
Supplementation with Vitamins C and E and Exercise-Induced Delayed-Onset Muscle Soreness: A Systematic Review


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search
2.3. Search Strategy
2.4. Data Extraction
2.5. Quality Assessment and Risk of Bias
3. Results
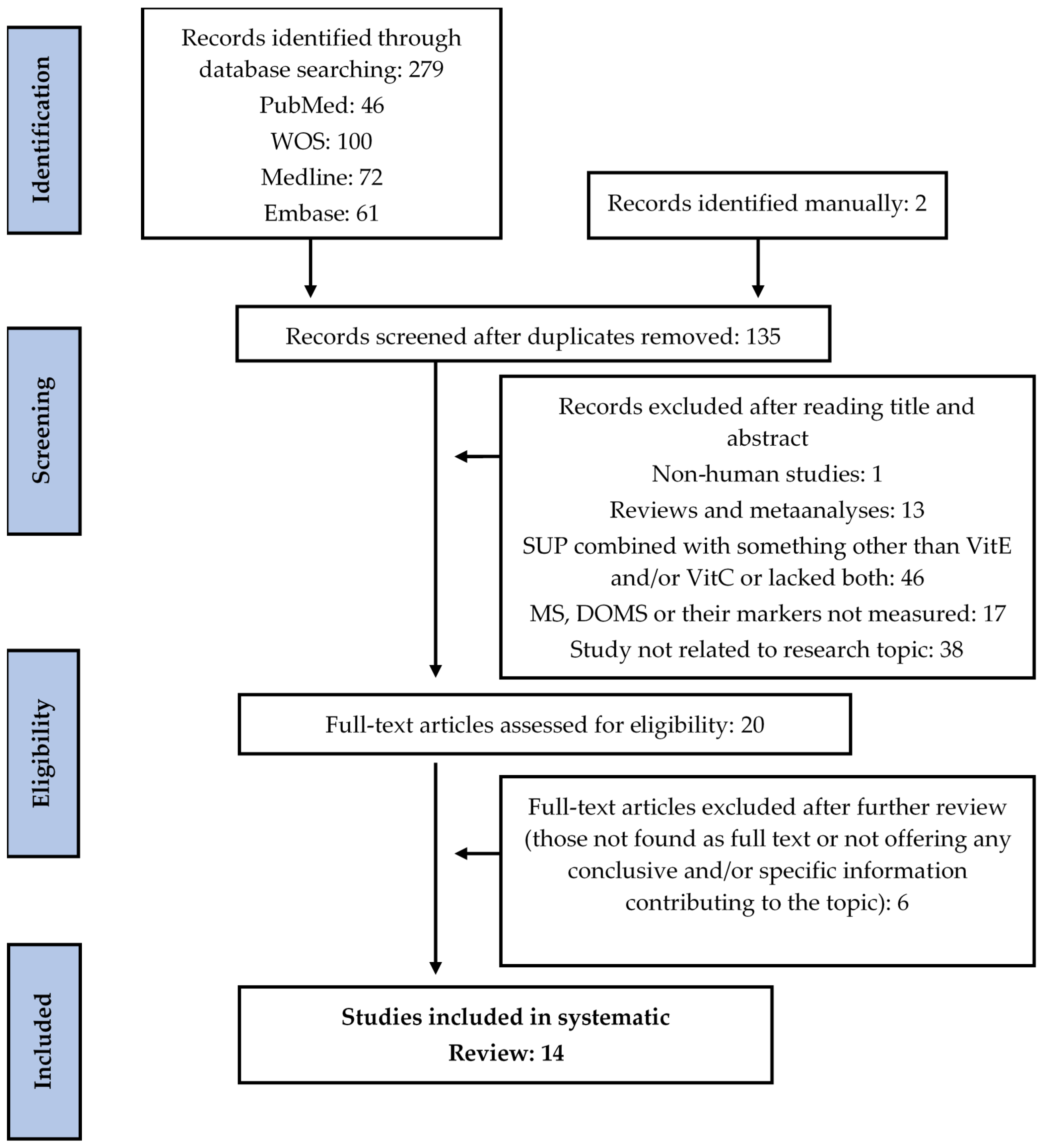
3.1. Study Selection
3.2. Characteristics of the Studies
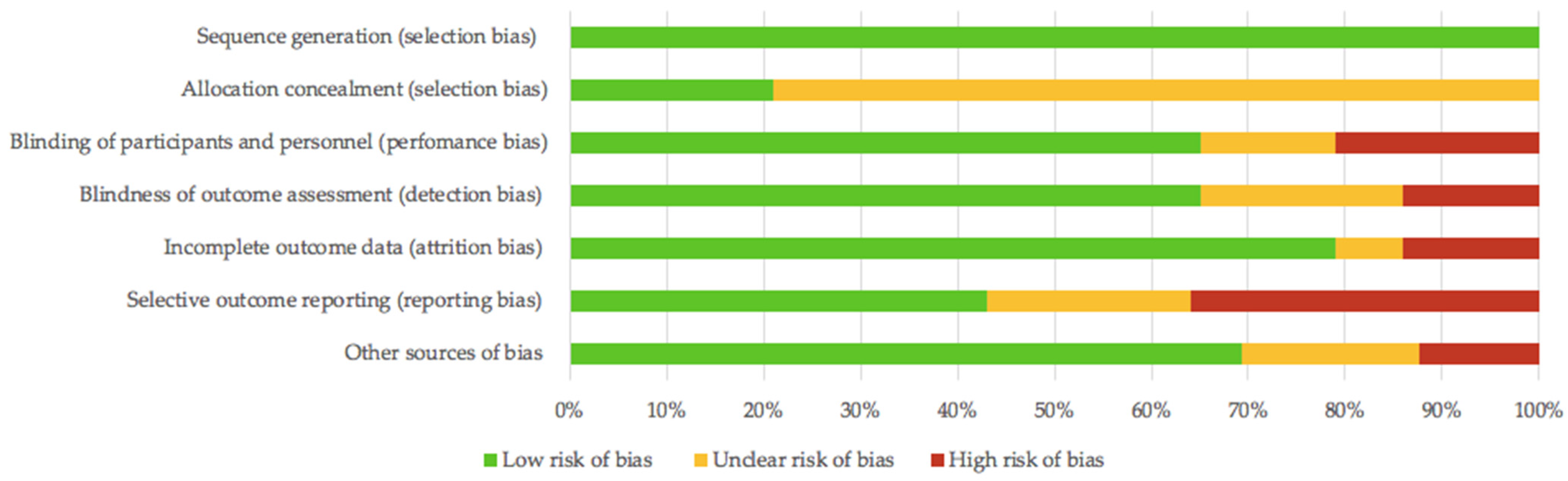
3.3. Quality Assessment and Risk of Bias
3.4. Results of Individual Studies
3.4.1. Acute Supplementation with Antioxidant Vitamins
3.4.2. Chronic Supplementation with Antioxidant Vitamins
Single Exercise Session
Chronic Exercise Protocol
4. Discussion
4.1. Comparison Statement
4.2. Supplementation Protocols
4.3. Eccentric Exercise Regimen
4.4. Variables besides DOMS
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Armstrong, R.B. Mechanisms of Exercise-Induced Delayed Onset Muscular Soreness: A Brief Review. Med. Sci. Sports Exerc. 1984, 16, 529–538. [Google Scholar] [CrossRef]
- Cheung, K.; Hume, P.A.; Maxwell, L. Delayed Onset Muscle Soreness: Treatment Strategies and Performance Factors. Sport. Med. 2003, 33, 145–164. [Google Scholar] [CrossRef]
- Theunissen, E.; Lecouvet, F.; Vanmarsenille, J.M. Delayed Onset Muscle Soreness (DOMS). Louv. Med. 2014, 133, 209–213. [Google Scholar]
- Hotfiel, T.; Freiwald, J.; Hoppe, M.W.; Lutter, C.; Forst, R.; Grim, C.; Bloch, W.; Hüttel, M.; Heiss, R. Advances in Delayed-Onset Muscle Soreness (DOMS): Part I: Pathogenesis and Diagnostics. Sportverletz. Sportschaden 2018, 32, 243–250. [Google Scholar] [CrossRef]
- Lewis, P.B.; Ruby, D.; Bush-Joseph, C.A. Muscle Soreness and Delayed-Onset Muscle Soreness. Clin. Sports Med. 2012, 31, 255–262. [Google Scholar] [CrossRef]
- Asmussen, E. Positive and Negative Muscular Work. Acta Physiol. Scand. 1953, 28, 364–382. [Google Scholar] [CrossRef]
- Smith, L.L. Acute Inflammation: The Underlying Mechanism in Delayed Onset Muscle Soreness? Med. Sci. Sports Exerc. 1991, 23, 542–551. [Google Scholar] [CrossRef] [PubMed]
- De Vries, H.A. Quantitative Electromyographic Investigation of the Spasm Theory of Muscle Pain. Am. J. Phys. Med. 1966, 45, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Hough, T. Ergographic Studies in Muscular Fatigue and Soreness. J. Boston Soc. Med. Sci. 1900, 5, 81–92. [Google Scholar] [PubMed]
- Weinstock, C.; König, D.; Harnischmacher, R.; Keul, J.; Berg, A.; Northoff, H. Effect of Exhaustive Exercise Stress on the Cytokine Response. Med. Sci. Sports Exerc. 1997, 29, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.T.; Barnes, C. Negative (Eccentric) Work Physiological Responses to Walking Uphill and Downhill on a Motor-Driven Treadmill. Ergonomics 1972, 15, 121–131. [Google Scholar] [CrossRef]
- Maughan, R.J.; Donnelly, A.E.; Gleeson, M.; Whiting, P.H.; Walker, K.A.; Clough, P.J. Delayed-onset Muscle Damage and Lipid Peroxidation in Man after a Downhill Run. Muscle Nerve 1989, 12, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Ashton, T.; McArdle, A.; MacLaren, D.P.M. The Emerging Role of Free Radicals in Delayed Onset Muscle Soreness and Contraction-Induced Muscle Injury. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2005, 142, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Witt, E.H.; Reznick, A.Z.; Viguie, C.A.; Starke-Reed, P.; Packer, L. Exercise, Oxidative Damage and Effects of Antioxidant Manipulation. J. Nutr. 1992, 122, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.; Hsu, T.G.; Hsu, K.M.; Cheng, H.; Liu, T.Y.; Hsu, C.F.; Kong, C.W. Oxidative DNA Damage in Human Peripheral Leukocytes Induced by Massive Aerobic Exercise. Free Radic. Biol. Med. 2001, 31, 1465–1472. [Google Scholar] [CrossRef]
- Powers, S.K.; Jackson, M.J. Exercise-Induced Oxidative Stress: Cellular Mechanisms and Impact on Muscle Force Production. Physiol. Rev. 2008, 88, 1243–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, M.R.; Izadi, A.; Kaviani, M. Antioxidants and Exercise Performance: With a Focus on Vitamin e and c Supplementation. Int. J. Environ. Res. Public Health 2020, 17, 8452. [Google Scholar] [CrossRef]
- Merry, T.L.; Ristow, M. Do Antioxidant Supplements Interfere with Skeletal Muscle Adaptation to Exercise Training? J. Physiol. 2016, 594, 5135–5147. [Google Scholar] [CrossRef]
- Gomez-Cabrera, M.C.; Viña, J.; Ji, L.L. Role of Redox Signaling and Inflammation in Skeletal Muscle Adaptations to Training. Antioxidants 2016, 5, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popovic, L.M.; Mitic, N.R.; Miric, D.; Bisevac, B.; Miric, M.; Popovic, B. Influence of Vitamin c Supplementation on Oxidative Stress and Neutrophil Inflammatory Response in Acute and Regular Exercise. Oxid. Med. Cell. Longev. 2015, 2015, 295497. [Google Scholar] [CrossRef]
- Ryan, M.J.; Dudash, H.J.; Docherty, M.; Geronilla, K.B.; Baker, B.A.; Haff, G.G.; Cutlip, R.G.; Alway, S.E. Vitamin E and C Supplementation Reduces Oxidative Stress, Improves Antioxidant Enzymes and Positive Muscle Work in Chronically Loaded Muscles of Aged Rats. Exp. Gerontol. 2010, 45, 882–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, L.P. The Role of Direct and Indirect Polyphenolic Antioxidants in Protection against Oxidative Stress. In Polyphenols: Mechanisms of Action in Human Health and Disease; Watson, R.R., Preedy, V.R., Zibadi, S., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 147–179. [Google Scholar] [CrossRef]
- Righi, N.C.; Schuch, F.B.; De Nardi, A.T.; Pippi, C.M.; de Almeida Righi, G.; Puntel, G.O.; da Silva, A.M.V.; Signori, L.U. Effects of Vitamin C on Oxidative Stress, Inflammation, Muscle Soreness, and Strength Following Acute Exercise: Meta-Analyses of Randomized Clinical Trials. Eur. J. Nutr. 2020, 59, 1–13. [Google Scholar] [CrossRef]
- Ranchordas, M.K.; Rogerson, D.; Soltani, H.; Costello, J.T. Antioxidants for Preventing and Reducing Muscle Soreness after Exercise: A Cochrane Systematic Review. Br. J. Sports Med. 2020, 54, 74–78. [Google Scholar] [CrossRef]
- Pollock, A.; Berge, E. How to Do a Systematic Review. Int. J. Stroke 2018, 13, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una Propuesta Para Mejorar La Publicación de Revisiones Sistemáticas y Metaanálisis. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmani-Nia, F.; Talebi, E.; Nakhostin, B.; Ebrahim, K. Effect of Two Regimes of Vitamin C on Delayed Onset of Muscle Soreness. J. Mov. Sci. Sports 2008, 5, 1–5. [Google Scholar]
- Bloomer, R.J.; Falvo, M.J.; Schilling, B.K.; Smith, W.A. Prior Exercise and Antioxidant Supplementation: Effect on Oxidative Stress and Muscle Injury. J. Int. Soc. Sports Nutr. 2007, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- Bryer, S.C.; Goldfarb, A.H. Effect of High Dose Vitamin C Supplementation on Muscle Soreness, Damage, Function, and Oxidative Stress to Eccentric Exercise. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 270–280. [Google Scholar] [CrossRef]
- Connolly, D.A.J.; Lauzon, C.; Agnew, J.; Dunn, M.; Reed, B. The Effects of Vitamin C Supplementation on Symptoms of Delayed Onset Muscle Soreness. J. Sports Med. Phys. Fitness 2006, 46, 462–467. [Google Scholar] [PubMed]
- Kashef, M. Effect of Vitamin E Supplementation on Delayed Onset Muscle Soreness in Young Men. J. Phys. Act. Horm. 2018, 2, 15–28. [Google Scholar]
- Silva, L.A.; Pinho, C.A.; Silveira, P.C.L.; Tuon, T.; De Souza, C.T.; Dal-Pizzol, F.; Pinho, R.A. Vitamin e Supplementation Decreases Muscular and Oxidative Damage but Not Inflammatory Response Induced by Eccentric Contraction. J. Physiol. Sci. 2010, 60, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Ashton, T.; Cable, T.; Doran, D.; Holloway, C.; McArdle, F.; MacLaren, D.P.M. Ascorbic Acid Supplementation Does Not Attenuate Post-Exercise Muscle Soreness Following Muscle-Damaging Exercise but May Delay the Recovery Process. Br. J. Nutr. 2006, 95, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Shafat, A.; Butler, P.; Jensen, R.L.; Donnelly, A.E. Effects of Dietary Supplementation with Vitamins C and E on Muscle Function during and after Eccentric Contractions in Humans. Eur. J. Appl. Physiol. 2004, 93, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Williams, C.; Kingsley, M.; Nicholas, C.W.; Lakomy, H.K.A.; McArdle, F.; Jackson, M.J. Muscle Soreness and Damage Parameters after Prolonged Intermittent Shuttle-Running Following Acute Vitamin C Supplementation. Int. J. Sports Med. 2001, 22, 68–75. [Google Scholar] [CrossRef]
- Thompson, D.; Williams, C.; Garcia-Roves, P.; McGregor, S.J.; McArdle, F.; Jackson, M.J. Post-Exercise Vitamin C Supplementation and Recovery from Demanding Exercise. Eur. J. Appl. Physiol. 2003, 89, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Bailey, D.M.; Hill, J.; Hurst, T.; Powell, J.R.; Williams, C. Prolonged Vitamin C Supplementation and Recovery from Eccentric Exercise. Eur. J. Appl. Physiol. 2004, 92, 133–138. [Google Scholar] [CrossRef]
- He, F.; Hockemeyer, J.A.K.; Sedlock, D. Does Combined Antioxidant Vitamin Supplementation Blunt Repeated Bout Effect? Int. J. Sports Med. 2015, 36, 407–413. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, D.C.X.; Rosa, F.T.; Simões-Ambrósio, L.; Jordao, A.A.; Deminice, R. Antioxidant Vitamin Supplementation Prevents Oxidative Stress but Does Not Enhance Performance in Young Football Athletes. Nutrition 2019, 63–64, 29–35. [Google Scholar] [CrossRef]
- Nie, J.; Lin, H. Effects of Vitamin C Supplementation on Recovery from Eccentric Exercise-Induced Muscle Soreness and Damage in Junior Athletes. J. Exerc. Sci. Fit. 2004, 2, 94–98. [Google Scholar]
- Gault, M.L.; Willems, M.E.T. Aging, Functional Capacity and Eccentric Exercise Training. Aging Dis. 2013, 4, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Dannecker, E.A.; Liu, Y.; Rector, R.S.; Thomas, T.R.; Fillingim, R.B.; Robinson, M.E. Sex Differences in Exercise-Induced Muscle Pain and Muscle Damage. J. Pain 2012, 13, 1242–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanidis, Y.; Stagos, D.; Papanikolaou, C.; Karatza, K.; Theodosi, A.; Veskoukis, A.S.; Deli, C.K.; Poulios, A.; Koulocheri, S.D.; Jamurtas, A.Z.; et al. Resistance-Trained Individuals Are Less Susceptible to Oxidative Damage after Eccentric Exercise. Oxid. Med. Cell. Longev. 2018, 2018, 6857190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Ferran, M.; Sanchis-Gomar, F.; Lavie, C.J.; Lippi, G.; Pareja-Galeano, H. Do Antioxidant Vitamins Prevent Exercise-Induced Muscle Damage? A Systematic Review. Antioxidants 2020, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- Byrnes, W.C.; Clarkson, P.M.; White, J.S.; Hsieh, S.S.; Frykman, P.N.; Maughan, R.J. Delayed Onset Muscle Soreness Following Repeated Bouts of Downhill Running. J. Appl. Physiol. 1985, 59, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The Association of Sleep and Pain: An Update and a Path Forward. J. Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, A.; Dobridge, J.; Hackney, A.C. Influence of Estrogen on Markers of Muscle Tissue Damage Following Eccentric Exercise. Fiziol. Cheloveka 2001, 27, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Del Coso, J.; Valero, M.; Lara, B.; Salinero, J.J.; Gallo-Salazar, C.; Areces, F. Myosin Light Chain Kinase (MLCK) Gene Influences Exercise Induced Muscle Damage during a Competitive Marathon. PLoS ONE 2016, 11, e0160053. [Google Scholar] [CrossRef]
- Del Coso, J.; Valero, M.; Salinero, J.J.; Lara, B.; Díaz, G.; Gallo-Salazar, C.; Ruiz-Vicente, D.; Areces, F.; Puente, C.; Carril, J.C.; et al. ACTN3 Genotype Influences Exercise-Induced Muscle Damage during a Marathon Competition. Eur. J. Appl. Physiol. 2017, 117, 409–416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Sequence Generati0n (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blindness of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Outcome Reporting (Reporting Bias) | Other Sources of Bias |
|---|---|---|---|---|---|---|---|
| Bryer et al., 2006 [30] |  |  | | | |  | |
| Conolly et al., 2006 [31] | | | | | | | |
| Close et al., 2006 [34] | | | | | | | |
| De Oliveira et al., 2019 [40] | | | | | | | |
| He et al., 2015 [39] | | | | | | | |
| Rahmani et al., 2008 [28] | | | | | | | |
| Thompson et al., 2004 [38] | | | | | | | |
| Shafat et al., 2004 [35] | | | | | | | |
| Bloomer et al., 2007 [29] | | | | | | | |
| Thompson et al., 2001 [36] | | | | | | | |
| Kashef 2018 [32] | | | | | | | |
| Thompson et al., 2003 [37] | | | | | | | |
| Silva et al., 2010 [33] | | | | | | | |
| Nie and Lin 2004 [41] | | | | | | | |
Low risk of bias; Unclear risk of bias; High risk of bias.| Study | Subjects | Supplementation and Timing | Exercise | DOMS, MS, and PMS Variables | Variables other than DOMS, MS, PMS | Results |
|---|---|---|---|---|---|---|
| Bryer et al., 2006 [30] | 18 healthy untrained males: SUP (n = 8) 21.4 ± 0.8 years PLA (n = 10) 24.4 ± 1.7 years | VitC (3000 mg) per day for 18 days 2 weeks pre-exercise and 4 days post-exercise | 70 eccentric elbow extensions with non-dominant arm | MS: linear scale from 1 to 10 Before exercise, immediately after, and 4, 24, 48, 72, and 96 h after exercise. | MIF ROM CK GSSG TGSH | MS → PLA > SUP across all time points. MS → increased in both groups yet was significantly reduced for the first 24 h in the VitC SUP group. |
| Conolly et al., 2006 [31] | 24 healthy untrained males and females: SUP (n = 12) 22.3 ± 3.9 years PLA (n = 12) 22.6 ± 4.6 years | VitC (1000 mg) 3 times per day for 8 days 3 days pre-exercise and 5 days post-exercise | 40 (2 sets x 20 reps) maximal eccentric elbow flexor contractions | DOMS: strength, flexibly, pain, and point tenderness assessments Before exercise and 24, 48, 72, and 96 h after exercise and DOMS induction. | - | DOMS → VitC is ineffective in protecting against selected markers of DOMS. |
| Close et al., 2006 [34] | 20 healthy physically active males: SUP (n = 10) 24.2 ± 1.5 years PLA (n = 10) 22.1 ± 0.4 years | VitC (1000 mg) per day for 15 days 2 h pre-exercise and 14 days post-exercise | Downhill running on motorized treadmill for 30 min | DOMS: VAS and pressure algometry Ratings of DOMS were presented as mean soreness of eleven assessed sites 2 h before exercise as well as 1, 2, 3, 4, 7, and 14 days post-exercise. | Plasma VitC ROS MDA TGSH MF | DOMS→ SUP = PLA at all time points. |
| De Oliveira et al., 2019 [40] | 21 male football players: SUP (n = 11) 16.7 ± 0.3 years PLA (n = 10) 17.0 ± 0.3 years | VitC (500 mg) and VitE (400 IU of α-tocopherol) per day for 15 days 7 days before and 7 days after exercise | Plyometric jump and strength resistance set to exhaustion | DOMS: VAS before and 24, 48, and 72 h post-exercise. | Plasma VitC Plasma VitE MDA CK GSSG TGSH | DOMS → SUP = PLA during recovery week. |
| He et al., 2015 [39] | 22 moderately trained males: SUP (n = 11) 20.5 ± 2.3 years PLA (n = 11) 21.3 ± 4.0 years | VitC (1000 mg) and VitE (400 IU) per day for 14 days Before each session and 2 days post session | 40-min downhill running on treadmill performed at the same time of day 2 different sessions separated by 3 weeks | DOMS: Rodenburg (1993) rating of soreness scale. Rated immediately after, and 24, 48, and 72 h after each trial. | CK ORAC | DOMS → PLA > SUP at 24 h after exercise in both the quadriceps and tibialis anterior. |
| Rahmani et al., 2008 [28] | 37 healthy non-athletic females (22.02 ± 1.54 years) 4 groups: SUP 100 mg (n = 9) SUP 200 mg (n = 10) PLA (n = 9) Control (no SUP or PLA) (n = 9) | VitC (100 mg) and VitC (200 mg) per day for 3 days Immediately before exercise and 24 and 48 h post-exercise | 70 eccentric contractions of the triceps muscle of the non-dominant side on a modified arm curl machine | PMS: soreness graded using a 30-point scale Evaluated 4 times on Day 1: 1 h pre exercise and 1h post-exercise Day 2: 2 h after SUP Day 3: 2 h after SUP. | CK ROM MEC EROM | DOMS → SUP (100 and 200 mg) = PLA. |
| Thompson et al., 2004 [38] | 14 physically active males: SUP (n = 7) 25.3 ± 1.4 years PLA (n = 7) 22.6 ± 1.7 years | VitC (200 mg) twice a day for 14 days Before exercise and 3 days post-exercise | Downhill running on motorized treadmill for 30 min | MS: soreness scale 0–100 mm Before exercise and 24, 48, and 72 h post-exercise. | Plasma VitC CK Myoglobin Interleukin-6 MF | MS → SUP = PLA at all time points after exercise. |
| Shafat et al., 2004 [35] | 12 healthy moderately active males: SUP (n = 6) 25.0 ± 7.5 years PLA(n = 6) 20.6 ± 1.1 years | VitC (500 mg) and VitE (1200 IU of α-tocopherol) per day for 37 days 30 days pre-exercise and 7 days post-exercise | 30 eccentric contractions of knee extensions with dominant leg | DOMS: VAS for a total of 8 body sites Before exercise, immediately after and every day for 7 days post-exercise. | MVC MF | MS→ SUP = PLA at all time points after exercise and recovery. |
| Bloomer et al., 2007 [29] | 30 healthy trained males 4 groups: No prior exercise SUP (n = 7) 23 ± 2 years No prior exercise PLA (n = 8) 25 ± 5 years Prior exercise SUP (n = 8) 22 ± 2 years Prior exercise PLA (n = 7) 25 ± 4 years | VitC (1000 mg) and VitE (378 mg mixed tocopherols/tocotrienols) two capsules per day for 16 days 14 days pre-exercise and 2 days post-exercise | 10 sets of 10 repetitions of the barbell Smith machine bench press exercise | MS: VAS Before exercise, immediately after and 24 and 48 h post-exercise. | MIF MF CK CRP Protein carbonyls Peroxides | MS→ SUP = PLA at all time points after exercise. |
| Thompson et al., 2001 [36] | 9 healthy physically active males 28.4 ± 1.3 years | VitC (1000 mg) per day for 1 day 2 h pre-exercise | LIST two sessions separated by 14 days | MS: VAS for whole-body Before exercise and 24, 48, and 72 h post-exercise. | Plasma VitC MDA CK Uric Acid Cortisol Total Iron | MS→ SUP = PLA at all time points after exercise. |
| Kashef 2018 [32] | 20 healthy sedentary males: SUP (n = 10) 22.4 ± 2.5 years PLA (n = 10) 22.7 ± 2.2 years | VitE (400 IU) per day for 30 days Post-dinner time 28 days pre-exercise and 2 days post-exercise | 10 min of bench leg step ups with both legs at a rate of 1 step per second | DOMS: Likert scale of muscle soreness MS measured as mean score Immediately after and 48 h post-exercise. | PP CRP CK | DOMS→ SUP = PLA at all time points after exercise. |
| Thompson et al., 2003 [37] | 16 healthy physically active males: SUP (n = 8) 23.6 ± 1.4 years PLA (n = 8) 24.3 ± 1.7 years | VitC (200 mg) dissolved in a 500 mL drink twice a day for 3 days Immediately after and 2 days post-exercise | LIST 2 sessions separated by 3 days | MS: VAS Mean score for five sites Before exercise and 24, 48, and 72 h post-exercise. | Plasma VitC MDA CK Serum cortisol Interleukin-6 Uric acid | MS→ SUP = PLA at time points in leg flexors and extensors. |
| Silva et al., 2010 [33] | 21 healthy untrained males: SUP (n = 11) 22.5 ± 4 years PLA (n = 10) 22.5 ± 4 years | VitE (800 IU of D-α-tocopherol acetate) per day for 21 days 14 days pre-exercise and 7 days post-exercise | 3 sets of flexion and extension of the elbow on the Scott bench at 2 min intervals until exhaustion | MS: VAS Before exercise and 2, 4, and 7 d post-exercise. | LDH Lipid peroxidation Protein carbonylation Interleukins | MS→ PLA > SUP at 4 and 7 days after eccentric exercise. |
| Nie and Lin 2004 [41] | 16 healthy male junior basketball players: SUP (n = 8) 16.7 ± 0.3 years PLA (n = 8) 16.5 ± 0.2 years | VitC (800 mg) per day for 1 days 3 h pre-exercise and 21 h post-exercise | Eccentric exercise trial (10 sets of full-squat jumps at maximum exertion and 30 sets of half-squat jumps) | PMS: VAS Before exercise, immediately after and 24 and 48 h post-exercise. | Plasma VitC MDA CK | MS → SUP = PLA at all time points after exercise. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torre, M.F.; Martinez-Ferran, M.; Vallecillo, N.; Jiménez, S.L.; Romero-Morales, C.; Pareja-Galeano, H. Supplementation with Vitamins C and E and Exercise-Induced Delayed-Onset Muscle Soreness: A Systematic Review. Antioxidants 2021, 10, 279. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020279
Torre MF, Martinez-Ferran M, Vallecillo N, Jiménez SL, Romero-Morales C, Pareja-Galeano H. Supplementation with Vitamins C and E and Exercise-Induced Delayed-Onset Muscle Soreness: A Systematic Review. Antioxidants. 2021; 10(2):279. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020279
Chicago/Turabian StyleTorre, María F., María Martinez-Ferran, Néstor Vallecillo, Sergio L. Jiménez, Carlos Romero-Morales, and Helios Pareja-Galeano. 2021. "Supplementation with Vitamins C and E and Exercise-Induced Delayed-Onset Muscle Soreness: A Systematic Review" Antioxidants 10, no. 2: 279. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020279