

The Fragmented Picture of Antimicrobial Resistance in Kenya: A Situational Analysis of Antimicrobial Consumption and the Imperative for Antimicrobial Stewardship

Abstract
:1. Introduction
2. Results
3. Drivers of Antibiotic Resistance
3.1. Socio-Economic Factors and Related Behaviors
3.2. Antibiotic Consumption
3.2.1. Antibiotic Use in Human Medicine
3.2.2. Antibiotic Use in Animal Health and Agriculture
3.3. Antibiotic Resistance
3.3.1. AMR Surveillance
3.3.2. AMR Laboratory and Diagnostic Capacity
3.4. Antimicrobial Stewardship
3.4.1. AMS and the One Health Approach

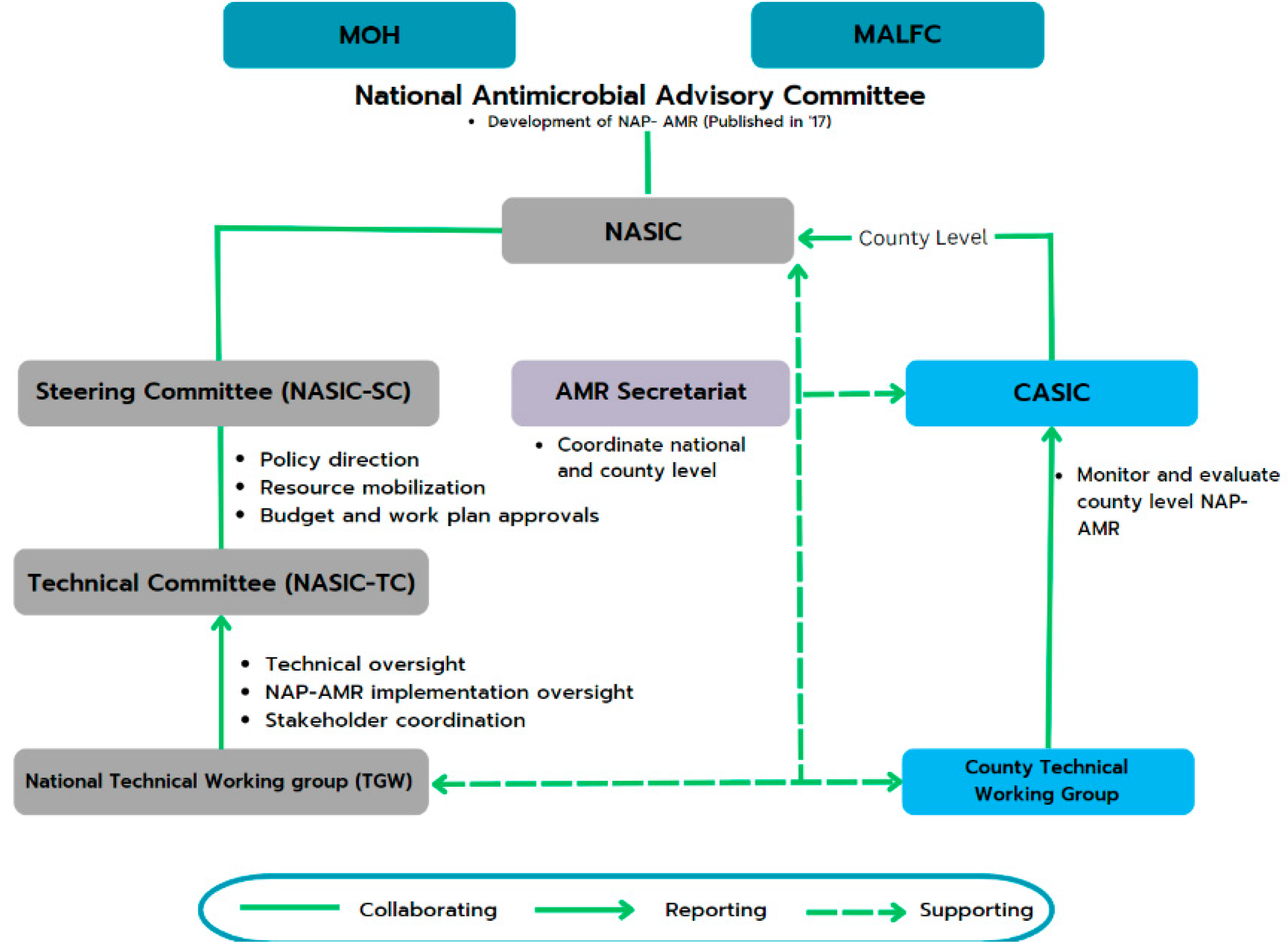
- At the national level, the National Antimicrobial Stewardship Interagency Committee (NASIC) and Technical Committees oversee and guide AMR-related activities. These committees report to the MOH and the Ministry of Agriculture, Livestock, Fisheries, and Cooperatives for guidance and funding.
- At the county level, 8 of Kenya’s 47 counties have County Antimicrobial Stewardship Interagency Committees (CASICs). These committees play a pivotal role in monitoring NAP implementation and allocating resources for AMR-related efforts [13].
3.4.2. AMR Awareness and Communication
3.4.3. IPC, Water, Sanitation and Hygiene (WASH) and Immunization
3.4.4. Funding for Programs
4. Expert Opinion
5. Potential Ways Forward
6. Limitations
7. Materials and Methods
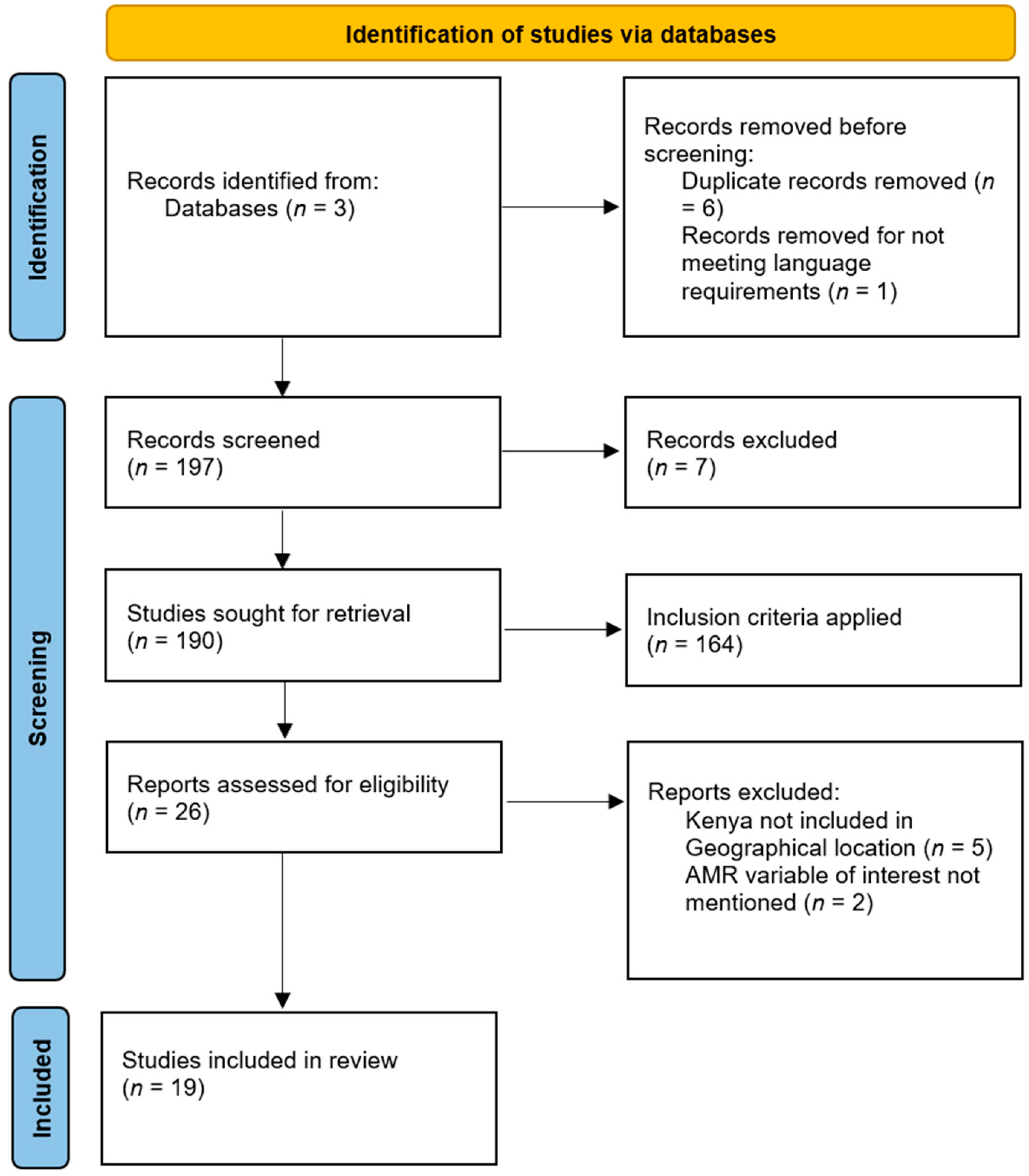
7.1. Scoping Review
7.1.1. Identifying Relevant Studies
7.1.2. Study Selection
7.1.3. Charting the Data
7.1.4. Summarizing and Reporting the Results
7.2. Expert Opinion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 27 November 2023).
- Rosenblatt-Farrell, N. The landscape of antibiotic resistance. Environ. Health Perspect. 2009, 117, A244–A250. [Google Scholar] [CrossRef]
- Abushaheen, M.A.; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Devang Dicakar, D.; Jhugroo, C.; Vellappally, S.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Disease-a-Month 2020, 66, 100971. [Google Scholar] [CrossRef] [PubMed]
- Dadgostar, P. Antimicrobial resistance: Implications and costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Catena, F.; Coccolini, F.; Hardcastle, T.C.; Roques, C.; Salameh, P. Drivers of antibiotic resistance transmission in low- and middle-income countries from a “one health” perspective—A review. Antibiotics 2020, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, A.; Reid, S.; Assefa, Y. A review of National Action Plans on antimicrobial resistance: Strengths and weaknesses. Antimicrob. Resist. Infect. Control 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2022. Global Antimicrobial Resistance and Use Surveillance System (GLASS). 2023. Available online: https://iris.who.int/bitstream/handle/10665/364996/9789240062702-eng.pdf?sequence=1 (accessed on 27 November 2023).
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrob. Resist. Infect. Control 2021, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Gulumbe, B.H.; Haruna, U.A.; Almazan, J.; Ibrahim, I.H.; Faggo, A.A.; Bazata, A.Y. Combating the menace of antimicrobial resistance in Africa: A review on Stewardship, surveillance and Diagnostic Strategies. Biol. Proced. Online 2022, 24, 19. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Levy Hara, G.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance—The need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Rolfe, R.; Kwobah, C.; Muro, F.; Ruwanpathirana, A.; Lyamuya, F.; Bodinayake, C.; Nagahawatte, A.; Piyasiri, B.; Sheng, T.; Bollinger, J.; et al. Barriers to implementing antimicrobial stewardship programs in three low- and middle-income country tertiary care settings: Findings from a multi-site qualitative study. Antimicrob. Resist. Infect. Control 2021, 10, 60. [Google Scholar] [CrossRef]
- World Health Organization. Kenya National Action Plan on Antimicrobial Resistance: Review of Progress in the Human Health Sector. Antimicrobial Resistance Policy Information and Action Brief Series. 2022. Available online: https://iris.who.int/bitstream/handle/10665/364530/9789240062689-eng.pdf?sequence=1 (accessed on 28 November 2023).
- OneHealthTrust.ResistanceMap—Antibiotic-Resistance. 2015. Available online: https://resistancemap.cddep.org/AntibioticResistance.php (accessed on 28 November 2023).
- Ita, T.; Luvsansharav, U.O.; Smith, R.M.; Mugoh, R.; Ayodo, C.; Oduor, B.; Jepleting, M.; Oguta, W.; Ouma, C.; Juma, J.; et al. Prevalence of colonization with multidrug-resistant bacteria in communities and hospitals in Kenya. Sci. Rep. 2022, 24, 12. [Google Scholar] [CrossRef] [PubMed]
- Global Antibiotic Resistance Partnership—Kenya Working Group. Situation Analysis and Recommendations: Antibiotic Use and Resistance in Kenya. Center for Disease Dynamics, Economics & Policy. 2011. Available online: https://onehealthtrust.org/wp-content/uploads/2017/06/kenya_full_report_web_15.pdf (accessed on 28 November 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.P.; Hafner, T.; Twesigye, G.; Ndiaye, A.; Kiggundu, R.; Mekonnen, N.; Kusu, N.; Berthe, S.; Lusaya, E.P.; Acho, A.; et al. Strengthening multisectoral coordination on antimicrobial resistance: A landscape analysis of efforts in 11 countries. J. Pharm. Policy Pract. 2021, 28, 14. [Google Scholar] [CrossRef] [PubMed]
- Moirongo, R.M.; Aglanu, L.M.; Lamshöft, M.; Adero, B.O.; Yator, S.; Anyona, S.; May, J.; Lorenz, E.; Eibach, D. Laboratory-based surveillance of antimicrobial resistance in regions of Kenya: An assessment of capacities, practices, and barriers by means of multi-facility survey. Front. Public Health 2022, 10, 1003178. [Google Scholar] [CrossRef]
- Omulo, S.; Thumbi, S.M.; Lockwood, S.; Verani, J.R.; Bigogo, G.; Masyongo, G.; Call, D.R. Evidence of superficial knowledge regarding antibiotics and their use: Results of two cross-sectional surveys in an urban informal settlement in Kenya. PLoS ONE 2017, 12, e0185827. [Google Scholar] [CrossRef]
- Mbugua, S.M.; Njoroge, G.; Kijogi, C.; Kamita, M.; Kimani, R.; Mwaura, P.; Aidi, B.W.; Gitaka, J. Exploring perspectives on antimicrobial stewardship: A qualitative study of health managers in Kenya. Glob. Health Res. Policy 2020, 5, 49. [Google Scholar] [CrossRef]
- Kimani, T.; Kiambi, S.; Eckford, S.; Njuguna, J.; Makonnen, Y.; Rugalema, G.; Morzaria, S.P.; Lubroths, J.; Fasina, F.O. Expanding beyond zoonoses: The benefits of a national One Health coordination mechanism to address antimicrobial resistance and other shared health threats at the human-animal-environment interface in Kenya. Rev. Sci. Tech. Off. Int. Des Epizoot. 2019, 38, 155–171. [Google Scholar] [CrossRef]
- Matee, M.; Mshana, S.E.; Mtebe, M.; Komba, E.V.; Moremi, N.; Lutamwa, J.; Kapona, O.; Sekamatte, M.; Mboera, L.E. Mapping and gap analysis on antimicrobial resistance surveillance systems in Kenya, Tanzania, Uganda and Zambia. Bull. Natl. Res. Cent. 2023, 47, 12. [Google Scholar] [CrossRef]
- Godman, B.; Egwuenu, A.; Wesangula, E.; Schellack, N.; Kalungia, A.C.; Tiroyakgosi, C.; Kgatlwane, J.; Mwita, J.C.; Patrick, O.; Lum Niba, L.; et al. Tackling antimicrobial resistance across sub-Saharan Africa: Current challenges and implications for the future. Expert Opin. Drug Saf. 2022, 21, 1089–1111. [Google Scholar] [CrossRef]
- Othieno, J.; Njagi, O.; Azegele, A. Opportunities and challenges in antimicrobial resistance behavior change communication. One Health 2020, 11, 100171. [Google Scholar] [CrossRef]
- Kariuki, S.; Kering, K.; Wairimu, C.; Onsare, R.; Mbae, C. Antimicrobial resistance rates and surveillance in Sub-Saharan Africa: Where are we now? Infect. Drug Resist. 2022, 15, 3589–3609. [Google Scholar] [CrossRef] [PubMed]
- Acam, J.; Kuodi, P.; Medhin, G.; Makonnen, E. Antimicrobial prescription patterns in East Africa: A systematic review. Syst. Rev. 2023, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Otieno, P.A.; Campbell, S.; Maley, S.; Arunga, T.O.; Okumu, M.O. A Systematic Review of Pharmacist-Led antimicrobial stewardship programs in Sub-Saharan Africa. Int. J. Clin. Pract. 2022, 2022, 3639943. [Google Scholar] [CrossRef] [PubMed]
- Murila, B.L.; Nyamu, D.G.; Kinuthia, R.; Njogu, P.M. Rational use of antibiotics and covariates of clinical outcomes in patients admitted to intensive care units of a tertiary hospital in Kenya. Hosp. Pract. 2022, 50, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Kamere, N.; Garwe, S.T.; Akinwotu, O.O.; Tuck, C.; Krockow, E.M.; Yadav, S.; Ganiyu Olawale, A.; Diyaolu, A.H.; Munkombwe, D.; Muringu, E.; et al. Scoping review of national antimicrobial stewardship activities in eight African countries and adaptable recommendations. Antibiotics 2022, 11, 1149. [Google Scholar] [CrossRef]
- Collignon, P.; Beggs, J.J. Socioeconomic enablers for contagion: Factors impelling the Antimicrobial Resistance epidemic. Antibiotics 2019, 8, 86. [Google Scholar] [CrossRef]
- Cruz, M. Quality-Assured Pharmacies Improving Healthcare for People with Low Incomes in Kenya. 2021. Available online: https://www.businesscalltoaction.org/news/quality-assured-pharmacies-Improving-healthcare-for-people-with-low-incomes-in-Kenya (accessed on 28 November 2023).
- Baptista, P.; Mignano, K.; World Bank Group. Bringing Safe, Quality Medicine to All Goodlife Pharmacy: A Health Hub for East Africa. International Finance Corporation. 2018. Available online: https://www.ifc.org/content/dam/ifc/doclink/2018/goodlife-pharmacy.pdf (accessed on 28 November 2023).
- Koech, L.C.; Irungu, B.; Ng’ang’a, M.; Ondicho, J.; Keter, L. Quality and brands of amoxicillin formulations in Nairobi, Kenya. BioMed Res. Int. 2020, 2020, 7091278. [Google Scholar] [CrossRef]
- Moturi, A.K.; Alegana, V.A.; Mumo, E.; Snow, R.W.; Okiro, E.A.; Macharia, P.M. Geographic accessibility to public and private health facilities in Kenya in 2021: An updated geocoded inventory and spatial analysis. Front. Public Health 2022, 3, 10. [Google Scholar] [CrossRef]
- Walcott-Bryant, A.; Ogallo, W.; Remy, S.L.; Tryon, K.; Shena, W.; Bosker-Kibacha, M. Addressing care continuity and quality challenges in the management of hypertension: Case study of the private health care sector in Kenya. J. Med. Internet Res. 2021, 23, e18899. [Google Scholar] [CrossRef] [PubMed]
- Rousham, E.K.; Unicomb, L.; Islam, M.A. Human, animal and environmental contributors to antibiotic resistance in low-resource settings: Integrating behavioural, epidemiological and One Health approaches. Proc. R. Soc. Biol. 2018, 285, 20180332. [Google Scholar] [CrossRef] [PubMed]
- Alila, P.O.; Atieno, R. Agricultural Policy in Kenya: Issues and Processes. Institute for Development Studies. 2023. Available online: https://www.fao.org/fileadmin/user_upload/fsn/docs/Ag_policy_Kenya.pdf (accessed on 28 November 2023).
- Mehdi, Y.; Létourneau-Montminy, M.P.; Gaucher, M.L.; Chorfi, Y.; Suresh, G.; Rouissi, T.; Kaur Brar, S.; Cote, C.; Avalos Ramirez, A.; Godbout, S. Use of antibiotics in broiler production: Global impacts and alternatives. Anim. Nutr. 2018, 4, 170–178. [Google Scholar] [CrossRef]
- Marshall, B.; Levy, S.B. Food animals and antimicrobials: Impacts on human health. Clin. Microbiol. Rev. 2011, 24, 718–733. [Google Scholar] [CrossRef]
- Ministry of Health. Kenya National Action Plan on Antimicrobial Resistance: Review of Progress in the Human Health Sector. Government of Kenya. 2017. Available online: https://www.health.go.ke/wp-content/uploads/2020/02/Kenya-National-Action-Plan-on-Antimicrobial-Resistance-Review-of-Progress-in-the-Human-Health-Sector.pdf (accessed on 28 November 2023).
- Fitzgibbon, J.E.; Wallis, C.L. Laboratory challenges Conducting international clinical research in Resource-Limited settings. J. Acquir. Immune Defic. Syndr. 2014, 65 (Suppl. S1), S36–S39. [Google Scholar] [CrossRef]
- Munyua, P.M.; Njenga, M.K.; Osoro, E.M.; Onyango, C.O.; Bitek, A.O.; Mwatondo, A.; Muturi, M.L.; Musee, N.; Bigogo, G.; Otiang, E.; et al. Successes and challenges of the One Health approach in Kenya over the last decade. BMC Public Health 2019, 19, 465. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Cheng, Z.; Zhang, X.; Lv, C.; Guo, C.; Liu, H.; Chang, Y.F.; Chen, S.; Guo, X.; Zhou, X.N.; et al. Global antimicrobial resistance: A system-wide comprehensive investigation using the Global One Health Index. Infect. Dis. Poverty 2022, 11, 92. [Google Scholar] [CrossRef] [PubMed]
- Canva. Modern Steps Project Management Process Infographic Graph. 2023. Available online: https://www.canva.com/design/DAF7o29Vm1s/NVHknSHounp_bUn33qQl8Q/edit (accessed on 28 November 2023).
- Ministry of Health of Kenya. Regional Meeting in Nairobi Aims to Combat Antimicrobial Resistance (AMR) Threat | Ministry of Health. Retrieved February 19, 2024. Available online: https://www.health.go.ke/regional-meeting-nairobi-aims-combat-antimicrobial-resistance-amr-threat (accessed on 28 November 2023).
- Mbaye, R.; Gebeyehu, R.; Hossmann, S.; Mbarga, N.; Bih-Neh, E.; Eteki, L.; Thelma, O.A.; Oyerinde, A.; Kiti, G.; Mburu, Y.; et al. Who is telling the story? A systematic review of authorship for infectious disease research conducted in Africa, 1980–2016. BMJ Glob. Health 2019, 4, e001855. [Google Scholar] [CrossRef]
- Kokutse, F. Lead Authors from Low-Income Countries on the Decrease. University World News. 2022. Available online: https://www.universityworldnews.com/post.php?story=20220628095022532 (accessed on 1 December 2023).
- Unicef. WASH and Infection Prevention and Control in Health Care Facilities Guidance Note. 2020. Available online: https://www.unicef.org/media/66386/file/WASH-COVID-19-infection-prevention-and-control-in-health-care-facilities-2020.pdf (accessed on 1 December 2023).
- Müller, C. Foreign Aid and the Challenges in Kenya. 2022. Available online: https://ieakenya.or.ke/blog/foreign-aid-and-the-challenges-in-kenya/ (accessed on 1 December 2023).
- Lancaster, C. Aid effectiveness in Africa: The unfinished agenda. J. Afr. Econ. 1999, 8, 487–503. [Google Scholar] [CrossRef]
- BRAC. BRAC Poultry Rearing. 2017. Available online: https://www.brac.net/brac-enteprises/item/885-brac-poultry (accessed on 1 December 2023).
- Saleque, M. Small Scale Poultry Farming Is a Key to Improving Livelihoods: BRAC Experience in Africa. ResearchGate. 2015. Available online: https://www.researchgate.net/publication/318122927_Small_scale_poultry_farming_is_a_key_to_improving_livelihoods_BRAC_experience_in_Africa (accessed on 1 December 2023).
- Ombelet, S.; Ronat, J.B.; Walsh, T.; Yansouni, C.P.; Cox, J.; Vlieghe, E.; Martiny, D.; Semret, M.; Vandenberg, O.; Jacobs, J.; et al. Clinical bacteriology in low-resource settings: Today’s solutions. Lancet Infect. Dis. 2018, 18, e248–e258. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-SCR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Corlett, R.T. Trouble with the Gray Literature. Biotropica 2010, 43, 3–5. [Google Scholar] [CrossRef]
- Godin, K.; Stapleton, J.; Kirkpatrick, S.I.; Hanning, R.M.; Leatherdale, S.T. Applying systematic review search methods to the grey literature: A case study examining guidelines for school-based breakfast programs in Canada. Syst. Rev. 2015, 4, 138. [Google Scholar] [CrossRef] [PubMed]
- Horsley, T.; Dingwall, O.; Sampson, M. Checking reference lists to find additional studies for systematic reviews. Cochrane Libr. 2011, 8, 1465–1858. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, M.; Sharma, A.; Vong, S. Developing a situation analysis tool to assess containment of antimicrobial resistance in South East Asia. BMJ 2017, 358, j3760. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Citation | Setting | Study Design | Variable | Summarized Key Findings |
|---|---|---|---|---|
| WHO, 2022 [5] | Kenya | Government and policy reports | Review of Kenya’s NAP | Established functional national-level governance structures and advancing efforts to create county-level structures. Introducing antimicrobial consumption (AMC) surveillance. |
| WHO, 2021 [7] | Global | Government and policy reports | Review of Kenya’s GLASS progress | Reported to GLASS for two consecutive years and yet to submit AMR data for this year. Has 10 surveillance sites in the national system. |
| Global Antibiotic Resistance Partnership—Kenya Working Group, 2011 [16] | Kenya | Government and policy reports | AMR situational analysis | AMR concerns: Amplified by inadequate hospital infection control practice (IPC). Compounded by the presence of counterfeit drugs. Limited research and surveillance systems. |
| Joshi et al., 2021 [18] | Kenya among other LMICs | Quantitative situational analysis | Strengthening multi-sectoral coordination | Aimed to strengthen and implement stewardship in human health and in animal health sectors. |
| Moirongo et al., 2022 [19] | Kenya | Quantitative survey | Laboratory-based surveillance of AMR | Most labs lack bacterial culture testing services. External quality assessment program underutilized for cultures in Antimicrobial Susceptibility Testing (AST) facilities. |
| Omulo et al., 2017 [20] | Kenya | Qualitative study | AMR awareness in Kibera Informal Settlement | The majority of respondent’s lack understanding of antibiotics and proper usage. Healthcare workers have high trust among the populace. Opportunity for educational interventions. |
| Mbugua et al., 2020 [21] | Kenya | Cross-sectional Qualitative study | Perspectives of Hospital Managers on AMS | AMS implementation: Lacking due to the absence of core complementary health services. Health managers acknowledge the importance of AMS programs. Focus on implementing AMS in hospitals |
| Kimani et al., 2019 [22] | Kenya | Qualitative study | National One Health approach to AMR | Significant progress in addressing diverse health threats. Gaps exist: lacking extensive coordination for all One Health issues; focus needed on both zoonosis and AMR challenges. |
| Matee et al., 2023 [23] | Kenya, Tanzania, Uganda and Zambia | Mixed-methods Review | Performance in addressing AMR | Essential to strengthen National Integrated AMR Surveillance systems. Includes community settings and address AMR across human, animal, food, and environmental sectors. Crucial to establish a clear data-sharing protocol for AMR information in the region. |
| Iskandar et al., 2021 [8] | LMICS | Mixed methods Review | AMR Surveillance | LMICs show AMR surveillance progress. Tailored action plans are vital, reflecting individual country contexts. Alignment of regional, national, and international efforts is crucial. |
| Gulumbe et al., 2022 [9] | Africa | Mixed methods Review | Review on stewardship, surveillance, and diagnostics | Inadequate action in remote and primary healthcare settings. Lack of affordable diagnostic tools, stewardship programs, and surveillance. Increased funding, government legislation, enforcement, and civil society advocacy are needed. |
| Godman et al., 2022 [24] | Sub-Saharan Africa | Mixed-methods Review | Challenges and implications of tackling AMR | Limited personnel, expertise, capacity, and resources for NAP activities. Absence of focal points to lead NAPs. Conflicting demands and donor-related priorities. |
| Iskandar et al., 2020 [5] | LMICS | Literature review | Review of AMR from a “one Health” perspective | Limited resources, economic hardships, conflicts, epidemics, and political hurdles. Shift focus to individuals and governments. Prioritize education, training, research, and socio-ecological behavior change. |
| Othieno et al., 2020 [25] | Kenya | Literature review | AMR communication strategy | Enhancing NAP through Communication: Crucial to create effective communication strategies. Aims to drive behavioral changes among all involved in AMR efforts. |
| Kariuki et al., 2022 [26] | Sub-Saharan Africa | Literature review | Situational analysis of AMR rates and Surveillance. | Kenya stands out as a well-implemented NAP example in the region. |
| Acam et al., 2023 [27] | East Africa | Literature review | Antibiotic prescription patterns | Indicates inappropriate antimicrobial use, contributing to antimicrobial resistance. Study findings underscore the need for action to improve antimicrobial prescription practices. |
| Otieno et al., 2022 [28] | Sub-Saharan Africa | Literature review | Pharmacist-led AMS programs | Pharmacist-led interventions: Result in improved guideline adherence and reduced antimicrobial therapy and healthcare costs. Challenges include guideline absence, prescriber attitudes, lack of AMS teams, limited resources, and infrastructure. |
| Murila et al., 2022 [29] | Kenya | Retrospective review | Rational use of antibiotics at KNH | High incidence of irrational antibiotic prescribing in Kenyatta National Hospital critical care unit (CCU). Mainly attributed to incorrect choice and duration of use. Emphasizes proper antibiotic selection and duration for better management. |
| Kamere et al., 2022 [30] | Kenya among African nations | Scoping review | National Antimicrobial Stewardship Activities | Vital to align political commitment with investment in technical workforce capacity. Effective AMR addressing requires a holistic approach. |
| Contributory Factors | Potential Issues | Proposed Interventions |
|---|---|---|
| Use of antibiotics in medical fields |
|
|
| Use of antibiotics in veterinary and agricultural fields |
|
|
| Healthcare divide |
|
|
| IPC, WASH and Immunization |
|
|
| Amr Surveillance and Diagnostic capacity |
| Promote decentralization by:
|
| AMR awareness and communication |
|
|
| AMS and Governance |
|
|
| Reliance on external funding |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohaili, A.; Asin, J.; Thomas, P.P.M. The Fragmented Picture of Antimicrobial Resistance in Kenya: A Situational Analysis of Antimicrobial Consumption and the Imperative for Antimicrobial Stewardship. Antibiotics 2024, 13, 197. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics13030197
Sohaili A, Asin J, Thomas PPM. The Fragmented Picture of Antimicrobial Resistance in Kenya: A Situational Analysis of Antimicrobial Consumption and the Imperative for Antimicrobial Stewardship. Antibiotics. 2024; 13(3):197. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics13030197
Chicago/Turabian StyleSohaili, Aarman, Judith Asin, and Pierre P. M. Thomas. 2024. "The Fragmented Picture of Antimicrobial Resistance in Kenya: A Situational Analysis of Antimicrobial Consumption and the Imperative for Antimicrobial Stewardship" Antibiotics 13, no. 3: 197. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics13030197