Chemoprevention of Experimental Periodontitis in Diabetic Rats with Silk Fibroin Nanoparticles Loaded with Resveratrol


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.1.1. Animals
2.1.2. Experimental Design
Preparation and Evaluation of Treatments
Induction of Diabetes
Induction of Periodontitis and Treatment
Sample Processing
Enzymatic Assay
Pathological Anatomy
3. Results
3.1. Glycemic Index and Weight
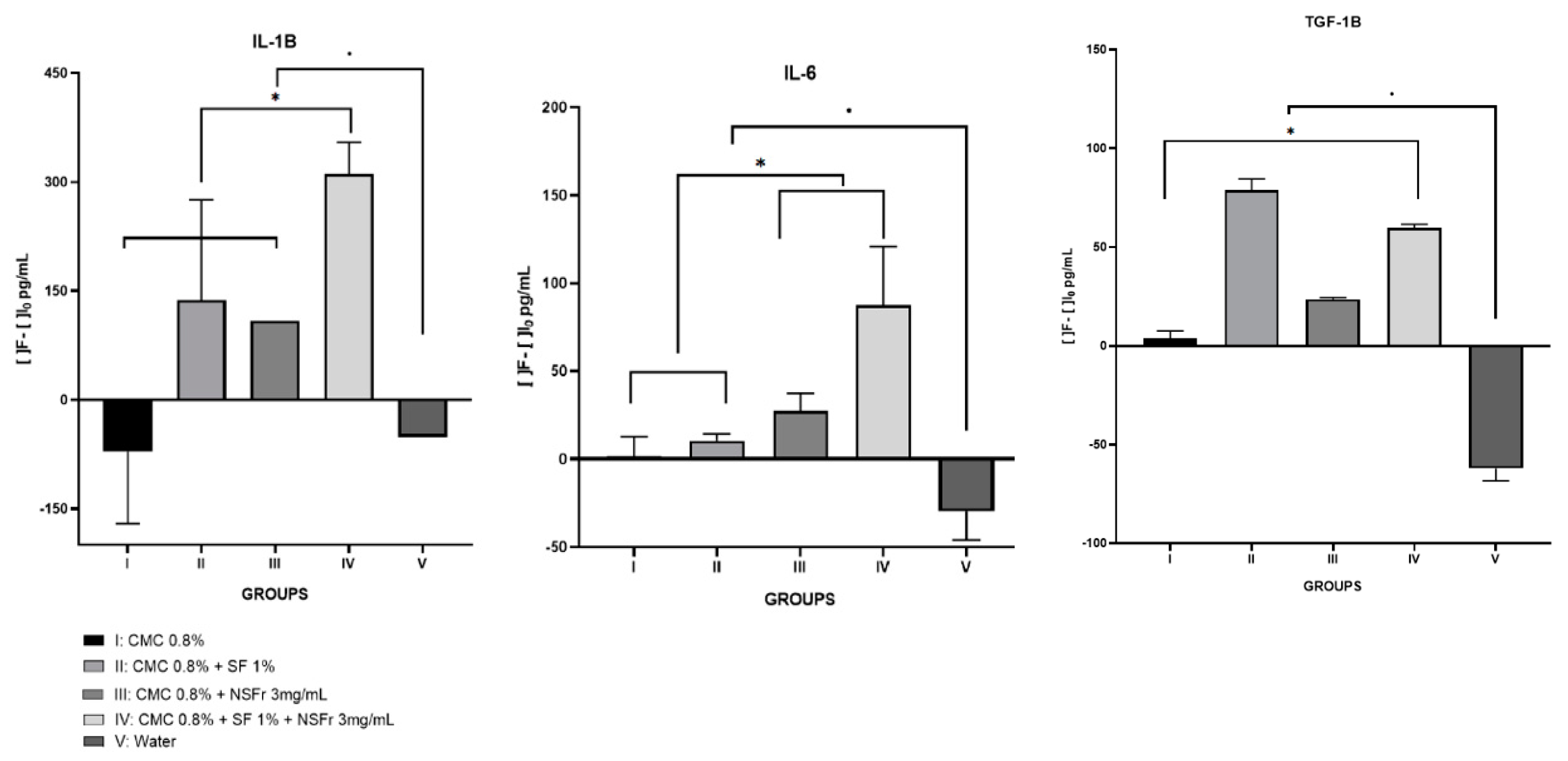
3.2. Elisa Assay
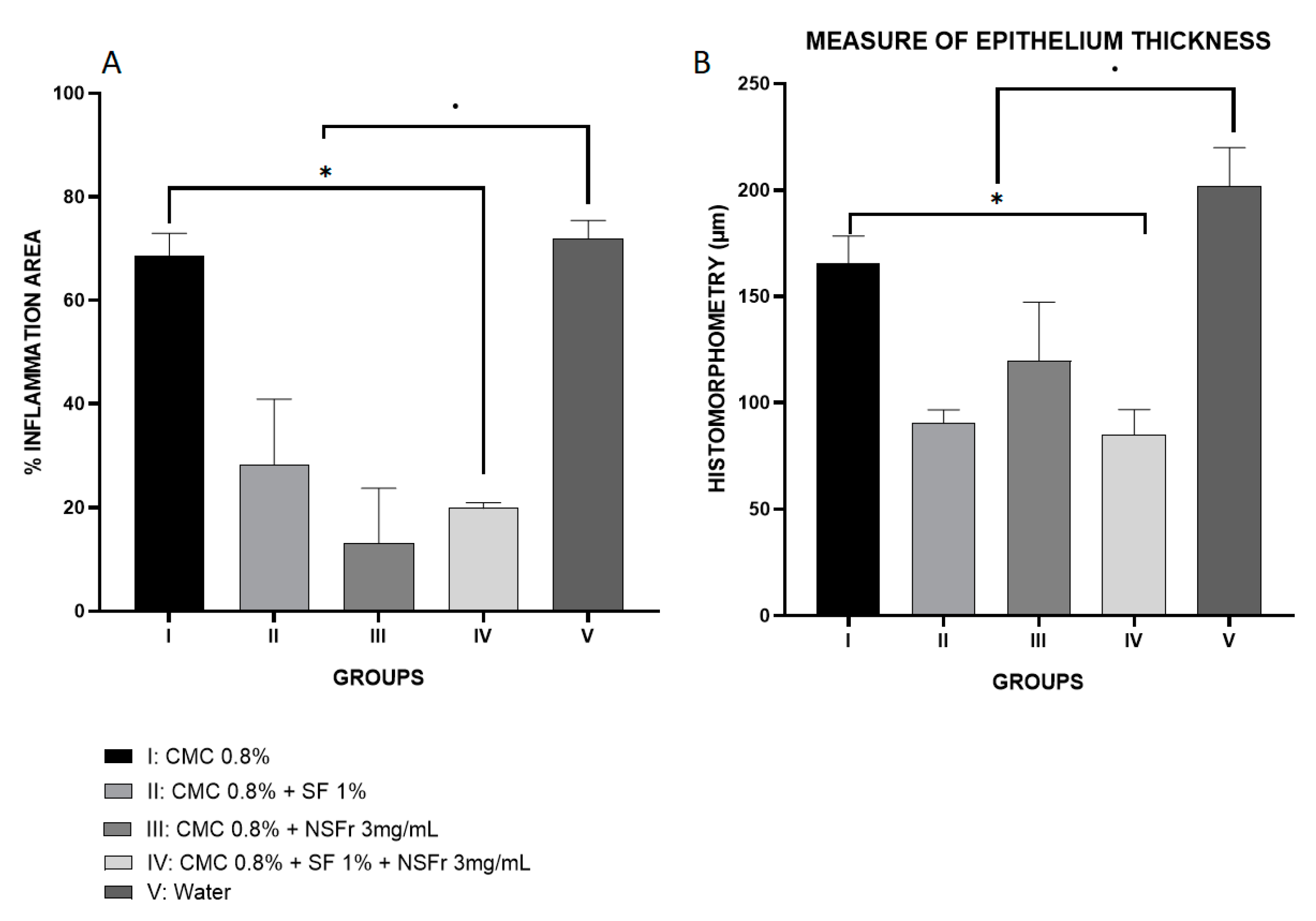
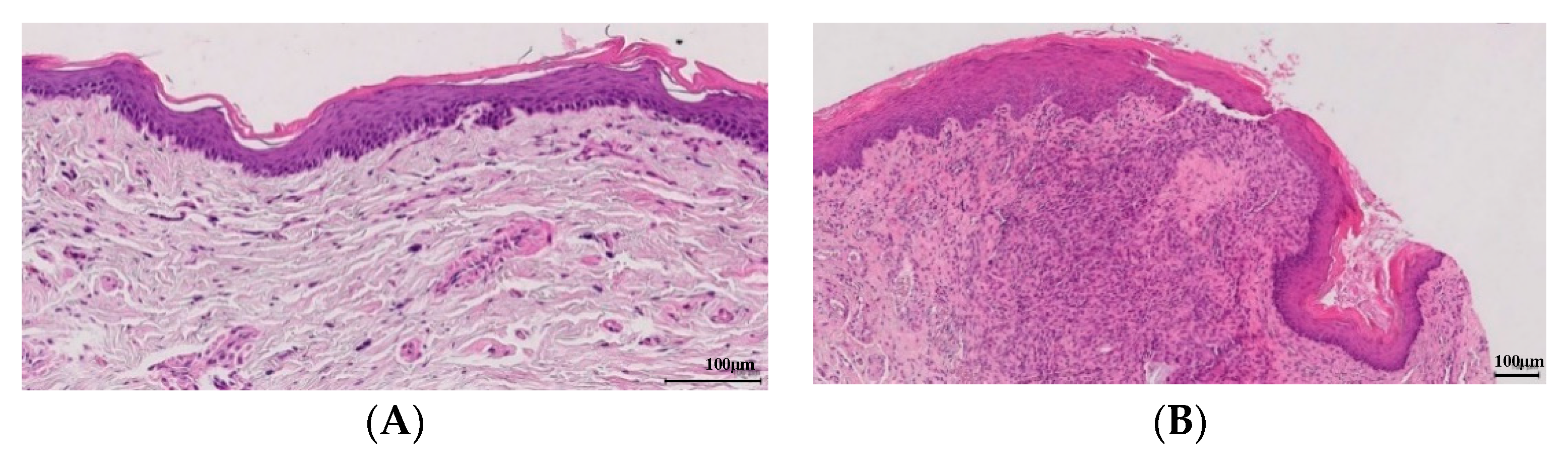
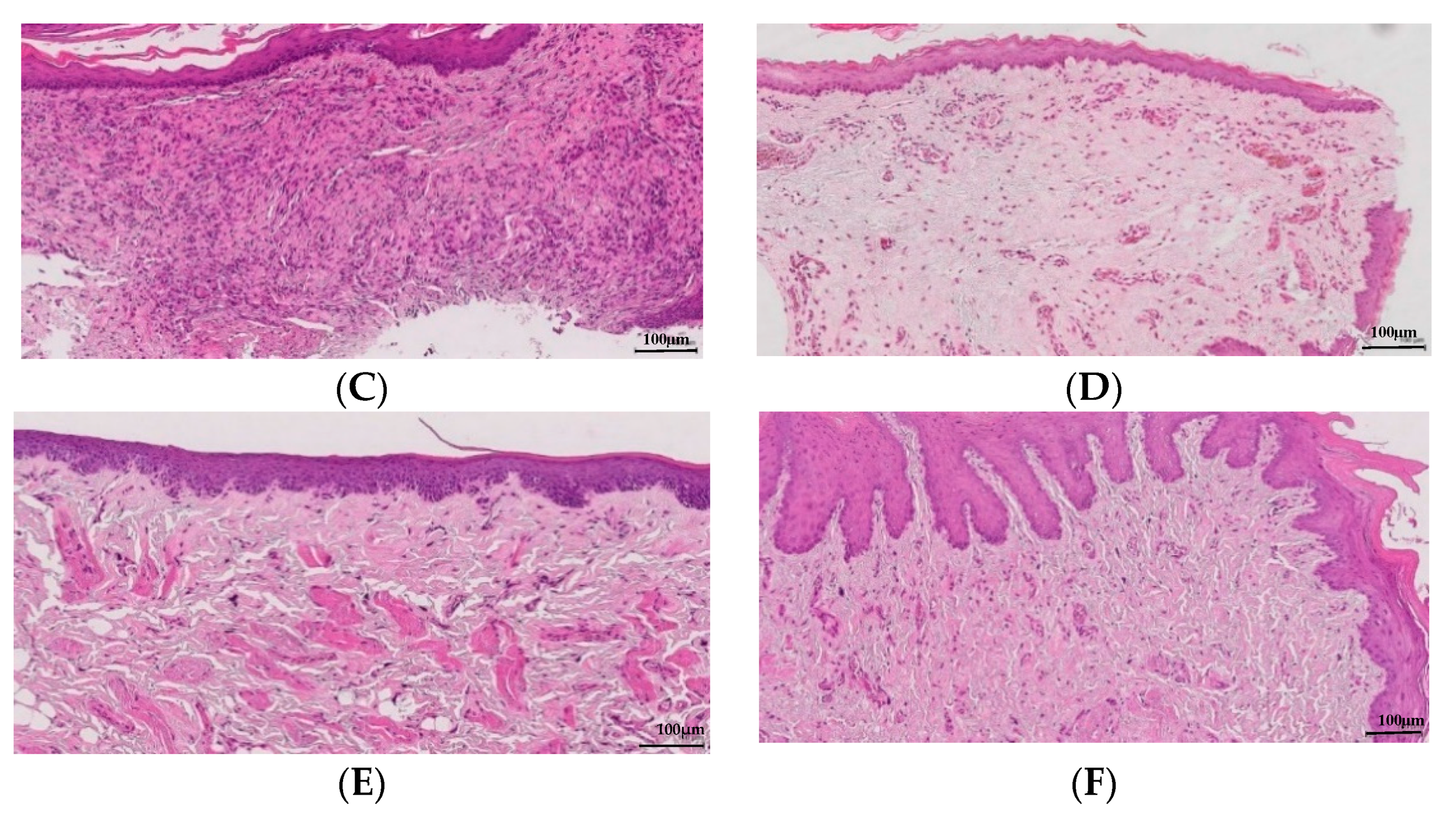
3.3. Pathological Anatomy
4. Discussion
4.1. ELISA Assays
4.2. Pathological Anatomy
4.3. Silk Fibroin and Resveratrol
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Borgnakke, W.S.; Ylöstalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Clin. Periodontol. 2013, 40, 135–152. [Google Scholar] [CrossRef]
- Aspriello, S.D.; Zizzi, A.; Tirabassi, G.; Buldreghini, E.; Biscotti, T.; Faloia, E.; Stramazzotti, D.; Boscaro, M.; Piemontese, M. Diabetes mellitus-associated periodontitis: Differences between type 1 and type 2 diabetes mellitus. J. Periodontol. 2011, 46, 164–169. [Google Scholar] [CrossRef]
- Salvi, G.E.; Beck, J.D.; Offenbacher, S. PGE2, IL-1 beta, and TNF-alpha responses in diabetics as modifiers of periodontal disease expression. Ann. Periodontol. 1998, 3, 40–50. [Google Scholar] [CrossRef]
- Salvi, G.E.; Collins, J.G.; Yalda, B.; Arnold, R.R.; Lang, N.P.; Offenbacher, S. Monocytic TNF alpha secretion patterns in IDDM patients with periodontal diseases. J. Clin. Periodontol. 1997, 24, 8–16. [Google Scholar] [CrossRef]
- Kamimura, D.; Ishihara, K.; Hirano, T. IL-6 signal transduction and its physiological roles: The signal orchestration model. Rev. Physiol. Biochem. Pharmacol. 2003, 149, 1–38. [Google Scholar] [PubMed]
- Kristiansen, O.P.; Mandrup-Poulsen, T. Interleukin-6 and diabetes: The good, the bad, or the indifferent? Diabetes 2005, 54, 114–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, F.J.; Turner, W.; Belibasakis, G.; Martuscelli, G. Effects of growth factors and cytokines on osteoblast differentiation. Periodontology 2000 2006, 41, 48–72. [Google Scholar] [CrossRef] [PubMed]
- Kritsy, C.P.; Lynch, S.E. Role of growth factors in cutaneous wound healing: A review. Crit. Rev. Oral Biol. Med. 1993, 4, 729–760. [Google Scholar] [CrossRef] [Green Version]
- Marek, A.; Brodzicki, J.; Liberek, A.; Korzon, M. TGF-b (transforming growth factor-b) in chronic inflammatory conditions—A new diagnostic and prognostic marker? Med. Sci. Monit. 2002, 8, 145–151. [Google Scholar]
- Sporn, M.B.; Roberts, A.B. A major advantage in the use of growth factors to enhance wound healing. J. Clin. Investig. 1993, 92, 2565–2576. [Google Scholar] [CrossRef] [Green Version]
- Skaleric, U.; Kramar, B.; Petelin, M.; Pavlica, Z.; Wahl, S.M. Changes in TGF-b1 levels in gingiva, crevicular fluid and serum associated with periodontal inflammation in humans and dogs. Eur. J. Oral Sci. 1997, 105, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Csiszar, A. Anti-inflammatory effects of resveratrol: Possible role in prevention of age-related cardiovascular disease. Ann. N. Y. Acad. Sci. 2011, 1215, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, E.F.; Orlando, D.R.; Araújo, A.M.S.; de Andrade, J.N.B.M.; Azzi, D.V.; de Lima, R.R.; Lobo-Júnior, A.R.; Pereira, L.J. Can Resveratrol treatment control the progression of induced periodontal disease? A systematic review and Meta-Analysis of preclinical studies. Nutrients 2019, 11, 953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonamine, C.Y.; Pinheiro-Machado, E.; Michalani, M.L.; Alves-Wagner, A.B.; Esteves, J.V.; Freitas, H.S.; Machado, U.F. Resveratrol improves glycemic control in type 2 diabetic obese mice by regulating glucose transporter expression in skeletal muscle and liver. Molecules 2017, 22, 1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, A.; Smeets, R.; Gosau, M.; Friedrich, R.E.; Fuest, S.; Behbahani, M.; Barbeck, M.; Rutkowski, R.; Burg, S.; Kluwe, L.; et al. Production and characterization of porus fibroin scaffolds for regenerative medical application. In Vivo 2019, 33, 757–762. [Google Scholar] [CrossRef]
- Martıínez-Mora, C.; Mrowiec, A.; García-Vizcaíno, E.M.; Alcaraz, A.; Cenis, J.L.; Nicolás, F.J. Fibroin and Sericin from Bombyx mori Silk Stimulate Cell Migration through Upregulation and Phosphorylation of c-Jun. PLoS ONE 2012, 7, e42271. [Google Scholar] [CrossRef]
- Lozano-Pérez, A.A.; Rivero, H.C.; Pérez Hernández, M.D.C.; Pagán, A.; Montalbán, M.G.; Víllora, G.; Cénis, J.L. Silk fibroin nanoparticles: Efficient vehicles for the natural antioxidant quercetin. Int. J. Pharm. 2017, 518, 11–19. [Google Scholar] [CrossRef]
- Lozano-Pérez, A.A.; Rodriguez-Nogales, A.; Ortiz-Cullera, V.; Algieri, F.; Garrido-Mesa, J.; Zorrilla, P.; Rodriguez-Cabezas, M.E.; Garrido-Mesa, N.; Utrilla, M.P.; De Matteis, L.; et al. Silk fibroin nanoparticles constitute a vector for controlled re-lease of resveratrol in an experimental model of inflammatory bowel disease in rats. Int. J. Nanomed. 2014, 9, 4507–4520. [Google Scholar]
- Lozano-Pérez, A.A.; Gil, A.L.; Pérez, S.A.; Cutillas, N.; Meyer, H.; Pedreño, M.; DAznar-Cervantes, S.; Janiak, C.; Cenis, J.L.; Ruiz, J. Antitumor properties of platinum(IV) prodrug-loaded silk fibroin nanoparticles. Dalton Trans. 2015, 44, 13513–13521. [Google Scholar] [CrossRef]
- Montalbán, M.; Coburn, J.; Lozano-Pérez, A.A.; Cenis, J.; Víllora, G.; Kaplan, D. Production of Curcumin-Loaded Silk Fibro-in Nanoparticles for Cancer Therapy. Nanomaterials 2018, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Koh, L.D.; Cheng, Y.; Teng, C.P.; Khin, Y.W.; Loh, X.J.; Tee, S.Y.; Low, M.; Ye, E.; Yu, H.D.; Zhang, Y.W.; et al. Structures, mechanical properties and applications of silk fibroin materials. Prog. Polym. Sci. 2015, 46, 86–110. [Google Scholar] [CrossRef]
- Ionel, A.; Lucaciu, O.; Moga, M.; Buhatel, D.; Ilea, A.; Tabaran, F.; Catoi, C.; Berce, C.; Toader, S.; Campian, R.S. Periodontal disease induced in Wistar rats—Experimental study. Hum. Vet. Med. Bioflux 2015, 7, 90–95. [Google Scholar]
- Camacho-Alonso, F.; López-Jornet, M.P.; Jiménez-Torres, M.J.; Orduña-Domingo, A. Wound Healing with PRGF Infiltration in CO2 Laser Lesions of the Tongue: An Animal Study. Photomed. Laser Surg. 2009, 27, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Boşca, A.B.; Miclăuş, V.; Ilea, A.; Câmpian, R.S.; Rus, V.; Ruxanda, F.; Raţiu, C.; Uifălean, A.; Pârvu, A.E. Role of nitro-oxidative stress in the pathogenesis of experimental rat periodontitis. Clujul Med. 2016, 89, 150–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionel, A.; Lucaciu, O.; Tăbăran, F.; Berce, C.; Toader, S.; Hurubeanu, L.; Bondor, C.; Câmpian, R.S. Histology and Histopathological and clinical expression of periodontal disease related to the systemic inflammatory response. Histol. Histopatol. 2017, 32, 379–384. [Google Scholar]
- Fritz, H.; Becker, H. The suitability of carboxymethylcellulose as a vehicle in reproductive studies. Arzneimittelforschung 1981, 31, 813–815. [Google Scholar]
- Ebersole, J.L.; Schuster, J.L.; Stevens, J.; Dawson, D., 3rd; Kryscio, R.J.; Lin, Y.; Thomas, M.V.; Miller, C.S. Patterns of salivary analytes provide diagnostic capacity for distinguishing chronic adult periodontitis from health. J. Clin. Immunol. 2013, 33, 271–279. [Google Scholar] [CrossRef]
- Corrêa, M.G.; Pires, P.R.; Ribeiro, F.V.; Pimentel, S.Z.; Casarin, R.C.; Cirano, F.R.; Tenenbaum, H.T.; Casati, M.Z. Systemic treatment with resveratrol and/or curcumin reduces the progression of experimental periodontitis in rats. J. Periodontal Res. 2016, 52, 201–209. [Google Scholar] [CrossRef]
- Hosokawa, Y.; Shindo, S.; Hosokawa, I.; Ozaki KMatsuo, T. IL-6 trans-signaling enhances CCL20 production from IL-1B stimulated human periodontal ligament cells. Inflamation 2013, 37, 381–386. [Google Scholar] [CrossRef]
- Gürkan, A.; Emingil, G.; Çinarcik SBerdareli, A. Gingival crevicular fluid transforming growth factor β1 in several forms of periodontal disease. Arch. Oral Biol. 2006, 51, 906–912. [Google Scholar] [CrossRef]
- Lorencini, M.; Silva, J.A.; Almeida, C.A.; Bruni-Cardoso, A.; Carvalho HFStach-Machado, D.R. A new paradigm in the periodontal disease progression: Gingival connective tissue remodeling with simultaneous collagen degradation and fibers thickening. Tissue Cell 2009, 41, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Séguier, S.; Gogly, B.; Bodineau, A.; Godeau GBrousse, N. Is collagen breakdown during periodontitis linked to inflammatory cells and expression of matrix metalloproteinases and tissue inhibitors of metalloproteinases in human gingival tissue? J. Periodontol. 2001, 72, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Kasprzak, A.; Surdacka, A.; Tomczak, M.; Przybyszewska, W.; Seraszek-Jaros, A.; Malkowska-Lanzafame, A.; Siodla, E.; Kaczmarek, E. Expression of angiogenesis-stimulating factors (VEGF, CD31, CD105) and angiogenetic index in gingivae of patients with chronic periodontitis. Folia Histochem. Cytobiol. 2012, 50, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Li, Y.; Xie, M.B. Silk fibroin-based nanoparticles for drug delivery. Int. J. Mol. Sci. 2015, 16, 4880–4903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melke, J.; Midha, S.; Ghosh, S.; Ito, K.; Hofmann, S. Silk fibroin as biomaterial for bone tissue engineering. Acta Biomater. 2016, 31, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanna, V.; Pala, N.; Dessì, G.; Manconi, P.M.; Mariani, A.; Dedola, S.; Rassu, M.; Crosio, C.; Iaccarino, C.; Sechi, M. Single-step green synthesis and characterization of gold-conjugated polyphenol nanoparticles with antioxidant and biological activities. Int. J. Nanomed. 2014, 9, 4935–4951. [Google Scholar]
- Lopez-Chaves, C.; Soto, J.; Montes, M.; Bettmer, J.; Llopis, J.; Sanchez, C. Gold nanoparticles: Distribution, bioaccumulation and toxicity. In vitro and in vivo studies. Nanomedicine 2018, 14, 1–12. [Google Scholar] [CrossRef]
- Du, J.; Tang, J.; Xu, S.; Ge, J.; Dong, Y.; Li, H.; Jin, M. A review on silver nanoparticles-induced ecotoxicity and the underlying toxicity mechanism. Regul. Toxicol. Pharmacol. 2018, 98, 231–239. [Google Scholar] [CrossRef]
- De Vries, K.; Strydom, M.; Steenkamp, V. Bioavailability of resveratrol: Possibilities for enhancement. J. Herb. Med. 2018, 11, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.C.; Lee, C.H.; Wahlqvist, M.L.; Huang, H.L.; Chang, H.Y.; Chen, L.; Shih, S.F.; Shin, S.J.; Tsai, W.C.; Chen, T.; et al. Poverty increases Type 2 Diabetes Incidence and Inequality of Care Despite Universal Health Coverage. Diabetes Care 2012, 35, 2286–2292. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joing workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. Diabetes Res. Clin. Pract. 2018, 173, 231–241. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Treatment |
|---|---|
| I | CMC 0.8% (placebo) |
| II | CMC 0.8% + SF 1% |
| III | CMC 0.8% + RES-SFN 3 mg/mL |
| IV | CMC 0.8% +SF 1% + RES-SFN 3 mg/mL |
| V | Water (Control) |
| Variable | Group. Median (IR) | p-Value | ||||
|---|---|---|---|---|---|---|
| I | II | III | IV | V | ||
| INITIAL IL-1β (pg/mL) | 1421.27 (1349.31–1446.21) | 1378.71 (1312.11–1448.89) | 1486.99 (1468.77–1504.61) | 1698.71 (1680.86–1718) | 1056.57 (944.07–1159.07) | |
| FINAL IL1β (pg/mL) | 1434.31 (1222.17–1544.79) | 1199.67 (1106.75–1432.35) | 1390.8 (1348.54–1492.23) | 1402.46 (1326.93–1430.5) | 1646.15 (1563–1737.05) | |
| INITIAL IL-6 (pg/mL) | 100.33 (78.97–132.51) | 47.09 (39.44–57.25) | 67.1 (55.22–75.85) | 181.37 (153.56–204.6) | 103.66 (96.47–118.35) | |
| FINAL IL-6 (pg/mL) | 100.99 (82.55–119.97) | 39.14 (30.19–44.67) | 43.26 (17.99–53.97) | 93.14 (81.58–97.41) | 136.89 (131.47–146.26) | |
| INITIAL TGF-1β (pg/mL) | 4.69 (2.21–7.86) | 78.72 (75.88–84.48) | 80.26 (77.99–81.19) | 62.12 (59.53–63.03) | 43.89 (41.45–50.73) | |
| FINAL TGF-1β (pg/mL) | 0.81 (0–3.24) | 0 (0–0) | 56.13 (55.56–56.7) | 0.6 (0–2.4) | 106.02 (101.98–109.82) | |
| INITIAL WEIGHT (g) | 330 (322.5–332.5) | 360 (349–390) | 321.5 (318–347) | 325 (294–390) | 351 (304–374.5) | 0.303 |
| INITIAL GLUCEMIA (mg/dL) | 591.5 (481.5–600) | 591 (583–600) | 525.5 (495–593.5) | 569.5 (491–589) | 502 (471–514) | 0.045 |
| IL-1βDIFF (pg/mL) | −71.25 (−170.54–199.11) | 137.26 (−53.63–275.54) | 108.87 (−23.45–156.07) | 311.25 (286.79–354.64) | −510.3 (−792.98–403.93) | 0.014 |
| IL-6 DIFF (pg/mL) | 1.58 (−3.58–12.55) | 10.5 (7.53–14.3) | 27.59 (21.88–37.23) | 87.6 (58.44–120.73) | −29.79 (−46.04–16.88) | 0.002 |
| TGF-1β DIFF (pg/mL) | 3.88 (−0.7–7.52) | 78.72 (75.88–84.48) | 23.57 (22.43–24.49) | 59.79 (58.63–61.52) | −62.13 (−68.37–51.25) | 0.001 |
| Measurement | Group, Median (IR) | ||||
|---|---|---|---|---|---|
| I | II | III | IV | V | |
| Inflammation area (x̄ %) | 68.734 | 28.250 | 13.108 | 19.805 | 71.978 |
| Epithelium thickness (x̄, µm) | 165.560 | 90.255 | 119.545 | 85.860 | 189.297 |
| Vessel formation | 2 | 1 | 1 | 1 | 3 |
| Collagen | 2 | 2 | 1 | 0 | 3 |
| Membrane integrity | 1 | 1 | 1 | 1 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giménez-Siurana, A.; Gómez García, F.; Pagan Bernabeu, A.; Lozano-Pérez, A.A.; Aznar-Cervantes, S.D.; Cenis, J.L.; López-Jornet, P. Chemoprevention of Experimental Periodontitis in Diabetic Rats with Silk Fibroin Nanoparticles Loaded with Resveratrol. Antioxidants 2020, 9, 85. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9010085
Giménez-Siurana A, Gómez García F, Pagan Bernabeu A, Lozano-Pérez AA, Aznar-Cervantes SD, Cenis JL, López-Jornet P. Chemoprevention of Experimental Periodontitis in Diabetic Rats with Silk Fibroin Nanoparticles Loaded with Resveratrol. Antioxidants. 2020; 9(1):85. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9010085
Chicago/Turabian StyleGiménez-Siurana, Ana, Francisco Gómez García, Ana Pagan Bernabeu, Antonio Abel Lozano-Pérez, Salvador D. Aznar-Cervantes, José Luis Cenis, and Pía López-Jornet. 2020. "Chemoprevention of Experimental Periodontitis in Diabetic Rats with Silk Fibroin Nanoparticles Loaded with Resveratrol" Antioxidants 9, no. 1: 85. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9010085