
Effects of Colchicine in a Rat Model of Diet-Induced Hyperlipidemia

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
2.2. Liver and Plasma Lipids Profile
2.3. Inflammation Markers
2.4. Oxidative Stress Markers
2.5. Histopathological Analysis of Liver, Heart and Aorta
2.6. Echocardiography
2.7. Statistical Analysis
3. Results
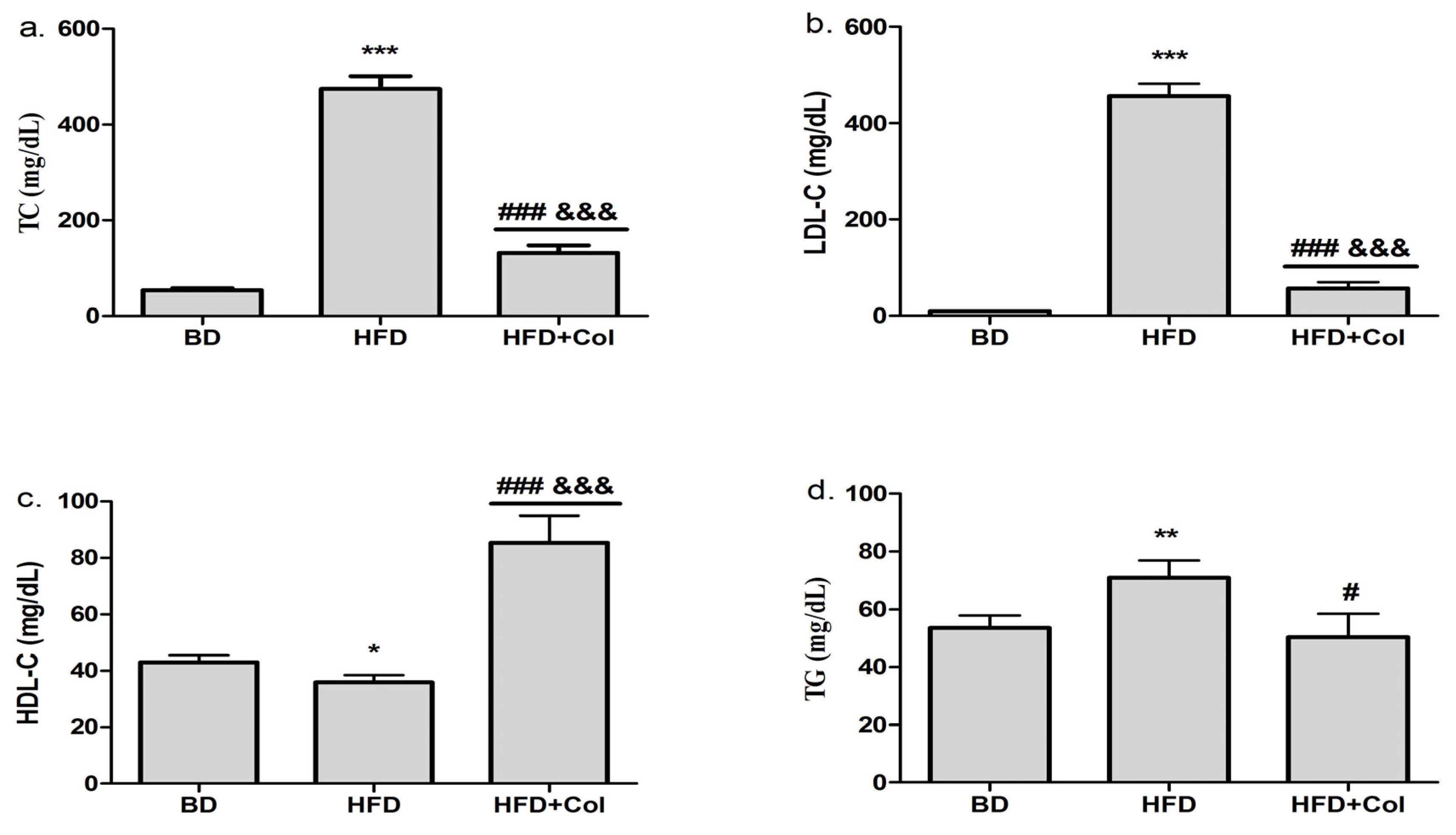
3.1. Effects of Colchicine on Plasma Lipid Profile
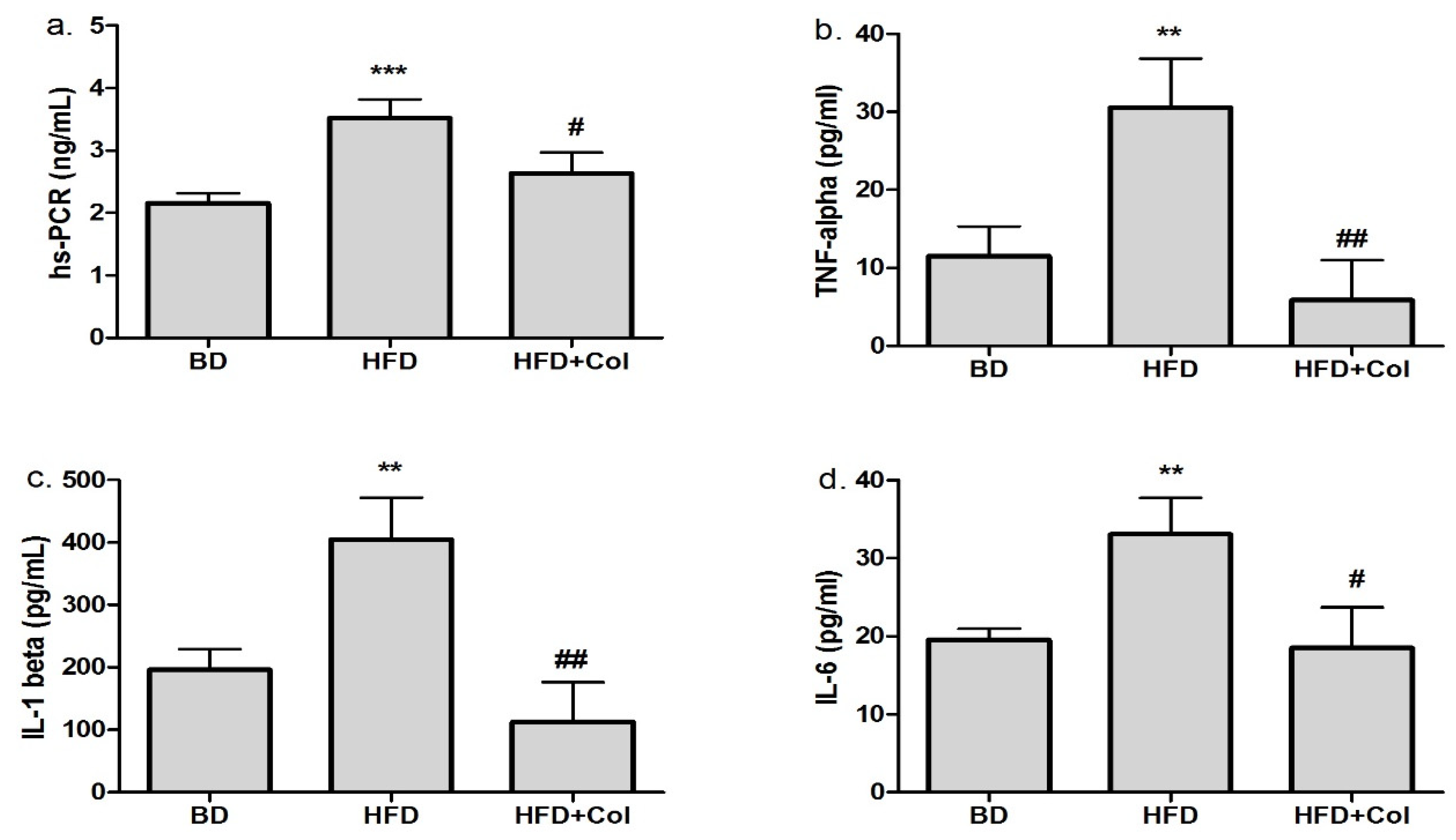
3.2. Anti-Inflammatory Effects of Colchicine
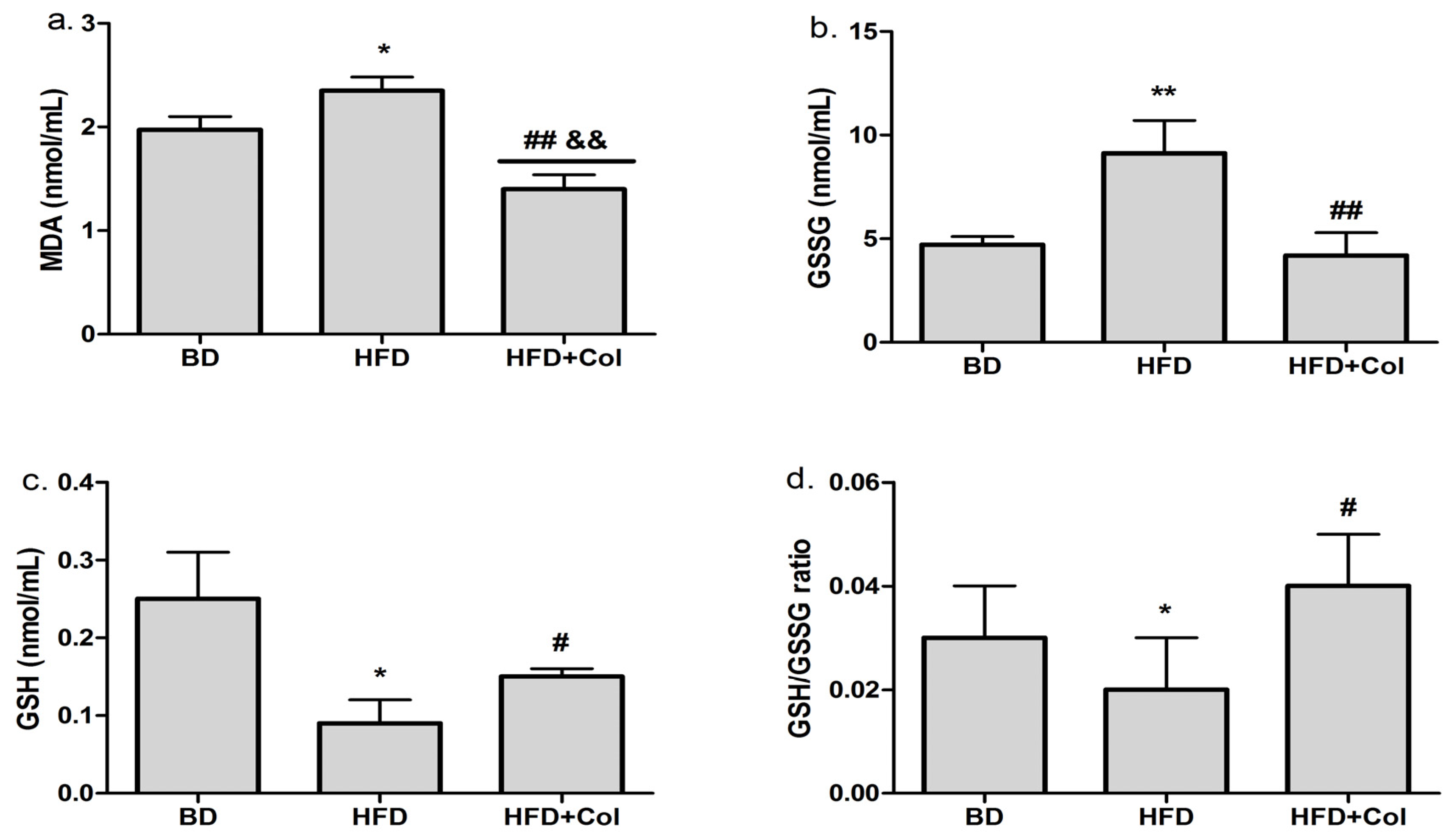
3.3. Antioxidant Effects of Colchicine
3.4. Colchicine Effects on Liver Enzymes
3.5. Histopathological Changes in Liver, Heart and Artery Tissue
3.6. Colchicine Effects on Echocardiographic Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abubakar, I.I.; Tillmann, T.; Banerjee, A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Cinteza, M.; Pana, B.; Cochino, E.; Florescu, M.; Margulescu, A.; Florian, A.; Vinereanu, D. Prevalence and control of cardiovascular risk factors in Romania—Cardio-Zone National Study. Cardiology 2009, 113, 110. [Google Scholar]
- Dorobantu, M.; Darabont, R.; Badila, E. Prevalence, Awareness, Treatment, and Control of Hypertension in Romania: Results of the SEPHAR Study. Int. J. Hypertens. 2010, 2010, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramji, D.P.; Davies, T.S. Cytokines in atherosclerosis: Key players in all stages of the disease and promising therapeutic targets. Cytokine Growth Factor Rev. 2015, 26, 673–685. [Google Scholar] [CrossRef] [Green Version]
- Sanjadi, M.; Rezvanie Sichanie, Z.; Totonchi, H.; Karami, J.; Rezaei, R.; Aslani, S. Atherosclerosis and autoimmunity: A growing relationship. Int. J. Rheum. Dis. 2018, 21, 908–921. [Google Scholar] [CrossRef] [Green Version]
- Soiza, R.L.; Donaldson, A.I.C.; Myint, P.K. Vaccine against arteriosclerosis: An update. Ther. Adv. Vaccines 2018, 9, 259–261. [Google Scholar]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; De Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics’ 2017 Update: A Report from the American Heart Association. Circulation 2017, 135, 146–603. [Google Scholar] [CrossRef]
- Wolf, D.; Ley, K. Immunity and Inflammation in Atherosclerosis. Circ. Res. 2019, 124, 315–327. [Google Scholar] [CrossRef]
- Taleb, S. L’inflammation dans l’athérosclérose. Arch. Cardiovasc. Dis. 2016, 109, 708–715. [Google Scholar] [CrossRef]
- Li, B.; Li, W.; Li, X.; Zhou, H. Inflammation: A Novel Therapeutic Target/Direction in Atherosclerosis. Curr. Pharm. Des. 2017, 23, 1216–1227. [Google Scholar] [CrossRef]
- Jose, T.; Magnus, B.; Lina, B.; Marie, L.B.P.; Bertrand, C.; Mat, J.D.; Egido, J.; Evans, P.C.; Francis, S.E.; Ketelhuth, D.F.J.; et al. Interplay between dyslipidemia and inflammation in atherosclerosis: Translating experimental targets into clinical practice. Eur. J. Prev. Cardiol. 2018, 25, 948–955. [Google Scholar]
- Zhu, Y.; Xian, X.; Wang, Z.; Bi, Y.; Chen, Q.; Han, X.; Tang, D.; Chen, R. Research progress on the relationship between atherosclerosis and inflammation. Biomolecules 2018, 8, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badimon, L.; Peña, E.; Arderiu, G.; Padró, T.; Slevin, M.; Vilahur, G.; Chiva-Blanch, G. C-reactive protein in atherothrombosis and angiogenesis. Front Immunol. 2018, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- The Emerging Risk Factors Collaboration. C-Reactive Protein, Fibrinogen, and Cardiovascular Disease Prediction. N. Engl. J. Med. 2012, 367, 1310–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Lüscher, T.F. Anti-inflammatory therapies for cardiovascular disease. Eur. Heart J. 2014, 35, 1782–1791. [Google Scholar] [CrossRef] [PubMed]
- Zălar, D.M.; Pop, C.; Buzdugan, E.; Todea, D.; Mogoșan, C.I. The Atherosclerosis-Inflammation relationship—A Pathophysiological approach. Farmacia 2019, 67, 6. [Google Scholar] [CrossRef]
- Singh, U.N.; Kumar, S.; Dhakal, S. Study of Oxidative Stress in Hypercholesterolemia. Int. J. Contemp. Med. Res. 2017, 4, 2454–7379. [Google Scholar]
- Piechota-Polanczyk, A.; Fichna, J. Review article: The role of oxidative stress in pathogenesis and treatment of inflammatory bowel diseases. Naunyn Schmiedebergs Arch. Pharmacol. 2014, 387, 605–620. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.L.; Shi, Y.H.; Hao, G.; Li, W.; Le, G.W. Increasing oxidative stress with progressive hyperlipidemia in humans: Relation between malondialdehyde and atherogenic index. J. Clin. Biochem. Nutr. 2008, 43, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Shan, Y.; Chen, L.; Lin, B.; Xiong, X.; Lin, L.; Jin, L. Colchicine protects rat skeletal muscle from ischemia/reperfusion injury by suppressing oxidative stress and inflammation. Iran. J. Basic Med. Sci. 2016, 19, 670–675. [Google Scholar]
- Jackman, R.W.; Rhoads, M.G.; Cornwell, E.; Kandarian, S.C. Microtubule-mediated NF-κB activation in the TNF-α signalling pathway. Exp. Cell Res. 2009, 315, 3242–3249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, D.; Pemberton, P.W.; Burrows, P.C.; Gordon, C.; Smith, A.; McMahon, R.F.T.; Warnes, T.W. Antioxidant properties of colchicine in acute carbon tetrachloride induced rat liver injury and its role in the resolution of established cirrhosis. Biochim. Biophys. Acta Mol. Basis Dis. 2000, 1502, 351–362. [Google Scholar] [CrossRef]
- Ridker, P.M. Targeting inflammatory pathways for the treatment of cardiovascular disease. Eur. Heart J. 2014, 35, 540–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, C.E.; Xu, R.; Sigal, S.H. Colchicine-Induced Hepatotoxicity. ACG Case Rep. J. 2017, 4, e120. [Google Scholar] [CrossRef] [PubMed]
- Zălar, D.-M.; Pop, C.; Buzdugan, E.; Kiss, B.; Ştefan, M.-G.; Ghibu, S.; Bâlteanu, V.-A.; Crişan, D.; Buruiană-Simic, A.; Grozav, A.; et al. Pharmacological Effects of Methotrexate and Infliximab in a Rats Model of Diet-Induced Dyslipidemia and Beta-3 Overexpression on Endothelial Cells. J. Clin. Med. 2021, 10, 3143. [Google Scholar] [CrossRef]
- Prins, K.W.; Tian, L.; Wu, D.; Thenappan, T.; Metzger, J.M.; Archer, S.L. Colchicine Depolymerizes Microtubules, Increases Junctophilin-2, and Improves Right Ventricular Function in Experimental Pulmonary Arterial Hypertension. J. Am. Heart Assoc. 2017, 6, e006195. [Google Scholar] [CrossRef] [Green Version]
- Pop, C.; Berce, C.; Ghibu, S.; Scurtu, I.; Sorițău, O.; Login, C.; Kiss, B.; Ștefan, M.G.; Fizeșan, I.; Silaghi, H.; et al. Effects of Lycium barbarum L. Polysaccharides on Inflammation and Oxidative Stress Markers in a Pressure Overload-Induced Heart Failure Rat Model. Molecules 2020, 25, 466. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef]
- Zhou, J.M.; Wang, H.M.; Lv, Y.Z.; Wang, Z.Z.; Xiao, W. Anti-atherosclerotic effect of Longxuetongluo Capsule in high cholesterol diet-induced atherosclerosis model rats. Biomed Pharmacother. 2018, 97, 793–801. [Google Scholar] [CrossRef]
- Talbert, R.L. Dyslipidemia. In Pharmacotherapy: A Pathophysiologic Approach, 10th ed.; DiPiro, J.T., Yee, G.C., Matzke, G.R., Wells, B.G., Posey, L., Eds.; McGraw Hill: New York, NY, USA, 2017. [Google Scholar]
- Gou, S.H.; Huang, H.F.; Chen, X.Y.; Liu, J.; He, M.; Ma, Y.Y.; Zhao, X.; Zhang, Y.; Ni, J. Lipid-lowering, hepatoprotective, and atheroprotective effects of the mixture Hong-Qu and gypenosides in hyperlipidemia with NAFLD rats. J. Chin. Med. Assoc. 2016, 79, 111–121. [Google Scholar] [CrossRef]
- Kumar, R.; Salwe, K.J.; Kumarappan, M. Evaluation of antioxidant, hypolipidemic, and antiatherogenic property of lycopene and astaxanthin in atherosclerosis-induced rats. Pharmacogn. Res. 2017, 9, 161–167. [Google Scholar]
- Tan, B.L.; Norhaizan, M.E. Effect of high-fat diets on oxidative stress, cellular inflammatory response and cognitive function. Nutrients 2019, 11, 2579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, D.P.; Gasparyan, A.Y.; Zimba, O. Benefits and adverse effects of hydroxychloroquine, methotrexate and colchicine: Searching for repurposable drug candidates. Rheumatol. Int. 2020, 40, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Verweij, S.L.; Van Der Valk, F.M.; Stroes, E.S.G. Novel directions in inflammation as a therapeutic target in atherosclerosis. Curr. Opin. Lipidol. 2015, 26, 580–585. [Google Scholar] [CrossRef]
- Martínez, G.J.; Robertson, S.; Barraclough, J.; Xia, Q.; Mallat, Z.; Bursill, C.; Celermajer, D.S.; Patel, S. Colchicine Acutely Suppresses Local Cardiac Production of Inflammatory Cytokines in Patients with an Acute Coronary Syndrome. J. Am. Heart Assoc. 2015, 4, e002128. [Google Scholar] [CrossRef] [Green Version]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-dose colchicine for secondary prevention of cardiovascular disease. J. Am. Coll. Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef] [Green Version]
- Yousuf, O.; Mohanty, B.D.; Martin, S.S.; Joshi, P.H.; Blaha, M.J.; Nasir, K.; Blumenthal, R.S.; Budoff, M.J. High-sensitivity C-reactive protein and cardiovascular disease: A resolute belief or an elusive link? J. Am. Coll. Cardiol. 2013, 62, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Fiolet, A.T.L.; Silvis, M.J.M.; Opstal, T.S.J.; Bax, W.A.; van der Horst, F.A.L.; Mosterd, A.; de Kleijn, D.; Cornel, J. Short-term effect of low-dose colchicine on inflammatory biomarkers, lipids, blood count and renal function in chronic coronary artery disease and elevated high-sensitivity C-reactive protein. PLoS ONE 2020, 15, 1–15. [Google Scholar] [CrossRef]
- Zhang, Q.; Qian, Z.Y.; Zhou, P.H.; Zhou, X.L.; Zhang, D.L.; He, N.; Zhang, J.; Liu, Y.; Gu, Q. Effects of oral selenium and magnesium co-supplementation on lipid metabolism, antioxidative status, histopathological lesions, and related gene expression in rats fed a high-fat diet. Lipids Health Dis. 2018, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pop, C.; Berce, C.; Ghibu, S.; Pop, A.; Kiss, B.; Irimie, A.; Popa, Ș.; Cismaru, G.; Loghin, F.; Mogoșan, C. Validation and characterisation of a heart failure animal model. Farmacia 2016, 64, 435–443. [Google Scholar]
- Zalewska, A.; Ziembicka, D.; Zendzian-Piotrowska, M.; MacIejczyk, M. The impact of high-fat diet on mitochondrial function, free radical production, and nitrosative stress in the salivary glands of wistar rats. Oxid. Med. Cell. Longev. 2019, 2019, 2606120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grozav, A.; Hanganu, D.; Crisan, O.; Porumb, D.; Cristea, C. Synthesis and antioxidant capacity of (chlorobenzylidene)hydrazinyl-thiazoles. Stud. Univ. Babes Bolyai Chem. 2019, 64, 509–516. [Google Scholar] [CrossRef]
- Kim, E.J.; Kim, B.H.; Seo, H.S.; Lee, Y.J.; Kim, H.H.; Son, H.H.; Choi, M.H. Cholesterol-induced non-alcoholic fatty liver disease and atherosclerosis aggravated by systemic inflammation. PLoS ONE 2014, 9, e97841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisue, K.; Sugamura, K.; Kurokawa, H.; Matsubara, J.; Ishii, M.; Izumiya, Y.; Kaikita, K.; Sugiyama, S. Colchicine Improves Survival, Left Ventricular Remodeling, and Chronic Cardiac Function After Acute Myocardial Infarction. Circ. J. 2017, 81, 1174–1182. [Google Scholar] [CrossRef] [Green Version]
- Massimo, I.; Mark, N. Colchicine and the heart. Eur. Heart J. 2021, 42, 2745–2760. [Google Scholar]
- Nadia, B.; Jean-Claude, T.; David, D.W.; Fausto, J.P.; Aldo, P.M.; Rafael, D.; Berry, C.; Koenig, W.; Lopez-Sendon, J.; Gamra, H.; et al. Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur. Heart J. 2020, 41, 4092–4099. [Google Scholar]
- Otto, C.M. Heartbeat: Colchicine and heart disease. Heart 2016, 102, 567–568. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Echocardiography Parameter | BD (n = 8) | HFD (n = 8) | HFD + Col (n = 8) |
|---|---|---|---|
| IVS (interventricular septum) (mm) | 1.43 ± 0.34 | 1.43 ± 0.25 | 1.46 ± 0.18 |
| PW (posterior wall) (mm) | 1.70 ± 0.30 | 1.70 ± 0.26 | 1.75 ± 0.24 |
| EDD (end-diastolic diameter) (mm) | 6.63 ± 0.95 | 7.41 ± 0.69 * | 7.10 ± 0.42 # |
| ESD (end-systolic diameter) (mm) | 4.17 ± 0.79 | 5.25 ± 0.71 * | 4.73 ± 0.47 # |
| LV mass (g) | 1.14 ± 0.06 | 1.24 ± 0.01 * | 1.21 ± 0.08 |
| EF (ejection fraction) Simpson rule (%) | 72.87 ± 7.81 | 66.61 ± 5.70 * | 74.59 ± 4.16 # |
| CO (cardiac output) (mL) | 124.16 ± 5.12 | 113.19 ± 2.41 * | 129.22 ± 5.61 # |
| Heart rate (bpm) | 258.80 ± 45.64 | 189.63 ± 28.37 | 233.17 ± 23.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zălar, D.-M.; Pop, C.; Buzdugan, E.; Kiss, B.; Ştefan, M.-G.; Ghibu, S.; Crişan, D.; Buruiană-Simic, A.; Grozav, A.; Borda, I.M.; et al. Effects of Colchicine in a Rat Model of Diet-Induced Hyperlipidemia. Antioxidants 2022, 11, 230. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11020230
Zălar D-M, Pop C, Buzdugan E, Kiss B, Ştefan M-G, Ghibu S, Crişan D, Buruiană-Simic A, Grozav A, Borda IM, et al. Effects of Colchicine in a Rat Model of Diet-Induced Hyperlipidemia. Antioxidants. 2022; 11(2):230. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11020230
Chicago/Turabian StyleZălar, Denisa-Mădălina, Cristina Pop, Elena Buzdugan, Bela Kiss, Maria-Georgia Ştefan, Steliana Ghibu, Doiniţa Crişan, Alexandra Buruiană-Simic, Adriana Grozav, Ileana Monica Borda, and et al. 2022. "Effects of Colchicine in a Rat Model of Diet-Induced Hyperlipidemia" Antioxidants 11, no. 2: 230. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11020230