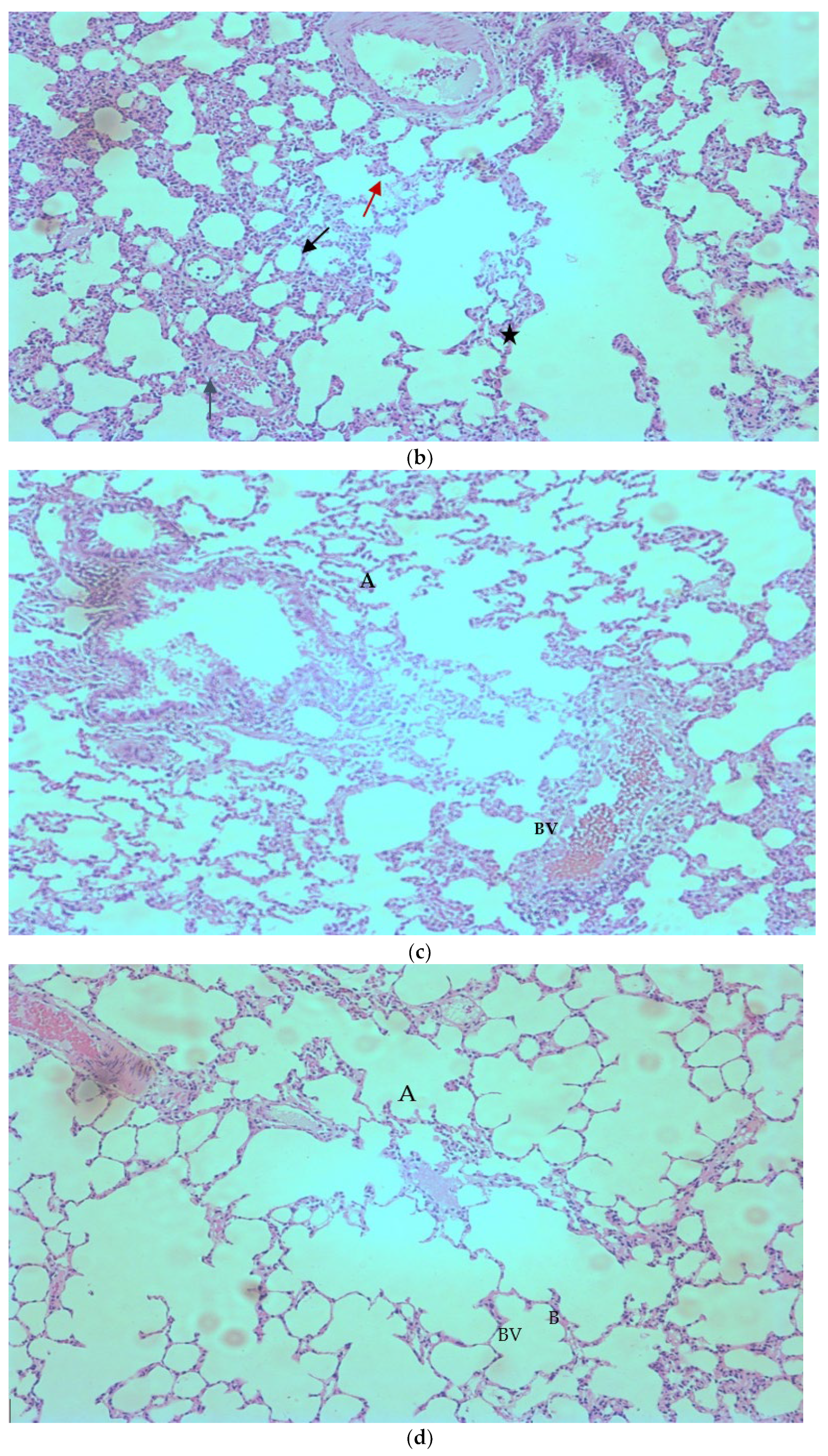
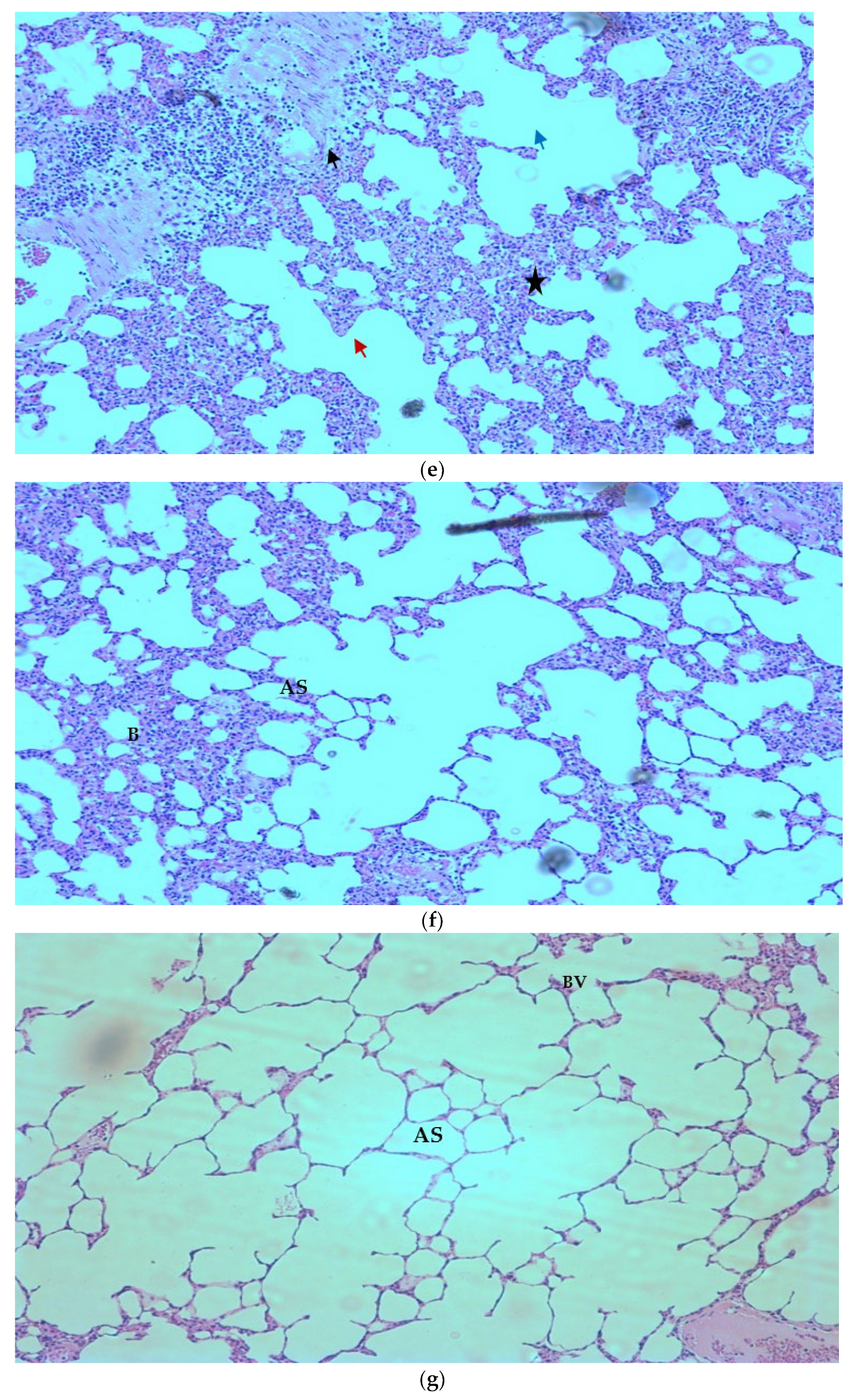
2.4. Rat Pneumonia Model (In-Vivo)
3. Discussion
4. Materials and Methods
4.1. Micro-Organisms
4.2. Animals
4.3. GC-MS Analysis of Frankincense Oil
4.4. Antibacterial Effect and Determination of MIC and MBC
4.5. Interaction Study of Frankincense Oil with Antibiotics against MDR Strains
4.6. Rat Pneumonia Model (In-Vivo)
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef] [Green Version]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiq, M.; Zeng, M.; Permana, B.; Bilal, H.; Anderson, J.; Yao, F.; Algammal, A.M.; Li, X.; Yuan, Y.; Jiao, X. Co-existence of bla NDM-5 and tet(X4) in international high-risk E. coli clone ST648 of Human origin in China. Front. Microbiol. 2022, 10, 4357. [Google Scholar] [CrossRef]
- Liu, Q.; Meng, X.; Li, Y.; Zhao, C.N.; Tang, G.Y.; Li, H. Bin Antibacterial and Antifungal Activities of Spices. Int. J. Mol. Sci. 2017, 18, 1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiq, M.; Yao, F.; Bilal, H.; Rahman, S.U.; Zeng, M.; Ali, I.; Zeng, Y.; Li, X.; Yuan, Y.; Jiao, X. Synergistic Activity of Tetrandrine and Colistin against mcr-1-Harboring Escherichia coli. Antibiotics 2022, 11, 1346. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.M.; Kong, L.C.; Liu, J.; Ma, H.X. Synergistic effect of eugenol with Colistin against clinical isolated Colistin-resistant Escherichia coli strains. Antimicrob. Resist. Infect. Control 2018, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Stefano, V.; Schillaci, D.; Cusimano, M.G.; Rishan, M.; Rashan, L. In Vitro Antimicrobial Activity of Frankincense Oils from Boswellia sacra Grown in Different Locations of the Dhofar Region (Oman). Antibiotics 2020, 9, 195. [Google Scholar] [CrossRef] [Green Version]
- Van Vuuren, S.F.; Kamatou, G.P.P.; Viljoen, A.M. Volatile composition and antimicrobial activity of twenty commercial frankincense essential oil samples. S. Afri. J. Bot. 2010, 76, 686–691. [Google Scholar] [CrossRef]
- De Rapper, S.; Van Vuuren, S.F.; Kamatou, G.P.P.; Viljoen, A.M.; Dagne, E. The additive and synergistic antimicrobial effects of select frankincense and myrrh oils—A combination from the pharaonic pharmacopoeia. Lett. Appl. Microbiol. 2012, 54, 352–358. [Google Scholar] [CrossRef]
- Lakhundi, S.; Zhang, K. Methicillin-Resistant Staphylococcus aureus: Molecular Characterization, Evolution, and Epidemiology. Clin. Microbiol. Rev. 2018, 31, e00020-18. [Google Scholar] [CrossRef]
- Kale, P.; Dhawan, B. The changing face of community-acquired methicillin-resistant Staphylococcus aureus. Indian J. Med. Microbiol. 2016, 34, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Poole, K. Pseudomonas Aeruginosa: Resistance to the Max. Front. Microbiol. 2011, 2, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breidenstein, E.B.M.; De la Fuente-Núñez, C.; Hancock, R.E.W. Pseudomonas aeruginosa: All roads lead to resistance. Trends Microbiol. 2011, 19, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Oliver, A.; Mulet, X.; López-Causapé, C.; Juan, C. The increasing threat of Pseudomonas aeruginosa high-risk clones. Drug Resist. Updat. 2015, 21, 41–59. [Google Scholar] [CrossRef]
- Fasinu, P.S.; Bouic, P.J.; Rosenkranz, B. An overview of the evidence and mechanisms of herb-drug interactions. Front. Pharmacol. 2012, 3, 69. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, M.E. Special Treatments: Constitutional Psychospiritual Points. Const. Facial Acupunct. 2014, 267–276. [Google Scholar] [CrossRef]
- Levison, M.E.; Levison, J.H. Pharmacokinetics and Pharma codynamics of Antibacterial Agents. Infect. Dis. Clin. N. Am. 2009, 23, 791. [Google Scholar] [CrossRef] [Green Version]
- Hosny, E.N.; Elhadidy, M.E.; Sawie, H.G.; Kilany, A.; Khadrawy, Y.A. Effect of frankincense oil on the neurochemical changes induced in rat model of status epilepticus. Clin. Phytoscience 2020, 61, 11. [Google Scholar] [CrossRef] [Green Version]
- Camarda, L.; Dayton, T.; Di Stefano, V.; Pitonzo, R.; Schillaci, D. Chemical composition and antimicrobial activity of some oleogum resin essential oils from Boswellia spp. (Burseraceae). Ann. Chim. 2007, 97, 837–844. [Google Scholar] [CrossRef]
- Ljaljević Grbić, M.; Unković, N.; Dimkić, I.; Janaćković, P.; Gavrilović, M.; Stanojević, O.; Stupar, M.; Vujisić, L.; Jelikić, A.; Stanković, S.; et al. Frankincense and myrrh essential oils and burn incense fume against micro-inhabitants of sacral ambients. Wisdom of the ancients? J. Ethnopharmacol. 2018, 219, 1–14. [Google Scholar] [CrossRef]
- Schillaci, D.; Arizza, V.; Dayton, T.; Camarda, L.; Di Stefano, V. In vitro anti-biofilm activity of Boswellia spp. oleogum resin essential oils. Lett. Appl. Microbiol. 2008, 47, 433–438. [Google Scholar] [CrossRef]
- Zhang, J.; Biggs, I.; Sirdaarta, J.; White, A.; Edwin Cock, I. Antibacterial and Anticancer Properties of Boswellia carteri Birdw. and Commiphora molmol Engl. Oleo-Resin Solvent Extractions. Pharmacogn. Commun. 2016, 6, 120–136. [Google Scholar] [CrossRef] [Green Version]
- Cheesman, M.J.; Ilanko, A.; Blonk, B.; Cock, I.E. Developing New Antimicrobial Therapies: Are Synergistic Combinations of Plant Extracts/Compounds with Conventional Antibiotics the Solution? Pharmacogn. Rev. 2017, 11, 57–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koohsari, H.; Ghaemi, E.A.; Sadegh Sheshpoli, M.; Jahedi, M.; Zahiri, M. The investigation of antibacterial activity of selected native plants from North of Iran. J. Med. Life 2015, 8, 38. [Google Scholar] [PubMed]
- Shaikh, A.S.; Thomas, A.B.; Chitlange, S.S. Herb–drug interaction studies of herbs used in treatment of cardiovascular disorders—A narrative review of preclinical and clinical studies. Phyther. Res. 2020, 34, 1008–1026. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.K.; Yusoff, K.; Mai, C.W.; Lim, W.M.; Yap, W.S.; Lim, S.H.E.; Lai, K.S. Additivity vs. Synergism: Investigation of the Additive Interaction of Cinnamon Bark Oil and Meropenem in Combinatory Therapy. Mol. A J. Synth. Chem. Nat. Prod. Chem. 2017, 22, 1733. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.D.; Paterna, N.J.; Senetra, A.S.; Casey, K.R.; Trieu, P.D.; Caputo, G.A.; Vaden, T.D.; Carone, B.R. Synergistic interactions of ionic liquids and antimicrobials improve drug efficacy. iScience 2021, 24, 101853. [Google Scholar] [CrossRef]
- Ocampo, P.S.; Lázár, V.; Papp, B.; Arnoldini, M.; Zur Wiesch, P.A.; Busa-Fekete, R.; Fekete, G.; Pál, C.; Ackermann, M.; Bonhoeffer, S. Antagonism between Bacteriostatic and Bactericidal Antibiotics Is Prevalent. Antimicrob. Agents Chemother. 2014, 58, 4573. [Google Scholar] [CrossRef] [Green Version]
- Cash, H.A.; Woods, D.E.; McCullough, B.; Johanson, W.G.; Bass, J.A. A rat model of chronic respiratory infection with Pseudomonas aeruginosa. Am. Rev. Respir. Dis. 1979, 119, 453–459. [Google Scholar] [CrossRef]
- Niu, H.; Yang, T.; Wang, J.; Wang, R.; Cai, Y. Immunomodulatory Effect of Colistin and its Protective Role in Rats with Methicillin-Resistant Staphylococcus aureus-induced Pneumonia. Front. Pharmacol. 2020, 11. [Google Scholar] [CrossRef]
- Chalmers, S.J.; Wylam, M.E. Methicillin-Resistant Staphylococcus aureus Infection and Treatment Options. Methods Mol. Biol. 2020, 2069, 229–251. [Google Scholar] [CrossRef] [PubMed]
- Vindhya, V.V. Sohanlal Invitro susceptibility of Imipenem by E-test in different conditions of Methicillin resistant Staphylococcus aureus. IP Int. J. Med. Microbiol. Trop. Dis. 2022, 8, 83–89. [Google Scholar] [CrossRef]
- Bassetti, M.; Vena, A.; Castaldo, N.; Righi, E.; Peghin, M. New antibiotics for ventilator-associated pneumonia. Curr. Opin. Infect. Dis. 2018, 31, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Stefani, S.; Campana, S.; Cariani, L.; Carnovale, V.; Colombo, C.; Lleo, M.M.; Iula, V.D.; Minicucci, L.; Morelli, P.; Pizzamiglio, G.; et al. Relevance of multidrug-resistant Pseudomonas aeruginosa infections in cystic fibrosis. Int. J. Med. Microbiol. 2017, 307, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Garcia, J.; Gruenberg, K.; MacDougall, C. Multidrug-Resistant Pseudomonas Infections: Hard to Treat, But Hope on the Horizon? Curr. Infect. Dis. Rep. 2018, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.J.; Jeong, S.H. Mobile Carbapenemase Genes in Pseudomonas aeruginosa. Front. Microbiol. 2021, 12, 30. [Google Scholar] [CrossRef]
- Mikhaeil, B.R.; Maatooq, G.T.; Badria, F.A.; Amer, M.M.A. Chemistry and immunomodulatory activity of frankincense oil. Zeitschrift Naturforsch.-Sect. C J. Biosci. 2003, 58, 230–238. [Google Scholar] [CrossRef]
- Başer, K.H.C.; Demirci, B.; Dekebo, A.; Dagne, E. Essential oils of some Boswellia spp., myrrh and opopanax. Flavour. Fragr. J. 2003, 18, 153–156. [Google Scholar] [CrossRef]
- Al-Harrasi, A.; Al-Saidi, S. Phytochemical analysis of the essential oil from botanically certified oleogum resin of Boswellia sacra (Omani Luban). Molecules 2008, 13, 2181–2189. [Google Scholar] [CrossRef] [Green Version]
- Al-Saidi, S.; Rameshkumar, K.B.; Hisham, A.; Sivakumar, N.; Al-Kindy, S. Composition and antibacterial activity of the essential oils of four commercial grades of Omani luban, the oleo-gum resin of Boswellia sacra FLUECK. Chem. Biodivers. 2012, 9, 615–624. [Google Scholar] [CrossRef]
- Da Silva, A.C.R.; Lopes, P.M.; De Azevedo, M.M.B.; Costa, D.C.M.; Alviano, C.S.; Alviano, D.S. Biological activities of α-pinene and β-pinene enantiomers. Molecules 2012, 17, 6290–6304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nidhi, P.; Rolta, R.; Kumar, V.; Dev, K.; Sourirajan, A. Synergistic potential of Citrus aurantium L. essential oil with antibiotics against Candida albicans. J. Ethnopharmacol. 2020, 262, 113135. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, B.C.; Queiroz, P.A.; Baldin, V.P.; Do Amaral, P.H.R.; Rodrigues, L.L.F.; Vandresen, F.; R Caleffi-Ferracioli, K.; De, L.; Scodro, R.B.; Cardoso, R.F.; et al. (-)-Camphene-based derivatives as potential antibacterial agents against Staphylococcus aureus and Enterococcus spp. Future Microbiol. 2020, 15, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Surendran, S.; Qassadi, F.; Surendran, G.; Lilley, D.; Heinrich, M. Myrcene—What Are the Potential Health Benefits of This Flavouring and Aroma Agent? Front. Nutr. 2021, 8, 400. [Google Scholar] [CrossRef] [PubMed]
- Yap, P.S.X.; Yiap, B.C.; Ping, H.C.; Lim, S.H.E. Essential oils, a new horizon in combating bacterial antibiotic resistance. Open Microbiol. J. 2014, 8, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashan, L.; White, A.; Haulet, M.; Favelin, N.; Das, P.; Cock, I.E. Chemical Composition, Antibacterial Activity, and Antibiotic Potentiation of Boswellia sacra Flueck. Oleoresin Extracts from the Dhofar Region of Oman. Evidence-Based Complement. Altern. Med. 2021, 2021, 9918935. [Google Scholar] [CrossRef] [PubMed]
- Fankam, A.G.; Kuete, V.; Voukeng, I.K.; Kuiate, J.R.; Pages, J.M. Antibacterial activities of selected Cameroonian spices and their synergistic effects with antibiotics against multidrug-resistant phenotypes. BMC Complement. Altern. Med. 2011, 11, 104. [Google Scholar] [CrossRef] [Green Version]
- Anesthesia (Guideline)|Vertebrate Animal Research. Available online: https://animal.research.uiowa.edu/iacuc-guidelines-anesthesia (accessed on 13 February 2022).
- Kandeel, M.; Abdelaziz, I.; Elhabashy, N.; Hegazy, H.; Tolba, Y. Nephrotoxicity oxidative stress of single large dose or two divided doses of gentamicin in rats. Pakistan J. Biol. Sci. 2011, 14, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Guo, P.; Zhang, S.W.; Zhang, J.; Dong, J.T.; Wu, J.D.; Tang, S.T.; Yang, J.T.; Zhang, W.J.; Wu, F. Effects of imipenem combined with low-dose cyclophosphamide on the intestinal barrier in septic rats. Exp. Ther. Med. 2018, 16, 1919. [Google Scholar] [CrossRef]
- Russo, T.A.; Davidson, B.A.; Carlino-MacDonald, U.B.; Helinski, J.D.; Priore, R.L.; Knight, P.R. The effects of Escherichia coli capsule, O-antigen, host neutrophils, and complement in a rat model of Gram-negative pneumonia. FEMS Microbiol. Lett. 2003, 226, 355–361. [Google Scholar] [CrossRef]
- Russo, T.A.; Bartholomew, L.A.; Davidson, B.A.; Helinski, J.D.; Carlino, U.B.; Knight, P.R.; Beers, M.F.; Atochina, E.N.; Notter, R.H.; Holm, B.A. Total extracellular surfactant is increased but abnormal in a rat model of gram-negative bacterial pneumonia. Am. J. Physiol. Lung Cell. Mol. Physiol. 2002, 283, L655–L663. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Name of the Constituent | RT | Area % |
|---|---|---|---|
| 1. | 4-Carene | 4.553 | 0.19 |
| 2. | α-Pinene | 5.287 | 29.31 |
| 3. | Camphene | 5.709 | 1.09 |
| 4. | β-Pinene | 6.031 | 9.75 |
| 5. | 4-Carene | 6.098 | 0.10 |
| 6. | α-Phellandrene | 6.375 | 2.29 |
| 7. | 1,3,8-p-Menthatriene | 6.686 | 15.87 |
| 8. | Limonene | 6.853 | 2.61 |
| 9. | Cycloheptene, 5-ethylidene-1-methyl | 7.231 | 0.11 |
| 10. | 1,6-Octadien-3-ol, 3,7-dimethyl- | 7.686 | 7.42 |
| 11. | Phenylethyl Alcohol | 7.797 | 0.17 |
| 12. | 1-Propanone, 1-(5-methyl-2-furanyl)- | 7.964 | 0.25 |
| 13. | cis-p-Mentha-2,8-dien-1-ol | 8.064 | 0.08 |
| 14. | Bicyclo[3.1.1]hept-3-en-2-ol, 4,6,6-trimethyl | 8.175 | 0.26 |
| 15. | Isoborneol | 8.431 | 0.16 |
| 16. | Cyclohexane, 1-butenylidene- | 8.819 | 0.56 |
| 17. | 2-Isopropenyl-5-methylhex-4-enal | 9.131 | 0.17 |
| 18. | 2-Cyclohexen-1-ol, 2-methyl-5-(1-methylethenyl)-, trans | 9.308 | 0.08 |
| 19. | 2-Methylbicyclo[4.3.0]non-1(6)-ene | 9.386 | 0.58 |
| 20. | 1H-Pyrrole-2-carboxaldehyde, 1-methyl- | 9.497 | 0.44 |
| 21. | 1,2,3,4,4a,5,6,8a-Octahydro-naphthalene | 9.653 | 0.26 |
| 22. | Isobornyl acetate | 9.997 | 8.97 |
| 23. | Camphene | 10.075 | 0.10 |
| 24. | 1,6,10,14-Hexadecatetraen-3-ol, 3,7,11,15-tetramethyl-, (E,E)- | 10.164 | 0.11 |
| 25. | Bicyclo[3.1.0]hexan-3-ol, 4-methyl-1-(1-methylethyl)-, (1.alpha., 3.beta., 4.beta., 5.alpha.)- | 10.286 | 0.14 |
| 26. | Bicyclo[4.1.0]heptan-3-ol, 4,7,7-trimethyl-, (1.alpha., 3.alpha., 4.beta., 6.alpha.)- | 10.364 | 0.34 |
| 27. | 2,6-Octadien-1-ol, 3,7-dimethyl-acetate, (Z)- | 10.586 | 0.11 |
| 28. | 2,6-Octadien-1-ol, 3,7-dimethyl-,acetate, (E)- | 10.930 | 4.70 |
| 29. | Bicyclo[7.2.0]undec-4-ene, 4,11,11-trimethyl-8-methylene- | 11.297 | 0.24 |
| 30. | Caryophyllene | 11.586 | 10.54 |
| 31. | alpha.-Caryophyllene | 11.875 | 0.09 |
| 32. | Naphthalene, 1,2,3,5,6,7,8,8a-octahydro-1,8a-dimethyl-7-(1-methylethenyl)-, [1R-(1.alpha., 7.beta., 8a.alpha.)]- | 12.219 | 0.07 |
| 33. | Caryophyllene oxide | 12.841 | 0.08 |
| 34. | Diethyl Phthalate | 13.063 | 0.10 |
| 35. | Caryophyllene oxide | 13.186 | 0.76 |
| 36. | E,E,E)-3,7,11,15-Tetramethylhexadeca-1,3,6,10,14-pentaene | 15.541 | 0.12 |
| 37. | 2,6,11,15-Tetramethyl-hexadeca-2,6,8,10,14-pentaene | 15.863 | 0.10 |
| 38. | β-Myrcene | 16.063 | 0.07 |
| 39. | 1,6,10-Dodecatriene, 7,11-dimethyl-3-methylene-, (Z)- | 16.341 | 1.11 |
| 40. | 2-Propenamide, N-(3,4-dichlorophenyl)-2-methyl- | 16.630 | 0.50 |
| Bacterial Pathogens | Fractional Inhibitory Concentration | Outcome | |||
|---|---|---|---|---|---|
| MIC Oil (µL/mL) | MIC of Ab (mg/mL) | MIC of Combination | FIC Index | ||
| MRSA ATCC 43300 | 10 | 0.002 | 0.002 | 1 | Indifference |
| P. aeruginosa ATCC 27853 | 20 | 0.004 | 0.004 | 1 | Indifference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almutairi, M.B.F.; Alrouji, M.; Almuhanna, Y.; Asad, M.; Joseph, B. In-Vitro and In-Vivo Antibacterial Effects of Frankincense Oil and Its Interaction with Some Antibiotics against Multidrug-Resistant Pathogens. Antibiotics 2022, 11, 1591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111591
Almutairi MBF, Alrouji M, Almuhanna Y, Asad M, Joseph B. In-Vitro and In-Vivo Antibacterial Effects of Frankincense Oil and Its Interaction with Some Antibiotics against Multidrug-Resistant Pathogens. Antibiotics. 2022; 11(11):1591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111591
Chicago/Turabian StyleAlmutairi, Megren Bin Faisal, Mohammed Alrouji, Yasir Almuhanna, Mohammed Asad, and Babu Joseph. 2022. "In-Vitro and In-Vivo Antibacterial Effects of Frankincense Oil and Its Interaction with Some Antibiotics against Multidrug-Resistant Pathogens" Antibiotics 11, no. 11: 1591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11111591