

The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England’s Community Pharmacies
 , , , ,
, , , , 
Abstract
:1. Introduction
- reducing need for, and unintentional exposure to, antimicrobials;
- optimising use of antimicrobials;
- investing in innovation, supply and access [3].
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Data Collection
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. PQS Uptake
3.2. Antibiotic Use Background Information
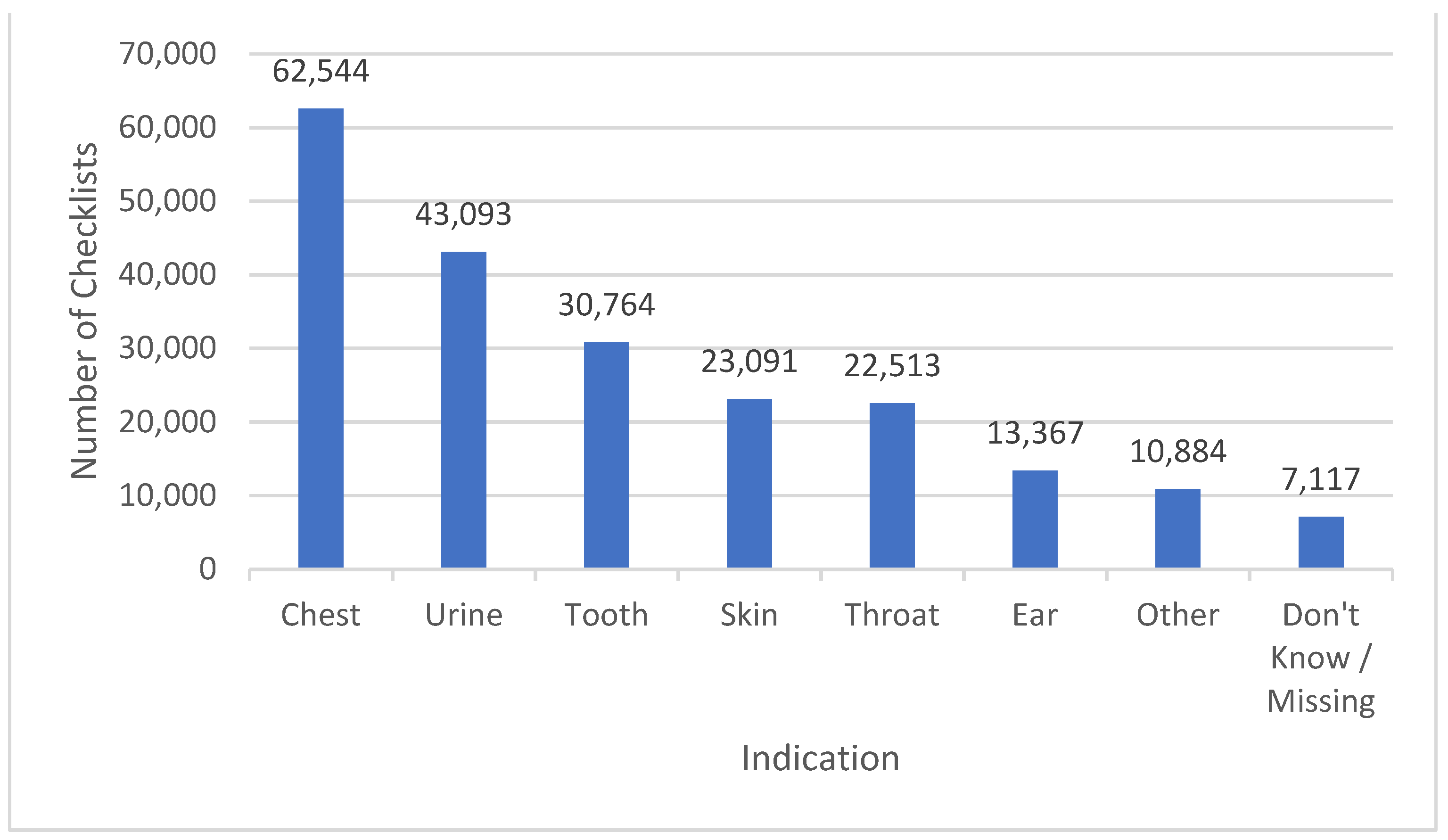
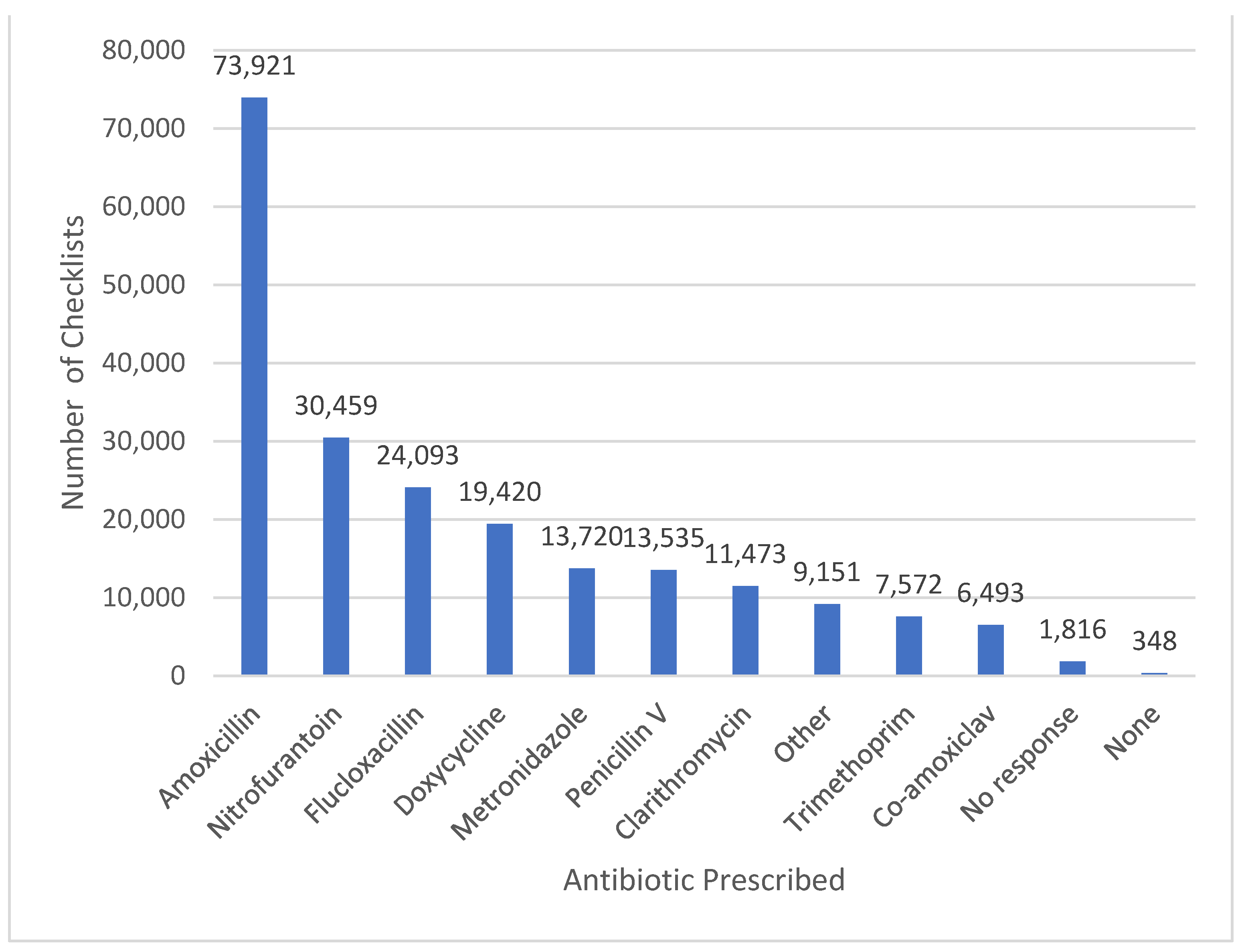
3.3. Patient Infections and Antibiotics Dispensed
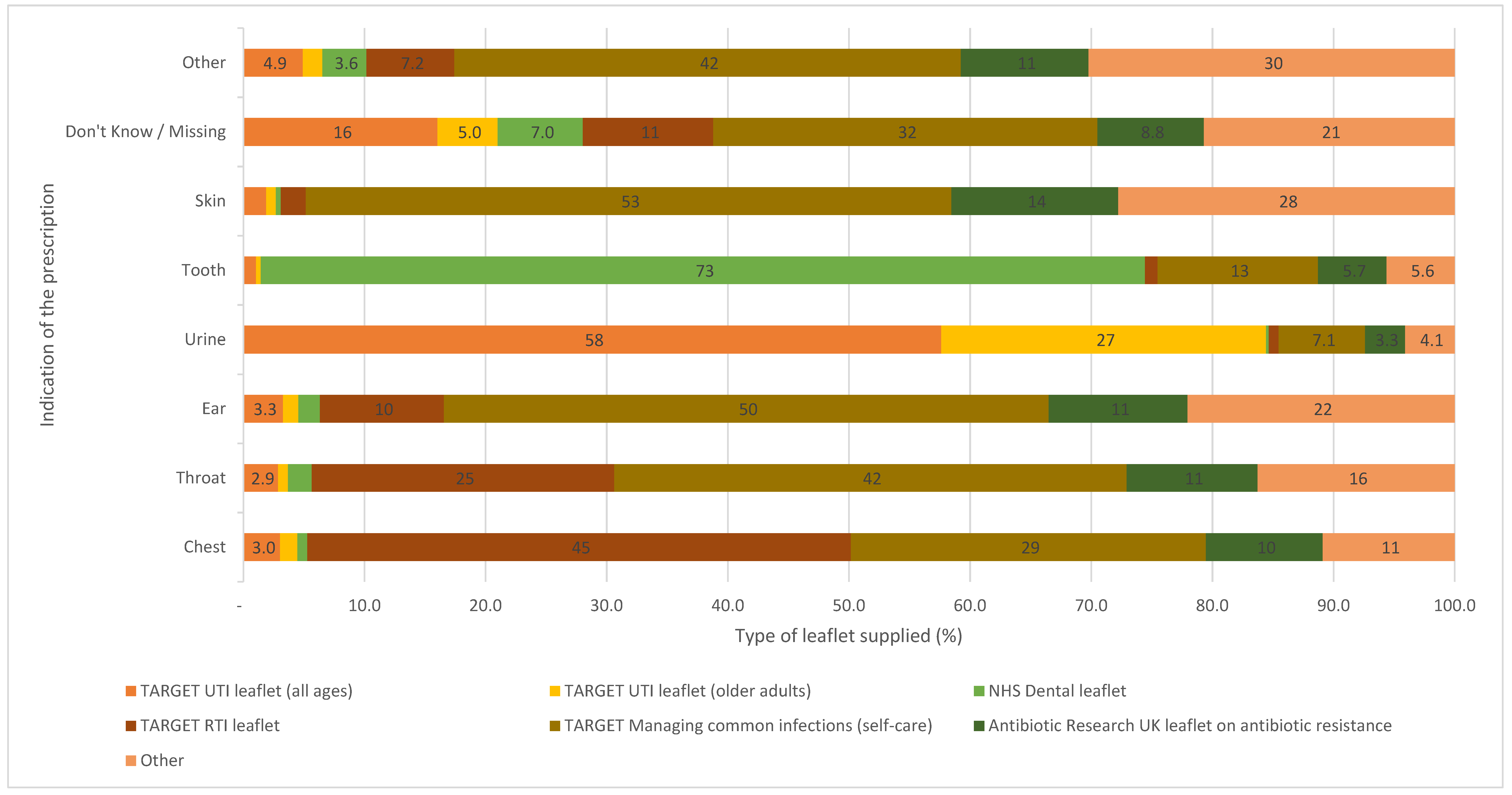
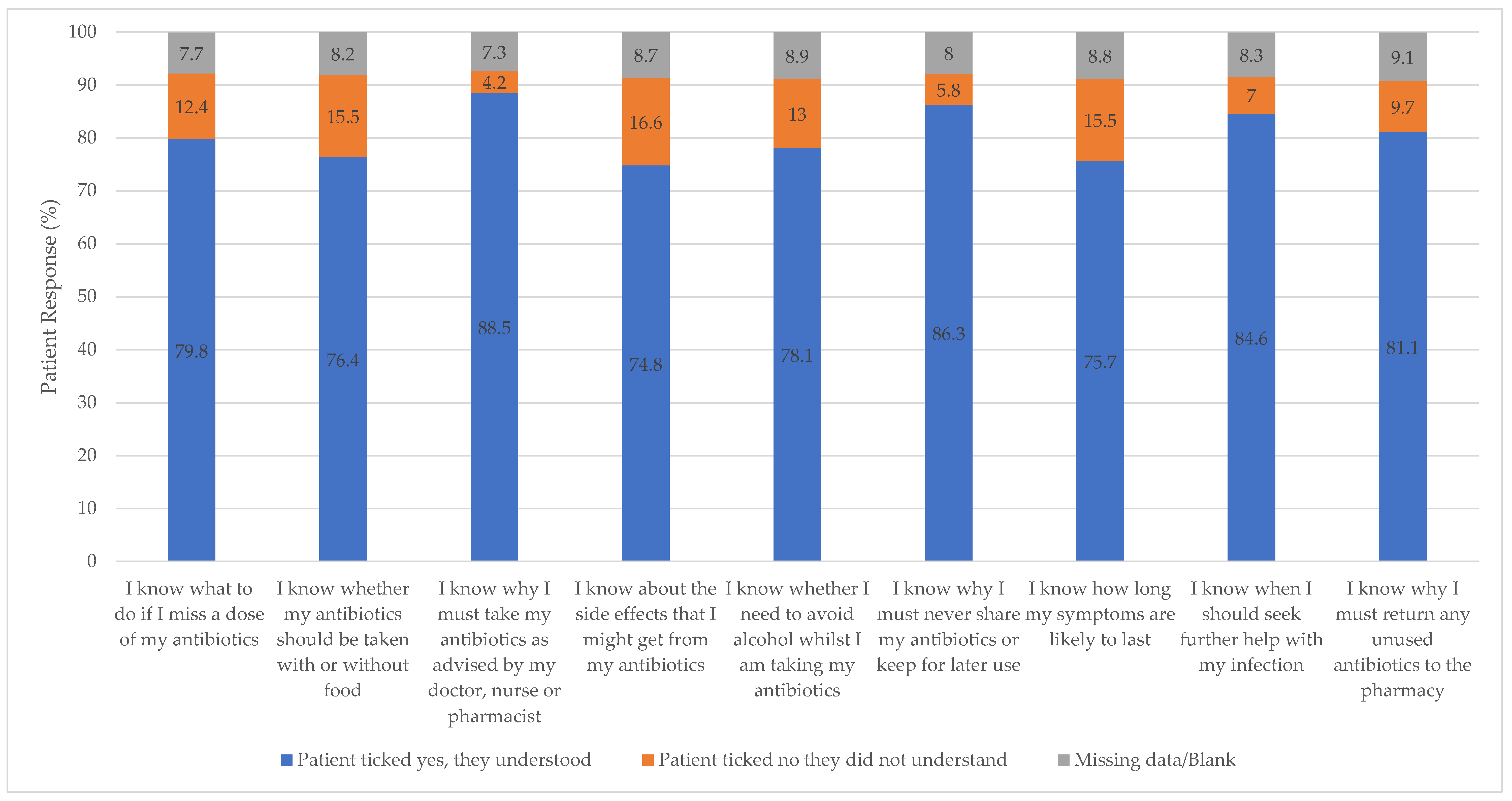
3.4. Provision of Information to Patients
3.5. Influenza Vaccinations
4. Discussion
4.1. Uptake of the TARGET Antibiotic Checklist
4.2. The Role of Community Pharmacy in Managing Infections
4.3. Strengths and Limitations
5. Implications and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care. UK 5-Year Action Plan for Antimicrobial Resistance 2019 to 2024. 2019. Available online: https://www.gov.uk/government/publications/uk-5-year-action-plan-for-antimicrobial-resistance-2019-to-2024 (accessed on 8 January 2022).
- Hara, G.L. Antimicrobial stewardship in hospitals: Does it work and can we do it? J. Glob. Antimicrob. Resist. 2014, 2, 1–6. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2021 to 2022. November 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1118310/ESPAUR-report-2021-to-2022.pdf (accessed on 1 January 2023).
- Todd, A.; Thomson, K.; Kasim, A.; Bambra, C. Cutting care clusters: The creation of an inverse pharmacy care law? An area-level analysis exploring the clustering of community pharmacies in England. BMJ Open 2018, 8, e022109. [Google Scholar] [CrossRef] [PubMed]
- Royal College of General Practitioners. TARGET Antibiotics Toolkit. 2023. Available online: https://elearning.rcgp.org.uk/course/view.php?id=553 (accessed on 1 December 2022).
- Royal College of General Practitioners. TARGET Antibiotic Checklist. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=13511&chapterid=784 (accessed on 8 August 2022).
- Allison, R.; Chapman, S.; Howard, P.; Thornley, T.; Ashiru-Oredope, D.; Walker, S.; Jones, L.F.; McNulty, C.A. Feasibility of a community pharmacy antimicrobial stewardship intervention (PAMSI): An innovative approach to improve patients’ understanding of their antibiotics. JAC-Antimicrob. Resist. 2020, 2, dlaa089. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.V.; Lecky, D.M.; Pursey, F.; Thomas, A.; Ashiru-Oredope, D.; Saei, A.; Thornley, T.; Howard, P.; Dickinson, A.; Ingram, C. Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI). Healthcare 2022, 10, 1288. [Google Scholar] [CrossRef] [PubMed]
- NHS England, NHS Improvement, and Pharmaceutical Services Negotiating Committee. The Community Pharmacy Contractual Framework for 2019/20 to 2023/24: Supporting Delivery for the NHS Long Term Plan; NHS England: London, UK, 2019; p. 26.
- National Health Service. The NHS Long Term Plan. 2019. Available online: https://www.longtermplan.nhs.uk/ (accessed on 1 December 2022).
- National Health Service Business Service Authority. Pharmacy Quality Scheme 2020/21 Part 2 Re-Determination. 2020. Available online: https://www.nhsbsa.nhs.uk/pharmacy-quality-scheme-202021-part-2-re-determination (accessed on 8 August 2022).
- NHS England. Pharmacy Quality Scheme (PQS) 2021–22. 2021. Available online: https://www.nhsbsa.nhs.uk/sites/default/files/2021-08/Pharmacy%20Quality%20Scheme%20Announcement%20September%202021-2022.pdf (accessed on 9 August 2022).
- Health Education England. Antimicrobial Stewardship for Community Pharmacy. 2020. Available online: http://portal.e-lfh.org.uk/component/details/602874 (accessed on 8 August 2022).
- Ashiru-Oredope, D.; Sharland, M.; Charani, E.; McNulty, C.; Cooke, J. Improving the quality of antibiotic prescribing in the NHS by developing a new Antimicrobial Stewardship Programme: Start Smart—Then Focus. J. Antimicrob. Chemother. 2012, 67 (Suppl. s1), i51–i63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, C.; Parekh, S.; Lecky, D.; Loader, J.; Triggs-Hodge, C.; Ashiru-Oredope, D. The National implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022. Antibiot. J. 2023; submitted. [Google Scholar]
- Pharmaceutical Services Negotiating Committee. Pharmacy Quality Scheme. Available online: https://psnc.org.uk/quality-and-regulations/pharmacy-quality-scheme/ (accessed on 8 November 2022).
- National Health Service Business Service Authority. Pharmaceutical List. 2019–20. Available online: https://www.england.nhs.uk/futurenhs-platform/ (accessed on 1 December 2022).
- NHS England. Pharmacy Quality Scheme. 2022. Available online: https://www.england.nhs.uk/ (accessed on 8 November 2022).
- UK Health Security Agency. Community Pharmacy Antibiotic Checklist Data Collection Tool. 2021–22. Available online: https://www.gov.uk/government/publications/european-antibiotic-awareness-day-resources-toolkit-for-healthcare-professionals-in-england (accessed on 8 August 2022).
- NHS Health Research Authority. Is My Study Research? 2023. Available online: https://www.hra-decisiontools.org.uk/research/ (accessed on 16 March 2023).
- National Health Service Business Service Authority. Community Pharmacy Season Influenza Vaccination Advanced Service. 2022. Available online: https://www.nhsbsa.nhs.uk/pharmacies-gp-practices-and-appliance-contractors/dispensing-contractors-information/community-pharmacy-seasonal-influenza-vaccination-advanced-service (accessed on 20 November 2022).
- Pharmaceutical Services Negotiating Committee. Pharmacy Quality Scheme Outcomes. 2021. Available online: https://psnc.org.uk/quality-and-regulations/pharmacy-quality-scheme/pharmacy-quality-scheme-outcomes/ (accessed on 1 December 2022).
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73 (Suppl. S2), ii2–ii10. [Google Scholar] [CrossRef] [PubMed]
- Rusic, D.; Bukić, J.; Seselja Perisin, A.; Leskur, D.; Modun, D.; Petric, A.; Vilovic, M.; Bozic, J. Are we making the most of community pharmacies? Implementation of antimicrobial stewardship measures in community pharmacies: A narrative review. Antibiotics 2021, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Patients in the Midlands Are Encouraged to Return Their Unused Pills to Local Pharmacies as Part of Antibiotic Amnesty Campaign. 2021. Available online: https://www.england.nhs.uk/midlands/2021/11/15/patients-in-the-midlands-are-encouraged-to-return-their-unused-pills-to-local-pharmacies-as-part-of-antibiotic-amnesty-campaign/ (accessed on 8 November 2022).
- NHS England. NHS Community Pharmacist Consultation Service (CPCS)—Integrating Pharmacy into Urgent Care. 2020. Available online: https://www.england.nhs.uk/primary-care/pharmacy/pharmacy-integration-fund/community-pharmacist-consultation-service/ (accessed on 1 January 2022).
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Urinary Tract Infection (Lower): Antimicrobial Prescribing; NICE Guideline [NG109]. 31 October 2018. Available online: https://www.nice.org.uk/guidance/ng109 (accessed on 1 December 2022).
- Jones, L.F.; Owens, R.; Sallis, A.; Ashiru-Oredope, D.; Thornley, T.; Francis, N.A.; Butler, C.; McNulty, C.A. Qualitative study using interviews and focus groups to explore the current and potential for antimicrobial stewardship in community pharmacy informed by the Theoretical Domains Framework. BMJ Open 2018, 8, e025101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Royal College of General Practitioners. Resources for the Community Pharmacy Setting. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=13511 (accessed on 2 January 2023).
- Parekh, S.; Livingstone, C.; Jani, Y.H. Evaluation of the England Community Pharmacy Quality Scheme (2018–2019 and 2019–2020) in reducing harm from NSAIDs in older patients. BMJ Open Qual. 2023, 12, e002002. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Castro-Sanchéz, E.; Bradley, S.; Nathwani, D.; Holmes, A.H.; Davey, P. Implementation of antibiotic stewardship in different settings-results of an international survey. Antimicrob. Resist. Infect. Control 2019, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-R.; Cho, I.H.; Jeong, B.C.; Lee, S.H. Strategies to minimize antibiotic resistance. Int. J. Environ. Res. Public Health 2013, 10, 4274–4305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Social Care. Community Pharmacy Contractual Framework 5-Year Deal: Year 4 (2022 to 2023) and Year 5 (2023 to 2024). 2022. Available online: https://www.gov.uk/government/publications/community-pharmacy-contractual-framework-2019-to-2024/community-pharmacy-contractual-framework-5-year-deal-year-4-2022-to-2023-and-year-5-2023-to-2024 (accessed on 8 November 2022).
- Royal College of General Practitioners. Leaflets to Discuss with Patients. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=12647 (accessed on 8 August 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Were the Antibiotics for the Individual Collecting? % | Was the Patient Taking Any Other Medicines? % | Was the Patient Allergic to Any Antibiotics? % | |
|---|---|---|---|
| Yes | 163,446 (78) | 107,360 (51) | 25,574 (12) |
| No | 42,123 (20) | 90,764 (43) | 165,383 (79) |
| Do not know/missing | 1954 (0.9) | 8307 (4.0) | 14,867 (7.1) |
| No Response | 1335 (0.6) | 2427 (1.2) | 3034 (1.5) |
| Total | 208,858 (100) | 208,858 (100) | 208,858 (100) |
| Response | Patient-Reported Prescription of the Same Antibiotic(s) within Previous 3 Months (%) | Pharmacy Staff Conversation with Patient about Resistance Due to Prescription of the Same Antibiotic(s) within the Previous 3 Months (%) |
|---|---|---|
| Yes | 36,097 (17) | 87,975 (42) |
| No | 156,836 (75) | 35,168 (17) |
| Not applicable | 0 | 67,210 (32) |
| Do not know/missing | 13,203 (6.3) | 9320 (4.5) |
| No response | 2722 (1.3) | 7490 (3.6) |
| Total checklists | 208,858 | 207,163 * |
| Influenza Vaccination Eligibility Category | No of Patients (% of Total) | No of Influenza Vaccines Already Received (% by Eligibility Criterion) | Gave the Patient an Influenza Vaccine on Site (% of Those Who Had Not Yet Received Vaccine) |
|---|---|---|---|
| Over 65 years | 47,622 (23) | 36,712 (77) | 4431 (41) |
| Problem with kidney function * | 2968 (1.4) | 1648 (56) | 265 (20) |
| Problem with liver function * | 740 (0.62) | 388 (52) | 85 (24) |
| Pregnant * | 2262 (1.1) | 1212 (54) | 238 (23) |
| Total | 52,592 (26) | 39,960 (76) | 5019 (36) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parekh, S.; Hayes, C.V.; Loader, J.; Ashiru-Oredope, D.; Hand, K.; Hicks, G.; Lecky, D. The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England’s Community Pharmacies. Antibiotics 2023, 12, 647. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12040647
Parekh S, Hayes CV, Loader J, Ashiru-Oredope D, Hand K, Hicks G, Lecky D. The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England’s Community Pharmacies. Antibiotics. 2023; 12(4):647. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12040647
Chicago/Turabian StyleParekh, Sejal, Catherine V. Hayes, Jill Loader, Diane Ashiru-Oredope, Kieran Hand, Gemma Hicks, and Donna Lecky. 2023. "The Use of the TARGET Antibiotic Checklist to Support Antimicrobial Stewardship in England’s Community Pharmacies" Antibiotics 12, no. 4: 647. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12040647