
Profiling the Immune Response to Periprosthetic Joint Infection and Non-Infectious Arthroplasty Failure


1
Mayo Clinic Graduate School of Biomedical Sciences, Department of Immunology, Mayo Clinic, Rochester, MN 55905, USA
2
Division of Clinical Microbiology, Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN 55905, USA
3
Division of Public Health, Infectious Diseases, and Occupational Medicine, Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA
*
Author to whom correspondence should be addressed.
Antibiotics 2023, 12(2), 296; https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12020296
Submission received: 30 December 2022
/
Revised: 20 January 2023
/
Accepted: 29 January 2023
/
Published: 1 February 2023
(This article belongs to the Special Issue Prosthetic Joint Infection: The Challenges of Prevention, Diagnosis and Treatment and Opportunities for Future Research - 2nd Volume)
Abstract
:Arthroplasty failure is a major complication of joint replacement surgery. It can be caused by periprosthetic joint infection (PJI) or non-infectious etiologies, and often requires surgical intervention and (in select scenarios) resection and reimplantation of implanted devices. Fast and accurate diagnosis of PJI and non-infectious arthroplasty failure (NIAF) is critical to direct medical and surgical treatment; differentiation of PJI from NIAF may, however, be unclear in some cases. Traditional culture, nucleic acid amplification tests, metagenomic, and metatranscriptomic techniques for microbial detection have had success in differentiating the two entities, although microbiologically negative apparent PJI remains a challenge. Single host biomarkers or, alternatively, more advanced immune response profiling-based approaches may be applied to differentiate PJI from NIAF, overcoming limitations of microbial-based detection methods and possibly, especially with newer approaches, augmenting them. In this review, current approaches to arthroplasty failure diagnosis are briefly overviewed, followed by a review of host-based approaches for differentiation of PJI from NIAF, including exciting futuristic combinational multi-omics methodologies that may both detect pathogens and assess biological responses, illuminating causes of arthroplasty failure.
1. Total Joint Arthroplasty Failure
Total joint arthroplasty is a common restorative surgery. In the United States (US), more than 1.5 million people undergo total hip arthroplasty (THA) or total knee arthroplasty (TKA) yearly and it is anticipated that numbers of arthroplasties will rise due to the aging population, high rates of obesity, and physical activity throughout the lifespan, including in later years. It has been predicted that THA and TKA procedures will grow by 137% and 601%, respectively, in the US between 2005 and 2030, resulting in more than 5 million primary THAs and TKAs and an estimated US$1.85 billion in annual hospital-related costs by 2040 [1,2,3,4,5]. A study of over 1.5 million primary TKA or THA patients from the US National Inpatient Sample found the mean age of patients undergoing primary TKA to have decreased from 68 years in 2001 to 66 years in 2011, while the mean age of those undergoing primary THA decreased from 66 years in 2001 to 65 years in 2011. In total, 64% and 56% of those in the TKA and THA groups, respectively, were women [6].
There are several reasons patients undergo joint replacement surgery. Most commonly, the procedure is in response to symptomatic osteoarthritis, followed by inflammatory arthritides, such as rheumatoid arthritis, or joint damage due to injury, tumors, or osteoporosis; regardless of underlying disease, these conditions result in pain, loss of joint mobility, and/or an overall decrease in quality of life [7,8,9,10]. In most cases, joint replacement provides dramatic pain relief and restoration of joint function, although 1 to 3% of patients require revision surgery due to complications, such as periprosthetic joint infection (PJI) or non-infectious arthroplasty failure (NIAF) [11,12,13,14,15]. As primary arthroplasty procedures increase in numbers, so do revision surgeries. It is estimated that surgical revision procedures will grow from ~130,000 annually in 2014 to ~300,000 by 2030, with an increase from ~55,000 to ~85,000 for hip and ~72,000 to more than 200,000 for knee revisions. Not only are numbers of joint revisions increasing, but the rate of revisions in younger patients, particularly those between the ages of 55 and 64, is growing, with total increases of 9.1% and 8.6% for THA and TKA, respectively, from 2002 to 2014 [16]. A 2014 retrospective study of 120,538 patients with TKAs found that, one-year post surgery, those younger than 50 years old were more likely to develop arthroplasty failure than those 65 years or older. In that study, PJI developed in 1.4% of those under 50 years of age and 0.7% in those over 65 years of age, while NIAF developed in 3.5% and 0.8%, respectively [17]. Determining the underlying cause of arthroplasty failure, whether infectious or non-infectious, and in turn, choosing a suitable treatment approach is essential, albeit difficult in some cases [9].
1.1. Periprosthetic Joint Infection
PJI occurs in ~1 to 3% of patients undergoing primary total joint arthroplasty and makes up 20% to 50% of arthroplasty failures [9,13,16,18,19,20,21]. In 1995, the National Institutes of Health (NIH) Consensus Development Panel on Total Hip Replacement described PJI as a “devastating complication” that is “challenging” to diagnose [10]; antimicrobial agents plus surgery are needed to treat it. The type of surgical intervention is based on the infecting organism(s), timing and duration of infection, and clinical presentation. For acute PJI, joint irrigation, followed by debridement, long-term antimicrobials, and implant retention (DAIR), is typical, costing around US$67,000 [22]. For non-acute cases, resection of components is characteristically necessary, either as one- or two-stage procedures. Two-stage exchange arthroplasties typically cost around US$114,000, though costs vary [9,23,24,25,26]. In all, management of PJI costs hospitals ~5-fold more than uncomplicated hip arthroplasty, totaling approximately US$2 billion per year, not including non-medical costs [5,27,28]. This cost is in addition to the individual patient burden, often including devastating morbidity, expense, impairment of quality of life, and potential loss of implanted devices, or even limbs, in extreme circumstances [9,29]. There are several risk factors associated with PJI, including obesity, smoking, and immune-disrupting disorders and their treatments, such as diabetes mellitus and rheumatoid arthritis. Men have been observed to be more prone to infection than women, although the biological underpinning for this observation is unknown [30,31,32,33,34,35,36,37,38,39,40,41].
PJI is typically caused by the formation of bacterial biofilms on device surfaces and in the surrounding tissues; biofilm formation involves the production of extracellular polymeric substances and immune-modulating products that protect microorganisms from antimicrobial agents and the host immune response [42,43,44,45,46]. Staphylococci, primarily Staphylococcus epidermidis and Staphylococcus aureus, are the most common causes, followed by polymicrobial infections, streptococci, anerobic bacteria, aerobic Gram-negative bacilli, and enterococci. In rare cases, other bacterial types, or even fungi, cause PJI (Figure 1) [9,47,48,49,50,51,52]. Culture-negative infections make up 6 to 15% of PJI cases, although rates up to 42% have been reported. Culture-negative PJI is particularly challenging due to the difficulty in selecting a treatment regimen for an unknown causative organism (which may be “over” or “under” treated) or even in classifying the joint as infected in the first place [47,53,54,55].
1.2. Non-Infectious Arthroplasty Failure
NIAF includes causes of arthroplasty failure other than infection, accounts for ~50 to 80% of arthroplasty failures and can cost upwards of US$40,000 per TKA revision and US$15,000 per THA revision [16,56,57,58]. It is typically divided into aseptic loosening, periprosthetic fracture, instability, osteolysis/adverse tissue reaction, and other/miscellaneous subgroups, with classification dependent on clinician discretion in many cases. As with arthroplasty failure due to PJI, revision surgery is often used to treat NIAF (unlike PJI, without antimicrobial treatment) [9,11,12,14,15,59,60,61,62,63,64]. Studies conducted at the Mayo Clinic in 2017 and 2019 found that the distribution of causes of NIAF of TKAs included 36% aseptic loosening, 21% periprosthetic fracture, 21% instability, 19% osteolysis, and 2% arthrofibrosis, while the distribution of causes of THA revisions for NIAF included 37% periprosthetic fracture, 26% aseptic loosening, 19% adverse tissue reaction to the device, 13% instability, and 5% other, including implant failure/stem fracture, and iliopsoas tendinitis requiring repositioning (Figure 2) [12,64].
2. Current Arthroplasty Failure Diagnostic Techniques
Despite the health and financial impact of arthroplasty failure, there are no universally accepted clinical definitions or diagnostic criteria for PJI and NIAF. Between 2001 and 2021, there was an ~30-fold increase in PubMed yearly publications for all PJI and those specifically related to PJI (Figure 3). The influx of PJI-related content and rising PJI numbers have led to several organizations, such as the Infectious Diseases Society of America (IDSA) and the Musculoskeletal Infection Society (MSIS) in 2011, International Consensus on Orthopedic Infections Meetings in 2013 and 2018, and the European Bone and Joint Infection Society (EBJIS) in 2021, to propose diagnostic guidelines, although there is constant evolution and refinement as a result of new knowledge and improving diagnostic approaches; a global consensus definition of PJI has yet to be reached [25,65,66,67,68,69]. It has been recently argued that while complex, multi-step approaches to PJI diagnosis may be useful in research settings, a single accurate differentiative assay would be most helpful in clinical practice [70]. In addition to distinguishing PJI from NIAF, an important consideration is a need to define the microbial etiology of PJI in the infected cases. Whether used in combination or as individual analyses, current diagnostic assays are primarily either microbial-based, such as traditional bacterial culture and molecular analyses, or host-based, such as histopathological evaluation and measurement of single host-based biomarkers. While able to discern PJI from NIAF in some cases, these techniques come with limitations.
2.1. Microbial-Based Diagnostic Techniques
Bacterial culture and molecular assays are traditionally used as microbial-based techniques for PJI diagnosis and pathogen identification [71]. Traditional bacterial culture consists of harvesting patient samples, such as synovial fluid, sonicate fluid (i.e., fluid generated from sonication of resected implants), and/or periprosthetic tissue, and inoculating them into or onto culture media, which are then incubated to assess for microbial growth. If microbial growth is detected, that growth is identified by additional analysis, such as matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry (MS) [71,72,73,74]. While bacterial culture remains the clinical gold standard for PJI diagnosis and allows recovery of microorganisms for antimicrobial susceptibility testing, it has limitations. Inherently, culture relies on growth in or on culture media such that inadequate growth conditions or low bacterial inocula can lead to negative results; further, culture is affected by antimicrobial usage before sampling (which is common). Due to these limitations, culture-based techniques may have imperfect sensitivity, even when infection is present. The type of sample analyzed also affects sensitivity. For example, periprosthetic tissue culture is generally less sensitive than sonicate fluid culture [73]. Contamination by extraneous microbiota may be a challenge with culture-based approaches, rendering determination as to whether isolated microorganisms are pathogens or contaminants difficult based on identity alone (e.g., S. epidermidis) in some cases. This can be overcome by culturing multiple samples (e.g., periprosthetic tissues) from each patient; recovery of the same species from more than one sample typically implies that it is a cause of infection. Time to detection is another limitation of culture-based methods; for example, anaerobic bacterial cultures are routinely incubated for 14 days prior to being reported as negative [9,75]. A 2022 study of 536 PJI patients found that the median time-to-positivity for all positive cultures was almost 3.5 days, although this was dependent on the microbial species, with S. aureus growing in the shortest mean time (1 day) and Cutibacterium acnes in the longest mean time (almost 7 days). Sample type also impacted time to results, with synovial fluid having the shortest mean time-to-positivity, followed by periprosthetic soft tissues [75].
Molecular assays, such as nucleic acid amplification tests (typically, polymerase chain reaction (PCR) assays) and those based on microbial sequencing, are increasingly used for PJI diagnosis and pathogen identification [9,71,76,77,78,79]. As molecular techniques detect microbial components and not living bacteria, they may theoretically have higher sensitivities than culture-based assays. This increased sensitivity may come with drawbacks. Similar to culture-based assays, molecular techniques may be limited by low bacterial abundance and prior antimicrobial usage. Detection of contaminants or otherwise clinically insignificant bacterial components is a limitation of molecular-based techniques. Because of the sensitivity of these techniques, microbial elements from sample contamination during harvest and/or processing or left over from previous infections may be detected, leading to erroneous results. Molecular techniques may be more expensive and have longer turnaround times than culture-based techniques, although this is not always the case. Recently, sequencing-based approaches to microbial detection, based on targeted sequencing of the 16S ribosomal RNA gene and shotgun metagenomic sequencing, have been described for PJI diagnosis, with the former being more commonly used in current clinical practice [74,80,81,82,83]. In 2022, bioMérieux received US Food and Drug Administration (FDA) authorization for the BioFire® Joint Infection Panel, which interrogates a single synovial fluid sample against a 31 microbial target panel in approximately one hour. A limitation of panel-based diagnostics is that it only detects microorganisms that are included in the panel; for example, the aforementioned panel does not include S. epidermidis, an important PJI pathogen [82]. Novel microbial-based detection techniques remain an area of interest for rapid PJI diagnosis and microbial identification.
2.2. Host-Based Diagnostic Techniques
Host-based biomarkers have been used to differentiate PJI from NIAF, beginning with the assessment of acute inflammation in periprosthetic tissue (a detailed review of which is beyond the scope of this manuscript). Elevated synovial fluid total nucleated cell count and polymorphonuclear (PMN) percentage were established as biomarkers for PJI early on (Table 1) [84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113]. Notably, time post-arthroplasty affects synovial fluid total nucleated cell count and PMN percentage; as such, the timing of sampling must be considered when interpreting results [114].
In 2019, the detection of α-defensin in synovial fluid by the lateral flow Synovasure™ PJI Test was approved by the FDA as the first FDA-approved host biomarker to aid in the detection of PJI [115,116]. α-defensin is an antimicrobial peptide primarily produced by neutrophils and macrophages and is thought to kill bacteria, fungi, and enveloped viruses by creating pores in microbial cell membranes [117,118]. The synovial fluid α-defensin lateral flow test generally exhibits good diagnostic accuracy for differentiating PJI from NIAF involving THA or TKA, with similar performance to an enzyme-linked immunosorbent assay (ELISA) [115], but performance may depend on which clinical definition for PJI is used, with lower correlation with EBJIS and IDSA, than MSIS definitions [119,120,121]. Diagnostic accuracy may be lower when analyzing arthroplasty types other than THA and TKA; for example, low sensitivity for PJI involving shoulder arthroplasties, which commonly involve Cutibacterium acnes, has been reported [122,123]. Use of synovial fluid α-defensin levels as sole indicators of PJI may be controversial [92,99,103,121,122,123,124,125,126,127,128,129]. A summary of α-defensin studies is included in Table 2 [96,98,99,102,103,104,106,115,120,121,124,126,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154].
Beyond the assessment of acute inflammation in periprosthetic tissue, synovial fluid total nucleated cell count and PMN percentage, and synovial fluid α-defensin testing, other host biomarkers across various sample types may aid in the clinical determination of infection [99,155,156,157]. For example, synovial fluid C-reactive protein (CRP), calprotectin, interleukin (Il) 6 (Il-6), leukocyte esterase (LE), or lipocalin may be assessed. A summary of synovial fluid biomarkers is included in Table 3 [88,91,92,94,96,98,99,100,101,102,104,106,107,108,111,113,144,147,148,149,153,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185]. Serum may also be evaluated by quantifying CRP, D-dimer, erythrocyte sedimentation rate (ESR), IL-6, or procalcitonin, which are often elevated in PJI [186,187,188,189,190]. With such single host biomarker assays, however, PJI diagnosis may be difficult in some cases, and information provided may be redundant between assays; further, underlying immune disorders, such as rheumatoid arthritis or other inflammatory diseases, and co-morbidities, may affect test performance [98,178,191,192,193,194,195]. While analysis of synovial fluid total nucleated cell count and polymorphonuclear percentage, and to a lesser extent, α-defensin, can be performed in most medical centers, synovial fluid testing for CRP, calprotectin, Il-6, LE, and lipocalin, may be more limited in availability.
Similar to PJI, there are no perfect assays for NIAF diagnosis. Mechanical-related failures, such as aseptic loosening and fractures, are typically diagnosed and distinguished by X-ray, though non-mechanical failures, such as instability and adverse tissue reaction, may be difficult to differentiate from PJI due to inflammatory responses at affected areas [11,12,59,60]. It has been suggested that some non-mechanical-related NIAF cases may actually represent infection [196,197,198], although recent work using culture, PCR, and deep microbial sequencing has shown that microorganisms are rarely found in NIAF [73,81,199,200,201]. Due to a lack of accurate NIAF diagnostic tools, a NIAF diagnosis may be contingent on the lack of a PJI diagnosis—that is, once arthroplasty failure is deemed to not be PJI-associated, NIAF is diagnosed. While helpful in determining whether antimicrobial treatment is necessary, the non-infectious pathogenesis underlying the failure may be unclear in such instances.
2.3. Importance of Fast and Accurate Arthroplasty Failure Diagnosis
The rise in arthroplasty procedures and the associated increase in PJI and NIAF, alongside the status of PJI diagnostics, justify the development of improved diagnostic techniques to differentiate PJI from NIAF and subsets within. Determining whether arthroplasty failure is due to PJI or NIAF and the causative organism, if infection is present, is important for selecting ideal management. As previously mentioned, results from currently used diagnostics may result in ambiguous classification, and in such cases, patients may receive unnecessarily broad-spectrum antimicrobial treatment or, alternatively, treatment that does not treat the actual cause of the arthroplasty failure. Unnecessary antimicrobial treatment may cause dysbiosis and drug-associated toxicity, in addition to aiding in the selection and expansion of antimicrobial-resistant bacteria, which is leading to dramatic effects on global health [53,202,203].
In 2022, the Antimicrobial Resistance Collaborators published an article estimating that 5 million deaths in 2019 worldwide were associated with bacterial antimicrobial resistance, although the full impact of antimicrobial resistance remains unknown due to the lack of global tracking systems. Methicillin-resistant S. aureus, an important cause of PJI, was a leading cause of death associated with antimicrobial resistance, resulting in more than 100,000 deaths in 2019 [204]. The World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) have included antimicrobial-resistant S. aureus on their Priority Pathogen and Urgent Threat lists, respectively, due to its impact on global health [205,206]. S. epidermidis, an important PJI pathogen, is associated with high rates of methicillin resistance. The CDC reported a greater than 15% increase in antimicrobial-resistant bacterial-associated infections and deaths in hospitals in 2020, possibly attributed to weakened infection prevention protocols and/or the usage of antibacterial agents during the COVID-19 pandemic [207].
These findings highlight the growing global crisis of antimicrobial resistance and illustrate the imperative of accurate and specific diagnoses of infectious diseases. Developing novel diagnostic techniques to differentiate PJI from NIAF and inform targeted antimicrobial usage will aid in patient management and in antimicrobial stewardship efforts, which will, in turn, assist in the fight against antimicrobial resistance globally.
3. Detailed Immune Response Profiling for Arthroplasty Failure Diagnosis
While evaluating individual host biomarkers may allow differentiation of PJI and NIAF in many instances, there remain cases that are clinically challenging to classify; expanded understanding as to how the full human immune system reacts during arthroplasty failure may provide insights into future diagnostic and possibly treatment opportunities. Immune profiling allows differentiation of PJI and NIAF, and may potentially identify subsets thereof, even in the context of inflammation related to surgical procedures or underlying inflammatory conditions. Recently, advances in multi-omics techniques have allowed a detailed characterization of the host immune response during PJI and NIAF (Figure 4).
3.1. Transcriptomic Immune Profiling
Transcriptomic analyses, such as RT-PCR and RNA-sequencing, have been conducted to interrogate the immune microenvironment during PJI and assess its potential impact on local bone and joint health. Transcriptomic studies performed on periprosthetic tissues from PJI show, unsurprisingly, that elevated expression of antimicrobial and immune cell activation genes dominates the immune response. In arthroplasty studies targeting specific transcripts, those associated with neutrophil activation, such as calprotectin, and IL-8, and macrophage inflammatory transcripts, such as chemokine (C-X-C motif) ligand (CXCL) 2 (CXCL2), and chemokine (C-C motif) ligand (CCL) 3 (CCL3), are elevated in PJI and associated with bone degeneration through bone-resorbing osteoclast generation, as well as induction of osteoblast inflammatory cytokine production [190,208,209]. Another targeted transcriptomic study of PJI-associated periprosthetic tissues found elevated levels of granulocyte colony-stimulating factor (G-CSF), IL-1β, IL-6, IL-8, and CD40L at infection sites [210]. In other targeted studies, levels of inflammatory mediators, such as toll-like receptor 2 (TLR-2), CCL2, presepsin, and osteopontin (OPN), were elevated in the serum of patients with PJI [186,211]. Of note, the last two are candidate biomarkers for sepsis diagnosis [212,213]. In addition to novel findings, many studies recapitulate antimicrobial-related inflammatory biomarkers already used in PJI diagnosis, such as α-defensin, IL-6, and D-dimer.
Untargeted transcriptomic analysis of sonicate fluid from PJI patients has also been conducted. In a 2022 study by Masters et al., sonicate fluid from hip and knee arthroplasty failures underwent RNA sequencing; overall differentially expressed gene (DEG) profiling separated PJI and NIAF samples by principal component analysis (PCA). Pathway analysis found elevated DEGs to be primarily related to host defense, immune response, and cellular development and repair of canonical pathways. In all, 28 previously described potential PJI biomarkers and three novel potential biomarkers, including CCL20, coagulation factor F7, and Fc receptor-like 4 (FCRL4), were elevated in PJI compared to NIAF [214].
3.2. Proteomic Immune Profiling
Proteomic analyses of PJI and NIAF samples have also been conducted to assess the functional output of the immune response during arthroplasty failure and investigate its potential diagnostic use. Proteomic, similar to transcriptomic, profiling of arthroplasty failure, found that the local immune response during PJI is primarily driven by elevated antimicrobial inflammatory proteins, while the proteome of NIAF samples is more related to tissue homeostasis and wound healing. For example, targeted proteomic immunoassays conducted on synovial fluid have found neutrophil elastase (ELA-2), bactericidal/permeability-increasing protein (BPI), lipocalin, lactotransferrin, thrombospondin, IL-1β, IL-10, IL-1α, lactate, interferon (IFN)γ, IL-5, and IL-17A to be elevated in PJI compared to NIAF [102,107,147,184]. The diagnostic accuracy of α-defensin, CRP, IL-6, and LE were unsurprisingly recapitulated. Expression of the antimicrobial complement cascade of proteins has also been studied in synovial fluid using multiplex immunoassay. Complement proteins C1q, C3b/C3i, C4b, C5, C5a, MBL, and properdin were elevated in the PJI compared to NIAF. Individually, C1q was most able to differentiate PJI from NIAF, although the combination of elevated C1q, C3b/C3i, C4b, C5, C5a, and MBL was most predictive of PJI [215].
Recently, we reported the characterization of the proteome of 200 sonicate fluid samples using a 92-target inflammatory protein panel not specifically designed for PJI [216]. Sixteen proteins were elevated in PJI, including CCL20, oncostatin M, extracellular newly identified receptor for advanced glycation end products binding protein (EN-RAGE), IL-6, IL-1α, IL-8, CXCL5, CXCL1, CXCL6, leukemia inhibitory factor (LIF), IL-17A, tumor necrosis factor (TNF), matrix metallopeptidase 1 (MMP-1), IFNγ, IL-18R1, and CCL4, and 21 proteins were elevated in NIAF, including macrophage-colony stimulating factor (CSF-1), osteoprotegerin, Flt3L, AXIN1, TNF-like weak inducer of apoptosis (TWEAK), TNF receptor superfamily member 9 (TNFRSF9), monocyte chemoattractant protein (MCP) 1 (MCP-1), complement C1r/C1s, Uegf, Bmp1 domain containing protein 1 (CDCP1), Skp, Cullin, F-box containing complex (SCF complex), eukaryotic translation initiation factor 4E (eIF4E)-binding protein 1 (4E-BP1), TNF-related activation-induced cytokine (TRANCE), CD40, MMP-10, sulfotransferase family 1A member 1 (ST1A1), MCP-4, IL-18, hepatocyte growth factor (HGF), IL-10RB, CCL3, signal transducing adaptor molecule binding protein binding protein (STAMBP), and CXCL10 [216]. While individual proteins were moderately to mildly predictive of PJI vs. NIAF (the most predictive being CCL20), a combination of elevated CCL20 and IL-8 and lowered MCP-1 and CCL3 was highly predictive. PCA differentially separated PJI and NIAF samples by overall proteomic profile. In addition to comparing all PJI to all NIAF samples, samples within PJI and NIAF subgroups were compared. Although proteomic profiling with the small panel studied was unable to detect differences between staphylococcal vs. non-staphylococcal PJI, or between aseptic loosening, instability, stiffness, osteolysis, or other causes of NIAF, two proteins were differentially expressed when comparing causative species of PJI, with elevated IL-17A in S. aureus compared to S. epidermidis and Staphylococcus lugdunensis-associated PJI, and elevated CCL11 in S. epidermidis compared to S. aureus and Streptococcus agalactiae-associated PJI [216]. These results, generated with a small protein panel, justify more extensive proteomic analyses of PJI with a view to determining whether more comprehensive proteomic profiles might be able to point to specific underlying potential PJI-causing pathogens.
To preliminarily characterize the proteome during PJI and NIAF in an untargeted manner, a subset of four S. aureus-associated PJI and four NIAF sonicate fluid samples that had undergone analysis using the 92-target inflammatory protein panel above [216] were analyzed using liquid chromatography with tandem mass spectrometry (LC-MS/MS) [217]. Of 810 proteins quantified, 35 were differentially abundant in S. aureus PJI and NIAF samples. PCA differentially separated the overall proteomic profiles of S. aureus PJI and NIAF sonicate fluid samples. Gene ontology pathway analysis found S. aureus PJI to be associated with elevated proteins in microbial defense response pathways, specifically those related to neutrophil degranulation and activation. Proteins within molecular function pathways related to endopeptidase and peptidase activity, transition metal and iron ion binding, and TLR and receptor for advanced glycation endproducts (RAGE) receptor binding were also elevated in PJI compared to NIAF. In all, fifteen proteins were elevated in PJI, including lactotransferrin, lipocalin, myeloperoxidase, calprotectin A8 and A9 subunits, cathepsin G, neutrophil elastase (ELA-2), eosinophil cationic protein (RNASE3), endoplasmic reticulum to nucleus signaling 1 (ERN1), matrix metalloproteinase-9 (MMP-9), lysozyme C, haptoglobin, lamin-B1, glycogen phosphorylase, liver form (PYGL), leucine-rich α-2-glycoprotein (LRG1). Twenty proteins were elevated in NIAF, including cartilage acidic protein 1 (CRTAC1), melanoma cell adhesion molecule (MCAM), IFI30 lysosomal thiol reductase (IFI30), osteopontin, β-hexosaminidase subunit β (HEXB), proteoglycan 4, pancreatic ribonuclease (RNASE1), dermcidin, CD44, annexin A2, serpin B6, branched-chain-amino-acid aminotransferase (BCAT1), dihydrolipoamide S-succinyltransferase (DLST), shock protein β-1 (HSPB1), early endosome antigen 1 (EEA1), collagen α-2(I) chain (COL1A2), fatty acid-binding protein, epidermal (FABP5), fructose-1,6-bisphosphatase 1 (FBP1), fatty acid-binding protein, heart (FABP3), and cathepsin D [217].
3.3. Cellular Immune Profiling
While the elevation of leukocytes, particularly neutrophils, is well-established in PJI, a robust understanding of the cellular profile during PJI is still being investigated. Cellularity profiling has primarily been conducted using synovial fluid and periprosthetic tissue. Due to the effects of processing, direct cellularity studies are limited when using sonicate fluid. To circumvent this, the transcriptomic results from the previously described Masters et al., 2022 bulk RNA-sequencing study on sonicate fluid were subjected to bioinformatic cellular deconvolution using CIBERSORTx [214,218]. Cellular deconvolution allows cellular analysis by “unmixing” bulk transcriptomic data to generate predicted cellularity profiles, in this case, made of 22 specific cell-types. Cellularity profiles created by CIBERSORTx are differentially clustered by PCA between PJI and NIAF. The differentiation of PJI and NIAF by predicted cellularity profiling was mainly separated by roles during inflammation—that is, cell types important for antimicrobial immunity were elevated in PJI, while NIAF populations were primarily composed of immune cells involved in tissue homeostasis and repair. In all, predicted total granulocyte, neutrophils, activated mast cells, CD8+ T cells, eosinophils, resting NK cells, activated CD4+ memory T cells were elevated in PJI, with predicted total macrophages/monocytes, M0 macrophages, M2 macrophages, total B cells, plasma cells, regulatory T cells, naïve B cells, and follicular helper T cells elevated in NIAF. Total granulocytes, neutrophils, and activated mast cells were most predictive of PJI from NIAF [218].
While it is known that infiltrating neutrophils are elevated during PJI, the role of mast cells during arthroplasty failure is uncharacterized. Tissue-resident mast cells have been described as “sentinel cells” able to detect microbial insults and initiate downstream antimicrobial inflammation by recruiting neutrophils and presenting bacterial antigens to the adaptive immune response, in additional to killing bacteria through secretion of antimicrobial peptides [219,220]. Activation of joint-specific mast cells has been linked to the induction of rheumatoid arthritis and increased joint inflammation during osteoarthritis and arthrofibrosis [174,221,222,223]. As such, it could be reasoned that mast cells may play a role in antimicrobial host defense during PJI. Further investigation of the possible presence of this cell type in PJI is needed.
Findings from cellular deconvolution analysis of sonicate fluid have been largely recapitulated by results of flow cytometry experiments on synovial fluid and periprosthetic tissue. Anti-bacterial granulocytes, primarily driven by neutrophils and eosinophils, NK cells, and monocytes, were elevated in PJI vs. NIAF synovial fluid samples [224]. Similar to findings in synovial fluid, macrophages and monocytes were elevated in PJI-associated compared to NIAF periprosthetic tissues.
Although not normally characterized as an immune cell type, elevated platelets have been reported in the blood of patients with PJI; their diagnostic usefulness remains controversial [225,226,227]. There have been conflicting reports regarding the presence of T cells in arthroplasty failure, with findings ranging from lower or no to increased T cells in PJI compared to NIAF [210,224]. Whether, and if, T cells play a role during arthroplasty failure warrants future investigation. It has been suggested that the inflammatory response to bacterial biofilms during PJI may lead the recruitment of anti-inflammatory myeloid-derived suppressor cells (MDSCs) to the joint, leading to immune response suppression and downstream chronic infection. Recruitment of MDSCs to the joint is elevated during PJI, likely due to the production of Il-12 by the host or of lactate and ATP synthase by certain biofilms themselves. Recruitment of MDSCs leads to the suppression of antimicrobial phagocyte recruitment and inhibits bacterial clearance [210,224,228,229,230]. The role of MDSCs in arthroplasty failure is an area for future research.
3.4. Limitations of Immune Profiling for Arthroplasty Failure Diagnosis
In addition to the limitations of each individual technique to profile immune response during arthroplasty failure, there are limits associated with detailed immune profiling and its overall potential diagnostic use. At this time, virtually all studies profiling immune response during arthroplasty failure have been conducted as research studies. Though some results may portend future clinical use, when and whether these techniques can be validated for clinical use is unknown. Cohort sizes have been relatively small, with limited comorbidities addressed. As such, whether currently identified immune profiles will be recapitulated in larger, more diverse clinical populations is unknown. These studies have typically been conducted on samples from patients with clear PJI or NIAF diagnoses. It is unknown how these approaches will perform in more challenging to diagnose cases, the very cases where improved diagnostics are needed. The logistics of conducting multi-omics analyses may also be problematic in clinical scenarios. Currently, these techniques and the necessary bioinformatic analyses are expensive and time-consuming. Prices of multi-omics analyses may decrease over time; the introduction of individualized medical tools, including personalized computational diagnostics, may become commonplace in the future.
A selection of cofactors—most not-yet-investigated—that may be relevant to accurate and reproducible results when assessing the immune response during arthroplasty failure is shown in Table 4. These variables may be important to note when planning, conducting, and analyzing the results of immune response profiling studies. Ways in which such variables impact immune responses to arthroplasty failure remain largely unexplored. As advanced multi-omic analyses develop, it will be interesting to investigate the clinical and diagnostic impact of these variables and their interactions.
4. The Future of PJI and NIAF Diagnostics
Multi-omics techniques to characterize immune response during arthroplasty failure represent a novel approach to potential future diagnosis of PJI and NIAF. While approaches described here differentiate PJI from NIAF, none have been discriminatory enough to define the underlying infectious organism(s) or cause of non-infectious failure, topics that deserve further study. Host-based diagnostics are not necessarily replacements for microbial-based detection tools, but will likely, instead, complement them. Complex bioinformatic tools, in combination with computational techniques, such as machine learning and artificial intelligence, are at the cutting edge of individualized diagnostics [231,232,233,234]. Advanced computational studies have already been conducted to better understand their potential use in PJI prediction [235,236,237,238]. These tools may be useful for addressing the current limitations of host-based profiling and synthesizing descriptive diagnostic readouts from multi-omics results in the future. Simultaneous assessment of host response and microorganism detection may allow single diagnostic reports to determine causative pathogen(s) and assess biological responses, providing insight into underlying key inflammatory etiologies and informing precision treatment (Figure 5). Continued development of tools to detect causes of arthroplasty failure remains a challenge that warrants ongoing collaborative investigation.
Author Contributions
Conceptualization, C.R.F. and R.P.; investigation, C.R.F.; writing—original draft preparation, C.R.F. and R.P.; writing—review and editing, C.R.F. and R.P.; visualization, C.R.F.; supervision, R.P. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number NIH R01 AR056647. C.R.F. was supported by the Mayo Clinic Graduate School of Biomedical Sciences and the Ph.D. Training Grant in Basic Immunology (NIH T32 AI07425-25). This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
R.P. reports grants from ContraFect, TenNor Therapeutics Limited, and BioFire. R.P. is a consultant to Next Gen Diagnostics, PathoQuest, PhAST, Torus Biosystems, Day Zero Diagnostics, Mammoth Biosciences, CARBX, HealthTrackRx, and Netflix. Mayo Clinic and R.P. have a relationship with Adaptive Phage Therapeutics. R.P. has a patent on Bordetella pertussis/parapertussis PCR issued, a patent on a device/method for sonication with royalties paid by Samsung to Mayo Clinic, and a patent on an anti-biofilm substance issued. R.P. receives honoraria from the National Board of Medical Examiners, Up-to-Date, and the Infectious Diseases Board Review Course.
References
- Patel, R. Periprosthetic joint infection. N. Engl. J. Med. 2023, 388, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Premkumar, A.; Kolin, D.A.; Farley, K.X.; Wilson, J.M.; McLawhorn, A.S.; Cross, M.B.; Sculco, P.K. Projected economic burden of periprosthetic joint infection of the hip and knee in the United States. J. Arthroplast. 2021, 36, 1484–1489.e1483. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of total joint replacement in the United States: Future projections to 2020–2040 using the national inpatient sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J. Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef] [PubMed]
- Hilibrand, A.S.; Rubin, L.E.; Grauer, J.N. Geographic variations and trends in primary and revision knee and total hip arthroplasties in the United States. J. Bone Surg. 2020, 5, e0051. [Google Scholar] [CrossRef] [PubMed]
- Pivec, R.; Johnson, A.J.; Mears, S.C.; Mont, M.A. Hip arthroplasty. Lancet 2012, 380, 1768–1777. [Google Scholar] [CrossRef]
- Nilsdotter, A.K.; Toksvig-Larsen, S.; Roos, E.M. A 5 year prospective study of patient-relevant outcomes after total knee replacement. Osteoarthr. Cartil. 2009, 17, 601–606. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Murray, D.G. Total hip replacement. J. Am. Med. Assoc. 1995, 273, 1950–1956. [Google Scholar] [CrossRef]
- Gausden, E.B.; Cross, W.W., 3rd; Mabry, T.M.; Pagnano, M.W.; Berry, D.J.; Abdel, M.P. Total hip arthroplasty for femoral neck fracture: What are the contemporary reasons for failure? J. Arthroplast. 2021, 36, S272–S276. [Google Scholar] [CrossRef]
- Ledford, C.K.; Perry, K.I.; Hanssen, A.D.; Abdel, M.P. What are the contemporary etiologies for revision surgery and revision after primary, noncemented total hip arthroplasty? J. Am. Acad. Orthop. Surg. 2019, 27, 933–938. [Google Scholar] [CrossRef]
- Kenney, C.; Dick, S.; Lea, J.; Liu, J.; Ebraheim, N.A. A systematic review of the causes of failure of revision total hip arthroplasty. J. Orthop. 2019, 16, 393–395. [Google Scholar] [CrossRef]
- Mathis, D.T.; Lohrer, L.; Amsler, F.; Hirschmann, M.T. Reasons for failure in primary total knee arthroplasty—An analysis of prospectively collected registry data. J. Orthop. 2021, 23, 60–66. [Google Scholar] [CrossRef]
- Kelmer, G.; Stone, A.H.; Turcotte, J.; King, P.J. Reasons for revision: Primary total hip arthroplasty mechanisms of failure. J. Am. Acad. Orthop. Surg. 2021, 29, 78–87. [Google Scholar] [CrossRef]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L., Jr. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35, S79–S85. [Google Scholar] [CrossRef]
- Meehan, J.P.; Danielsen, B.; Kim, S.H.; Jamali, A.A.; White, R.H. Younger age is associated with a higher risk of early periprosthetic joint infection and aseptic mechanical failure after total knee arthroplasty. J. Bone Jt. Surg. Am. 2014, 96, 529–535. [Google Scholar] [CrossRef]
- Zimmerli, W. Infection and musculoskeletal conditions: Prosthetic-joint-associated infections. Best Pract. Res. Clin. Rheumatol. 2006, 20, 1045–1063. [Google Scholar] [CrossRef]
- Trampuz, A.; Widmer, A.F. Infections associated with orthopedic implants. Curr. Opin. Infect. Dis. 2006, 19, 349–356. [Google Scholar] [CrossRef]
- Kim, K.T.; Lee, S.; Ko, D.O.; Seo, B.S.; Jung, W.S.; Chang, B.K. Causes of failure after total knee arthroplasty in osteoarthritis patients 55 years of age or younger. Knee Surg. Relat. Res. 2014, 26, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Postler, A.; Lutzner, C.; Beyer, F.; Tille, E.; Lutzner, J. Analysis of total knee arthroplasty revision causes. BMC Musculoskelet. Disord. 2018, 19, 55. [Google Scholar] [CrossRef] [PubMed]
- Peel, T.N.; Dowsey, M.M.; Buising, K.L.; Liew, D.; Choong, P.F. Cost analysis of debridement and retention for management of prosthetic joint infection. Clin. Microbiol. Infect. 2013, 19, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kuzyk, P.R.; Dhotar, H.S.; Sternheim, A.; Gross, A.E.; Safir, O.; Backstein, D. Two-stage revision arthroplasty for management of chronic periprosthetic hip and knee infection: Techniques, controversies, and outcomes. J. Am. Acad. Orthop. Surg. 2014, 22, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Renz, N.; Trampuz, A. Management of periprosthetic joint infection. Hip. Pelvis. 2018, 30, 138–146. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef]
- Wixted, C.M.; Charalambous, L.T.; Kim, B.I.; Cochrane, N.H.; Belay, E.S.; Joseph, H.L.; Seyler, T.M. Direct costs vary by outcome in two-stage revision arthroplasty for the treatment of hip periprosthetic joint infection. Arthroplast. Today 2023, 19, 101061. [Google Scholar] [CrossRef]
- Bozic, K.J.; Ries, M.D. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J. Bone Jt. Surg. Am. 2005, 87, 1746–1751. [Google Scholar] [CrossRef]
- Bozic, K.J.; Katz, P.; Cisternas, M.; Ono, L.; Ries, M.D.; Showstack, J. Hospital resource utilization for primary and revision total hip arthroplasty. J. Bone Jt. Surg. Am. 2005, 87, 570–576. [Google Scholar] [CrossRef]
- Akindolire, J.; Morcos, M.W.; Marsh, J.D.; Howard, J.L.; Lanting, B.A.; Vasarhelyi, E.M. The economic impact of periprosthetic infection in total hip arthroplasty. Can. J. Surg. 2020, 63, E52–E56. [Google Scholar] [CrossRef]
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic joint infection: The incidence, timing, and predisposing factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [Green Version]
- Namba, R.S.; Inacio, M.C.; Paxton, E.W. Risk factors associated with surgical site infection in 30,491 primary total hip replacements. J. Bone Jt. Surg. Br. 2012, 94, 1330–1338. [Google Scholar] [CrossRef]
- Namba, R.S.; Inacio, M.C.; Paxton, E.W. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: An analysis of 56,216 knees. J. Bone Jt. Surg. Am. 2013, 95, 775–782. [Google Scholar] [CrossRef]
- Malinzak, R.A.; Ritter, M.A.; Berend, M.E.; Meding, J.B.; Olberding, E.M.; Davis, K.E. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J. Arthroplast. 2009, 24, 84–88. [Google Scholar] [CrossRef]
- Dowsey, M.M.; Choong, P.F.M. Obese diabetic patients are at substantial risk for deep infection after primary TKA. Clin. Orthop. Relat. R 2009, 467, 1577–1581. [Google Scholar] [CrossRef]
- Peersman, G.; Laskin, R.; Davis, J.; Peterson, M. Infection in total knee replacement: A retrospective review of 6489 total knee replacements. Clin. Orthop. Relat. Res. 2001, 392, 15–23. [Google Scholar] [CrossRef]
- Peel, T.N.; Dowsey, M.M.; Daffy, J.R.; Stanley, P.A.; Choong, P.F.; Buising, K.L. Risk factors for prosthetic hip and knee infections according to arthroplasty site. J. Hosp. Infect. 2011, 79, 129–133. [Google Scholar] [CrossRef]
- Dowsey, M.M.; Choong, P.F.M. Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty. Clin. Orthop. Relat. R 2008, 466, 153–158. [Google Scholar] [CrossRef]
- Berbari, E.F.; Hanssen, A.D.; Duffy, M.C.; Steckelberg, J.M.; Ilstrup, D.M.; Harmsen, W.S.; Osmon, D.R. Risk factors for prosthetic joint infection: Case-control study. Clin. Infect. Dis. 1998, 27, 1247–1254. [Google Scholar] [CrossRef]
- Berbari, E.F.; Osmon, D.R.; Lahr, B.; Eckel-Passow, J.E.; Tsaras, G.; Hanssen, A.D.; Mabry, T.; Steckelberg, J.; Thompson, R. The Mayo prosthetic joint infection risk score: Implication for surgical site infection reporting and risk stratification. Infect. Control. Hosp. Epidemiol. 2012, 33, 774–781. [Google Scholar] [CrossRef]
- Bongartz, T.; Halligan, C.S.; Osmon, D.R.; Reinalda, M.S.; Bamlet, W.R.; Crowson, C.S.; Hanssen, A.D.; Matteson, E.L. Incidence and risk factors of prosthetic joint infection after total hip or knee replacement in patients with rheumatoid arthritis. Arthritis Rheum. 2008, 59, 1713–1720. [Google Scholar] [CrossRef] [Green Version]
- Jamsen, E.; Huhtala, H.; Puolakka, T.; Moilanen, T. Risk factors for infection after knee arthroplasty. A register-based analysis of 43,149 cases. J. Bone Jt. Surg. Am. 2009, 91, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Arciola, C.R.; Campoccia, D.; Montanaro, L. Implant infections: Adhesion, biofilm formation and immune evasion. Nat. Rev. Microbiol. 2018, 16, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Schilcher, K.; Horswill, A.R. Staphylococcal biofilm development: Structure, regulation, and treatment strategies. Microbiol. Mol. Biol. Rev. 2020, 84, e00026-00019. [Google Scholar] [CrossRef] [PubMed]
- Gries, C.M.; Kielian, T. Staphylococcal biofilms and immune polarization during prosthetic joint infection. J. Am. Acad. Orthop. Surg. 2017, 25 (Suppl. 1), S20–S24. [Google Scholar] [CrossRef]
- Ricciardi, B.F.; Muthukrishnan, G.; Masters, E.; Ninomiya, M.; Lee, C.C.; Schwarz, E.M. Staphylococcus aureus evasion of host immunity in the setting of prosthetic joint infection: Biofilm and beyond. Curr. Rev. Musculoskelet. Med. 2018, 11, 389–400. [Google Scholar] [CrossRef]
- Masters, E.A.; Ricciardi, B.F.; Bentley, K.L.M.; Moriarty, T.F.; Schwarz, E.M.; Muthukrishnan, G. Skeletal infections: Microbial pathogenesis, immunity and clinical management. Nat. Rev. Microbiol. 2022, 20, 385–400. [Google Scholar] [CrossRef]
- Del Pozo, J.L.; Patel, R. Infection associated with prosthetic joints. N. Engl. J. Med. 2009, 361, 787–794. [Google Scholar] [CrossRef]
- Gross, C.E.; Della Valle, C.J.; Rex, J.C.; Traven, S.A.; Durante, E.C. Fungal periprosthetic joint infection: A review of demographics and management. J. Arthroplast. 2021, 36, 1758–1764. [Google Scholar] [CrossRef]
- Nace, J.; Siddiqi, A.; Talmo, C.T.; Chen, A.F. Diagnosis and management of fungal periprosthetic joint infections. J. Am. Acad. Orthop. Surg. 2019, 27, e804–e818. [Google Scholar] [CrossRef]
- Tai, D.B.G.; Patel, R.; Abdel, M.P.; Berbari, E.F.; Tande, A.J. Microbiology of hip and knee periprosthetic joint infections: A database study. Clin. Microbiol. Infect. 2022, 28, 255–259. [Google Scholar] [CrossRef]
- Marculescu, C.E.; Berbari, E.F.; Cockerill, F.R., 3rd; Osmon, D.R. Unusual aerobic and anaerobic bacteria associated with prosthetic joint infections. Clin. Orthop. Relat. Res. 2006, 451, 55–63. [Google Scholar] [CrossRef]
- Flurin, L.; Greenwood-Quaintance, K.E.; Patel, R. Microbiology of polymicrobial prosthetic joint infection. Diagn. Microbiol. Infect. Dis. 2019, 94, 255–259. [Google Scholar] [CrossRef]
- Palan, J.; Nolan, C.; Sarantos, K.; Westerman, R.; King, R.; Foguet, P. Culture-negative periprosthetic joint infections. EFORT Open Rev. 2019, 4, 585–594. [Google Scholar] [CrossRef]
- Berbari, E.F.; Marculescu, C.; Sia, I.; Lahr, B.D.; Hanssen, A.D.; Steckelberg, J.M.; Gullerud, R.; Osmon, D.R. Culture-negative prosthetic joint infection. Clin. Infect Dis. 2007, 45, 1113–1119. [Google Scholar] [CrossRef]
- Hersh, B.L.; Shah, N.B.; Rothenberger, S.D.; Zlotnicki, J.P.; Klatt, B.A.; Urish, K.L. Do culture negative periprosthetic joint infections remain culture negative? J. Arthroplast. 2019, 34, 2757–2762. [Google Scholar] [CrossRef]
- Okafor, C.; Hodgkinson, B.; Nghiem, S.; Vertullo, C.; Byrnes, J. Cost of septic and aseptic revision total knee arthroplasty: A systematic review. BMC Musculoskelet. Disord. 2021, 22, 706. [Google Scholar] [CrossRef]
- Lavernia, C.; Lee, D.J.; Hernandez, V.H. The increasing financial burden of knee revision surgery in the United States. Clin. Orthop. Relat. Res. 2006, 446, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Klouche, S.; Sariali, E.; Mamoudy, P. Total hip arthroplasty revision due to infection: A cost analysis approach. Orthop. Traumatol.-Sur. 2010, 96, 124–132. [Google Scholar] [CrossRef]
- Salmons, H.I.; Fruth, K.M.; Lewallen, D.G.; Trousdale, R.T.; Berry, D.J.; Abdel, M.P. Revision total hip arthroplasty for aseptically failed metal-on-metal hip resurfacing arthroplasty. J. Arthroplast. 2022, 37, 2399–2405. [Google Scholar] [CrossRef] [PubMed]
- Cottino, U.; Sculco, P.K.; Sierra, R.J.; Abdel, M.P. Instability after total knee arthroplasty. Orthop. Clin. N. Am. 2016, 47, 311–316. [Google Scholar] [CrossRef]
- Owen, A.R.; Tibbo, M.E.; van Wijnen, A.J.; Pagnano, M.W.; Berry, D.J.; Abdel, M.P. Acquired idiopathic stiffness after contemporary total knee arthroplasty: Incidence, risk factors, and results over 25 years. J. Arthroplast. 2021, 36, 2980–2985. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.; Deschamps, G.; Neyret, P.; Chambat, P. Revision in non-infected total knee arthroplasty: An analysis of 69 consecutive cases. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2000, 86, 694–706. [Google Scholar]
- Athanasou, N.A. The pathobiology and pathology of aseptic implant failure. Bone Jt. Res. 2016, 5, 162–168. [Google Scholar] [CrossRef]
- Abdel, M.P.; Ledford, C.K.; Kobic, A.; Taunton, M.J.; Hanssen, A.D. Contemporary failure aetiologies of the primary, posterior-stabilised total knee arthroplasty. Bone Jt. J. 2017, 99, 647–652. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J. Arthroplast. 2018, 33, 1309–1314.e1302. [Google Scholar] [CrossRef]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebse, R. The EBJIS definition of periprosthetic joint infection. Bone Jt. J. 2021, 103, 18–25. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Infection, I.C.G.o.P.J. Definition of periprosthetic joint infection. J. Arthroplast. 2014, 29, 1331. [Google Scholar] [CrossRef]
- Shohat, N.; Bauer, T.; Buttaro, M.; Budhiparama, N.; Cashman, J.; Della Valle, C.J.; Drago, L.; Gehrke, T.; Gomes, L.S.M.; Goswami, K. Hip and knee section, what is the definition of a periprosthetic joint infection (PJI) of the knee and the hip? Can the same criteria be used for both joints?: Proceedings of international consensus on orthopedic infections. J. Arthroplast. 2019, 34, S325–S327. [Google Scholar] [CrossRef] [PubMed]
- Sigmund, I.K.; Luger, M.; Windhager, R.; McNally, M.A. Diagnosing periprosthetic joint infections: A comparison of infection definitions: EBJIS 2021, ICM 2018, and IDSA 2013. Bone Jt. Res. 2022, 11, 608–618. [Google Scholar] [CrossRef]
- Deirmengian, C.; McLaren, A.; Higuera, C.; Levine, B.R. Physician use of multiple criteria to diagnose periprosthetic joint infection may be less accurate than the use of an individual test. Cureus 2022, 14, e31418. [Google Scholar] [CrossRef]
- Higgins, E.; Suh, G.A.; Tande, A.J. Enhancing diagnostics in orthopedic infections. J. Clin. Microbiol. 2022, 60, e0219621. [Google Scholar] [CrossRef] [PubMed]
- Peel, T.N.; Dylla, B.L.; Hughes, J.G.; Lynch, D.T.; Greenwood-Quaintance, K.E.; Cheng, A.C.; Mandrekar, J.N.; Patel, R. Improved diagnosis of prosthetic joint infection by culturing periprosthetic tissue specimens in blood culture bottles. mBio 2016, 7, e01776-01715. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Piper, K.E.; Jacobson, M.J.; Hanssen, A.D.; Unni, K.K.; Osmon, D.R.; Mandrekar, J.N.; Cockerill, F.R.; Steckelberg, J.M.; Greenleaf, J.F.; et al. Sonication of removed hip and knee prostheses for diagnosis of infection. N. Engl. J. Med. 2007, 357, 654–663. [Google Scholar] [CrossRef]
- Yin, H.; Xu, D.; Wang, D. Diagnostic value of next-generation sequencing to detect periprosthetic joint infection. BMC Musculoskelet. Disord. 2021, 22, 252. [Google Scholar] [CrossRef]
- Tarabichi, S.; Goh, G.S.; Zanna, L.; Qadiri, Q.S.; Baker, C.M.; Gehrke, T.; Citak, M.; Parvizi, J. Time to positivity of cultures obtained for periprosthetic joint infection. J. Bone Jt. Surg. 2023, 105, 107–112. [Google Scholar] [CrossRef]
- Gomez, E.; Cazanave, C.; Cunningham, S.A.; Greenwood-Quaintance, K.E.; Steckelberg, J.M.; Uhl, J.R.; Hanssen, A.D.; Karau, M.J.; Schmidt, S.M.; Osmon, D.R.; et al. Prosthetic joint infection diagnosis using broad-range PCR of biofilms dislodged from knee and hip arthroplasty surfaces using sonication. J. Clin. Microbiol. 2012, 50, 3501–3508. [Google Scholar] [CrossRef]
- Melendez, D.P.; Uhl, J.R.; Greenwood-Quaintance, K.E.; Hanssen, A.D.; Sampath, R.; Patel, R. Detection of prosthetic joint infection by use of PCR-electrospray ionization mass spectrometry applied to synovial fluid. J. Clin. Microbiol. 2014, 52, 2202–2205. [Google Scholar] [CrossRef]
- Melendez, D.P.; Greenwood-Quaintance, K.E.; Berbari, E.F.; Osmon, D.R.; Mandrekar, J.N.; Hanssen, A.D.; Patel, R. Evaluation of a genus- and group-specific rapid PCR assay panel on synovial fluid for diagnosis of prosthetic knee infection. J. Clin. Microbiol. 2016, 54, 120–126. [Google Scholar] [CrossRef]
- Ryu, S.Y.; Greenwood-Quaintance, K.E.; Hanssen, A.D.; Mandrekar, J.N.; Patel, R. Low sensitivity of periprosthetic tissue PCR for prosthetic knee infection diagnosis. Diagn. Microbiol. Infect. Dis. 2014, 79, 448–453. [Google Scholar] [CrossRef]
- Ivy, M.I.; Thoendel, M.J.; Jeraldo, P.R.; Greenwood-Quaintance, K.E.; Hanssen, A.D.; Abdel, M.P.; Chia, N.; Yao, J.Z.; Tande, A.J.; Mandrekar, J.N.; et al. Direct detection and identification of prosthetic joint infection pathogens in synovial fluid by metagenomic shotgun sequencing. J. Clin. Microbiol. 2018, 56, e00402-00418. [Google Scholar] [CrossRef]
- Thoendel, M.J.; Jeraldo, P.R.; Greenwood-Quaintance, K.E.; Yao, J.Z.; Chia, N.; Hanssen, A.D.; Abdel, M.P.; Patel, R. Identification of prosthetic joint infection pathogens using a shotgun metagenomics approach. Clin. Infect. Dis. 2018, 67, 1333–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azad, M.A.; Wolf, M.J.; Strasburg, A.P.; Daniels, M.L.; Starkey, J.C.; Donadio, A.D.; Abdel, M.P.; Greenwood-Quaintance, K.E.; Patel, R. Comparison of the BioFire joint infection panel to 16S ribosomal RNA gene-based targeted metagenomic sequencing for testing synovial fluid from patients with knee arthroplasty failure. J. Clin. Microbiol. 2022, 1, e0112622. [Google Scholar] [CrossRef] [PubMed]
- Flurin, L.; Hemenway, J.J.; Fisher, C.R.; Vaillant, J.J.; Azad, M.; Wolf, M.J.; Greenwood-Quaintance, K.E.; Abdel, M.P.; Patel, R. Clinical use of a 16S ribosomal RNA gene-based Sanger and/or next generation sequencing assay to test preoperative synovial fluid for periprosthetic joint infection diagnosis. mBio 2022, 1, e0132222. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.B.; Fehring, T.K.; Odum, S.M.; Griffin, W.L.; Nussman, D.S. The value of white blood cell counts before revision total knee arthroplasty. J. Arthroplast. 2003, 18, 1038–1043. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Hanssen, A.D.; Osmon, D.R.; Mandrekar, J.; Steckelberg, J.M.; Patel, R. Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am. J. Med. 2004, 117, 556–562. [Google Scholar] [CrossRef]
- Zmistowski, B.; Restrepo, C.; Huang, R.; Hozack, W.J.; Parvizi, J. Periprosthetic joint infection diagnosis: A complete understanding of white blood cell count and differential. J. Arthroplast. 2012, 27, 1589–1593. [Google Scholar] [CrossRef]
- Dinneen, A.; Guyot, A.; Clements, J.; Bradley, N. Synovial fluid white cell and differential count in the diagnosis or exclusion of prosthetic joint infection. Bone Jt. J. 2013, 95, 554–557. [Google Scholar] [CrossRef]
- Wyles, C.C.; Larson, D.R.; Houdek, M.T.; Sierra, R.J.; Trousdale, R.T. Utility of synovial fluid aspirations in failed metal-on-metal total hip arthroplasty. J. Arthroplast. 2013, 28, 818–823. [Google Scholar] [CrossRef]
- Gallo, J.; Juranova, J.; Svoboda, M.; Zapletalova, J. Excellent AUC for joint fluid cytology in the detection/exclusion of hip and knee prosthetic joint infection. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2017, 161, 310–319. [Google Scholar] [CrossRef]
- Higuera, C.A.; Zmistowski, B.; Malcom, T.; Barsoum, W.K.; Sporer, S.M.; Mommsen, P.; Kendoff, D.; Della Valle, C.J.; Parvizi, J. Synovial fluid cell count for diagnosis of chronic periprosthetic hip infection. J. Bone Jt. Surg. Am. 2017, 99, 753–759. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, J.G.; Jang, K.M.; Han, S.B.; Lim, H.C.; Bae, J.H. Diagnostic value of synovial white blood cell count and serum C-reactive protein for acute periprosthetic joint infection after knee arthroplasty. J. Arthroplast. 2017, 32, 3724–3728. [Google Scholar] [CrossRef]
- Lee, Y.S.; Koo, K.H.; Kim, H.J.; Tian, S.; Kim, T.Y.; Maltenfort, M.G.; Chen, A.F. Synovial fluid biomarkers for the diagnosis of periprosthetic joint infection: A systematic review and meta-analysis. J. Bone Jt. Surg. Am. 2017, 99, 2077–2084. [Google Scholar] [CrossRef]
- Shahi, A.; Parvizi, J. The role of biomarkers in the diagnosis of periprosthetic joint infection. EFORT Open Rev. 2017, 1, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Sousa, R.; Serrano, P.; Gomes Dias, J.; Oliveira, J.C.; Oliveira, A. Improving the accuracy of synovial fluid analysis in the diagnosis of prosthetic joint infection with simple and inexpensive biomarkers: C-reactive protein and adenosine deaminase. Bone Jt. J. 2017, 99, 351–357. [Google Scholar] [CrossRef]
- Balato, G.; Franceschini, V.; Ascione, T.; Lamberti, A.; Balboni, F.; Baldini, A. Diagnostic accuracy of synovial fluid, blood markers, and microbiological testing in chronic knee prosthetic infections. Arch. Orthop. Trauma. Surg. 2018, 138, 165–171. [Google Scholar] [CrossRef]
- De Vecchi, E.; Romano, C.L.; De Grandi, R.; Cappelletti, L.; Villa, F.; Drago, L. Alpha defensin, leukocyte esterase, C-reactive protein, and leukocyte count in synovial fluid for pre-operative diagnosis of periprosthetic infection. Int. J. Immunopathol. Pharmacol. 2018, 32, 2058738418806072. [Google Scholar] [CrossRef]
- Kuo, F.C.; Lu, Y.D.; Wu, C.T.; You, H.L.; Lee, G.B.; Lee, M.S. Comparison of molecular diagnosis with serum markers and synovial fluid analysis in patients with prosthetic joint infection. Bone Jt. J. 2018, 100, 1345–1351. [Google Scholar] [CrossRef]
- Tahta, M.; Simsek, M.E.; Isik, C.; Akkaya, M.; Gursoy, S.; Bozkurt, M. Does inflammatory joint diseases affect the accuracy of infection biomarkers in patients with periprosthetic joint infections? A prospective comparative reliability study. J. Orthop. Sci. 2019, 24, 286–289. [Google Scholar] [CrossRef]
- Carli, A.V.; Abdelbary, H.; Ahmadzai, N.; Cheng, W.; Shea, B.; Hutton, B.; Sniderman, J.; Philip Sanders, B.S.; Esmaeilisaraji, L.; Skidmore, B.; et al. Diagnostic accuracy of serum, synovial, and tissue testing for chronic periprosthetic joint infection after hip and knee replacements: A systematic review. J. Bone Jt. Surg. Am. 2019, 101, 635–649. [Google Scholar] [CrossRef]
- Dijkman, C.; Thomas, A.R.; Koenraadt, K.L.M.; Ermens, A.A.M.; van Geenen, R.C.I. Synovial neutrophilic gelatinase-associated lipocalin in the diagnosis of periprosthetic joint infection after total knee arthroplasty. Arch. Orthop. Trauma Surg. 2020, 140, 941–947. [Google Scholar] [CrossRef]
- Mihalic, R.; Zdovc, J.; Brumat, P.; Trebse, R. Synovial fluid interleukin-6 is not superior to cell count and differential in the detection of periprosthetic joint infection. Bone Jt Open 2020, 1, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Ivy, M.; Block, D.R.; Abdel, M.P.; Hanssen, A.D.; Beauchamp, C.; Perry, K.I.; Rosemark, C.L.; Greenwood-Quaintance, K.E.; Mandrekar, J.; et al. Comparative analysis of 23 synovial fluid biomarkers for hip and knee periprosthetic joint infection detection. J. Orthop. Res. 2020, 38, 2664–2674. [Google Scholar] [CrossRef] [PubMed]
- Ivy, M.I.; Sharma, K.; Greenwood-Quaintance, K.E.; Tande, A.J.; Osmon, D.R.; Berbari, E.F.; Mandrekar, J.; Beauchamp, C.P.; Hanssen, A.D.; Abdel, M.P.; et al. Synovial fluid alpha defensin has comparable accuracy to synovial fluid white blood cell count and polymorphonuclear percentage for periprosthetic joint infection diagnosis. Bone Jt. J. 2021, 103, 1119–1126. [Google Scholar] [CrossRef]
- Levent, A.; Neufeld, M.E.; Piakong, P.; Lausmann, C.; Gehrke, T.; Citak, M. Which International Consensus Meeting preoperative minor criteria is the most accurate marker for the diagnosis of periprosthetic joint infection in hip and knee arthroplasty? J. Arthroplast. 2021, 36, 3728–3733. [Google Scholar] [CrossRef] [PubMed]
- Van den Kieboom, J.; Tirumala, V.; Xiong, L.; Klemt, C.; Kwon, Y.M. Concomitant hip and knee periprosthetic joint infection in periprosthetic fracture: Diagnostic utility of serum and synovial fluid markers. J. Arthroplast. 2021, 36, 722–727. [Google Scholar] [CrossRef]
- Baker, C.M.; Goh, G.S.; Tarabichi, S.; Shohat, N.; Parvizi, J. Synovial c-reactive protein is a useful adjunct for diagnosis of periprosthetic joint infection. J. Arthroplast. 2022, 37, 2437–2443.e2431. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, Z.; Li, M.; Li, W.; Fang, X.; Zhang, W. Synovial fluid neutrophil gelatinase-associated lipocalin can be used to accurately diagnose prosthetic joint infection. Int. J. Infect. Dis. 2022, 123, 170–175. [Google Scholar] [CrossRef]
- Lazic, I.; Burdach, A.; Pohlig, F.; von Eisenhart-Rothe, R.; Suren, C. Utility of synovial calprotectin lateral flow test to exclude chronic prosthetic joint infection in periprosthetic fractures: A prospective cohort study. Sci. Rep. 2022, 12, 18385. [Google Scholar] [CrossRef]
- Dilley, J.E.; Seetharam, A.; Meneghini, R.M.; Kheir, M.M. Synovial fluid absolute neutrophil count and neutrophil-to-lymphocyte ratio are not superior to polymorphonuclear percentage in detecting periprosthetic joint infection. J. Arthroplast. 2023, 38, 146–151. [Google Scholar] [CrossRef]
- Qin, L.; Hu, N.; Li, X.; Chen, Y.; Wang, J.; Huang, W. Evaluation of synovial fluid neutrophil CD64 index as a screening biomarker of prosthetic joint infection. Bone Jt. J. 2020, 102, 463–469. [Google Scholar] [CrossRef]
- Qin, L.; Li, X.; Wang, J.; Gong, X.; Hu, N.; Huang, W. Improved diagnosis of chronic hip and knee prosthetic joint infection using combined serum and synovial IL-6 tests. Bone Jt. Res. 2020, 9, 587–592. [Google Scholar] [CrossRef]
- Wang, H.; Qin, L.; Wang, J.; Huang, W. Synovial fluid IL-1beta appears useful for the diagnosis of chronic periprosthetic joint infection. J. Orthop. Surg. Res. 2021, 16, 144. [Google Scholar] [CrossRef]
- Qin, L.; Wang, H.; Zhao, C.; Chen, C.; Chen, H.; Li, X.; Wang, J.; Hu, N.; Huang, W. Serum and synovial biomarkers for distinguishing between chronic periprosthetic joint infections and rheumatoid arthritis: A prospective cohort study. J. Arthroplast. 2022, 37, 342–346. [Google Scholar] [CrossRef]
- Christensen, C.P.; Bedair, H.; Della Valle, C.J.; Parvizi, J.; Schurko, B.; Jacobs, C.A. The natural progression of synovial fluid white blood-cell counts and the percentage of polymorphonuclear cells after primary total knee arthroplasty: A multicenter study. J. Bone Jt. Surg. Am. 2013, 95, 2081–2087. [Google Scholar] [CrossRef]
- Deirmengian, C.; Madigan, J.; Kallur Mallikarjuna, S.; Conway, J.; Higuera, C.; Patel, R. Validation of the alpha defensin lateral flow test for periprosthetic joint infection. J. Bone Jt. Surg. Am. 2021, 103, 115–122. [Google Scholar] [CrossRef]
- Pupaibool, J.; Fulnecky, E.J.; Swords, R.L., Jr.; Sistrunk, W.W.; Haddow, A.D. Alpha-defensin-novel synovial fluid biomarker for the diagnosis of periprosthetic joint infection. Int. Orthop. 2016, 40, 2447–2452. [Google Scholar] [CrossRef]
- White, S.H.; Wimley, W.C.; Selsted, M.E. Structure, function, and membrane integration of defensins. Curr. Opin. Struct. Biol. 1995, 5, 521–527. [Google Scholar] [CrossRef]
- Xu, D.; Lu, W. Defensins: A double-edged sword in host immunity. Front. Immunol. 2020, 11, 764. [Google Scholar] [CrossRef]
- Huard, M.; Detrembleur, C.; Poilvache, H.; Pastor, Y.G.I.; Van Cauter, M.; Driesen, R.; Yombi, J.C.; Neyt, J.; Cornu, O. Alpha defensin: A diagnostic accuracy depending on the infection definition used. J. Arthroplast. 2020, 35, 1355–1360. [Google Scholar] [CrossRef]
- Renz, N.; Yermak, K.; Perka, C.; Trampuz, A. Alpha defensin lateral flow test for diagnosis of periprosthetic joint infection: Not a screening but a confirmatory test. J. Bone Jt. Surg. Am. 2018, 100, 742–750. [Google Scholar] [CrossRef]
- Sigmund, I.K.; Yermak, K.; Perka, C.; Trampuz, A.; Renz, N. Is the enzyme-linked immunosorbent assay more accurate than the lateral flow alpha defensin test for diagnosing periprosthetic joint infection? Clin. Orthop. Relat. R 2018, 476, 1645. [Google Scholar] [CrossRef] [PubMed]
- Unter Ecker, N.; Koniker, A.; Gehrke, T.; Salber, J.; Zahar, A.; Hentschke, M.; Citak, M. What is the diagnostic accuracy of alpha-defensin and leukocyte esterase test in periprosthetic shoulder infection? Clin. Orthop. Relat. R 2019, 477, 1712. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, L.; Plate, A.; Stadler, L.; Sutter, R.; Frustaci, D.; Zbinden, R.; Zingg, P.O.; Gerber, C.; Achermann, Y. Alpha-defensin lateral flow test does not appear to be useful in predicting shoulder periprosthetic joint infections. Int. Orthop. 2020, 44, 1023–1029. [Google Scholar] [CrossRef]
- Balato, G.; Dall'Anese, R.; Balboni, F.; Ascione, T.; Pezzati, P.; Bartolini, G.; Quercioli, M.; Baldini, A. Synovial fluid alpha-defensin in periprosthetic knee infection workup: Liquid chromatography-mass spectrometry detection of alpha-defensin in synovial fluid. Bone Jt. J. 2022, 104, 1047–1051. [Google Scholar] [CrossRef]
- Suen, K.; Keeka, M.; Ailabouni, R.; Tran, P. Synovasure 'quick test' is not as accurate as the laboratory-based alpha-defensin immunoassay: A systematic review and meta-analysis. Bone Jt. J. 2018, 100, 66–72. [Google Scholar] [CrossRef]
- Gehrke, T.; Lausmann, C.; Citak, M.; Bonanzinga, T.; Frommelt, L.; Zahar, A. The accuracy of the alpha defensin lateral flow device for diagnosis of periprosthetic joint infection: Comparison with a gold standard. J. Bone Jt. Surg. Am. 2018, 100, 42–48. [Google Scholar] [CrossRef]
- Eriksson, H.K.; Nordström, J.; Gabrysch, K.; Hailer, N.P.; Lazarinis, S. Does the alpha-defensin immunoassay or the lateral flow test have better diagnostic value for periprosthetic joint infection? A systematic review. Clin. Orthop. Relat. R 2018, 476, 1065. [Google Scholar] [CrossRef]
- Kuiper, J.W.P.; Verberne, S.J.; Vos, S.J.; van Egmond, P.W. Does the alpha defensin ELISA test perform better than the alpha defensin lateral flow test for PJI diagnosis? A systematic review and meta-analysis of prospective studies. Clin. Orthop. Relat. Res. 2020, 478, 1333–1344. [Google Scholar] [CrossRef]
- Kleeman-Forsthuber, L.T.; Johnson, R.M.; Brady, A.C.; Pollet, A.K.; Dennis, D.A.; Jennings, J.M. Alpha-defensin offers limited utility in routine workup of periprosthetic joint infection. J. Arthroplast. 2021, 36, 1746–1752. [Google Scholar] [CrossRef]
- Bingham, J.; Clarke, H.; Spangehl, M.; Schwartz, A.; Beauchamp, C.; Goldberg, B. The alpha defensin-1 biomarker assay can be used to evaluate the potentially infected total joint arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 4006–4009. [Google Scholar] [CrossRef]
- Kasparek, M.F.; Kasparek, M.; Boettner, F.; Faschingbauer, M.; Hahne, J.; Dominkus, M. Intraoperative diagnosis of periprosthetic joint infection using a novel alpha-defensin lateral flow assay. J. Arthroplast. 2016, 31, 2871–2874. [Google Scholar] [CrossRef]
- Sigmund, I.K.; Holinka, J.; Gamper, J.; Staats, K.; Bohler, C.; Kubista, B.; Windhager, R. Qualitative alpha-defensin test (Synovasure) for the diagnosis of periprosthetic infection in revision total joint arthroplasty. Bone Jt. J. 2017, 99, 66–72. [Google Scholar] [CrossRef]
- Okroj, K.T.; Calkins, T.E.; Kayupov, E.; Kheir, M.M.; Bingham, J.S.; Beauchamp, C.P.; Parvizi, J.; Della Valle, C.J. The alpha-defensin test for diagnosing periprosthetic joint infection in the setting of an adverse local tissue reaction secondary to a failed metal-on-metal bearing or corrosion at the head-neck junction. J. Arthroplast. 2018, 33, 1896–1898. [Google Scholar] [CrossRef]
- Berger, P.; Van Cauter, M.; Driesen, R.; Neyt, J.; Cornu, O.; Bellemans, J. Diagnosis of prosthetic joint infection with alpha-defensin using a lateral flow device: A multicentre study. Bone Jt. J. 2017, 99, 1176–1182. [Google Scholar] [CrossRef]
- Suda, A.J.; Tinelli, M.; Beisemann, N.D.; Weil, Y.; Khoury, A.; Bischel, O.E. Diagnosis of periprosthetic joint infection using alpha-defensin test or multiplex-PCR: Ideal diagnostic test still not found. Int. Orthop. 2017, 41, 1307–1313. [Google Scholar] [CrossRef]
- Balato, G.; Franceschini, V.; Ascione, T.; Lamberti, A.; D'Amato, M.; Ensini, A.; Baldini, A. High performance of alpha-defensin lateral flow assay (Synovasure) in the diagnosis of chronic knee prosthetic infections. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1717–1722. [Google Scholar] [CrossRef]
- De Saint Vincent, B.; Migaud, H.; Senneville, E.; Loiez, C.; Pasquier, G.; Girard, J.; Putman, S. Diagnostic accuracy of the alpha defensin lateral flow device (Synovasure) for periprosthetic infections in microbiologically complex situations: A study of 42 cases in a French referral centre. Orthop. Traumatol. Surg. Res. 2018, 104, 427–431. [Google Scholar] [CrossRef]
- Riccio, G.; Cavagnaro, L.; Akkouche, W.; Carrega, G.; Felli, L.; Burastero, G. Qualitative alpha-defensin versus the main available tests for the diagnosis of periprosthetic joint infection: Best predictor test? J. Bone Infect. 2018, 3, 156–164. [Google Scholar] [CrossRef]
- Stone, W.Z.; Gray, C.F.; Parvataneni, H.K.; Al-Rashid, M.; Vlasak, R.G.; Horodyski, M.; Prieto, H.A. Clinical evaluation of synovial alpha defensin and synovial C-reactive protein in the diagnosis of periprosthetic joint infection. J. Bone Jt. Surg. Am. 2018, 100, 1184–1190. [Google Scholar] [CrossRef]
- Plate, A.; Stadler, L.; Sutter, R.; Anagnostopoulos, A.; Frustaci, D.; Zbinden, R.; Fucentese, S.F.; Zinkernagel, A.S.; Zingg, P.O.; Achermann, Y. Inflammatory disorders mimicking periprosthetic joint infections may result in false-positive alpha-defensin. Clin. Microbiol. Infect. 2018, 24, e1212.e1–e1212.e6. [Google Scholar] [CrossRef]
- Sigmund, I.K.; Holinka, J.; Lang, S.; Stenicka, S.; Staats, K.; Hobusch, G.; Kubista, B.; Windhager, R. A comparative study of intraoperative frozen section and alpha defensin lateral flow test in the diagnosis of periprosthetic joint infection. Acta Orthop. 2019, 90, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdo, R.C.T.; Gobbi, R.G.; Leite, C.B.G.; Pasoto, S.G.; Leon, E.P.; Lima, A.; Bonfa, E.; Pecora, J.R.; Demange, M.K. Performance of alpha-defensin lateral flow test after synovial fluid centrifugation for diagnosis of periprosthetic knee infection. World J. Orthop. 2021, 12, 565–574. [Google Scholar] [CrossRef] [PubMed]
- De Saint Vincent, B.; Martinot, P.; Pascal, A.; Senneville, E.; Loiez, C.; Pasquier, G.; Girard, J.; Putman, S.; Migaud, H. Does the alpha-defensin lateral flow test conserve its diagnostic properties in a larger population of chronic complex periprosthetic infections? Enlargement to 112 tests, from 42 tests in a preliminary study, in a reference center. Orthop. Traumatol. Surg. Res. 2021, 107, 102912. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.Z.; Li, R.; Fu, J.; Chai, W.; Hao, L.B.; Chen, J.Y. Leukocyte esterase test and alpha-defensin test have similar accuracy for the diagnosis of periprosthetic joint infection. Int. Orthop. 2021, 45, 1677–1682. [Google Scholar] [CrossRef]
- Zeng, Y.Q.; Deng, S.; Zhu, X.Y.; Sun, X.B.; Feng, W.J.; Zeng, J.C.; Zhang, H.T.; Zeng, Y.R. Diagnostic accuracy of the synovial fluid alpha-defensin lateral flow test in periprosthetic joint infection: A meta-analysis. Orthop. Surg. 2021, 13, 708–718. [Google Scholar] [CrossRef]
- Kuiper, J.W.P.; Verberne, S.J.; van Egmond, P.W.; Slot, K.; Temmerman, O.P.P.; Vos, C.J. Are accuracy studies for periprosthetic joint infection diagnosis inherently flawed? And what to do with Schrödinger’s hips? A prospective analysis of the alpha defensin lateral-flow test in chronic painful hip arthroplasties. Hip. Pelvis. 2022, 34, 236–244. [Google Scholar] [CrossRef]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Diagnosing periprosthetic joint infection: Has the era of the biomarker arrived? Clin. Orthop. Relat. R 2014, 472, 3254–3262. [Google Scholar] [CrossRef]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Combined measurement of synovial fluid alpha-defensin and C-reactive protein levels: Highly accurate for diagnosing periprosthetic joint infection. J. Bone Jt. Surg. Am. 2014, 96, 1439–1445. [Google Scholar] [CrossRef]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Booth, R.E., Jr.; Parvizi, J. The alpha-defensin test for periprosthetic joint infection outperforms the leukocyte esterase test strip. Clin. Orthop. Relat. Res. 2015, 473, 198–203. [Google Scholar] [CrossRef]
- Frangiamore, S.J.; Gajewski, N.D.; Saleh, A.; Farias-Kovac, M.; Barsoum, W.K.; Higuera, C.A. Alpha-defensin accuracy to diagnose periprosthetic joint infection-best available test? J. Arthroplast. 2016, 31, 456–460. [Google Scholar] [CrossRef]
- Bonanzinga, T.; Zahar, A.; Dutsch, M.; Lausmann, C.; Kendoff, D.; Gehrke, T. How reliable is the alpha-defensin immunoassay test for diagnosing periprosthetic joint infection? A prospective study. Clin. Orthop. Relat. Res. 2017, 475, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Kleiss, S.; Jandl, N.M.; Novo de Oliveira, A.; Ruther, W.; Niemeier, A. Diagnostic accuracy of alpha-defensin enzyme-linked immunosorbent assay in the clinical evaluation of painful hip and knee arthroplasty with possible prosthetic joint infection: A prospective study of 202 cases. Bone Jt. J. 2019, 101, 970–977. [Google Scholar] [CrossRef]
- Li, R.; Li, X.; Ni, M.; Fu, J.; Xu, C.; Chai, W.; Chen, J.Y. What is the performance of novel synovial biomarkers for detecting periprosthetic joint infection in the presence of inflammatory joint disease? Bone Jt. J. 2021, 103, 32–38. [Google Scholar] [CrossRef]
- Iorio, R.; Viglietta, E.; Mazza, D.; Petrucca, A.; Borro, M.; Iolanda, S.; Simmaco, M.; Ferretti, A. Accuracy and cost-effectivenss of a novel method for alpha defensins measurement in the diagnosis of periprosthetic joint infections. J. Arthroplast. 2021, 36, 3275–3281. [Google Scholar] [CrossRef]
- Parvizi, J.; Ghanem, E.; Menashe, S.; Barrack, R.L.; Bauer, T.W. Periprosthetic infection: What are the diagnostic challenges? J. Bone Jt. Surg. Am. 2006, 88 (Suppl. 4), 138–147. [Google Scholar] [CrossRef]
- Saleh, A.; Ramanathan, D.; Siqueira, M.B.P.; Klika, A.K.; Barsoum, W.K.; Rueda, C.A.H. The diagnostic utility of synovial fluid markers in periprosthetic joint infection: A systematic review and meta-analysis. J. Am. Acad. Orthop. Surg. 2017, 25, 763–772. [Google Scholar] [CrossRef]
- Lenski, M.; Scherer, M.A. Synovial IL-6 as inflammatory marker in periprosthetic joint infections. J. Arthroplast. 2014, 29, 1105–1109. [Google Scholar] [CrossRef]
- Parvizi, J.; McKenzie, J.C.; Cashman, J.P. Diagnosis of periprosthetic joint infection using synovial C-reactive protein. J. Arthroplast. 2012, 27, 12–16. [Google Scholar] [CrossRef]
- Parvizi, J.; Jacovides, C.; Adeli, B.; Jung, K.A.; Hozack, W.J. Mark B. Coventry Award: Synovial C-reactive protein: A prospective evaluation of a molecular marker for periprosthetic knee joint infection. Clin. Orthop. Relat. Res. 2012, 470, 54–60. [Google Scholar] [CrossRef]
- De Vecchi, E.; Villa, F.; Bortolin, M.; Toscano, M.; Tacchini, L.; Romano, C.L.; Drago, L. Leucocyte esterase, glucose and C-reactive protein in the diagnosis of prosthetic joint infections: A prospective study. Clin. Microbiol. Infect. 2016, 22, 555–560. [Google Scholar] [CrossRef]
- Gallo, J.; Svoboda, M.; Zapletalova, J.; Proskova, J.; Juranova, J. Serum IL-6 in combination with synovial IL-6/CRP shows excellent diagnostic power to detect hip and knee prosthetic joint infection. PLoS ONE 2018, 13, e0199226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plate, A.; Anagnostopoulos, A.; Glanzmann, J.; Stadler, L.; Weigelt, L.; Sutter, R.; Kastli, M.; Zinkernagel, A.S.; Zingg, P.O.; Achermann, Y. Synovial C-reactive protein features high negative predictive value but is not useful as a single diagnostic parameter in suspected periprosthetic joint infection (PJI). J. Infect. 2019, 78, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Grzelecki, D.; Walczak, P.; Szostek, M.; Grajek, A.; Rak, S.; Kowalczewski, J. Blood and synovial fluid calprotectin as biomarkers to diagnose chronic hip and knee periprosthetic joint infections. Bone Jt. J. 2021, 103, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Qin, L.; Wang, J.; Hu, N.; Huang, W. Combined serum and synovial C-reactive protein tests: A valuable adjunct to the diagnosis of chronic prosthetic joint infection. BMC Musculoskelet. Disord. 2021, 22, 670. [Google Scholar] [CrossRef] [PubMed]
- Praz, C.; Gubbiotti, L.; Buia, G.; Chapus, V.; Dunet, J.; Grandhomme, F.; Michon, J.; Rochcongar, G.; Hulet, C. Value of the synovial C-reactive protein test in the diagnosis of total hip and knee periprosthetic joint infections: A case-control study. Orthop. Traumatol. Surg. Res. 2021, 107, 102903. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Ploegmakers, J.J.W.; Kampinga, G.A.; Wagenmakers-Huizenga, L.; Jutte, P.C.; Muller Kobold, A.C. Synovial calprotectin: A potential biomarker to exclude a prosthetic joint infection. Bone Jt. J. 2017, 99, 660–665. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Ploegmakers, J.J.W.; Ottink, K.; Kampinga, G.A.; Wagenmakers-Huizenga, L.; Jutte, P.C.; Kobold, A.C.M. Synovial calprotectin: An inexpensive biomarker to exclude a chronic prosthetic joint infection. J. Arthroplast. 2018, 33, 1149–1153. [Google Scholar] [CrossRef]
- Salari, P.; Grassi, M.; Cinti, B.; Onori, N.; Gigante, A. Synovial fluid calprotectin for the preoperative diagnosis of chronic periprosthetic joint infection. J. Arthroplast. 2020, 35, 534–537. [Google Scholar] [CrossRef]
- Trotter, A.J.; Dean, R.; Whitehouse, C.E.; Mikalsen, J.; Hill, C.; Brunton-Sim, R.; Kay, G.L.; Shakokani, M.; Durst, A.Z.E.; Wain, J.; et al. Preliminary evaluation of a rapid lateral flow calprotectin test for the diagnosis of prosthetic joint infection. Bone Jt. Res. 2020, 9, 202–210. [Google Scholar] [CrossRef]
- Warren, J.; Anis, H.K.; Bowers, K.; Pannu, T.; Villa, J.; Klika, A.K.; Colon-Franco, J.; Piuzzi, N.S.; Higuera, C.A. Diagnostic utility of a novel point-of-care test of calprotectin for periprosthetic joint infection after total knee arthroplasty: A prospective cohort study. J. Bone Jt. Surg. Am. 2021, 103, 1009–1015. [Google Scholar] [CrossRef]
- Warren, J.A.; Klika, A.K.; Bowers, K.; Colon-Franco, J.; Piuzzi, N.S.; Higuera, C.A. Calprotectin lateral flow test: Consistent across criteria for ruling out periprosthetic joint infection. J. Arthroplast. 2022, 37, 1153–1158. [Google Scholar] [CrossRef]
- Cheok, T.; Smith, T.; Siddiquee, S.; Jennings, M.P.; Jayasekera, N.; Jaarsma, R.L. Synovial fluid calprotectin performs better than synovial fluid polymerase chain reaction and interleukin-6 in the diagnosis of periprosthetic joint infection: A systematic review and meta-analysis. Bone Jt. J. 2022, 104, 311–320. [Google Scholar] [CrossRef]
- Grassi, M.; Salari, P.; Farinelli, L.; D'Anzeo, M.; Onori, N.; Gigante, A. Synovial biomarkers to detect chronic periprosthetic joint infection: A pilot study to compare calprotectin rapid test, calprotectin ELISA immunoassay and leukocyte esterase test. J. Arthroplast. 2022, 37, 781–786. [Google Scholar] [CrossRef]
- Chen, Z.; Ma, Y.; Li, X.; Deng, Z.; Zheng, M.; Zheng, Q. The immune cell landscape in different anatomical structures of knee in osteoarthritis: A gene expression-based study. Biomed. Res. Int. 2020, 2020, 9647072. [Google Scholar] [CrossRef]
- Xing, J.; Li, J.; Yan, Z.; Li, Y.; Liu, X.; He, L.; Xu, T.; Wang, C.; Zhao, L.; Jie, K. Diagnostic accuracy of calprotectin in periprosthetic joint infection: A diagnostic meta-analysis. J. Orthop. Surg. Res. 2022, 17, 11. [Google Scholar] [CrossRef]
- Xie, K.; Dai, K.; Qu, X.; Yan, M. Serum and synovial fluid interleukin-6 for the diagnosis of periprosthetic joint infection. Sci. Rep. 2017, 7, 1496. [Google Scholar] [CrossRef]
- Li, J.; Zhou, Q.; Deng, B. Serum versus synovial fluid interleukin-6 for periprosthetic joint infection diagnosis: A systematic review and meta-analysis of 30 diagnostic test accuracy studies. J. Orthop. Surg. Res. 2022, 17, 564. [Google Scholar] [CrossRef]
- Qin, L.; Du, C.; Yang, J.; Wang, H.; Su, X.; Wei, L.; Zhao, C.; Chen, C.; Chen, H.; Hu, N.; et al. Synovial fluid interleukin levels cannot distinguish between prosthetic joint infection and active rheumatoid arthritis after hip or knee arthroplasty. Diagnostics 2022, 12, 1196. [Google Scholar] [CrossRef]
- Su, X.; Chen, Y.; Zhan, Q.; Zhu, B.; Chen, L.; Zhao, C.; Yang, J.; Wei, L.; Xu, Z.; Wei, K.; et al. The ratio of Il-6 to Il-4 in synovial fluid of knee or hip performances a noteworthy diagnostic value in prosthetic joint infection. J. Clin. Med. 2022, 11, 6520. [Google Scholar] [CrossRef]
- Shahi, A.; Tan, T.L.; Kheir, M.M.; Tan, D.D.; Parvizi, J. Diagnosing periprosthetic joint infection: And the winner is? J. Arthroplast. 2017, 32, S232–S235. [Google Scholar] [CrossRef]
- Wang, C.; Li, R.; Wang, Q.; Wang, C. Synovial fluid leukocyte esterase in the diagnosis of peri-prosthetic joint infection: A systematic review and meta-analysis. Surg. Infect. 2018, 19, 245–253. [Google Scholar] [CrossRef]
- Chisari, E.; Yacovelli, S.; Goswami, K.; Shohat, N.; Woloszyn, P.; Parvizi, J. Leukocyte esterase versus ICM 2018 criteria in the diagnosis of periprosthetic joint infection. J. Arthroplast. 2021, 36, 2942–2945.e2941. [Google Scholar] [CrossRef] [PubMed]
- Logoluso, N.; Pellegrini, A.; Suardi, V.; Morelli, I.; Battaglia, A.G.; D'Anchise, R.; De Vecchi, E.; Zagra, L. Can the leukocyte esterase strip test predict persistence of periprosthetic joint infection at second-stage reimplantation? J. Arthroplast. 2022, 37, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Vergara, A.; Fernandez-Pittol, M.J.; Munoz-Mahamud, E.; Morata, L.; Bosch, J.; Vila, J.; Soriano, A.; Casals-Pascual, C. Evaluation of lipocalin-2 as a biomarker of periprosthetic joint infection. J. Arthroplast. 2019, 34, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Svoboda, M.; Gallo, J.; Zapletalova, J.; Proskova, J.; Juranova, J.; Loveckova, Y. Glucose, lactate, NGAL and coefficient of energy balance in synovial fluid in patients with hip and knee prosthetic joint infection. Acta Chir. Orthop. Traumatol. Cech. 2022, 89, 16–26. [Google Scholar]
- Vicenti, G.; Bizzoca, D.; Nappi, V.; Pesce, V.; Solarino, G.; Carrozzo, M.; Moretti, F.; Dicuonzo, F.; Moretti, B. Serum biomarkers in the diagnosis of periprosthetic joint infection: Consolidated evidence and recent developments. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 43–50. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, H.; Ding, P.; Jiao, Q. The accuracy of D-dimer in the diagnosis of periprosthetic infections: A systematic review and meta-analysis. J. Orthop Surg. Res. 2022, 17, 99. [Google Scholar] [CrossRef]
- Piper, K.E.; Fernandez-Sampedro, M.; Steckelberg, K.E.; Mandrekar, J.N.; Karau, M.J.; Steckelberg, J.M.; Berbari, E.F.; Osmon, D.R.; Hanssen, A.D.; Lewallen, D.G.; et al. C-reactive protein, erythrocyte sedimentation rate and orthopedic implant infection. PLoS ONE 2010, 5, e9358. [Google Scholar] [CrossRef]
- Xie, K.; Qu, X.; Yan, M. Procalcitonin and alpha-defensin for diagnosis of periprosthetic joint infections. J. Arthroplast. 2017, 32, 1387–1394. [Google Scholar] [CrossRef]
- Dapunt, U.; Giese, T.; Maurer, S.; Stegmaier, S.; Prior, B.; Hansch, G.M.; Gaida, M.M. Neutrophil-derived MRP-14 is up-regulated in infectious osteomyelitis and stimulates osteoclast generation. J. Leukoc. Biol. 2015, 98, 575–582. [Google Scholar] [CrossRef]
- Shohat, N.; Goswami, K.; Fillingham, Y.; Tan, T.L.; Calkins, T.; Della Valle, C.J.; George, J.; Higuera, C.; Parvizi, J. Diagnosing periprosthetic joint infection in inflammatory arthritis: Assumption is the enemy of true understanding. J. Arthroplast. 2018, 33, 3561–3566. [Google Scholar] [CrossRef]
- Ren, Y.; Biedermann, L.; Gwinner, C.; Perka, C.; Kienzle, A. Serum and synovial markers in patients with rheumatoid arthritis and periprosthetic joint infection. J. Pers. Med. 2022, 12, 810. [Google Scholar] [CrossRef]
- George, J.; Jawad, M.; Curtis, G.L.; Samuel, L.T.; Klika, A.K.; Barsoum, W.K.; Higuera, C.A. Utility of serological markers for detecting persistent infection in two-stage revision arthroplasty in patients with inflammatory arthritis. J. Arthroplast. 2018, 33, S205–S208. [Google Scholar] [CrossRef]
- Saleh, A.; George, J.; Faour, M.; Klika, A.K.; Higuera, C.A. Serum biomarkers in periprosthetic joint infections. Bone Jt. Res. 2018, 7, 85–93. [Google Scholar] [CrossRef]
- Abdelbary, H.; Cheng, W.; Ahmadzai, N.; Carli, A.V.; Shea, B.J.; Hutton, B.; Fergusson, D.A.; Beaule, P.E. Combination tests in the diagnosis of chronic periprosthetic joint infection: Systematic review and development of a stepwise clinical decision-making tool. J. Bone Jt. Surg. Am. 2020, 102, 114–124. [Google Scholar] [CrossRef]
- Tunney, M.M.; Patrick, S.; Gorman, S.P.; Nixon, J.R.; Anderson, N.; Davis, R.I.; Hanna, D.; Ramage, G. Improved detection of infection in hip replacements. A currently underestimated problem. J. Bone Jt. Surg. Br. 1998, 80, 568–572. [Google Scholar] [CrossRef]
- Tunney, M.M.; Patrick, S.; Curran, M.D.; Ramage, G.; Hanna, D.; Nixon, J.R.; Gorman, S.P.; Davis, R.I.; Anderson, N. Detection of prosthetic hip infection at revision arthroplasty by immunofluorescence microscopy and PCR amplification of the bacterial 16S rRNA gene. J. Clin. Microbiol. 1999, 37, 3281–3290. [Google Scholar] [CrossRef]
- Moojen, D.J.; van Hellemondt, G.; Vogely, H.C.; Burger, B.J.; Walenkamp, G.H.; Tulp, N.J.; Schreurs, B.W.; de Meulemeester, F.R.; Schot, C.S.; van de Pol, I.; et al. Incidence of low-grade infection in aseptic loosening of total hip arthroplasty. Acta Orthop. 2010, 81, 667–673. [Google Scholar] [CrossRef]
- Piper, K.E.; Jacobson, M.J.; Cofield, R.H.; Sperling, J.W.; Sanchez-Sotelo, J.; Osmon, D.R.; McDowell, A.; Patrick, S.; Steckelberg, J.M.; Mandrekar, J.N.; et al. Microbiologic diagnosis of prosthetic shoulder infection by use of implant sonication. J. Clin. Microbiol. 2009, 47, 1878–1884. [Google Scholar] [CrossRef]
- Vergidis, P.; Greenwood-Quaintance, K.E.; Sanchez-Sotelo, J.; Morrey, B.F.; Steinmann, S.P.; Karau, M.J.; Osmon, D.R.; Mandrekar, J.N.; Steckelberg, J.M.; Patel, R. Implant sonication for the diagnosis of prosthetic elbow infection. J. Shoulder Elbow. Surg. 2011, 20, 1275–1281. [Google Scholar] [CrossRef]
- Cazanave, C.; Greenwood-Quaintance, K.E.; Hanssen, A.D.; Karau, M.J.; Schmidt, S.M.; Gomez Urena, E.O.; Mandrekar, J.N.; Osmon, D.R.; Lough, L.E.; Pritt, B.S.; et al. Rapid molecular microbiologic diagnosis of prosthetic joint infection. J. Clin. Microbiol. 2013, 51, 2280–2287. [Google Scholar] [CrossRef] [PubMed]
- Goh, G.S.; Parvizi, J. Diagnosis and treatment of culture-negative periprosthetic joint infection. J. Arthroplast. 2022, 37, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.F.; Eggleston, K.; Rotimi, V.; Zeckhauser, R.J. Antibiotic resistance as a global threat: Evidence from China, Kuwait and the United States. Glob. Health 2006, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, A.R. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- CDC. Antibiotic Resistance Threats in the United States; Department of Health and Human Services: Atlanta, GA, USA, 2019. [Google Scholar]
- CDC. COVID-19: U.S. Impact on Antimicrobial Resistance, Special Report; Department of Health and Human Services, CDC: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/drugresistance/covid19.html (accessed on 30 December 2022).
- Dapunt, U.; Maurer, S.; Giese, T.; Gaida, M.M.; Hansch, G.M. The macrophage inflammatory proteins MIP1alpha (CCL3) and MIP2alpha (CXCL2) in implant-associated osteomyelitis: Linking inflammation to bone degradation. Mediat. Inflamm. 2014, 2014, 728619. [Google Scholar] [CrossRef]
- Dapunt, U.; Giese, T.; Stegmaier, S.; Moghaddam, A.; Hansch, G.M. The osteoblast as an inflammatory cell: Production of cytokines in response to bacteria and components of bacterial biofilms. BMC Musculoskelet. Disord. 2016, 17, 243. [Google Scholar] [CrossRef]
- Heim, C.E.; Vidlak, D.; Scherr, T.D.; Hartman, C.W.; Garvin, K.L.; Kielian, T. IL-12 promotes myeloid-derived suppressor cell recruitment and bacterial persistence during Staphylococcus aureus orthopedic implant infection. J. Immunol. 2015, 194, 3861–3872. [Google Scholar] [CrossRef]
- Marazzi, M.G.; Randelli, F.; Brioschi, M.; Drago, L.; Romano, C.L.; Banfi, G.; Massaccesi, L.; Crapanzano, C.; Morelli, F.; Corsi Romanelli, M.M.; et al. Presepsin: A potential biomarker of PJI? A comparative analysis with known and new infection biomarkers. Int. J. Immunopathol. Pharmacol. 2018, 31, 394632017749356. [Google Scholar] [CrossRef]
- Zou, Q.; Wen, W.; Zhang, X.-C. Presepsin as a novel sepsis biomarker. World J. Emerg. Med. 2014, 5, 16. [Google Scholar] [CrossRef]
- Castello, L.M.; Baldrighi, M.; Molinari, L.; Salmi, L.; Cantaluppi, V.; Vaschetto, R.; Zunino, G.; Quaglia, M.; Bellan, M.; Gavelli, F.; et al. The role of osteopontin as a diagnostic and prognostic biomarker in sepsis and septic shock. Cells 2019, 8, 174. [Google Scholar] [CrossRef]
- Masters, T.L.; Bhagwate, A.V.; Dehankar, M.K.; Greenwood-Quaintance, K.E.; Abdel, M.P.; Mandrekar, J.N.; Patel, R. Human transcriptomic response to periprosthetic joint infection. Gene 2022, 825, 146400. [Google Scholar] [CrossRef]
- Fröschen, F.S.; Schell, S.; Wimmer, M.D.; Hischebeth, G.T.; Kohlhof, H.; Gravius, S.; Randau, T.M. Synovial complement factors in patients with periprosthetic joint infection after undergoing revision arthroplasty of the hip or knee joint. Diagnostics 2021, 11, 434. [Google Scholar] [CrossRef]
- Fisher, C.R.; Salmons, H.I.; Mandrekar, J.; Greenwood-Quaintance, K.E.; Abdel, M.P.; Patel, R. A 92 protein inflammation panel performed on sonicate fluid differentiates periprosthetic joint infection from non-infectious causes of arthroplasty failure. Sci. Rep. 2022, 12, 16135. [Google Scholar] [CrossRef]
- Fisher, C.F.; Mangalaparthi, K.K.; Greenwood-Quaintance, K.E.; Abdel, M.P.; Pandey, A. Mass spectrometry-based proteomic profiling of sonicate fluid differentiates Staphylococcus aureus periprosthetic joint infection from non-infectious failure: A pilot study. medRxiv 2023. [Google Scholar] [CrossRef]
- Fisher, C.R.; Krull, J.E.; Bhagwate, A.; Masters, T.; Greenwood-Quaintance, K.E.; Abdel, M.P.; Patel, R. Sonicate fluid cellularity predicted by transcriptomic deconvolution differentiates infectious from non-infectious arthroplasty failure. J. Bone Jt. Surg. Am. 2022, 105, 63–73. [Google Scholar] [CrossRef]
- Johnzon, C.F.; Ronnberg, E.; Pejler, G. The role of mast cells in bacterial infection. Am. J. Pathol. 2016, 186, 4–14. [Google Scholar] [CrossRef]
- Piliponsky, A.M.; Acharya, M.; Shubin, N.J. Mast cells in viral, bacterial, and fungal infection immunity. Int. J. Mol. Sci. 2019, 20, 2851. [Google Scholar] [CrossRef]
- Nigrovic, P.A.; Binstadt, B.A.; Monach, P.A.; Johnsen, A.; Gurish, M.; Iwakura, Y.; Benoist, C.; Mathis, D.; Lee, D.M. Mast cells contribute to initiation of autoantibody-mediated arthritis via IL-1. Proc. Natl. Acad. Sci. USA 2007, 104, 2325–2330. [Google Scholar] [CrossRef]
- Nigrovic, P.A.; Lee, D.M. Synovial mast cells: Role in acute and chronic arthritis. Immunol. Rev. 2007, 217, 19–37. [Google Scholar] [CrossRef]
- Limberg, A.K.; Salib, C.G.; Tibbo, M.E.; Vargas-Hernandez, J.S.; Bettencourt, J.W.; Bayram, B.; Berry, C.E.; Dudakovic, A.; Bolon, B.; van Wijnen, A.J.; et al. Immune cell populations differ in patients undergoing revision total knee arthroplasty for arthrofibrosis. Sci. Rep. 2022, 12, 22627. [Google Scholar] [CrossRef] [PubMed]
- Korn, M.F.; Stein, R.R.; Dolf, A.; Shakeri, F.; Buness, A.; Hilgers, C.; Masson, W.; Gravius, S.; Kohlhof, H.; Burger, C.; et al. High-dimensional analysis of immune cell composition predicts periprosthetic joint infections and dissects its pathophysiology. Biomedicines 2020, 8, 358. [Google Scholar] [CrossRef] [PubMed]
- Paziuk, T.; Rondon, A.J.; Goswami, K.; Tan, T.L.; Parvizi, J. A novel adjunct indicator of periprosthetic joint infection: Platelet count and mean platelet volume. J. Arthroplast. 2020, 35, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Festa, E.; Ascione, T.; Bernasconi, A.; Di Gennaro, D.; Basso, M.A.; Guarino, A.; Balato, G. Diagnostic performance of neutrophil to lymphocyte ratio, monocyte to lymphocyte ratio, platelet to lymphocyte ratio, and platelet to mean platelet volume ratio in periprosthetic hip and knee infections: A systematic review and meta-analysis. Diagnostics 2022, 12, 2033. [Google Scholar] [CrossRef]
- Sahin, E.; Karaismailoglu, B.; Ozsahin, M.K.; Guven, M.F.; Kaynak, G. Low value of platelet count to mean platelet volume ratio to diagnose chronic PJI: A case control study. Orthop. Traumatol. Surg. Res. 2021, 107, 102899. [Google Scholar] [CrossRef]
- Heim, C.E.; Vidlak, D.; Odvody, J.; Hartman, C.W.; Garvin, K.L.; Kielian, T. Human prosthetic joint infections are associated with myeloid-derived suppressor cells (MDSCs): Implications for infection persistence. J. Orthop. Res. 2018, 36, 1605–1613. [Google Scholar] [CrossRef]
- Heim, C.E.; Bosch, M.E.; Yamada, K.J.; Aldrich, A.L.; Chaudhari, S.S.; Klinkebiel, D.; Gries, C.M.; Alqarzaee, A.A.; Li, Y.; Thomas, V.C.; et al. Lactate production by Staphylococcus aureus biofilm inhibits HDAC11 to reprogramme the host immune response during persistent infection. Nat. Microbiol. 2020, 5, 1271–1284. [Google Scholar] [CrossRef]
- Bosch, M.E.; Bertrand, B.P.; Heim, C.E.; Alqarzaee, A.A.; Chaudhari, S.S.; Aldrich, A.L.; Fey, P.D.; Thomas, V.C.; Kielian, T. Staphylococcus aureus ATP synthase promotes biofilm persistence by influencing innate immunity. mBio 2020, 11, e01581-20. [Google Scholar] [CrossRef]
- Deo, R.C. Machine learning in medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef]
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Lee, M.J.; Asadi, H. eDoctor: Machine learning and the future of medicine. J. Intern. Med. 2018, 284, 603–619. [Google Scholar] [CrossRef]
- Weiskittel, T.M.; Correia, C.; Yu, G.T.; Ung, C.Y.; Kaufmann, S.H.; Billadeau, D.D.; Li, H. The trifecta of single-cell, systems-biology, and machine-learning approaches. Genes 2021, 12, 1098. [Google Scholar] [CrossRef]
- Wiens, J.; Shenoy, E.S. Machine learning for healthcare: On the verge of a major shift in healthcare epidemiology. Clin. Infect. Dis. 2018, 66, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Polisetty, T.S.; Jain, S.; Pang, M.; Karnuta, J.M.; Vigdorchik, J.M.; Nawabi, D.H.; Wyles, C.C.; Ramkumar, P.N. Concerns surrounding application of artificial intelligence in hip and knee arthroplasty: A review of literature and recommendations for meaningful adoption. Bone Jt. J. 2022, 104, 1292–1303. [Google Scholar] [CrossRef]
- Klemt, C.; Laurencin, S.; Uzosike, A.C.; Burns, J.C.; Costales, T.G.; Yeo, I.; Habibi, Y.; Kwon, Y.M. Machine learning models accurately predict recurrent infection following revision total knee arthroplasty for periprosthetic joint infection. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2582–2590. [Google Scholar] [CrossRef]
- Fu, S.; Wyles, C.C.; Osmon, D.R.; Carvour, M.L.; Sagheb, E.; Ramazanian, T.; Kremers, W.K.; Lewallen, D.G.; Berry, D.J.; Sohn, S.; et al. Automated detection of periprosthetic joint infections and data elements using natural language processing. J. Arthroplast. 2021, 36, 688–692. [Google Scholar] [CrossRef]
- Shohat, N.; Goswami, K.; Tan, T.L.; Yayac, M.; Soriano, A.; Sousa, R.; Wouthuyzen-Bakker, M.; Parvizi, J.; ESCMID Study Group of Implant Associated Infections; Northern Infection Network of Joint Arthroplasty. 2020 Frank Stinchfield Award: Identifying who will fail following irrigation and debridement for prosthetic joint infection. Bone Jt. J. 2020, 102, 11–19. [Google Scholar] [CrossRef]
Figure 1.
Causes of periprosthetic joint infection after total hip and total knee arthroplasty based on data from Tai, D.B.G. et al. Clin Microbiol Infect 2022, 28, 255–259 [50]. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).
Figure 1.
Causes of periprosthetic joint infection after total hip and total knee arthroplasty based on data from Tai, D.B.G. et al. Clin Microbiol Infect 2022, 28, 255–259 [50]. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).

Figure 2.
Common causes of non-infectious arthroplasty involving (A) total knee arthroplasty (TKA) and (B) total hip arthroplasty (THA). TKA data are from Abdel, M.P. et al. Bone Joint J 2017, 99-B, 647–652 [64]. THA data from Ledford, C.K. et al. J Am Acad Orthop Surg 2019, 27 [12]. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).
Figure 2.
Common causes of non-infectious arthroplasty involving (A) total knee arthroplasty (TKA) and (B) total hip arthroplasty (THA). TKA data are from Abdel, M.P. et al. Bone Joint J 2017, 99-B, 647–652 [64]. THA data from Ledford, C.K. et al. J Am Acad Orthop Surg 2019, 27 [12]. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).

Figure 3.
Periprosthetic joint infection (PJI)-related publication counts between 1969 and 2022. (A) All PJI-related publications were calculated based on a PubMed query with keywords “PJI”, “prosthetic joint infection”, or “periprosthetic joint infection”. (B) PJI diagnosis-related publications were calculated based on a PubMed query with keywords “PJI diagnosis”, “prosthetic joint infection diagnosis”, or “periprosthetic joint infection diagnosis”. Query conducted on 16 January 2023. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).
Figure 3.
Periprosthetic joint infection (PJI)-related publication counts between 1969 and 2022. (A) All PJI-related publications were calculated based on a PubMed query with keywords “PJI”, “prosthetic joint infection”, or “periprosthetic joint infection”. (B) PJI diagnosis-related publications were calculated based on a PubMed query with keywords “PJI diagnosis”, “prosthetic joint infection diagnosis”, or “periprosthetic joint infection diagnosis”. Query conducted on 16 January 2023. Graph created in GraphPad Prism v9.4.0 (San Diego, CA, USA).

Figure 4.
Immune response to arthroplasty failure due to periprosthetic joint infection (PJI) or non-infectious arthroplasty failure (NIAF) detailing cell-types recruited/activated and host markers. Bolded, starred (*) entries represent those currently used for the diagnosis of PJI. Abbreviations used: 4E-BP1, eukaryotic translation initiation factor 4E (eIF4E)-binding protein 1; BCAT1, branched-chain-amino-acid aminotransferase; BPI, bactericidal/permeability-increasing protein; CCL, chemokine (C-C motif) ligand; CDCP1, complement C1r/C1s, Uegf, Bmp1 domain containing protein 1; COL1A2, collagen α-2(I) chain; CRTAC1, cartilage acidic protein 1; CRP, C-reactive protein; CSF-1, macrophage-colony stimulating factor; CXCL, chemokine (C-X-C motif) ligand; DLST, dihydrolipoamide S-succinyltransferase; EEA1, early endosome antigen 1; ELA-2, neutrophil elastase; EN-RAGE, extracellular newly identified receptor for advanced glycation end products binding protein; ERN1, endoplasmic reticulum to nucleus signaling 1; FABP3, fatty acid-binding protein–heart; FABP5, fatty acid-binding protein–epidermal; FBP1, fructose-1,6-bisphosphatase 1; FCRL4, Fc receptor-like 4; G-CSF, granulocyte colony-stimulating factor, HEXB, β-hexosaminidase subunit β; HGF, hepatocyte growth factor; HSPB1, heat shock protein β-1; IFI30, IFI30 lysosomal thiol reductase; IL, interleukin; LE, leukocyte esterase; LIF, leukemia inhibitory factor; LRG1, leucine-rich α-2-glycoprotein; MBL, mannose-binding lectin; MCAM, melanoma cell adhesion molecule; MCP, monocyte chemoattractant protein; MDSC, myeloid derived suppressor cell; MMP, matrix metallopeptidase; PYGL, glycogen phosphorylase–liver; RNASE1, pancreatic ribonuclease; RNASE3, eosinophil cationic protein; SCF complex, Skp, Cullin, F-box containing complex; TLR-2, toll-like receptor 2; TNF, tumor necrosis factor; TNFRSF9, TNF receptor superfamily member 9; TRANCE, TNF-related activation-induced cytokine; TWEAK, TNF-like weak inducer of apoptosis; ST1A1, sulfotransferase family 1A member 1; STAMBP, signal transducing adaptor molecule binding protein. Created with Biorender.com.
Figure 4.
Immune response to arthroplasty failure due to periprosthetic joint infection (PJI) or non-infectious arthroplasty failure (NIAF) detailing cell-types recruited/activated and host markers. Bolded, starred (*) entries represent those currently used for the diagnosis of PJI. Abbreviations used: 4E-BP1, eukaryotic translation initiation factor 4E (eIF4E)-binding protein 1; BCAT1, branched-chain-amino-acid aminotransferase; BPI, bactericidal/permeability-increasing protein; CCL, chemokine (C-C motif) ligand; CDCP1, complement C1r/C1s, Uegf, Bmp1 domain containing protein 1; COL1A2, collagen α-2(I) chain; CRTAC1, cartilage acidic protein 1; CRP, C-reactive protein; CSF-1, macrophage-colony stimulating factor; CXCL, chemokine (C-X-C motif) ligand; DLST, dihydrolipoamide S-succinyltransferase; EEA1, early endosome antigen 1; ELA-2, neutrophil elastase; EN-RAGE, extracellular newly identified receptor for advanced glycation end products binding protein; ERN1, endoplasmic reticulum to nucleus signaling 1; FABP3, fatty acid-binding protein–heart; FABP5, fatty acid-binding protein–epidermal; FBP1, fructose-1,6-bisphosphatase 1; FCRL4, Fc receptor-like 4; G-CSF, granulocyte colony-stimulating factor, HEXB, β-hexosaminidase subunit β; HGF, hepatocyte growth factor; HSPB1, heat shock protein β-1; IFI30, IFI30 lysosomal thiol reductase; IL, interleukin; LE, leukocyte esterase; LIF, leukemia inhibitory factor; LRG1, leucine-rich α-2-glycoprotein; MBL, mannose-binding lectin; MCAM, melanoma cell adhesion molecule; MCP, monocyte chemoattractant protein; MDSC, myeloid derived suppressor cell; MMP, matrix metallopeptidase; PYGL, glycogen phosphorylase–liver; RNASE1, pancreatic ribonuclease; RNASE3, eosinophil cationic protein; SCF complex, Skp, Cullin, F-box containing complex; TLR-2, toll-like receptor 2; TNF, tumor necrosis factor; TNFRSF9, TNF receptor superfamily member 9; TRANCE, TNF-related activation-induced cytokine; TWEAK, TNF-like weak inducer of apoptosis; ST1A1, sulfotransferase family 1A member 1; STAMBP, signal transducing adaptor molecule binding protein. Created with Biorender.com.

Figure 5.
Potential multi-omics diagnostic scheme using simultaneous microorganism detection and assessment of host response to determine whether infection is present, and if so, to define the causative pathogen(s) and inform treatment. Created with Biorender.com.
Figure 5.
Potential multi-omics diagnostic scheme using simultaneous microorganism detection and assessment of host response to determine whether infection is present, and if so, to define the causative pathogen(s) and inform treatment. Created with Biorender.com.


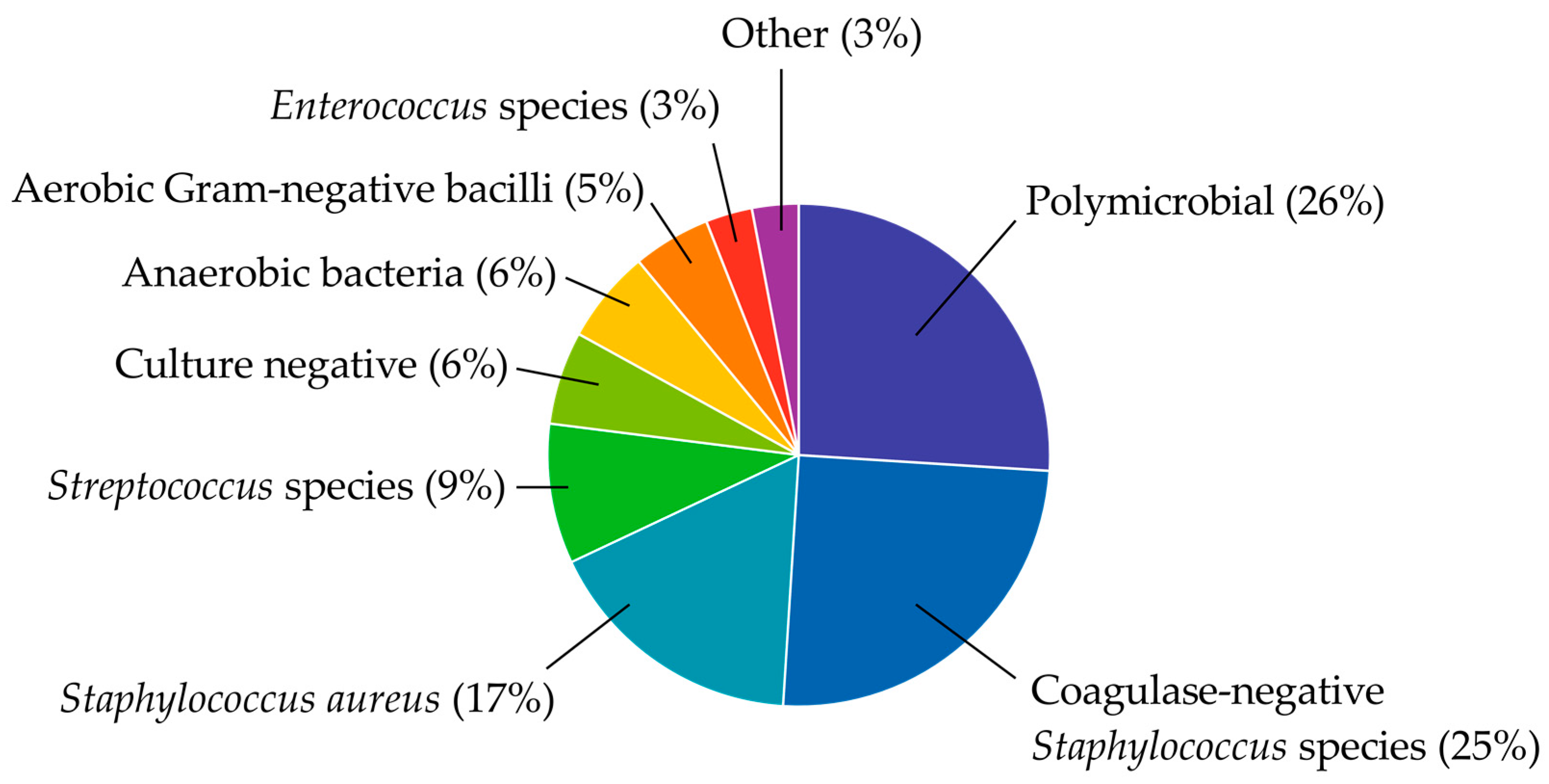{kind=link}
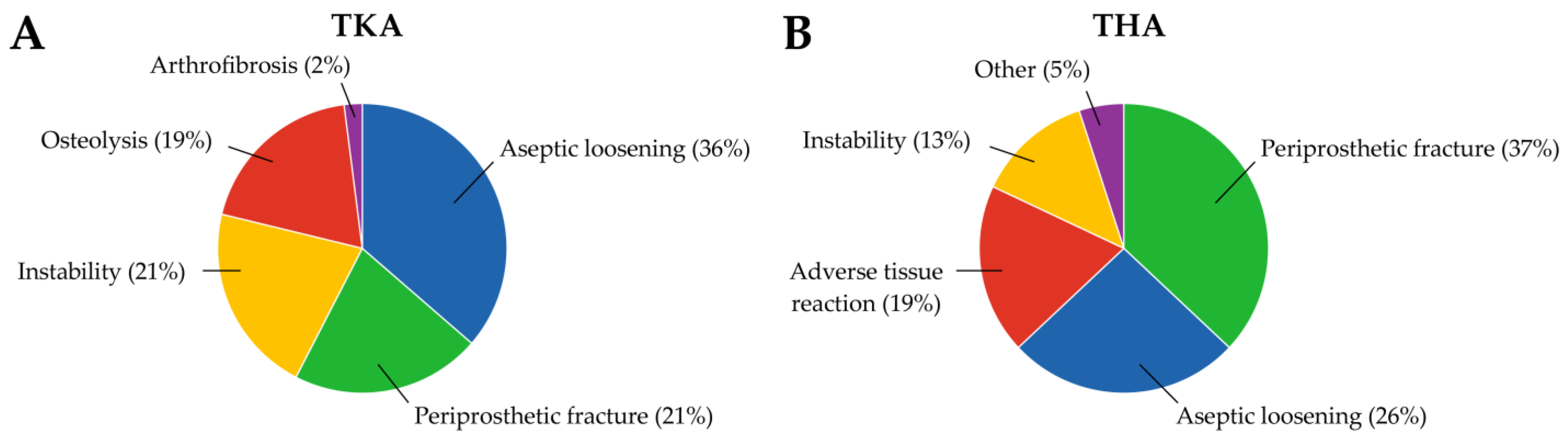{kind=link}
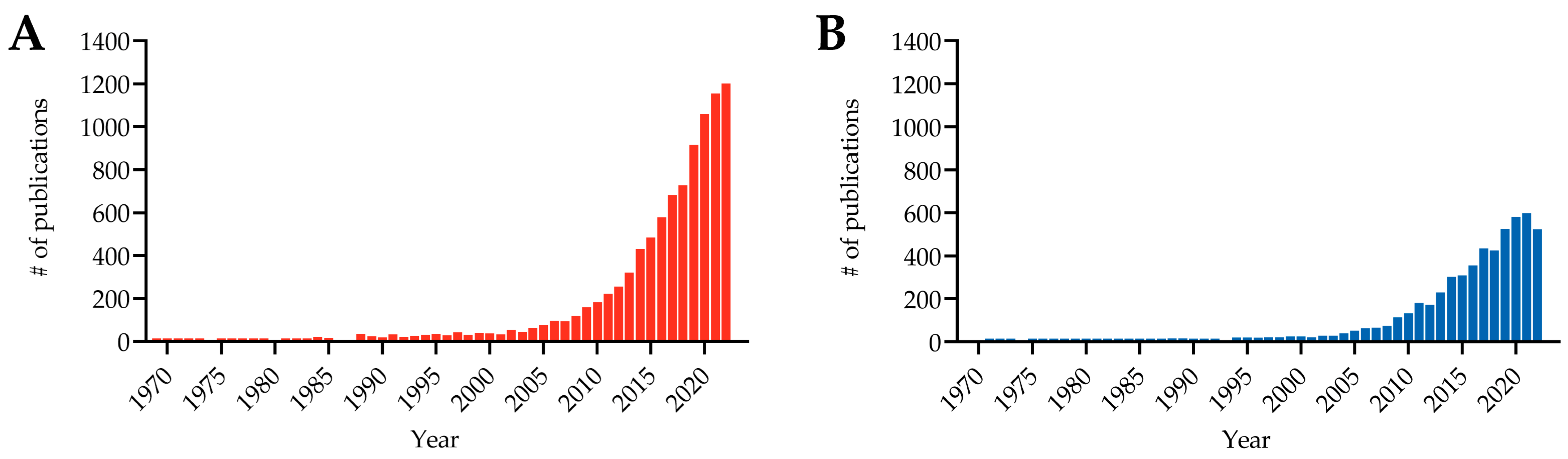{kind=link}
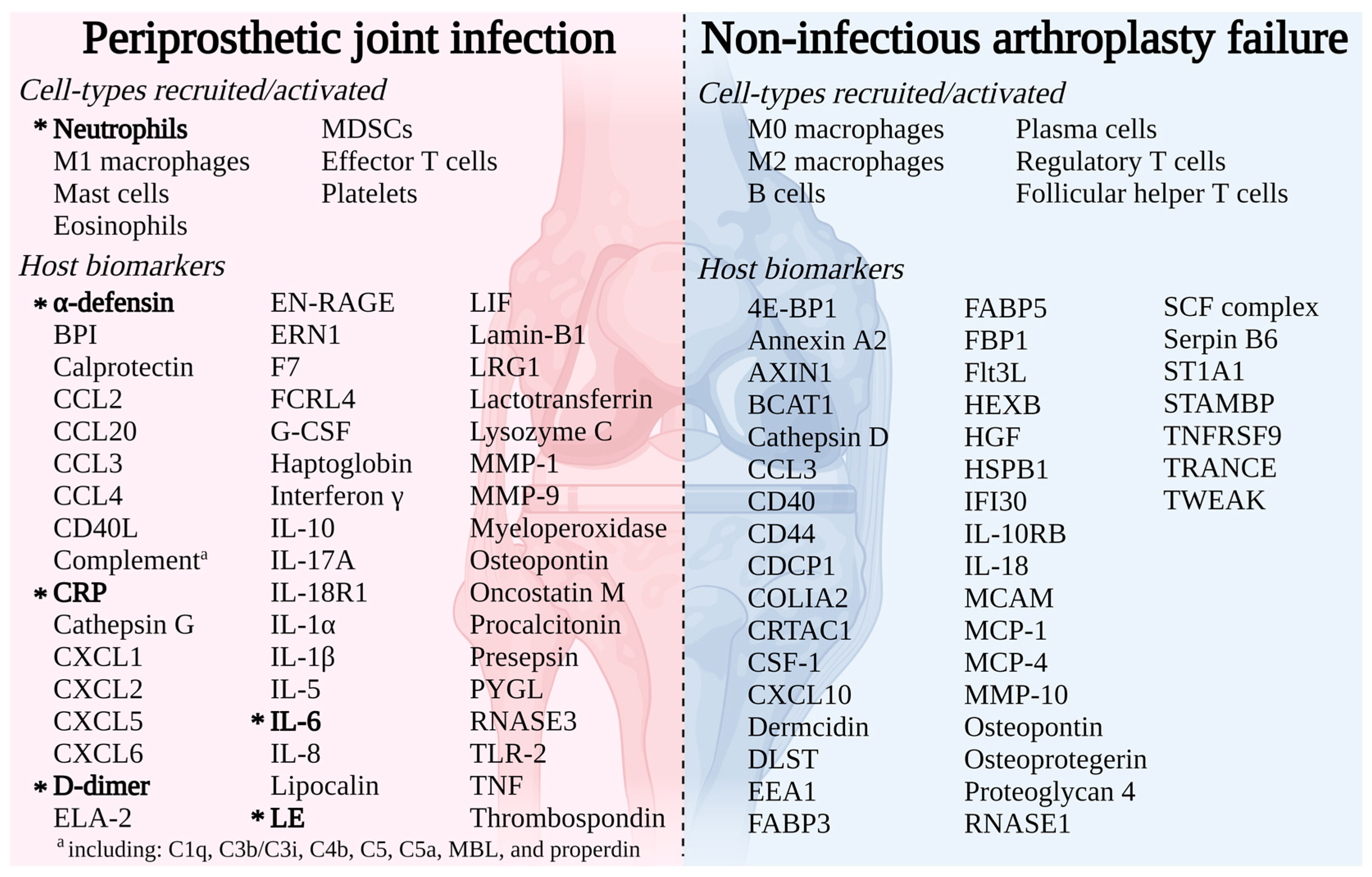{kind=link}
{kind=link}
Table 1.
Sensitivity and specificity of synovial fluid total nucleated cell count and polymorphonuclear percentage for periprosthetic joint infection diagnosis.
Table 1.
Sensitivity and specificity of synovial fluid total nucleated cell count and polymorphonuclear percentage for periprosthetic joint infection diagnosis.
| Biomarker | Knee/Hip/Other | Time Since Arthroplasty | Cut-Point | Sensitivity (%) a | Specificity (%) a | Citation |
|---|---|---|---|---|---|---|
| Total nucleated cell count—cutoff values in cells/µL | ||||||
| Mason et al., 2003 | 440/-/- | NR | 2500 50,000 | 69 19 | 98 100 | [84] |
| Trampuz et al., 2004 | 133/-/- | >6 months | 1700 | 94 (80–99) | 88 (80–93) | [85] |
| Zmistowski et al., 2012 | 153/-/- | NR | 3000 | 94 | 93 | [86] |
| Dinneen et al., 2013 | 48/27/- | NR | 1590 | 90 (78–100) | 91 (83–100) | [87] |
| Wyles et al., 2013 | -/39/- | NR | 3000 | 100 (40–100) | 57 (85–100) | [88] |
| Gallo et al., 2017 | 203/188/- | >7 months | 3450 | 95 | 95 | [89] |
| Higuera et al., 2017 | -/453/- | ≥3 months | 3966 | 90 | 91 | [90] |
| Kim et al., 2017 | 197/-/- | >7 days | 11,200 16,000 | 100 (73–100) 75 (43–95) | 99 (96–100) 100 (98–100) | [91] |
| Lee et al., 2017 | 33 studies | Pooled | Pooled | 89 (86–91) | 86 (80–90) | [92] |
| Shahi et al., 2017 | 836 total | NR | 10,000 | 86 | 83 | [93] |
| Sousa et al., 2017 | 40/15/- | >1 month | 1463 2064 | 100 91 | 7275 | [94] |
| Balato et al., 2018 | 250/-/- | >90 days | 3000 | 81 (74–86) | 91 (86–95) | [95] |
| De Vecchi et al., 2018 | 45/21/- | NR | 1600 3000 | 100 (87–100) 94 (78–99) | 82 (65–93) 91 (75–98) | [96] |
| Kuo et al., 2018 | 131/83/- | NR | 835 | 84 (65–96) | 78 (72–84) | [97] |
| Tahta et al., 2018 | 38/-/- | >3 months | 2347 | 86 (70–100) | 76 (63–98) | [98] |
| Carli et al., 2019 | 26 studies | Pooled | Pooled | 93 | 90 | [99] |
| Dijkman et al., 2020 | 80/-/- | NR | 2575 | 92 | 84 | [100] |
| Mihalič et al., 2020 | 25/24/- | NR | 1700 | 82 (55–100) | 97 (92–100) | [101] |
| Sharma et al., 2020 | 93/14/- | NR | 1100 | 89 | 98 | [102] |
| Ivy et al., 2021 | 74/25/- | NR | 1700 | 83 (59–96) | 81 (70–89) | [103] |
| Levent et al., 2021 | 143/116/- | NR | 3000 | 88 | 88 | [104] |
| van den Kieboom et al., 2021 | 43/101/- | NR | 3000 4552 | 87 (66–97) 86 | 78 (66–87) 85 | [105] |
| Baker et al., 2022 | 358/36/- | >90 days | 3000 | 92 | 99 | [106] |
| Huang et al., 2022 | 39/39/- | NR | 3005 | 90 (78–97) | 100 (88–100) | [107] |
| Lazic et al., 2022 | 4/10/- | NR | 4550 | 40 (12–74) | 100 (79–100) | [108] |
| Dilley et al., 2023 | 485/245/- | >6 weeks | 5600 | 72 | 86 | [109] |
| Polymorphonuclear (PMN) percentage—cutoff values in % of total white blood cell count | ||||||
| Mason et al., 2003 | 440/-/- | NR | 6080 | 7657 | 89100 | [84] |
| Trampuz et al., 2004 | 133/-/- | >6 months | 65 | 97 (85–100) | 98 (93–100) | [85] |
| Zmistowski et al., 2012 | 153/-/- | NR | 75 | 83 | 88 | [86] |
| Dinneen et al., 2013 | 48/27/- | NR | 65 | 90 (80–100) | 87 (76–97) | [87] |
| Wyles et al., 2013 | -/39/- | NR | 80 | 100 (40–100) | 97 (81–100) | [88] |
| Gallo et al., 2017 | 203/188/- | >7 months | 75 | 93 | 91 | [89] |
| Higuera et al., 2017 | -/453/- | ≥3 months | 80 | 92 | 86 | [90] |
| Lee et al., 2017 | 33 studies | Pooled | Pooled | 89 (82–93) | 86 (77–92) | [92] |
| Sousa et al., 2017 | 40/15/- | >1 month | 7881 | 8778 | 7275 | [94] |
| Balato et al., 2018 | 250/-/- | >90 days | 80 | 84 (77–89) | 95 (90–98) | [95] |
| Mihalič et al., 2020 | 25/24/- | NR | 65 | 82 (55–100) | 97 (92–100) | [101] |
| Qin et al., 2020 | 24/26/- | NR | 70 | 92 (74–99) | 80 (59–93) | [110] |
| Qin et al., 2020 | 45/48/- | >6 weeks | 70 | 89 (75–97) | 84 (72–92) | [111] |
| Sharma et al., 2020 | 93/14/- | NR | 72 | 92 | 91 | [102] |
| Ivy et al., 2021 | 74/25/- | NR | 65 | 90 (65–99) | 87 (78–94) | [103] |
| van den Kieboom et al., 2021 | 43/101/- | NR | 80 | 79 | 63 | [105] |
| Wang et al., 2021 | 45/48/- | >6 weeks | 70 | 95 (82–99) | 93 (83–98) | [112] |
| Qin et al., 2022 | 30/40/- | >2.5 years | 70 | 89 | 80 | [113] |
| Dilley et al., 2023 | 485/245/- | >6 weeks | 82 | 81 | 78 | [109] |
a % and 95% confidence interval, if reported; NR, not reported.
Table 2.
Sensitivity and specificity of synovial fluid α-defensin for periprosthetic joint infection diagnosis.
Table 2.
Sensitivity and specificity of synovial fluid α-defensin for periprosthetic joint infection diagnosis.
| Assay | Knee/Hip/Other | Cut-Point | Sensitivity (%) a | Specificity (%) a | Citation |
|---|---|---|---|---|---|
| Lateral flow | |||||
| Bingham et al., 2014 | 61/-/- | NA | 100 (79–100) | 95 (83–99) | [130] |
| Kasparek et al., 2016 | 29/11/- | NA | 67 (35–89) | 93 (75–99) | [131] |
| Sigmund et al., 2017 | 17/30/- | NA | 69 (46–92) | 94 (86–100) | [132] |
| Okroj et al., 2018 | -/26/- | NA | 100 | 68 | [133] |
| Berger et al., 2017 | 85/36/- | NA | 97 (85–100) | 97 (90–99) | [134] |
| Suda et al., 2017 | 19/11/- | NA | 77 | 82 | [135] |
| Balato et al., 2018 | 51/-/- | NA | 88 (75–95) | 97 (87–100) | [136] |
| de Saint Vincent et al., 2018 | 23/13/3 | NA | 89 | 91 | [137] |
| Gehrke et al., 2018 | 99/96/- | NA | 92 (84–97) | 100 (97–100) | [126] |
| Renz et al., 2018 | 151/61/- | NA | 84 (71–94) | 96 (92–99) | [120] |
| Riccio et al., 2018 | 49/22/2 | NA | 85 (70–94) | 97 (84–100) | [138] |
| Sigmund et al., 2018 | 54/17/- | NA | 77 (49–92) | 98 (90–100) | [121] |
| Stone et al., 2018 | 121/62/- | NA | 81 (65–92) | 96 (91–99) | [139] |
| Tahta et al., 2018 | 38/-/- | NA | 92 (80–100) | 98 (90–100) | [98] |
| Plate et al., 2018 | 60/49/- | NA | 90 (68–99) | 92 (85–97) | [140] |
| Carli et al., 2019 | 9 studies | NA | 96 | 82 | [99] |
| Sigmund et al., 2019 | 48/53/- | NA | 69 (51–83) | 94 (85–98) | [141] |
| Sharma et al., 2020 | 93/14/- | NA | 88 | 95 | [102] |
| Abdo et al., 2021 | 53/-/- | NA | 86 (65–97) | 100 (89–100) | [142] |
| de Saint Vincent et al., 2021 | 59/39/8 | NA | 96 | 91 | [143] |
| Deirmengian et al., 2021 | 203/102/- | NA | 94 (84–99) | 95 (91–97) | [115] |
| Ivy et al., 2021 | 74/25/- | NA | 83 (59–96) | 94 (86–98) | [103] |
| Yu et al., 2021 | 82/48/- | NA | 83 | 86 | [144] |
| Zeng et al., 2021 | 1443 total (pooled) | NA | 83 (77–88) | 95 (93–97) | [145] |
| Baker et al., 2022 | 358/36/- | NA | 99 | 87 | [106] |
| Kuiper et al., 2022 | -/57/- | NA | 83 (36–100) | 92 (81–98) | [146] |
| Enzyme-linked immunoassay (ELISA)—cutoff values in mg/L | |||||
| Deirmengian et al., 2014 | 84/11/- | 4.8 | 100 (88–100) | 100 (95–100) | [147] |
| Deirmengian et al., 2014 | 116/33/- | 5.2 | 97 (86–100) | 96 (90–99) | [148] |
| Deirmengian et al., 2015 | 43/3/- | 1.6 | 100 (85–100) | 100 (85–100) | [149] |
| Frangiamore et al., 2016 | 78 total(1st stage) 38 total (2nd stage) | 5.2 5.2 | 100 (86–100) 67 (12–95) | 98 (90–100) 97 (83–99) | [150] |
| Bonanzinga et al., 2017 | 65/91/- | 5.2 | 97 (92–99) | 97 (92–99) | [151] |
| De Vecchi et al., 2018 | 45/21/- | 5.2 | 84 (67–94) | 94 (79–99) | [96] |
| Sigmund et al., 2018 | 54/17/- | 5.2 | 85 (56–97) | 98 (90–100) | [121] |
| Carli et al., 2019 | 9 studies | Pooled | 97 | 87 | [99] |
| Kleiss et al., 2019 | 112/90/- | 5.2 | 78 (67–89) | 97 (93–99) | [152] |
| Abdo et al., 2021 | 53/-/- | 5.2 | 96 (77–100) | 100 (89–100) | [142] |
| Deirmengian et al., 2021 | 203/102/- | 5.2 | 89 (76–96) | 98 (94–99) | [115] |
| Ivy et al., 2021 | 74/25/- | 5.2 | 83 (59–96) | 96 (90–99) | [103] |
| Levent et al., 2021 | 143/116/- | 5.2 | 92 | 92 | [104] |
| Li et al., 2021 | 17/33 | 35.5 | 96 | 100 | [153] |
| Mass spectrometry | |||||
| Iorio et al., 2021 | 88/50/- | 5.2 mg/L | 93 (85–98) | 96 (89–99) | [154] |
| Balato et al., 2022 | 125/-/- | 1 µg/L | 100 (96–100) | 97 (90–98) | [124] |
a % and 95% confidence interval, if reported; NA, not applicable.
Table 3.
Sensitivity and specificity of synovial fluid C-reactive protein (CRP), calprotectin, interleukin-6 (Il-6), leukocyte esterase (LE), and lipocalin for periprosthetic joint infection diagnosis.
Table 3.
Sensitivity and specificity of synovial fluid C-reactive protein (CRP), calprotectin, interleukin-6 (Il-6), leukocyte esterase (LE), and lipocalin for periprosthetic joint infection diagnosis.
| Biomarker | Knee/Hip/Other | Cut-Point | Sensitivity (%) a | Specificity (%) a | Citation |
|---|---|---|---|---|---|
| C-reactive protein (CRP)—cutoff values in mg/L | |||||
| Parvizi et al., 2012 | 43/12/- | 9.5 | 83 | 95 | [158] |
| Parvizi et al., 2012 | 66/-/- | 3.7 | 84 | 97 | [159] |
| Wyles et al., 2013 | -/39/- | 8 | 75 (19–99) | 68 (50–83) | [88] |
| Deirmengian et al., 2014 | 84/11/- | 12.2 | 90 (73–98) | 97 (90–100) | [147] |
| Deirmengian et al., 2014 | 116/33/- | 3 | 98 (86–100) | 79 (70–86) | [148] |
| De Vecchi et al., 2016 | 84/45/- | 10 | 82 (61–93) | 94 (87–98) | [160] |
| Kim et al., 2017 | 197/-/- | 34.9 74.5 | 100 (74–100) 58 (28–85) | 91 (83–95) 100 (97–100) | [91] |
| Lee et al., 2017 | 33 studies | Pooled | 85 (78–90) | 88 (78–94) | [92] |
| Sousa et al., 2017 | 40/15/- | 1.6 6.7 8.0 | 91 78 74 | 88 94 97 | [94] |
| De Vecchi et al., 2018 | 45/21/- | 1.0 | 88 (70–96) | 97 (83–100) | [96] |
| Gallo et al., 2018 | 116/124/- | 8.8 | 92 (73–99) | 100 (95–100) | [161] |
| Tahta et al., 2018 | 38/-/- | 11.7 | 76 (62–97) | 90 (80–100) | [98] |
| Carli et al., 2019 | 9 studies | Pooled | 93 | 89 | [99] |
| Plate et al., 2019 | 91/80/21 | 2.9 | 88 | 82 | [162] |
| Sharma et al., 2020 | 93/14/- | 5.6 | 80 | 92 | [102] |
| Baker et al., 2022 | 358/36/- | 6.9 | 74 | 98 | [106] |
| Grzelecki et al., 2021 | 50/35/- | 6.9 | 64 | 95 | [163] |
| Li et al., 2021 | 17/33/- | 9.0 | 76 | 96 | [153] |
| Wang et al., 2021 | 36/61/- | 7.3 | 85 (70–94) | 93 (83–98) | [164] |
| Praz et al., 2021 | 91/102/- | 2.74.4 | 85 (71–93) 83 (71–94.3) | 77 (68–84) 88 (82–94) | [165] |
| Qin et al., 2022 | 30/40/- | 11.6 | 89 | 49 | [113] |
| Calprotectin—cutoff values in mg/L | |||||
| Wouthuyzen-Bakker et al., 2017 | 10/45/6 | 50 (LF) | 89 (69–98) | 90 (78–96) | [166] |
| Wouthuyzen-Bakker et al., 2018 | 12/21/1 | 50 (LF) | 87 (60–98) | 92 (78–98) | [167] |
| Salari et al., 2020 | 76/-/- | 50 ELISA | 100 (100–100) | 95 (89–100) | [168] |
| Trotter et al., 2020 | 17/42/- | 14 (LF) | 75 (53–90) | 76 (60–87) | [169] |
| Grzelecki et al., 2021 | 50/35/- | 1.5 | 96 | 95 | [163] |
| Warren et al., 2021, 2022 | 123/-/- | 14 (LF) 14 (ELISA) 50 (LF) 50 (ELISA) | 98 98 98 98 | 87 83 96 96 | [170,171] |
| Cheok et al., 2022 | 5 studies | Pooled | 94 (82–98) | 93 (85–97) | [172] |
| Grassi et al., 2022 | 93/-/- | 50 (LF) 50 (ELISA) | 97 (87–100) 92 (79–98) | 94 (84–99) 100 (93–100) | [173] |
| Hantouly et al., 2022 | 8 studies | Pooled | 92 (84–98) | 93 (84–99) | [174] |
| Lazic et al., 2022 | 4/10/- | 50 (LF) | 67 (40–93) | 79 (57–100) | [108] |
| Xing et al., 2022 | 7 studies | Pooled | 94 (87–98) | 93 (87–96) | [175] |
| Interleukin-6 (Il-6)—cutoff values in ng/mL | |||||
| Deirmengian et al., 2014 | 84/11/- | 2.3 | 89 (71–98) | 97 (89–100) | [147] |
| Lee et al., 2017 | 33 studies | Pooled | 81 (70–89) | 94 (88–97) | [92] |
| Xie et al., 2017 | 8 studies | Pooled | 91 (82–96) | 90 (84–95) | [176] |
| Gallo et al., 2018 | 116/124/- | 21.0 | 68 (47–85) | 95 (87–99) | [161] |
| Carli et al., 2019 | 5 studies | Pooled | 97 | 84 | [99] |
| Mihalič et al., 2020 | 25/24/- | 2.3 | 73 (45–100) | 95 (87–100) | [101] |
| Qin et al., 2020 | 45/48/- | 1.86 | 95 (82–99) | 93 (83–98) | [111] |
| Sharma et al., 2020 | 93/14/- | 0.417 | 74 | 88 | [102] |
| Cheok et al., 2022 | 6 studies | Pooled | 86 (74–92) | 94 (90–96) | [172] |
| Li et al., 2022 | 30 studies | Pooled | 87 (75–93) | 90 (85–93) | [177] |
| Qin et al., 2022 | 63/39/- | 1.3 | 90 (74–97) | 89 (73–96) | [178] |
| Qin et al., 2022 | 30/40/- | 2.0 | 91 | 97 | [113] |
| Su et al., 2022 | 78/102/- | 1.2 | 91 (79–97) | 52 (38–66) | [179] |
| Leukocyte esterase (LE) | |||||
| Deirmengian et al., 2015 | 43/3/- | + | 69 (41–89) | 100 (84–100) | [149] |
| De Vecchi et al., 2016 | 84/45/- | + | 93 (74–99) | 97 (91–99) | [160] |
| Lee et al., 2017 | 33 studies | Pooled | 77 | 95 | [92] |
| Shahi et al., 2017 | 659 total | + | 75 | 91 | [180] |
| De Vecchi et al., 2018 | 45/21/- | + + + | 94 (79–99) 56 (38–56) | 97 (83–100) 100 (87–100) | [96] |
| Wang et al., 2018 | 11 studies | Pooled | 90 (76–96) | 97 (95–98) | [181] |
| Carli et al., 2019 | 9 studies 10 studies | + + + | 97 84 | 9396 | [99] |
| Dijkman et al., 2020 | 89/-/- | + + | 39 | 88 | [100] |
| Sharma et al., 2020 | 93/14/- | + + | 81 90 | 9584 | [102] |
| Chisari et al., 2021 | 226/33/- | + + + | 74 51 | 91100 | [182] |
| Grzelecki et al., 2021 | 50/35/- | + + | 82 | 98 | [163] |
| Levent et al., 2021 | 143/116/- | + + | 78 | 91 | [104] |
| Yu et al., 2021 | 82/48/- | + + | 80 | 95 | [144] |
| Grassi et al., 2022 | 93/-/- | + | 46 (30 -63) | 94 (84–99) | [173] |
| Logoluso et al., 2022 | 21/58/- | + | 82 | 99 | [183] |
| Lipocalin | |||||
| Vergara et al., 2018 | 54/18/- | 152 ng/mL | 86 | 77 | [184] |
| Dijkman et al., 2020 | 89/-/- | 740 ng/mL | 92 | 83 | [100] |
| Li et al., 2021 | 17/33/- | 763 ng/mL | 100 | 100 | [153] |
| Huang et al., 2022 | 39/39/- | 263 ng/mL | 93 (77–99) | 98 (89–100) | [107] |
| Svoboda et al., 2022 | 56/33/- | 998 µg/mL | 100 | 100 | [185] |
a % and 95% confidence interval, if reported; LF, lateral flow test; ELISA, enzyme-linked immunoassay.
Table 4.
Variables to consider when profiling the immune response to arthroplasty failure.
| Patient-Related | Sample-Related | Treatment-Related | Failure-Related |
|---|---|---|---|
|
|
|
|
a Aseptic loosening, periprosthetic fracture; b Instability, adverse tissue reaction; PJI, periprosthetic joint infection; NIAF, non-infectious arthroplasty failure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Fisher, C.R.; Patel, R. Profiling the Immune Response to Periprosthetic Joint Infection and Non-Infectious Arthroplasty Failure. Antibiotics 2023, 12, 296. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12020296
AMA Style
Fisher CR, Patel R. Profiling the Immune Response to Periprosthetic Joint Infection and Non-Infectious Arthroplasty Failure. Antibiotics. 2023; 12(2):296. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12020296
Chicago/Turabian StyleFisher, Cody R., and Robin Patel. 2023. "Profiling the Immune Response to Periprosthetic Joint Infection and Non-Infectious Arthroplasty Failure" Antibiotics 12, no. 2: 296. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12020296
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.