
Glutathione Peroxidase in Stable Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy, Eligibility Criteria, and Study Selection
2.2. Statistical Analysis
3. Results
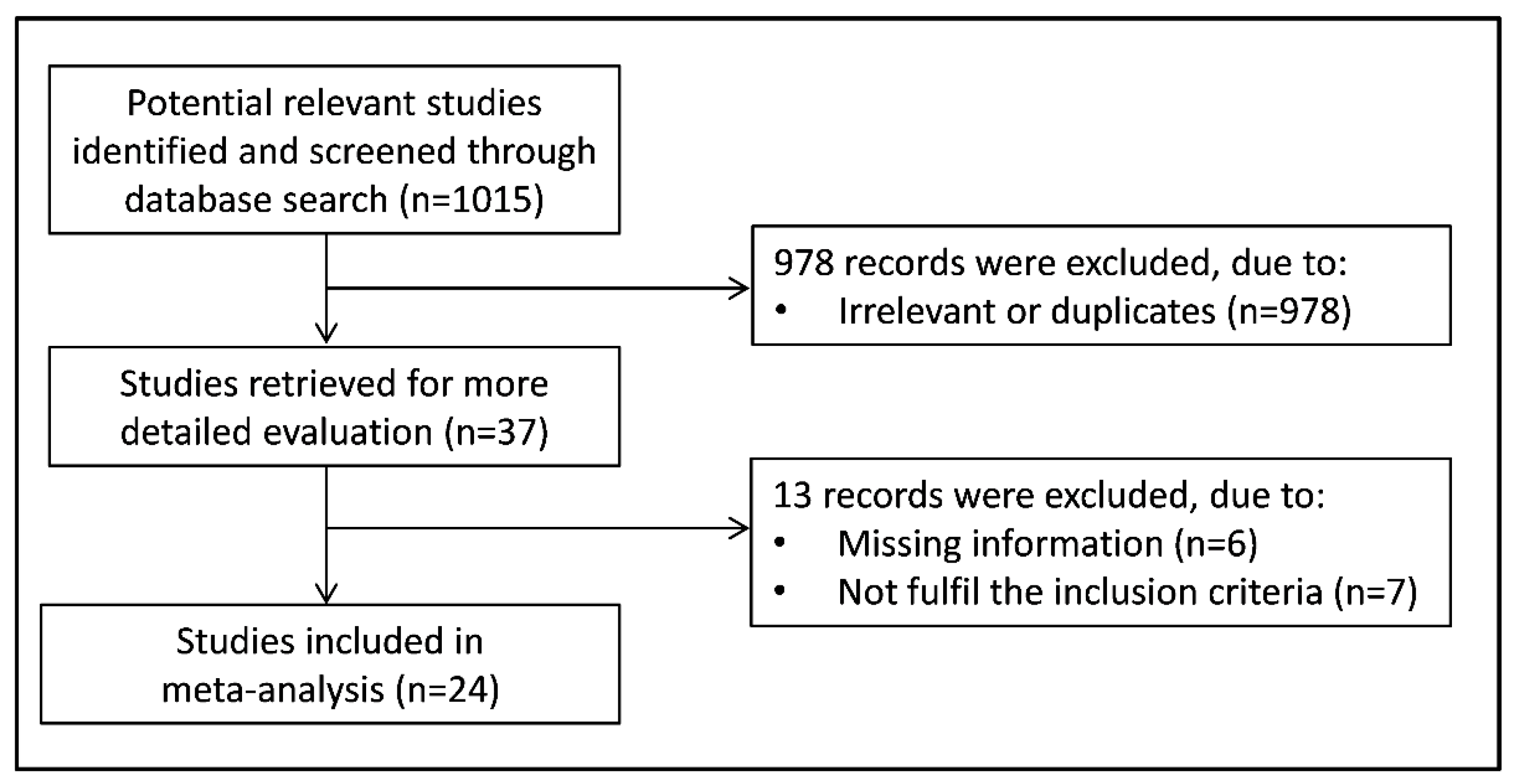
3.1. Systematic Research
3.2. Meta-Analysis of Whole Blood/Erythrocyte GPx Concentrations
3.2.1. Study Characteristics
3.2.2. Risk of Bias
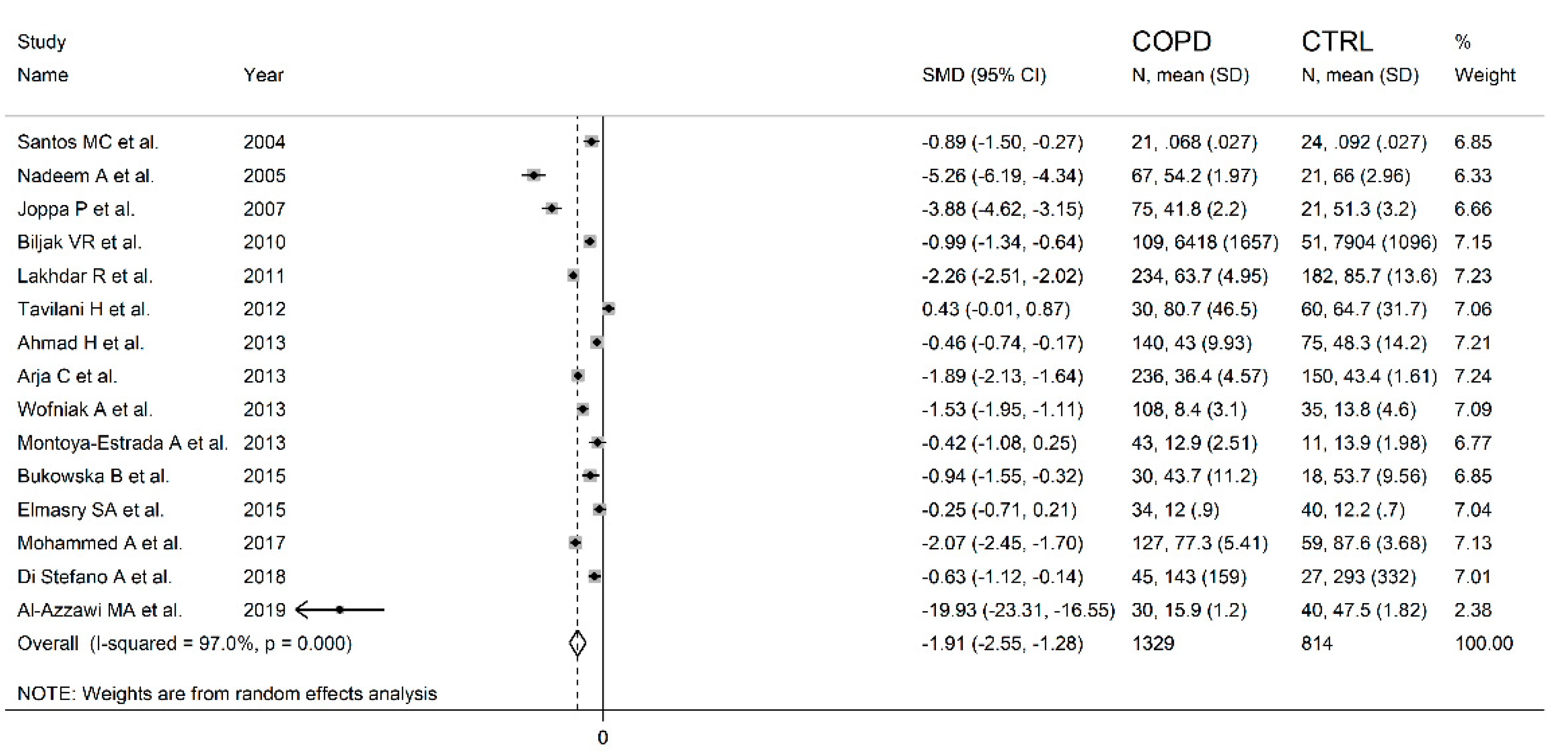
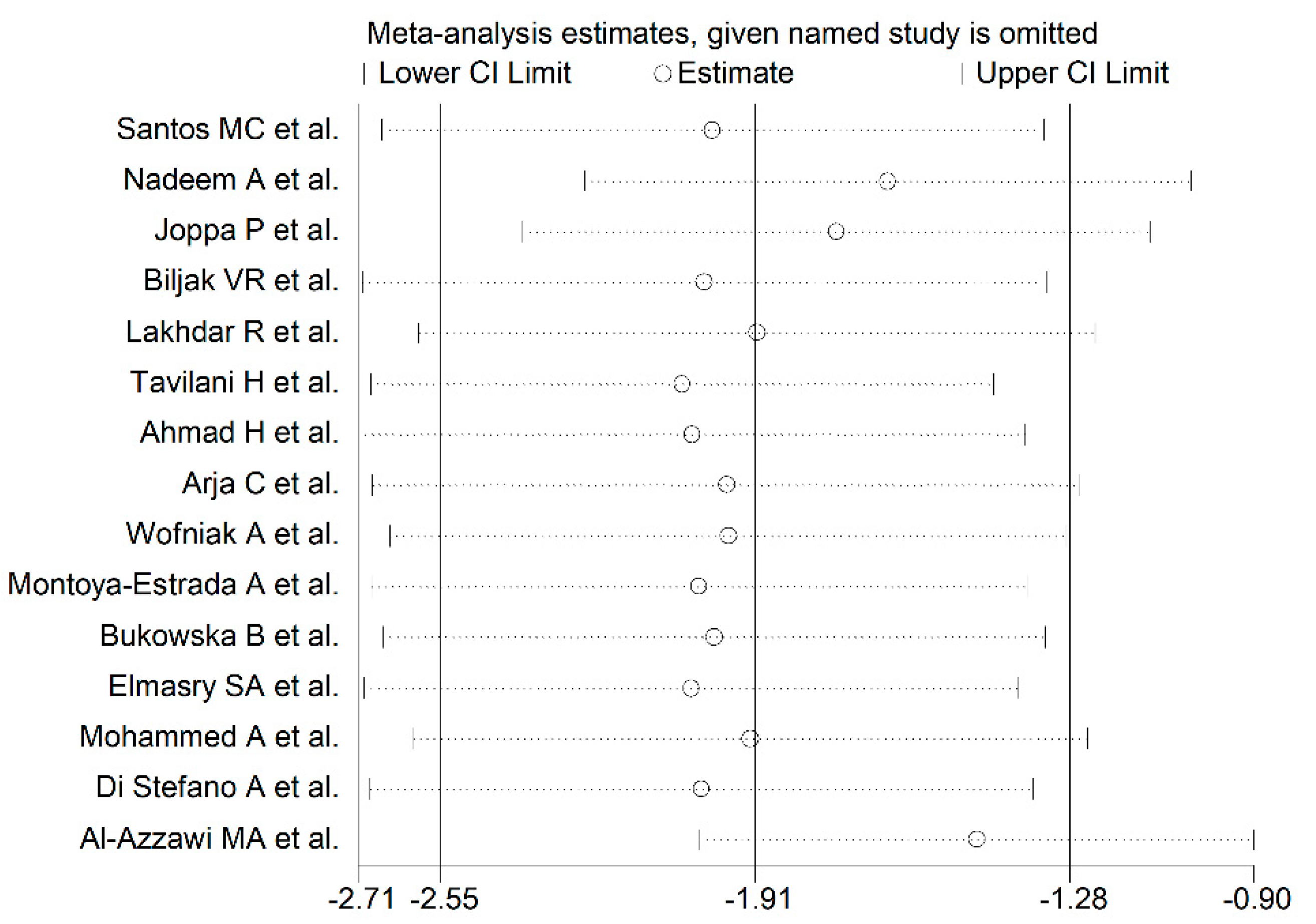
3.2.3. Results of Individual Studies and Syntheses
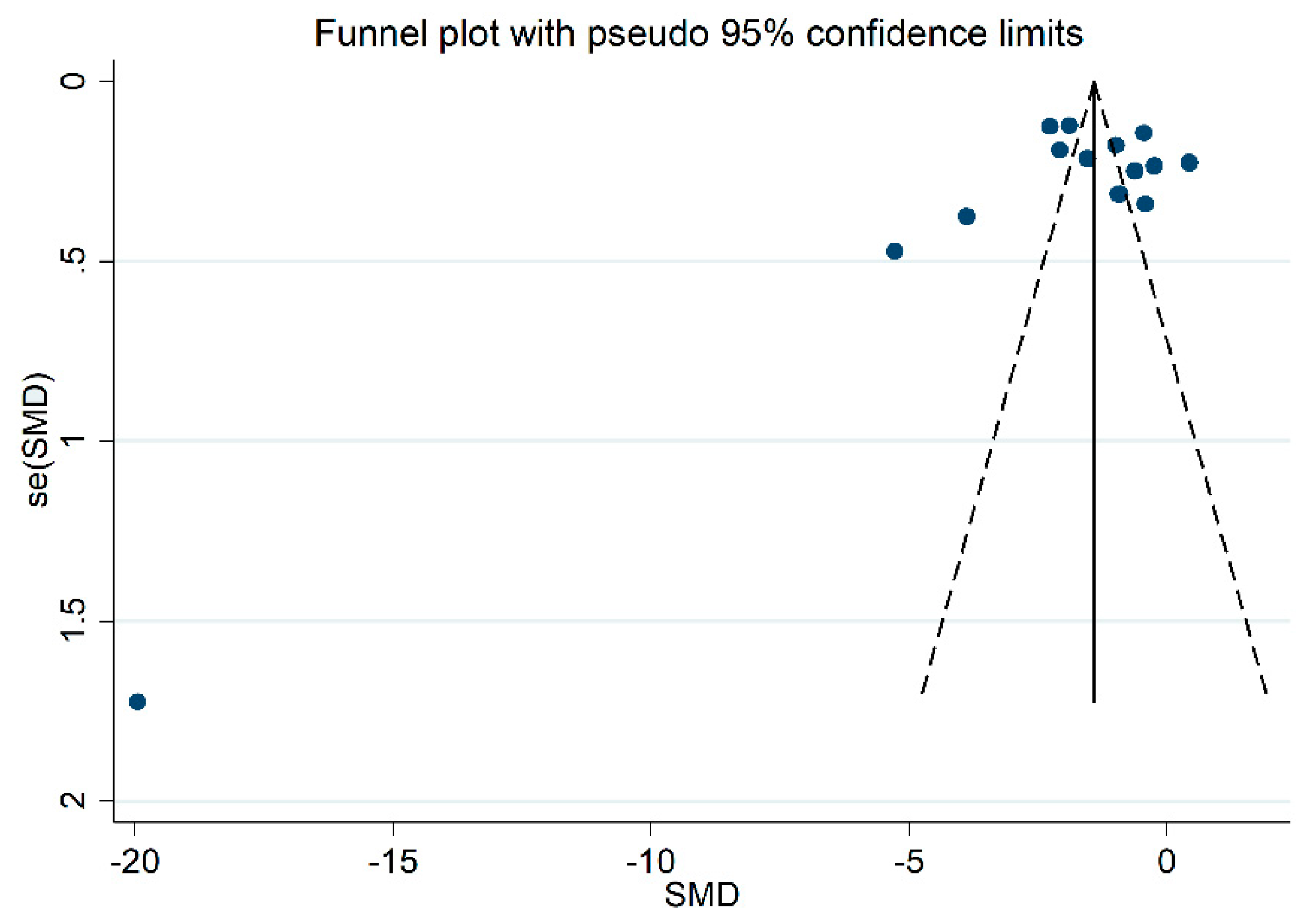
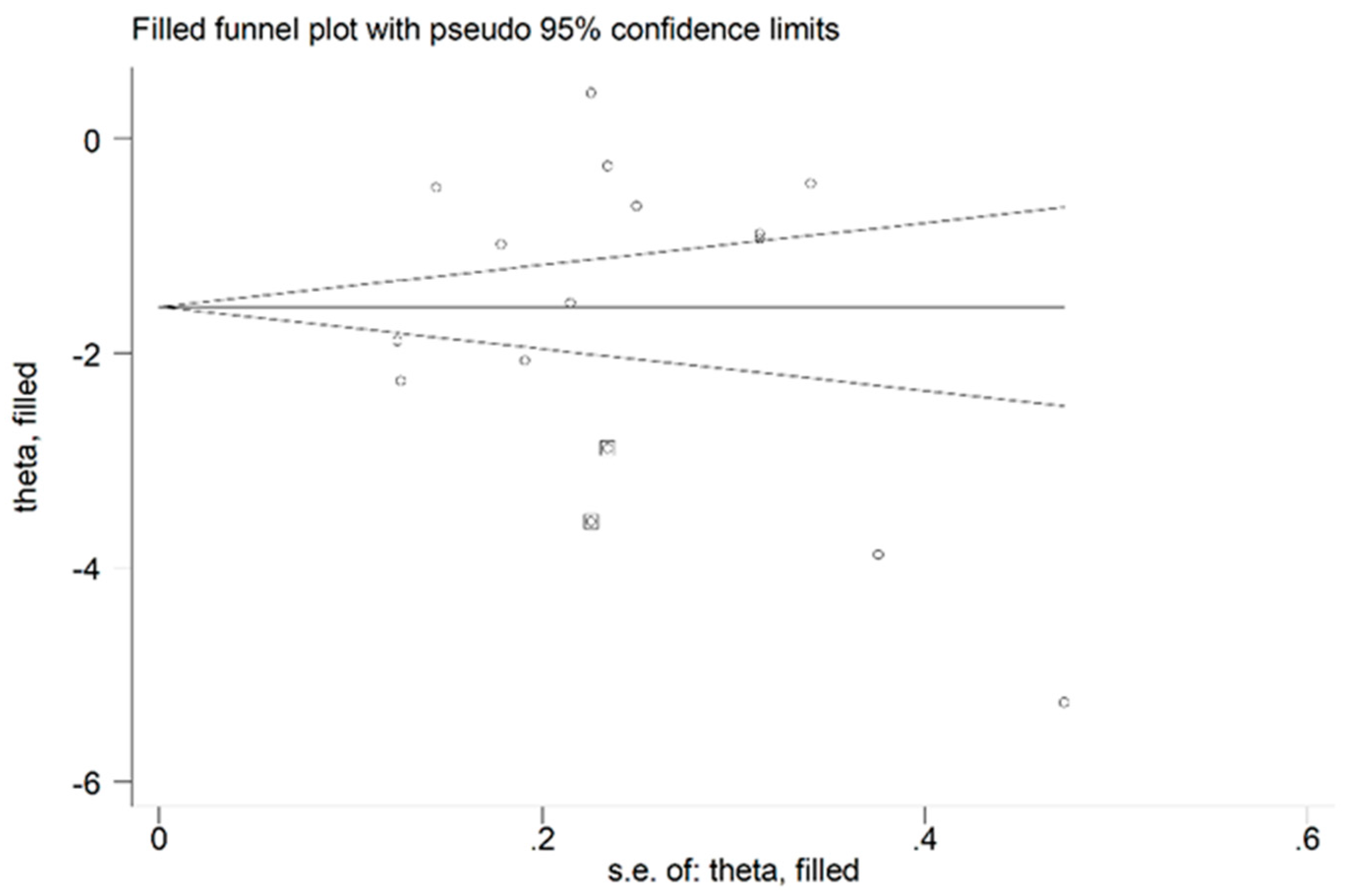
3.2.4. Publication Bias
3.2.5. Meta-Regression and Sub-group Analysis
3.2.6. Certainty of Evidence
3.3. Meta-analysis of Serum/Plasma GPx Concentrations
3.3.1. Study Characteristics
3.3.2. Risk of Bias
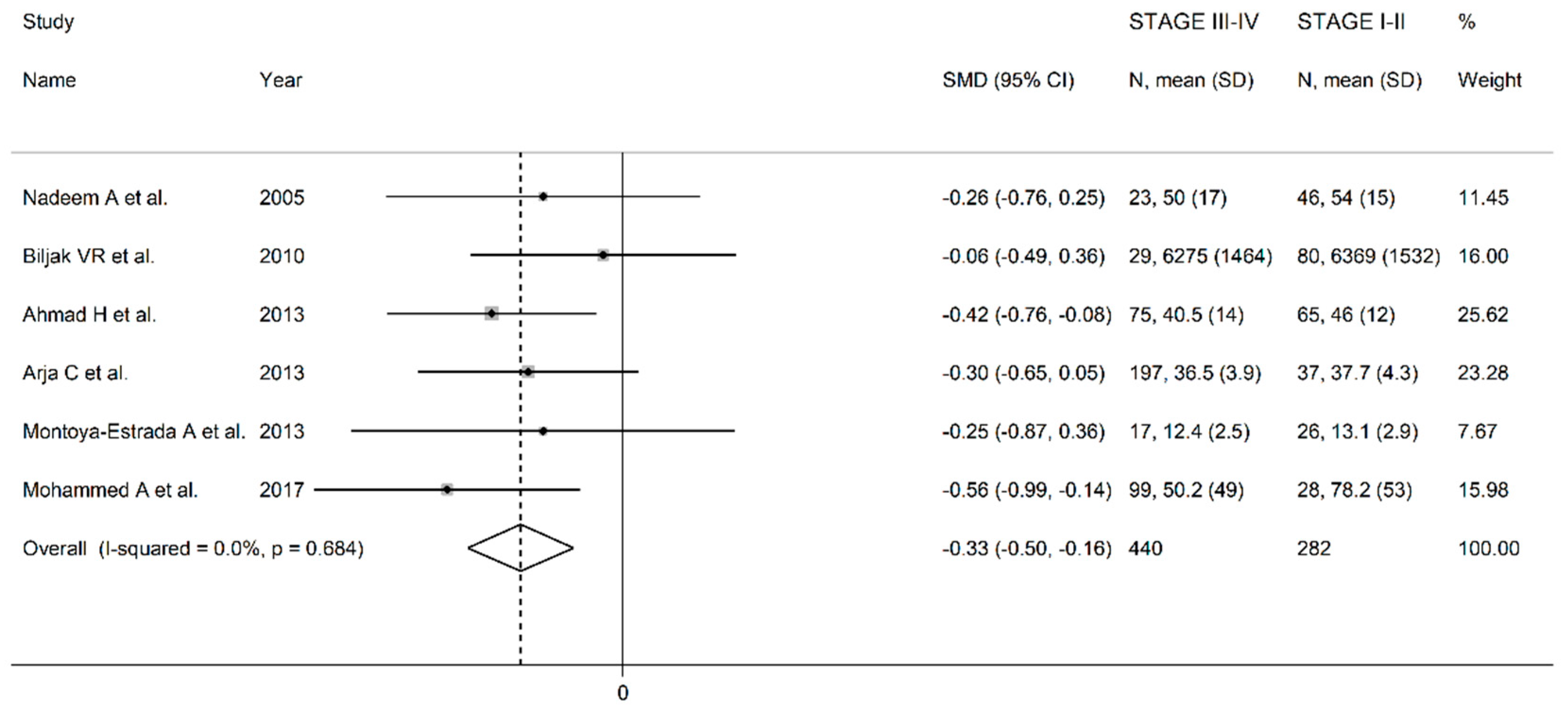
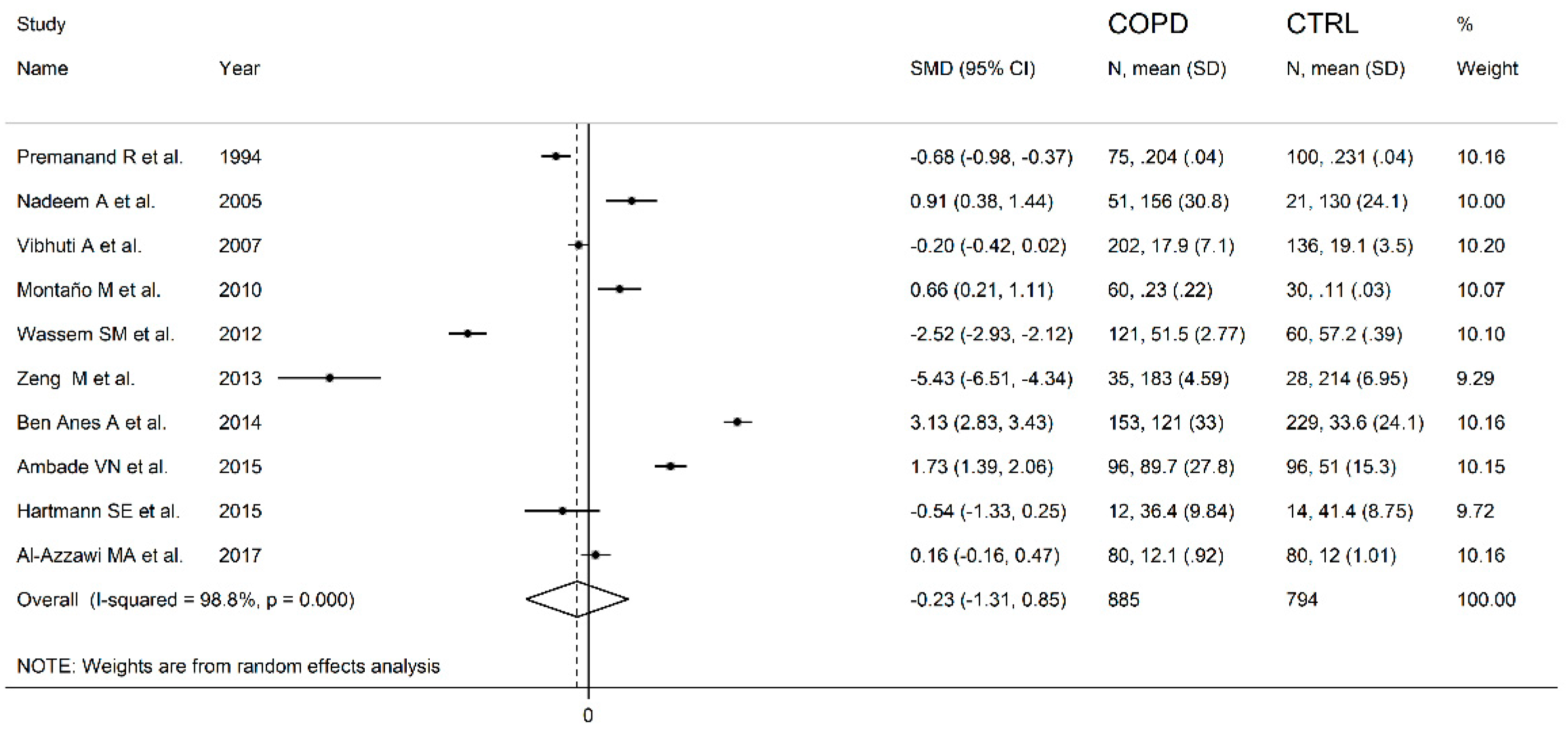
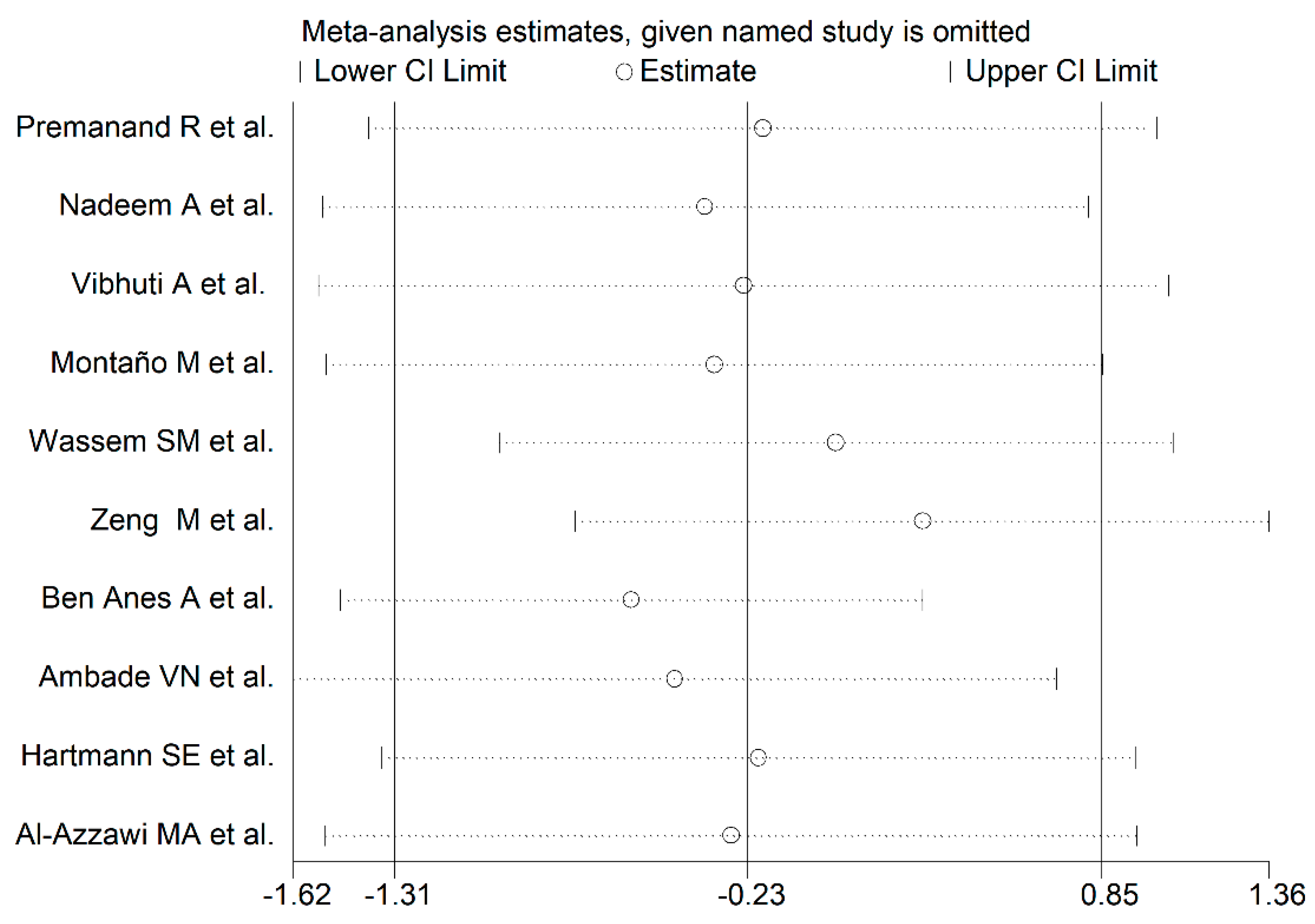
3.3.3. Results of Individual Studies and Syntheses
3.3.4. Publication Bias
3.3.5. Meta-regression and Sub-group Analysis
3.3.6. Certainty of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Blanco, I.; Diego, I.; Bueno, P.; Casas-Maldonado, F.; Miravitlles, M. Geographic distribution of COPD prevalence in the world displayed by Geographic Information System maps. Eur. Respir J. 2019, 54, 1900610. [Google Scholar] [CrossRef]
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [Green Version]
- Zuo, L.; Wijegunawardana, D. Redox Role of ROS and Inflammation in Pulmonary Diseases. Adv. Exp. Med. Biol 2021, 1304, 187–204. [Google Scholar] [PubMed]
- McGuinness, A.J.; Sapey, E. Oxidative Stress in COPD: Sources, Markers, and Potential Mechanisms. J. Clin. Med. 2017, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkham, P.A.; Barnes, P.J. Oxidative stress in COPD. Chest 2013, 144, 266–273. [Google Scholar] [CrossRef]
- Rahman, I. The role of oxidative stress in the pathogenesis of COPD: Implications for therapy. Treat. Respir Med. 2005, 4, 175–200. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Burney, P.G.; Silverman, E.K.; Celli, B.R.; Vestbo, J.; Wedzicha, J.A.; Wouters, E.F. Chronic obstructive pulmonary disease. Nat. Rev. Dis. Primers 2015, 1, 15076. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Pu, J.; Hao, B.; Huang, L.; Chen, J.; Hong, W.; Zhou, Y.; Li, B.; Ran, P. LncRNA RP11-86H7.1 promotes airway inflammation induced by TRAPM2.5 by acting as a ceRNA of miRNA-9-5p to regulate NFKB1 in HBECS. Sci. Rep. 2020, 10, 11587. [Google Scholar] [CrossRef]
- Finicelli, M.; Squillaro, T.; Galderisi, U.; Peluso, G. Micro-RNAs: Crossroads between the Exposure to Environmental Particulate Pollution and the Obstructive Pulmonary Disease. Int. J. Mol. Sci. 2020, 21, 7221. [Google Scholar] [CrossRef]
- Zinellu, E.; Zinellu, A.; Fois, A.G.; Fois, S.S.; Piras, B.; Carru, C.; Pirina, P. Reliability and Usefulness of Different Biomarkers of Oxidative Stress in Chronic Obstructive Pulmonary Disease. Oxid Med. Cell Longev. 2020, 2020, 4982324. [Google Scholar] [CrossRef]
- Barnes, P.J. Oxidative stress-based therapeutics in COPD. Redox Biol. 2020, 33, 101544. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohé, R.; Maiorino, M. Glutathione peroxidases. Biochim. Biophys. Acta 2013, 1830, 3289–3303. [Google Scholar] [CrossRef]
- Sarıkaya, E.; Doğan, S. Chapter: Glutathione Peroxidase in Health and Diseases in Glutathione System and Oxidative Stress in Health and Disease, Margarete Dulce Bagatini; IntechOpen: London, UK, 2020. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Tobias, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.C.; Oliveira, A.L.; Viegas-Crespo, A.M.; Vicente, L.; Barreiros, A.; Monteiro, P.; Pinheiro, T.; Bugalho De Almeida, A. Systemic markers of the redox balance in chronic obstructive pulmonary disease. Biomarkers 2004, 9, 461–469. [Google Scholar] [CrossRef]
- Nadeem, A.; Raj, H.G.; Chhabra, S.K. Increased oxidative stress and altered levels of antioxidants in chronic obstructive pulmonary disease. Inflammation 2005, 29, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Joppa, P.; Petrásová, D.; Stancák, B.; Dorková, Z.; Tkácová, R. Oxidative stress in patients with COPD and pulmonary hypertension. Wien. Klin Wochenschr. 2007, 119, 428–434. [Google Scholar] [CrossRef]
- Biljak, V.R.; Rumora, L.; Cepelak, I.; Pancirov, D.; Popović-Grle, S.; Sorić, J.; Grubisić, T.Z. Glutathione cycle in stable chronic obstructive pulmonary disease. Cell Biochem. Funct. 2010, 28, 448–453. [Google Scholar] [CrossRef]
- Lakhdar, R.; Denden, S.; Mouhamed, M.H.; Chalgoum, A.; Leban, N.; Knani, J.; Lefranc, G.; Miled, A.; Ben Chibani, J.; Khelil, A.H. Correlation of EPHX1, GSTP1, GSTM1, and GSTT1 genetic polymorphisms with antioxidative stress markers in chronic obstructive pulmonary disease. Exp. Lung Res. 2011, 37, 195–204. [Google Scholar] [CrossRef]
- Tavilani, H.; Nadi, E.; Karimi, J.; Goodarzi, M.T. Oxidative stress in COPD patients, smokers, and non-smokers. Respir Care 2012, 57, 2090–2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.; Shameem, M.; Husain, Q. Altered oxidant-antioxidant levels in the disease prognosis of chronic obstructive pulmonary disease. Int. J. Tuberc. Lung Dis. 2013, 17, 1104–1109. [Google Scholar] [CrossRef]
- Arja, C.; Surapaneni, K.M.; Raya, P.; Adimoolam, C.; Balisetty, B.; Kanala, K.R. Oxidative stress and antioxidant enzyme activity in South Indian male smokers with chronic obstructive pulmonary disease. Respirology 2013, 18, 1069–1075. [Google Scholar]
- Woźniak, A.; Górecki, D.; Szpinda, M.; Mila-Kierzenkowska, C.; Woźniak, B. Oxidant-antioxidant balance in the blood of patients with chronic obstructive pulmonary disease after smoking cessation. Oxid. Med. Cell Longev. 2013, 2013, 897075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montoya-Estrada, A.; Torres-Ramos, Y.D.; Flores-Pliego, A.; Ramirez-Venegas, A.; Ceballos-Reyes, G.M.; Guzman-Grenfell, A.M.; Hicks, J.J. Urban PM2.5 activates GAPDH and induces RBC damage in COPD patients. Front. Biosci. 2013, 5, 638–649. [Google Scholar] [CrossRef] [Green Version]
- Bukowska, B.; Sicińska, P.; Pająk, A.; Koceva-Chyla, A.; Pietras, T.; Pszczółkowska, A.; Górski, P.; Koter-Michalak, M. Oxidative stress and damage to erythrocytes in patients with chronic obstructive pulmonary disease--changes in ATPase and acetylcholinesterase activity. Biochem. Cell Biol. 2015, 93, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Elmasry, S.A.; Al-Azzawi, M.A.; Ghoneim, A.H.; Nasr, M.Y.; AboZaid, M.M.N. Role of oxidant–antioxidant imbalance in the pathogenesis of chronic obstructive pulmonary disease. Egypt J. Chest Dis. Tuberc. 2015, 64, 813–820. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, A.; Gutta, V.; Ansari, M.S.; Venkata, R.S.; Jamil, K. Altered antioxidant enzyme activity with severity and comorbidities of chronic obstructive pulmonary disease (COPD) in South Indian population. COPD Res. Pract. 2017, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Di Stefano, A.; Coccini, T.; Roda, E.; Signorini, C.; Balbi, B.; Brunetti, G.; Ceriana, P. Blood MCP-1 levels are increased in chronic obstructive pulmonary disease patients with prevalent emphysema. Int. J. Chron. Obs. Pulmon. Dis. 2018, 13, 1691–1700. [Google Scholar] [CrossRef] [Green Version]
- Al-Azzawi, M.A.; Al-Rubaeaee, A.A.; Ghoneim, A.H.; AboZaid, M.M. The effect of cigarette smoking on the oxidant–antioxidant imbalance in patients with chronic obstructive pulmonary disease. Egypt J. Chest Dis. Tuberc. 2019, 68, 462–470. [Google Scholar]
- Premanand, R.; Naidu, K.V.S.; Kumari, K.S.; Reddy, K.K. Lipid peroxides, vitamin E levels and glutathione peroxidase activity in serum of respiratory disease patients. Indian J. Clin. Biochem. 1994, 9, 50–53. [Google Scholar] [CrossRef]
- Vibhuti, A.; Arif, E.; Deepak, D.; Singh, B.; Pasha, M.Q. Correlation of oxidative status with BMI and lung function in COPD. Clin. Biochem. 2007, 40, 958–963. [Google Scholar] [CrossRef]
- Montaño, M.; Cisneros, J.; Ramírez-Venegas, A.; Pedraza-Chaverri, J.; Mercado, D.; Ramos, C.; Sansores, R.H. Malondialdehyde and superoxide dismutase correlate with FEV(1) in patients with COPD associated with wood smoke exposure and tobacco smoking. Inhal. Toxicol. 2010, 22, 868–874. [Google Scholar] [CrossRef]
- Waseem, S.M.; Mobarak, M.H.; Islam, N.; Ahmad, Z. Comparative study of pulmonary functions and oxidative stress in smokers and non-smokers. Indian J. Physiol. Pharmacol. 2012, 56, 345–352. [Google Scholar]
- Zeng, M.; Li, Y.; Jiang, Y.; Lu, G.; Huang, X.; Guan, K. Local and systemic oxidative stress status in chronic obstructive pulmonary disease patients. Can. Respir J. 2013, 20, 35–41. [Google Scholar] [CrossRef]
- ben Anes, A.; Fetoui, H.; Bchir, S.; ben Nasr, H.; Chahdoura, H.; Chabchoub, E.; Yacoub, S.; Garrouch, A.; Benzarti, M.; Tabka, Z.; et al. Increased oxidative stress and altered levels of nitric oxide and peroxynitrite in Tunisian patients with chronic obstructive pulmonary disease: Correlation with disease severity and airflow obstruction. Biol. Trace Elem. Res. 2014, 161, 20–31. [Google Scholar] [CrossRef]
- Ambade, V.N.; Sontakke, A.N.; Barthwal, M.S.; Tyagi, R.; Basannar, D.R. Diagnostic Utility of Biomarkers in COPD. Respir Care 2015, 60, 1729–1742. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, S.E.; Waltz, X.; Kissel, C.K.; Szabo, L.; Walker, B.L.; Leigh, R.; Anderson, T.J.; Poulin, M.J. Cerebrovascular and ventilatory responses to acute isocapnic hypoxia in healthy aging and lung disease: Effect of vitamin C. J. Appl. Physiol. 2015, 119, 363–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Azzawi, M.A.; Ghoneim, A.H.; Elmadbouh, I. Evaluation of Vitamin D, Vitamin D Binding Protein Gene Polymorphism with Oxidant—Antioxidant Profiles in Chronic Obstructive Pulmonary Disease. J. Med. Biochem. 2017, 36, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Mahwah, NJ, USA, 1988. [Google Scholar]
- Brigelius-Flohé, R.; Flohé, L. Regulatory Phenomena in the Glutathione Peroxidase Superfamily. Antioxid. Redox Signal. 2020, 33, 498–516. [Google Scholar] [CrossRef]
- Toppo, S.; Flohé, L.; Ursini, F.; Vanin, S.; Maiorino, M. Catalytic mechanisms and specificities of glutathione peroxidases: Variations of a basic scheme. Biochim. Biophys. Acta 2009, 1790, 1486–1500. [Google Scholar] [CrossRef]
- Lubos, E.; Loscalzo, J.; Handy, D.E. Glutathione peroxidase-1 in health and disease: From molecular mechanisms to therapeutic opportunities. Antioxid. Redox Signal. 2011, 15, 1957–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sotgia, S.; Paliogiannis, P.; Sotgiu, E.; Mellino, S.; Zinellu, E.; Fois, A.G.; Pirina, P.; Carru, C.; Mangoni, A.A.; Zinellu, A. Systematic Review and Meta-Analysis of the Blood Glutathione Redox State in Chronic Obstructive Pulmonary Disease. Antioxidants 2020, 9, 1146. [Google Scholar] [CrossRef] [PubMed]
- Dabo, A.J.; Ezegbunam, W.; Wyman, A.E.; Moon, J.; Railwah, C.; Lora, A.; Majka, S.M.; Geraghty, P.; Foronjy, R.F. Targeting c-Src Reverses Accelerated GPX-1 mRNA Decay in Chronic Obstructive Pulmonary Disease Airway Epithelial Cells. Am. J. Respir Cell Mol. Biol. 2020, 62, 598–607. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-COPD | COPD | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| First Author Year, Country | Matrix Type | n | Age Mean | Gender (M/F) | GPx Mean ± SD | n | Age Mean | Gender (M/F) | GPX Mean ± SD |
| WHOLE BLOOD/ERYTHROCYTES | |||||||||
| Santos MC et al. 2004, Portugal | Er | 24 | NR | NR | 0.092 ± 0.027 U/g Hb | 21 | NR | NR | 0.068 ± 0.027 U/g Hb |
| Nadeem A et al. 2005, India | Er | 21 | NR | NR | 65.96 ± 13.56 mU/g Hb | 67 | NR | NR | 54.17 ± 16.12 mU/g Hb |
| Joppa P et al. 2007, Slovakia | Er | 21 | 48 | 9/12 | 51.30 ± 14.66 U/g Hb | 75 | 65 | 58/17 | 41.80 ± 18.05 U/g Hb |
| Biljak VR et al. 2010, Croatia | Er | 51 | 52 | 21/30 | 7904 ± 1096 U/L | 109 | 71 | 82/27 | 6418 ± 1657 U/L |
| Lakhdar R et al. 2011, Tunisia | Er | 182 | 56 | 173/9 | 85.70 ± 13.61 U/g Hb | 234 | 62 | 222/12 | 63.66 ± 4.95 U/g Hb |
| Tavilani H et al. 2012, Iran | Er | 60 | 67 | NR | 64.7 ± 31.70 U/g Hb | 30 | 66 | NR | 80.74 ± 46.50 U/g Hb |
| Ahmad H et al. 2013, India | Er | 75 | 42 | 53/22 | 48.32 ± 14.20 U/g Hb | 140 | 45 | 111/29 | 43.04 ± 9.93 U/g Hb |
| Arja C et al. 2013, India | Er | 150 | 61 | NR | 43.63 ± 1.61 U/g Hb | 236 | 63 | NR | 36.36 ± 4.57 U/g Hb |
| Wozniak A et al. 2013, Poland | Er | 35 | 45 | 19/16 | 13.8 ± 46 U/g Hb | 108 | 49 | 61/47 | 8.4 ± 3.1 U/g Hb |
| Montoya-Estrada A et al. 2013, Mexico | Er | 11 | 61 | 1/10 | 13.90 ± 1.98 mU/mg protein | 43 | 69 | 30/13 | 12.89 ± 2.51 mU/mg protein |
| Bukowska B et al. 2015, Poland | Er | 18 | NR | NR | 53.66 ± 9.56 mU/g Hb | 30 | NR | NR | 43.70 ± 11.20 mU/g Hb |
| Elmasry SA et al. 2015, Egypt | WB | 40 | 54 | 31/9 | 12.2 ± 0.7 U/mL | 34 | 55 | 27/7 | 12 ± 0.9 U/mL |
| Mohammed A et al. 2017, India | Er | 59 | 51 | 38/21 | 63.77 ± 3.38 U/mg protein | 127 | 60 | 98/29 | 59.43 ± 5.63 U/mg protein |
| Di Stefano A et al. 2018, Italy | WB | 27 | NR | 12/15 | 293 ± 332 U/mL | 45 | NR | 39/6 | 143 ± 159 U/mL |
| Al-Azzawi MA et al. 2019, Egypt | Er | 40 | 45 | 28/12 | 47.5 ± 1.82 U/mL | 30 | 65 | 21/9 | 15.9 ± 1.2 U/mL |
| SERUM/PLASMA | |||||||||
| Premanand R et al. 1994, India | S | 100 | NR | 60/40 | 0.231 ± 0.040 U/mL | 75 | NR | 43/32 | 0.204 ± 0.040 U/mL |
| Nadeem A et al. 2005, India | P | 21 | NR | NR | 129.9 ± 24.1 mU/g Hb | 51 | NR | NR | 156.4 ± 30.8 mU/g Hb |
| Vibhuti A et al. 2007, India | P | 136 | 50 | 110/26 | 19.1 ± 3.5 U/mL | 202 | 59 | 160/42 | 17.9 ± 7.1 U/mL |
| Montaño M et al. 2010, Mexico | P | 30 | 65 | 0/30 | 0.11 ± 0.03 U/mL | 60 | 73 | 0/60 | 0.23 ± 0.22 U/mL |
| Wassem SM et al. 2012, India | S | 60 | 38 | 46/14 | 57.21 ± 0.39 mU/mg protein | 121 | 48 | 80/41 | 51.46 ± 2.77 mU/mg protein |
| Zeng M et al. 2013, China | P | 28 | 69 | 23/5 | 214.2 ± 6.9 U | 35 | 71 | 31/4 | 183.0 ± 4.6 U |
| Ben Anes A et al. 2014, Tunisia | P | 229 | 58 | NR | 33.6 ± 24.1 U/ml | 153 | 61 | NR | 121.3 ± 33.0 U/ml |
| Ambade VN et al. 2015, India | P | 96 | 60 | 73/23 | 50.95 ± 15.30 U/L | 96 | 68 | 73/23 | 89.73 ± 27.84 U/L |
| Hartmann SE et al. 2015, Canada | P | 14 | 68 | 6/8 | 41.41 ± 8.75 U/ml | 12 | 69 | 4/8 | 36.41 ± 9.84 U/ml |
| Al-Azzawi MA et al. 2017, Egypt | P | 80 | 53 | 62/18 | 11.98 ± 1.01 mU/ml | 80 | 55 | 58/22 | 12.13 ± 0.92 mU/ml |
| Study | Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Was the Exposure Measured in a Valid and Reliable Way? | Were Objective, Standard Criteria Used for Measurement of the Condition? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the Outcomes Measured in a Valid and Reliable Way? | Was Appropriate Statistical Analysis Used? | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Santos et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Nadeem et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Joppa et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Biljak et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Lakhdar et al. | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Tavilani et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Ahmad et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Arja et al. | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Wozniak et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Montoya et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Bukowska et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Elmasry et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Mohammed et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Di Stefano et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Al-Azzawi et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Premanand et al. | No | Yes | Yes | Yes | No | No | Yes | No | Moderate |
| Nadeem et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Vibhuti et al. | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Montano et al. | No | No | Yes | No | No | No | Yes | No | High |
| Waseem et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Zeng et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Ben Anes et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Ambade et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Hartmann et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Al-Azzawi et al. | No | Yes | No | No | No | No | Yes | No | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zinellu, E.; Zinellu, A.; Pau, M.C.; Piras, B.; Fois, A.G.; Mellino, S.; Carru, C.; Mangoni, A.A.; Pirina, P. Glutathione Peroxidase in Stable Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. Antioxidants 2021, 10, 1745. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111745
Zinellu E, Zinellu A, Pau MC, Piras B, Fois AG, Mellino S, Carru C, Mangoni AA, Pirina P. Glutathione Peroxidase in Stable Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. Antioxidants. 2021; 10(11):1745. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111745
Chicago/Turabian StyleZinellu, Elisabetta, Angelo Zinellu, Maria Carmina Pau, Barbara Piras, Alessandro G. Fois, Sabrina Mellino, Ciriaco Carru, Arduino A. Mangoni, and Pietro Pirina. 2021. "Glutathione Peroxidase in Stable Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis" Antioxidants 10, no. 11: 1745. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111745