1. Introduction
Heart failure (HF) is a complex multifactorial syndrome caused by structural and/or functional cardiac abnormalities, resulting in a reduced cardiac output or elevated intracardiac pressures [
1]. Heart failure prevalence is continuously rising throughout the world. In developed countries, approximately 2% of the adult population has heart failure.
Therapeutic developments over the past several decades have focused on blocking the neurohumoral (RAAS and adrenergic system) activation and on the inhibition of the breakdown of vasoactive peptides. Although this approach improved the survival of HFrEF (heart failure with reduced ejection fraction) patients [
2], the outcome of the disease still remained poor [
3,
4,
5,
6,
7,
8]. Therefore, there is an overwhelming need for new therapies in heart failure. Novel drugs in experimental and clinical trials targeting myocardial contractility (e.g., omecamtiv mecarbil), cytokines (e.g., anti-TNFα), myocardial metabolism (e.g., perhexiline) or oxidative stress [
9,
10] are promising and may present an alternative approach in the treatment of heart failure in the future.
Oxidative stress also has an important role in the pathogenesis of different cardiac pathologies, such as ischemia-reperfusion injury, cardiac remodeling and heart failure [
11,
12]. Resveratrol (3,5,4-trihydroxystilbene), a natural phytoalexin found in a wide variety of plants (e.g., nuts, berries and grapes) is produced in response to environmental stress [
13]. Given that resveratrol has a marked scavenger effect, it is not surprising that it can protect cells against oxidative damages [
14,
15,
16,
17]. Beyond its scavenger effect, resveratrol also has antioxidant effects in other ways. Resveratrol (RES) via the activation of the NAD
+-dependent histone/protein deacetylase SIRT1 (silent information regulator) and AMPK (AMP-activated protein kinase) facilitates mitochondrial biogenesis in cardiomyocytes. This is accompanied by enhanced oxidative phosphorylation and a higher amount of high energy phosphates (CrP and ATP) that can result in increased contractility and efficient protection against oxidative stress [
18,
19,
20]. Endothelial and vascular function can also be improved more by the RES treatment via decreasing the cholesterol and triglyceride levels via increasing the endothelial nitric oxide synthase (eNOS) activity and nitrogen oxide (NO) level, as well as due to its anti-inflammatory effects [
21,
22,
23,
24].
In systolic heart failure (HFrEF), the contractility of the heart muscle cells is decreased; moreover, a chronic low-intensity inflammation can be seen that can further aggravate heart failure. Our workgroup demonstrated previously that resveratrol supplementation in a post-infarct rodent model prevented the development of heart failure [
25]. RES improved the left ventricular function, as well as decreased myocardial fibrosis, oxidative stress and the amount of proinflammatory proteins (cyclooxygenase-2 (COX-2) and iNOS). Other workgroups showed similar results in various animal heart failure models. However, in human clinical trials, the effect of RES has not yet been confirmed [
13,
26].
The aim of our study was, therefore, to assess the effects of resveratrol treatment on the left ventricular function and on the exercise capacity, as well as on the biomarker and inflammatory cytokine levels in HFrEF.
2. Materials and Methods
2.1. Study Design
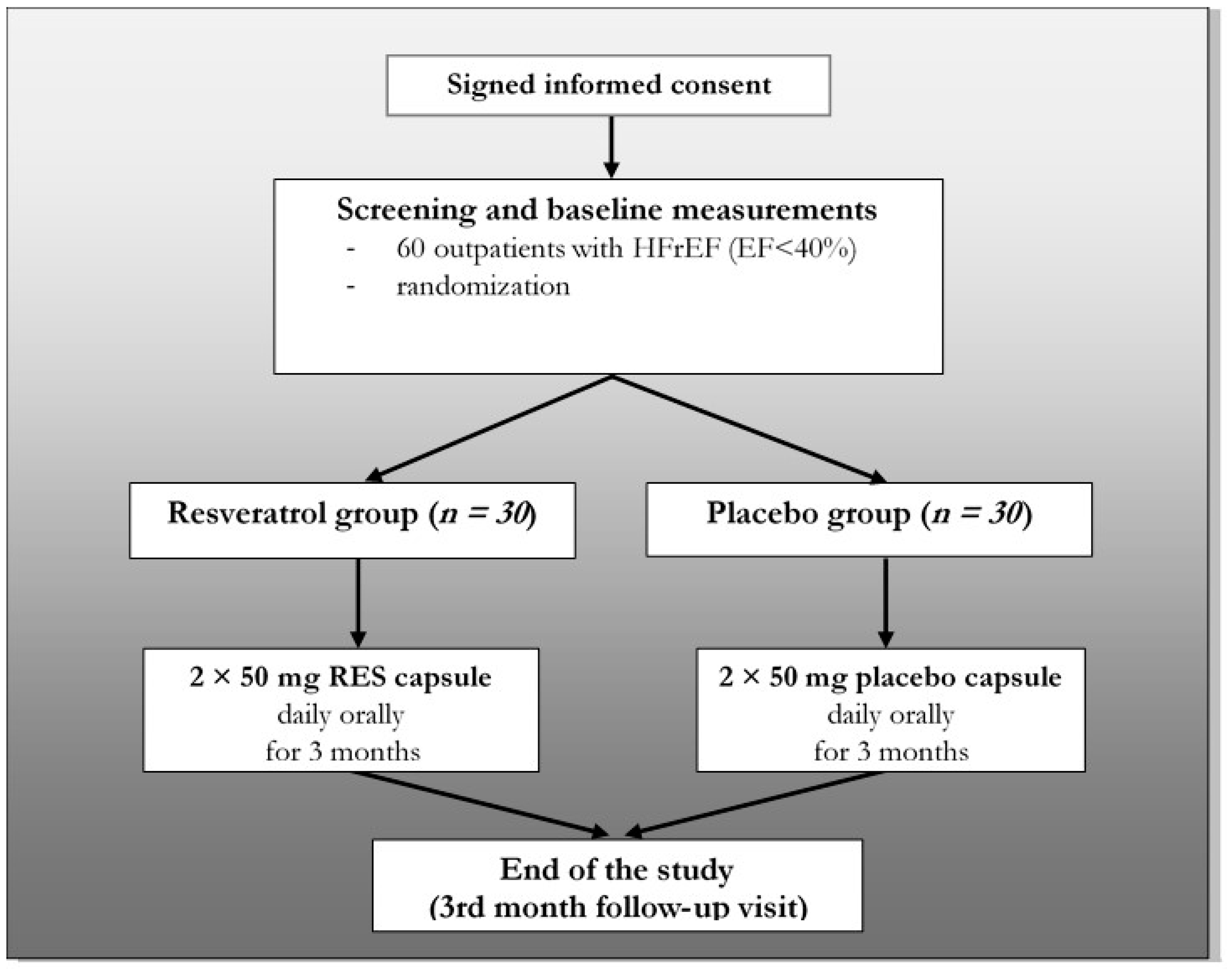
Our trial was a single-center, double-blind, randomized, placebo-controlled study. The study design is summarized in
Figure 1. The study was conducted in accordance with the principles stated in the Declaration of Helsinki (1996), International Conference on Harmonization Good Clinical Practice, as well as local and national regulations. The protocol of the trial was approved by the Regional Ethics Committee of the University of Pecs (license number: 5830). All patients provided written informed consent prior to any study-related procedures.
2.2. Eligibility
The main inclusion and exclusion criteria are listed in
Table 1. Briefly, 60 stable outpatients (ages: 66.7 ± 2.01 years, 17 women and 43 men) with HFrEF in NYHA (New York Heart Association) class II or III were enrolled between 01 March 2016 and 30 November 2017 into our study (ejection fraction (EF) <40% and ischemic/non-ischemic origin: 34/26). They were randomized into two groups (resveratrol group and placebo group). one-hundred milligrams of resveratrol was administered orally (2 × 50 mg) for 3 months in the RES group (
n = 30) and placebo capsule in the other group (
n = 30).
The resveratrol and the matching placebo capsules were purchased from Argina Nutraceuticals Ltd. (Fót, Hungary). The resveratrol capsule is commercially available and has an official license for being marketed.
All the involved patients were in the evidence-based drug treatment of HFrEF, including angiotensin-converting enzyme (ACE) inhibitors (or ARBs—angiotensin receptor blockers), beta-blockers, mineralocorticoid receptor antagonists and ivabradine. None of the patients received ARNI (angiotensin receptor-neprilysin inhibitor). The preventive drug regime and the used doses were based on the actual European Society of Cardiology (ESC) heart failure guideline [
1]. The patients had baseline visits and follow-up visits after 1 month and after 3 months of treatment. During visits, the compliance of patients was checked, and at the final visit (3-month follow-up visit), they were asked to return the remained capsules. During the whole study period, subjects were in stable clinical conditions and received unchanged medical therapy (
Table 2). The baseline characteristics of the randomized patients are detailed in
Table 2. There were no significant differences in epidemiological characteristics between the placebo and RES-treated groups at the baseline.
On the day of randomization and 3-months-later physical examination, blood pressure and weight measurement, echocardiography, lab test, six-minute walk test (6MWT), spirometry and quality of life questionnaire (QoL test) were performed. At the 1-month follow-up visit, only a physical examination, blood pressure, weight measurement and lab test were done (
Table 3).
2.3. Statistical Analysis
SPSS statistical software, version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) was used to conduct a descriptive analysis and to describe the sample. After using the Kolmogorov-Smirnov test to check the normality of the data distribution, differences of the mean values within the groups were analyzed by repeated-measures ANOVA with a Greenhouse–Geisser correction. Differences between the groups were calculated by one-way ANOVA test. Data are expressed as mean ± S.E.M. Significance level was defined as p < 0.05. The homogeneity of the groups was tested by Levene’s F-test. The nonparametric Friedman test (post-hoc analysis with Wilcoxon signed-rank test) was applied to analyze the potential changes of the quality of life of the patients.
2.4. Blood Pressure and Body Weight Measurement
Body weight and blood pressure were measured during randomization at 1-month and at 3-month follow-up visits. For body weight measurements, a high-quality calibrated digital scale was used (CAS PB-150 digital scale; CAS Corporation, Tustin, CA, USA). Blood pressures were measured using an automated electronic device after a 5-min resting; the location of the cuff was the upper arm at the level of the heart (OMRON M2 Intellisense, Tokyo, Japan). The technique of the measurement was based on the actual hypertension guideline [
27].
2.5. Laboratory Test
Laboratory analysis performed on blood samples that were extracted from the cubital vein after a 12-h-long fasting period. From blood samples, NT-proBNP; fasting lipid levels (total cholesterol, low-density lipoprotein (LDL)—cholesterol, high-density lipoprotein (HDL) -cholesterol and triglycerides); troponin T; glycosylated hemoglobin-HgbA1c; serum albumin; renal and liver function; serum iron parameters and quantitative and qualitative blood cell counts were measured in the Department of Laboratory Medicine, University of Pecs, Pecs, Hungary.
Special parameters (galectin-3, interleukin (IL)-1 and IL-6) were determined using an ELISA method in the Szentagothai Research Centre, University of Pecs. Blood samples were collected into Vacutainer tubes containing EDTA and protease inhibitor. Galactin-3 level (Invitrogen™ Human Galectin-3 ELISA Kit, Thermo Fisher Scientific, EHLGALS3, Waltham, MA, USA), IL-1 cytokine level (Invitrogen™ Human IL-1 R4 (IL1RL1) ELISA Kit, Thermo Fisher Scientific, EHIL1RL1, Waltham, MA, USA) and IL-6 (Invitrogen™ Novex IL-6 Human ELISA Kit, Thermo Fisher Scientific, KHC00612.3.3., Waltham, MA, USA) cytokine levels were determined by the enzyme immunoassay method.
2.6. Echocardiography
Transthoracic echocardiography was performed for noninvasive evaluation of cardiac structure and function at baseline and after the 3-month-long treatment. We used a GE Vivid E9 ultrasound imaging device (GE Healthcare, Chicago, IL, USA). Structures were visualized from parasternal long axis; short axis and apical four, two and five-chamber views. M-mode (one-dimensional mode), 2D-mode, 3D-mode, PW (pulsed-wave), CW (continuous wave) and tissue Doppler mode imaging were used to determine the left ventricular ejection fraction (EF, %), the diameters (mm) and volumes (mL) of the left ventricle and left atrium, the diastolic function (E/A and E/E’), the global longitudinal strain of the left ventricle (GLS, %), the wall thicknesses of the left ventricle (mm) and the right ventricular parameters. The EF was measured by two different methods (“Simpson” and “Quinone”). The investigators were blinded to the protocol; thus, they did not know whether the patient was taking resveratrol or placebo.
2.7. Six-Minute Walk Test (6MWT)
The 6-min walk test (6MWT) is a submaximal exercise test that measures the walking distance for 6 min. The test was performed on a 30-m-long section of the corridor in our department according to the guidelines of the American Thoracic Society (ATS). The patients were at rest comfortably for 10 min prior to the test. The supervisor was a study nurse, who was blinded to the protocol. After 6 min or if the patient could not go any further, the test was stopped, and the distance, as well as the reason for stopping (dyspnea, fatigue, chest pain, etc.), were recorded [
28].
2.8. Spirometry
Spirometry is a routine method to evaluate the lung function, and it has many uses, including chest surgery or the grading of chronic obstructive pulmonary disease (COPD), etc. It is well-known that heart failure can influence the pulmonary function, which may include combined obstructive (e.g., significant FEV1 reduction) and restrictive changes [
29].
We used a PISTON PDD 301/s spirometer (Piston Ltd., Budapest, Hungary) for measuring the basic resting lung parameters of the patients at baseline and 3 months later.
During the test, the patient wore a soft nose clip to prevent air escaping through the nose, as well as a mouthpiece filter to prevent the spread of microorganisms. During the test, patients were asked to take the deepest breath they could and then exhale into the sensor as hard and as long as possible. Generally, a period of quiet breathing in and out from the sensor precedes the test, and the rapid breathing in (forced inspiratory part) comes before the forced exhalation. We determined the most common parameters in the percentage of the reference values, such as forced vital capacity (FVC); forced expiratory volume (FEV1); FEV1/FVC ratio; peak expiratory flow (PEF); forced expiratory flow 25–75% (FEF 25–75); maximal expiratory flows (MEF 25%, MEF 50% and MEF 75%) and inspiratory vital capacity (IVC).
2.9. Quality of Life Questionnaire (QoL Test)
Quality of life (QoL) in heart failure patients is severely compromised by the symptoms of the disease. Quality of life is also a good predictor of mortality and the need for hospitalization. For the assessment of QoL, we used the “Euro QoL five-dimension” (EQ-5D) questionnaire. Among health-related quality of life (HR QoL) questionnaires, EQ-5D has gained widespread use due to its simplicity to administer, score and interpret. This scoring system consists of five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression), each with three levels of response or severity (no problems—2 point, some problems—1 point or extreme problems—0 point). In addition to the index-based scoring system, the visual analog scale (VAS) component of the EQ-5D enables the patient to place their current health state on a range from 0 (worst imaginable health state) to 100 (best imaginable health state) [
30].
2.10. RNA Isolation, RNA-Seq Library Preparation and Sequencing
QIAamp RNA Blood Mini Kit was used for purification of total RNA from the whole blood. During the QIAamp procedure for purification of RNA from blood, erythrocytes are selectively lysed, and leukocytes are recovered by centrifugation. The leukocytes are then lysed using highly denaturing conditions that immediately inactivate RNases, allowing the isolation of intact RNA. After homogenization of the lysate by a brief centrifugation through a QIA shredder spin column, ethanol is added to adjust the binding conditions, and the sample is applied to the QIAamp spin column. RNA is bound to the silica membrane during a brief centrifugation step. Contaminants are washed out, and total RNA is eluted in 30 μL or more of RNase-free water.
RNA concentrations were measured using Qubit 3.0 (Invitrogen, Carlsbad, CA, USA). The RNA quality was verified on an Agilent 2100 Bioanalyzer using an RNA 6000 Nano Kit (Agilent Technologies, Santa Clara, CA, USA). High-quality (RIN > 8) RNA samples were processed for library preparation. Further sample preparation was conducted by Illumina TruSeq® Stranded Total RNA sample preparation guide.
2.11. RNA-Sequencing Data Processing and Analysis
Paired-end fastq files were imported into the CLC Genomics Workbench (CLC Bio, version 12, Hilden, Germany). Adaptor sequences and bases with low quality were trimmed. Reads containing more than 2 ambiguous bases were discarded. Preprocessed sequencing reads were aligned to the gene regions and transcripts of the GRCh38 human genome.
Differential expression of genes at the end of the study was assessed in each experimental group compared to baseline expression values while controlling cross-checking of the patient IDs of paired data. Differentially expressed genes (DEGs) were filtered out, using a threshold of fold change (FC) absolute value > 1.5 and false discovery rate (FDR)-adjusted p-value < 0.05. DEGs were visualized on a heat map using CLC Genomics Workbench 12. Hierarchical clustering was conducted, using Euclidean distances and complete linkages.
4. Discussion
Our present work firstly proved that resveratrol beneficially influences heart failure in a randomized double-blind clinical trial (RCT). The major findings of our trial are that the resveratrol treatment improved heart function, exercise tolerance, several spirometry parameters and quality of life and decreased the level of cholesterol and inflammatory cytokines in systolic heart failure patients.
It is well-established that resveratrol has various beneficial effects on the cardiovascular system. It has a marked antioxidant effect due to its scavenger capability and due to enhancing the antioxidant enzyme production (SOD, CAT and eNOS), as well as decreasing the amount of prooxidant enzymes (NOXs and MPO) [
31,
32,
33]. Therefore, resveratrol also has a marked anti-inflammatory and antiplatelet effect [
34,
35,
36]. Resveratrol also has beneficial effect on metabolic parameters; it can decrease the cholesterol level and improve the insulin resistance [
37,
38]. However, these data are derived almost completely from preclinical studies.
It was published previously by our workgroup that resveratrol in a murine post-infarct heart failure model improves the heart function and decreases myocardial fibrotic remodeling via its anti-inflammatory effect and via blocking the profibrotic intracellular signaling routes [
25]. Other workgroups showed similar results in various animal heart failure models; however, in a human clinical trial, the effect of RES has not been confirmed yet [
13,
26].
In this one-center double-blind RCT, the baseline characteristics of symptomatic systolic heart failure (HFrEF) patients were well-balanced due to the used randomization method (adaptive minimization) [
39]. Guideline-directed medical treatment (GDMT) was administered in the maximal tolerated dose, and almost every patient was given ACEI or ARB and beta-blockers, and only one-quarter of the patients was not on MRA treatments (
Table 2).
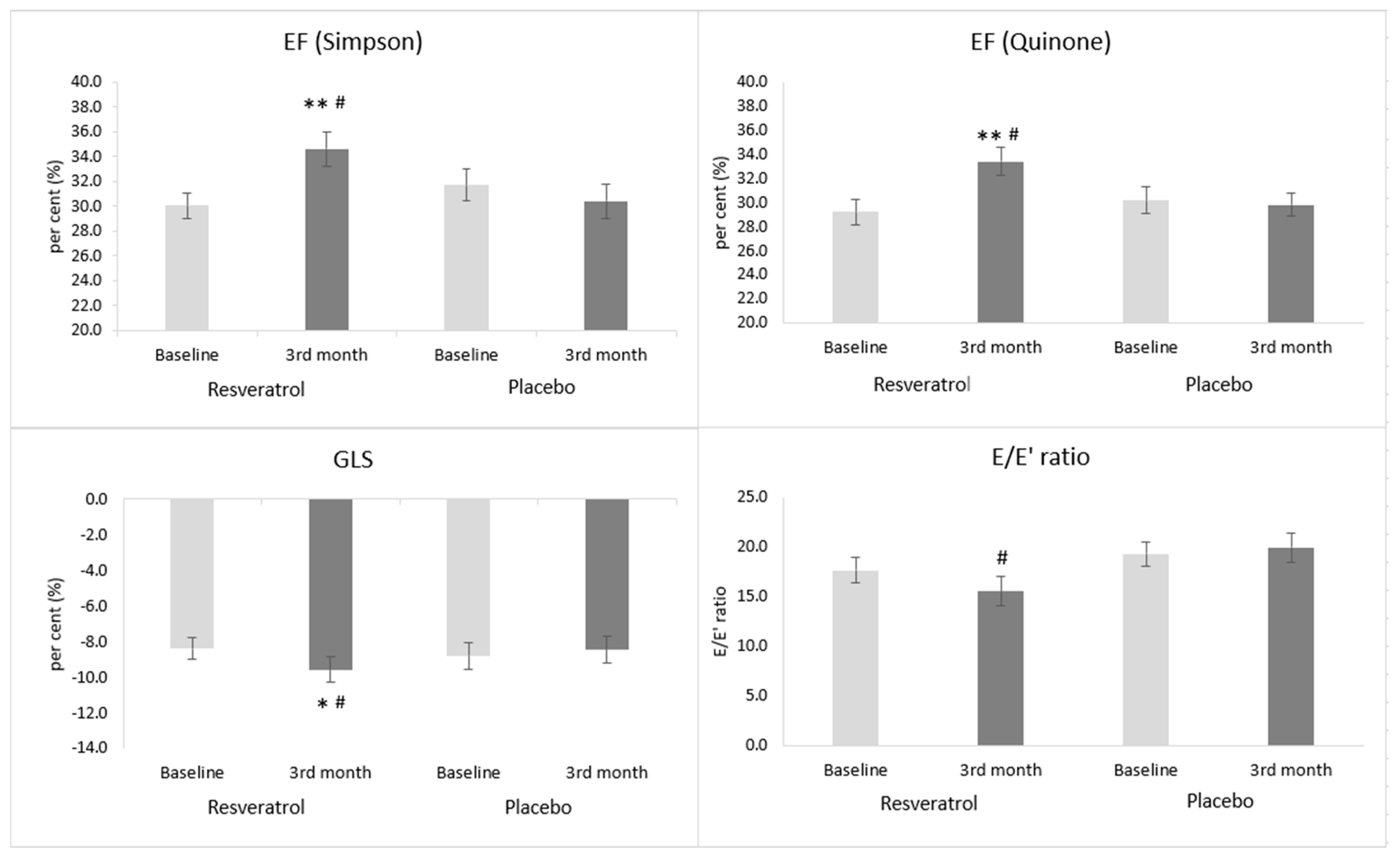
In our heart failure patients, resveratrol supplementation improved the systolic left ventricular function expressed as the ejection fraction (EF). The EF was measured in two different ways, by using the Quinones and the Simpson methods. We chose the Quinones method instead of the Teichholz’s method, because according to the literature, it is better correlation with volumetric methods [
40]. Nowadays, however, the volumetric Simpson method is by far the most commonly used method for quantifying left ventricular function. In the case of both methods, a similar increase could be seen in the resveratrol-treated group; however, in the placebo group, no change was observable.
Global longitudinal strain (GLS) is another measure of LV global function that also correlates with the extent of myocardial fibrosis in patients with HFrEF [
41]. In the placebo-treated group, the GLS value remained unchanged by the end of the treatment period. The resveratrol treatment, however, caused an improvement of the GLS value in parallel with other measures indicating systolic heart function. Moreover, GLS can show the extent of myocardial remodeling, especially myocardial fibrosis. In parallel with the improvement of systolic heart function, diastolic heart function also got better (i.e., the E/e’ ratio decreased) in the resveratrol group. In the placebo group the diastolic function was unchanged.
Natural polyphenols could improve heart function in a wide variety of experimental heart failure models [
42,
43,
44]. However, in human clinical trials, there are only a few data regarding the effect of resveratrol treatment on heart function. Our workgroup proved previously that a low-dose resveratrol treatment (10 mg/day) improved the diastolic function in patients with coronary artery disease (CAD), while, in the case of systolic LV function, only a favorable tendency was present (NS) [
45]. In another small trial also conducted in CAD patients using a higher dose (100 mg/day) of resveratrol, both the systolic and diastolic function improved.
Not only the heart function but, also, the exercise tolerance determined by the 6MWT showed significant improvement in resveratrol-treated patients by the end of the three-month-long treatment period. This result is in accordance with the preclinical results carried out in several murine models [
46]. However, there are no clinical data regarding the effect of resveratrol on the physical exercise capacity in heart failure patients yet. In an interesting trial, Voduc N. and his coworkers proved that resveratrol itself in healthy people has no positive effect on exercise capacity and on the maximal oxygen consumption (VO
2max) [
47]; moreover, Glieman L. et al. demonstrated that, in aged men, the resveratrol treatment blunted the positive cardiovascular effects of exercise and moderated the increase of VO
2max caused by the training program [
48]. Therefore, the increase of exercise capacity can be predominantly the consequence of the improvement of heart function in heart failure patients.
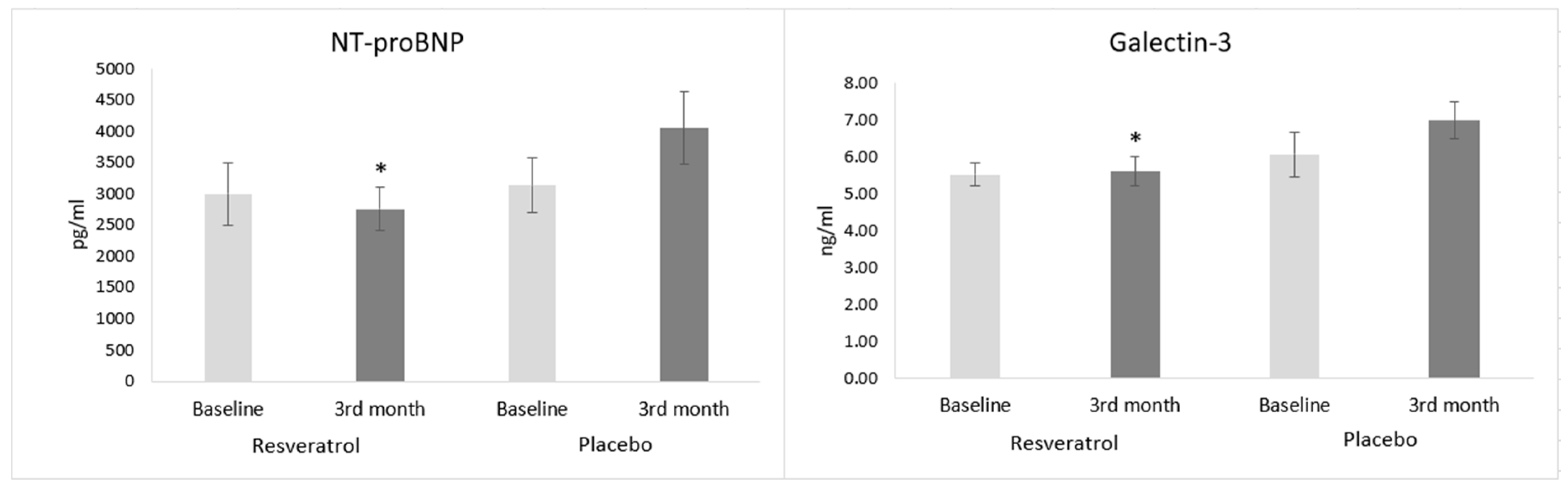
The analysis of cardiac biomarkers strengthens the findings regarding heart function and exercise tolerance. Galectin-3, which is secreted by macrophages, has been known for its significant role in mediating cardiac fibrosis and inflammation [
49]. These data were also proved in a human clinical examination [
50]. In our trial, the resveratrol treatment decreased the galectin-3 level, but in the placebo group, no change could be seen. This result supports the beneficial changes that occurred in the case of GLS, because GLS is directly proportional to the extent of interstitial fibrosis [
41].
NT-proBNP is the most widely used biomarker in the diagnosis and risk stratification of heart failure. It shows a strong correlation with the severity of heart failure, although its value can be variable due to alterations in the volume status of patients. In our trial, the resveratrol supplementation decreased the level of NT-proBNP (NS), and in the placebo group, a worsening tendency could be seen, so by the end of the treatment period, a significantly lower natriuretic peptide level was achieved in the RES group than in the placebo group. In a study conducted in stable CAD patients, Militaru and coworkers found that resveratrol decreases the NT-proBNP level even without overt heart failure [
51]. The continuously increasing level of heart failure biomarkers (NT-proBNP and galectin-3) in the placebo group can be a consequence of the progression of the disease. According to the literature, there was a linear relationship between NT-proBNP and the number of hospitalization, as well as mortality, due to heart failure [
52].
The improvement of left ventricular heart function in the resveratrol-treated group is in-line with the decreased volume retention and with the decongestion of organs. It is known that extravascular fluid accumulation in the lungs is accompanied by the alteration of several spirometry measures, e.g., forced vital capacity (FVC) and inspiratory vital capacity (IVC) [
53,
54]. Moreover, Gehlback et al. showed that, after heart transplantation, not only the ventilation volumes but the airflow velocity (FEV1) was also better [
54]. Due to resveratrol supplementation in the present trial, FVC and IVC increased significantly by the end of the treatment period. However, in the case of airway obstruction parameters, no significant changes could be seen in this study. FEV1 showed only a mild, nonsignificant improvement in the RES group.
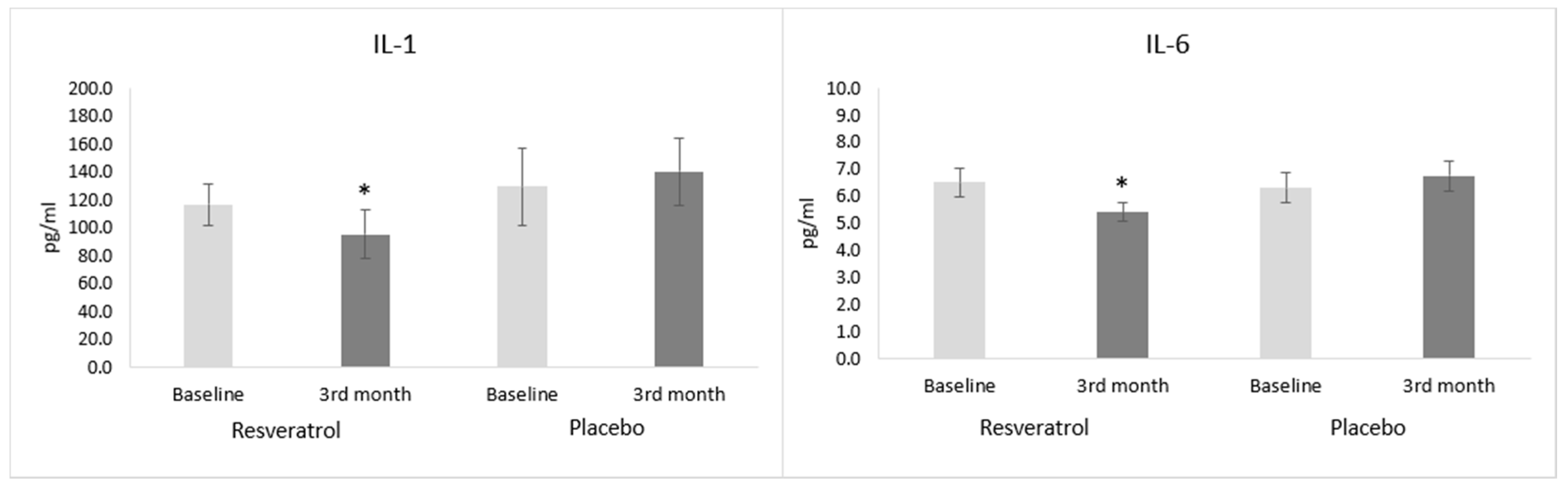
The level of inflammatory cytokines, IL-1 and IL-6 decreased in the resveratrol-treated heart failure patients compared to the placebo group. Similar results were seen in the literature [
55]. This favorable change is parallel with the level of galectin-3β that mediates inflammation. The levels of inflammatory cytokines produced by the activated leukocytes are inversely proportional to the systolic left ventricular function [
56]. The increasing level of IL-1 and IL-6 in the placebo group can be explained by the slow progression of heart failure in our enrolled population. The correlation between inflammation and adverse cardiovascular outcomes in heart failure was documented. Essentially, heart failure progression was attributed to sustained proinflammatory cytokine signaling, based on the observation that proinflammatory cytokines were elevated and continuously worsened during the progression of the disease [
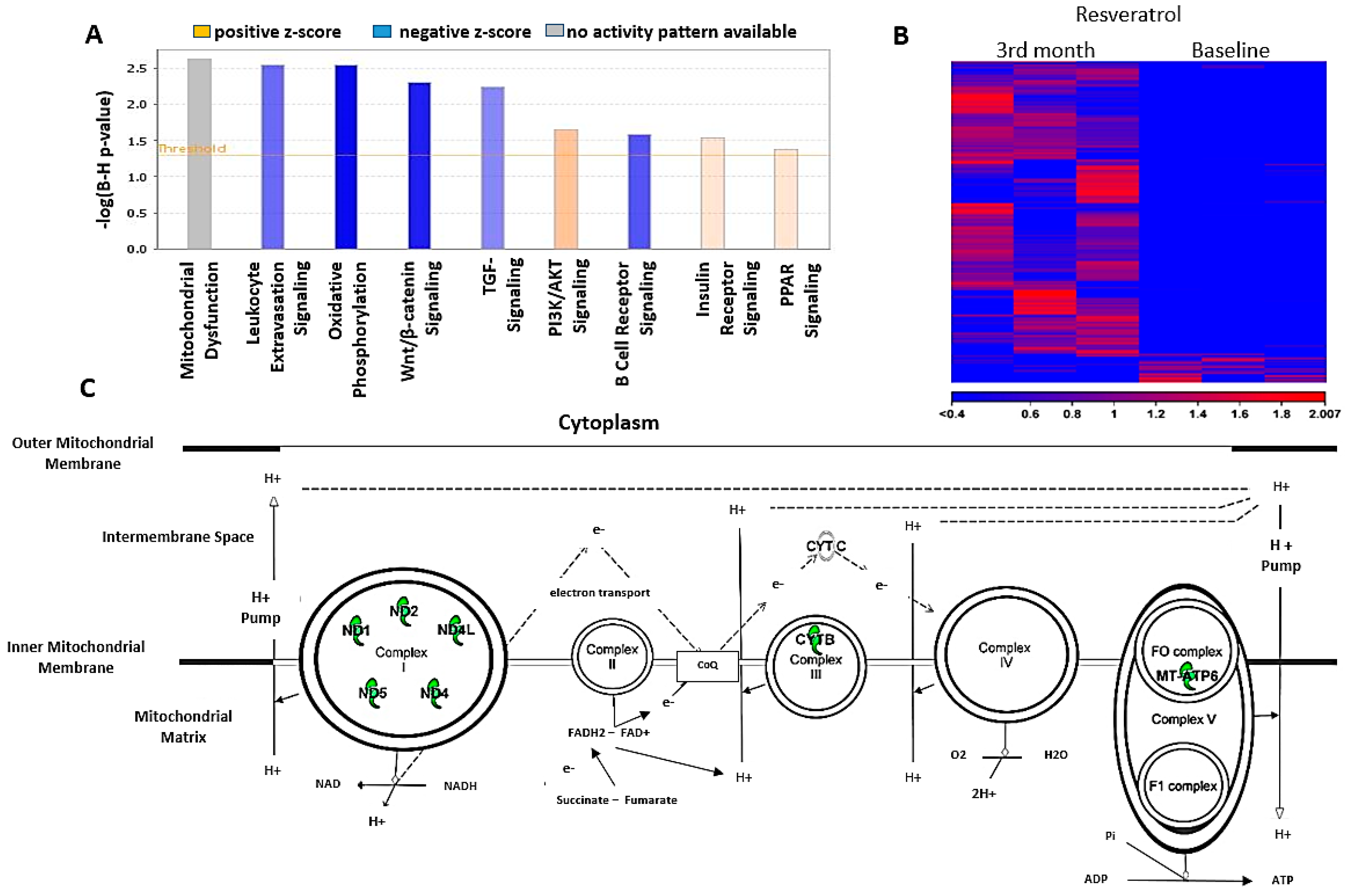
57]. Interestingly, the mRNA profile analysis of leukocytes revealed a significant decrease in genes encoding several mitochondrial respiratory proteins. Resveratrol, however, did not interfere with the expression of various proteins playing a part in the mitochondrial quality control. Moderating the production of ETC proteins in leukocytes can decrease the oxidative phosphorylation in leukocytes, which is directly proportional to their activity. The decreased production of proinflammatory cytokines in this work can be a sign of the moderated activity of leukocytes. This anti-inflammatory effect can be an important aspect of the resveratrol treatment in heart failure patients, besides its well-known mitochondrial protective effects in cardiomyocytes.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}