1. Introduction
Cancer is currently the most common cause of premature mortality in most developed countries and ranks second in terms of global mortality, accounting for 9.6 million deaths in 2018 [
1,
2]. Moreover, the incidence of cancer is expected to increase as the population ages [
3]. In 2018, cancer was the leading cause of death in Spain for both men and women, with 297.8 and 186.7 deaths per 100,000 inhabitants, respectively [
4]. Genetic predisposition is a well-known risk factor but it is estimated that the contribution of genetic factors on cancer risk is approximately between 5% and 10%, whereas environmental and lifestyle factors may account for the remaining 90–95% of cases [
5]. Among environmental factors, cumulative lifetime exposure to oxidative damage has been suggested to be involved in both cancer initiation and progression [
6]. Diet, a potentially modifiable lifestyle risk factor, may contribute up to 35% of cancer cases, which highlights opportunities for cancer incidence prevention [
5].
Extensive and robust evidence has demonstrated in the last few decades that diet plays a direct role in the development of certain types of cancer, such as breast cancer (BC) [
7,
8,
9]. In this context, natural compounds in the diet, including vitamins and minerals, have been postulated as anticarcinogenic agents due to their antioxidant properties [
10,
11]. These micronutrients prevent an excess of reactive oxygen species (ROS) and maintain an adequate reduction–oxidation balance. ROS production promotes DNA damage in cancer and genetic instability. Antioxidants can scavenge free radicals and quench the process of lipid peroxidation, which may reduce the oxidative DNA damage caused by free radicals, and ultimately protect against BC [
12,
13]. Antioxidant vitamins and minerals interrupt free radical chain reactions and operate in the early and late stages of carcinogenesis. Furthermore, antioxidants promote cancer cell death by producing modifications in cell signaling, changes in the cell cycle progression, and modulation of enzymatic activities [
14].
Despite the existing evidence on the anticarcinogenic activity of antioxidants in vitro and animal studies, results from epidemiological studies have engaged extensive controversy owing to inconsistent findings [
15,
16,
17,
18]. Some studies have reported no clear evidence for the association between dietary antioxidants and BC [
15,
16,
18], whereas few others have suggested possible inverse associations [
17,
19]. Hence, we aimed to prospectively investigate whether dietary intake of vitamins A, C, and E, selenium, and zinc was associated with risk of overall, pre-, and postmenopausal BC in the SUN (Seguimiento Universidad de Navarra) Study, a Mediterranean cohort of graduates.
3. Results
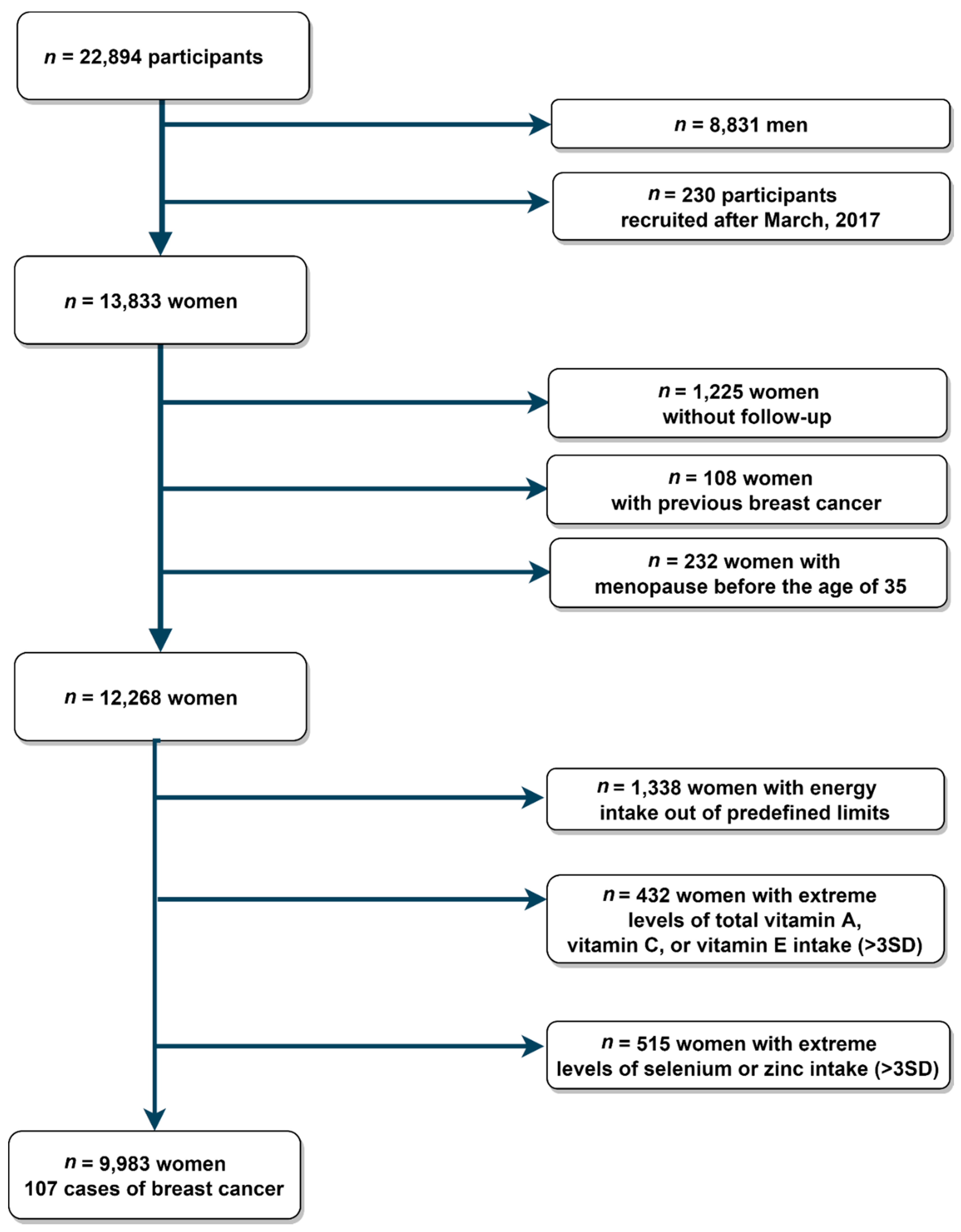
During a mean average of 11.3 years of follow-up, 107 incident BC cases were diagnosed in 9983 women. The crude BC incidence was 94.7 per 100,000 person-year. Among the 72 cases with known subtype, 57 cases were luminal (79.2%), 8 cases were HER2 (11.1%), and 7 cases were triple negative (9.7%) tumors. The distribution of the study subjects by baseline characteristics is summarized in
Table 1. The mean age of participants was 35.1 years (SD = 10.5 years), most of them were non-smokers, non-users of multivitamin or mineral supplements, had a low consumption of sugar-sweetened beverages, and they were largely nulliparous and mostly premenopausal.
Pearson correlations between dietary intake of antioxidants (non-energy-adjusted) and energy intake were moderate for selenium (
r = 0.58), vitamin E (
r = 0.57), and weaker for zinc (
r = 0.36), vitamin C (
r = 0.36), and vitamin A (
r = 0.29). The individual and cumulative contributions of different foods to the variability in antioxidant vitamins and minerals as well as the between-person variability are shown in
Supplemental Table S1. In brief, the primary food group contributors of dietary daily intake were vegetables and fruits for vitamins A and C, fats and oils for vitamin E, fish and seafood for selenium, and dairy products for zinc. Regarding sources of variability, fruits and vegetables explained more than 98% of the between-person variability for vitamin A and C intake, while fats and oils explained 43% for vitamin E intake, cereals and legumes 40% of selenium intake, and dairy products represented 82% of the between-person variability for zinc intake.
Hazard ratios and 95% CI for the risk of BC according to dietary intake of vitamin A, vitamin C, and vitamin E among overall, premenopausal, and postmenopausal women are shown in
Table 2,
Table 3 and
Table 4, respectively. Dietary vitamin A, vitamin C, and vitamin E intakes were not significantly associated with overall BC risk (highest vs. lowest tertile): HR, 1.07; 95%CI (0.64–1.77;
Ptrend = 0.673) for vitamin A; 1.00 (0.58–1.71;
Ptrend = 0.846) for vitamin C; and 0.92 (0.55–1.54;
Ptrend = 0.728) for vitamin E. When we stratified by menopausal status, no significant association was observed between tertiles of these antioxidant dietary intakes and BC incidence, except for vitamin E intake. Among postmenopausal women, we found an inverse association between vitamin E intake and BC risk for tertile 3 vs. tertile 1: HR, 0.35; 95% CI (0.14–0.86;
Ptrend = 0.027).
Table 5 and
Table 6 show the results for multivariable-adjusted models assessing dietary intakes of selenium and zinc with overall BC and among pre- and postmenopausal women. No significant association was observed between antioxidant minerals intake and overall BC, either for premenopausal or postmenopausal BC, across different levels of dietary antioxidant intake.
When we considered luminal BC as outcome, we did not find associations between levels of antioxidant vitamin or mineral intake and BC risk (
Supplemental Table S2).
After re-running the models under different assumptions, no evidence of a clear association was found between antioxidants and BC risk. (
Supplemental Tables S3–S5).
4. Discussion
In this prospective cohort study of Spanish university graduates, we aimed to prospectively investigate the relationship between the intake of vitamins A, C, and E, selenium, and zinc and BC risk. After multiple adjustments for traditional risk factors, we did not find any evidence of the association between antioxidant vitamins or minerals with overall BC risk. When we stratified our analyses by menopausal status, an inverse association with BC was observed only for vitamin E intake among postmenopausal women.
A large number of epidemiologic studies have examined for a long period the association of natural antioxidants with BC risk. Findings, however, have been predominantly discordant [
15]. Discrepancies in results seem to differ by study design. On the one hand several case-control studies have suggested an inverse relationship between antioxidant vitamins and BC risk. On the other hand, most cohort studies published in the last decade have found no consistent evidence of such association. For example, a recent meta-analysis of observational studies which included the most up-to-date studies on vitamin C intake and BC risk [
19] concluded that higher dietary vitamin C intake was significantly associated with a lower BC risk in pooled analyses and case-control studies; nevertheless, no significant observation was observed in subgroup analyses of cohort studies. Similar findings were observed in a previous meta-analysis in which dietary intake of retinol, vitamins A, C, and E became non-significant when data from cohort studies were pooled [
16]. Recall and selection bias in case-control studies might explain such inconsistencies between study designs, although no clear explanations exist [
36]. Case-control studies are prone to selection bias, particularly diet and cancer studies, due to the difficulty of selecting the appropriate control group [
37]. Moreover, recall bias may often occur because cases may associate unhealthy foods and habits with their BC malignancy [
15].
The present study provides no evidence of an association between antioxidant vitamins and BC, except for vitamin E and postmenopausal women, but the association was restricted to dietary intake. Evidence of supplementation of antioxidant vitamins has not been compelling for BC [
38,
39], consistent with prior findings from large cohorts. In the European Prospective Investigation into Cancer and Nutrition (EPIC) study, neither dietary vitamin C nor vitamin E was associated with overall BC, and neither were they in analyses stratified by menopausal status [
40]. Similarly, a pooled analysis from five established cohorts in the UK Dietary Cohort Consortium study found no evidence of an association between dietary vitamin C intake and BC risk [
17]; these findings are consistent with the Swedish Mammography Screening Cohort in which no overall association between intake of vitamin C, beta-carotene, retinol, or vitamin E and BC incidence was found [
41]. Only a few observational studies have assessed the relationship between BC risk and dietary selenium and zinc intake, finding no evidence of such association [
42,
43]. Interestingly, the conclusions from the systematic review and meta-analysis of prospective studies conducted by Kuria et al. [
18] suggested a protective effect of a recommended daily allowance of selenium intake for overall cancer; nevertheless, the potential protective effect was non-significant for BC.
Regarding dietary vitamins and minerals intake, the national recommended dietary allowances intakes for adult women are 600 mcg/d for vitamin A, 60 mg/d for vitamin C, 12 mg/d for vitamin E, 55 mcg/d for selenium, and 7 mg/d for zinc [
44]. In our study, median intake in all energy-adjusted antioxidant tertiles was higher than the national recommended dietary allowances, except for vitamin E, for which not even the median intake in the highest tertile met such allowances. The dietary intake levels of vitamin and antioxidants of the present study are higher than the levels reported by the Anibes study, the latest national published research [
45].
Animal studies have demonstrated the important role of ROS and breast malignancy [
46]. Non-enzymatic antioxidants include natural compounds such as vitamins A, C, and E, or minerals such as selenium and zinc, supplied through foods and supplements that help endogenous compounds reduce a variety of ROS. A potential mechanism for inducing tumor reduction is based on the antioxidants’ capacity to control the redox balance in malignant cells [
46,
47]. Reactive species may cause severe oxidative stress and may lead to DNA damage, suppress tumor genes, and alter cellular homeostasis leading to carcinogenesis [
12,
13]. Specifically, vitamin A, selenium, and zinc have been hypothesized to diminish the risk of BC by inhibition of cell proliferation, induction of differentiation, and apoptosis [
48,
49,
50]. Vitamin C plays a key role as a prooxidant breakage of cellular DNA [
51], and vitamin E additionally suppresses lipid peroxidation and induces apoptosis of tumor cells [
52,
53]. A major interest has been drawn among postmenopausal women, of whom the consumption of antioxidants has been theorized to have greater benefits than among premenopausal women [
54]. While premenopausal women maintain an oxidative balance between ROS and the body’s antioxidant mechanisms, produced mostly by the inhibition of the 8-hydroxylation of guanine DNA bases [
55], the levels of estrogens generally decline as menopause nears, leading to increased levels of oxidative stress [
56]. Lower levels of estrogens have pro-oxidant effects that may trigger the oxidation of bases, DNA adducts, and genetic material damage [
55].
In our study, there was no clear evidence of an association between antioxidants and BC risk. A potential explanation for these results may rely on the bioavailability of antioxidant compounds. Some authors have suggested that not only intake levels but also their bioavailability may influence their health benefits [
57]. Furthermore, compounds’ antioxidant activity largely depends on the cooking method, as foods may suffer losses of antioxidant properties [
58]. Environmental and cultivation conditions may also play a significant role on the antioxidant activity of certain foods. Different agroclimatic locations as well as factors such as temperature, moisture, and harvesting period may determine the antioxidant content [
59]. Assessment of the overall dietary antioxidant capacity rather than individual antioxidant intake has emerged as an alternative approach in the last few years. Similar to the food synergy concept [
60], the food antioxidant matrix may be greater than the corresponding action of the individual antioxidants. In other words, the cumulative effects of individual antioxidants may be too small to see a clear effect, and correlations and interactions between the endogenous enzymatic and exogenous non-enzymatic compounds may not be accounted for. In this context, several alternatives have emerged in the last years to measure the oxidative balance of an individual. Yet, there are no unified methodological criteria for the definition of overall antioxidant capacity [
61]. A specific oxidative balance index for BC, which accounts for dietary and BC risk factors as well as bioavailability may be useful for further research to clarify the role of antioxidant vitamins and minerals in BC.
The strengths of this study include its prospective and dynamic design, high overall retention (91%), long follow-up, use of reliable measures to collect dietary habits and other lifestyle information, the ability to adjust for multiple potential confounders, and the complete verification of BC cases by a trained oncologist. However, we acknowledge some limitations of the present study. First, dietary information of vitamins and minerals were assessed with a semi-quantitative FFQ, which may be prone to recall bias; nevertheless, the questionnaire has been repeatedly validated [
23,
24,
25], and we excluded participants with energy intakes outside predefined limits [
22]. Second, participants’ diet was evaluated at baseline and may not reflect long-term intake as accurate as repeated measurements of diet during follow-up. Third, we did not take into consideration antioxidant capacity losses caused by cooking methods. Fourth, absence of residual confounding cannot be assumed; however, we adjusted for several potential BC risk factors based on prior literature and previous findings of the SUN cohort. Fifth, the relatively small numbers of BC cases in our cohort may have somewhat limited the statistical power to examine associations. Additionally, multiple testing might explain the presence of significant results in our study, as we examined several compounds; nevertheless, most of the results remained non-significant. Therefore, replication of our findings in larger cohorts should be warranted. Lastly, the participants’ characteristics and homogeneity (Mediterranean middle-age with graduate education) may not represent the general population. In turn, the generalization of our findings should be based on biological mechanisms rather than on statistical representativeness. Moreover, the homogeneity of our cohort increases the reliability of the self-reported data collection and reduces confusion related to education and other socioeconomic factors, increasing the internal validity of these results.


 ,
, 


{kind=link}