Aminogam® Gel Allows Faster Wound Healing after Oral Surgery by Formation of Mature Connective Tissue with Low Vascular Density and Reducing Inflammatory Infiltration. A Retrospective Study on 580 Cases with Histological and Confocal Laser Investigation

 ,
,  ,
,  ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Material and Methods
- -
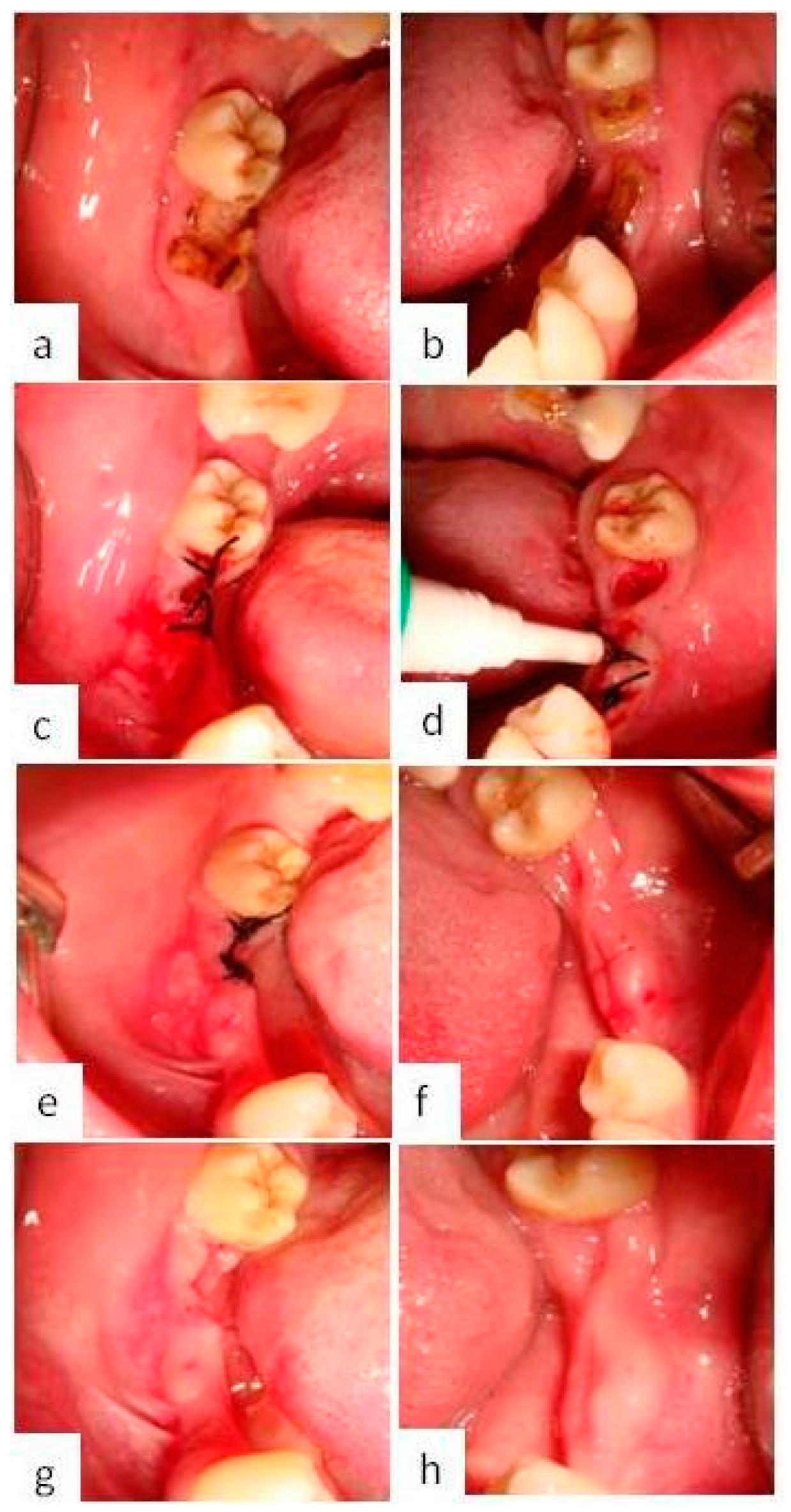
- Group A patients
- -
- Group B patients
- -
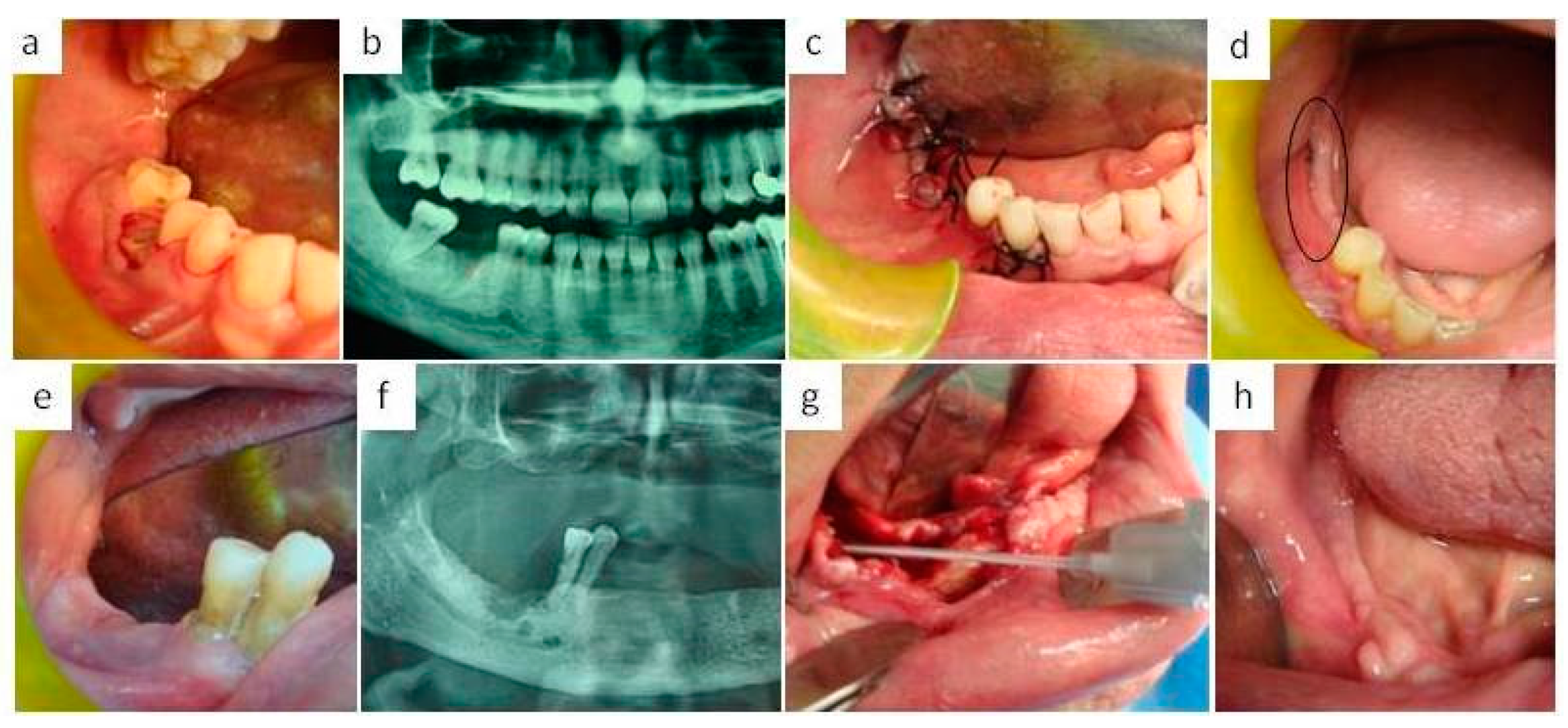
- Group C patients
- -
- Group D patients
- -
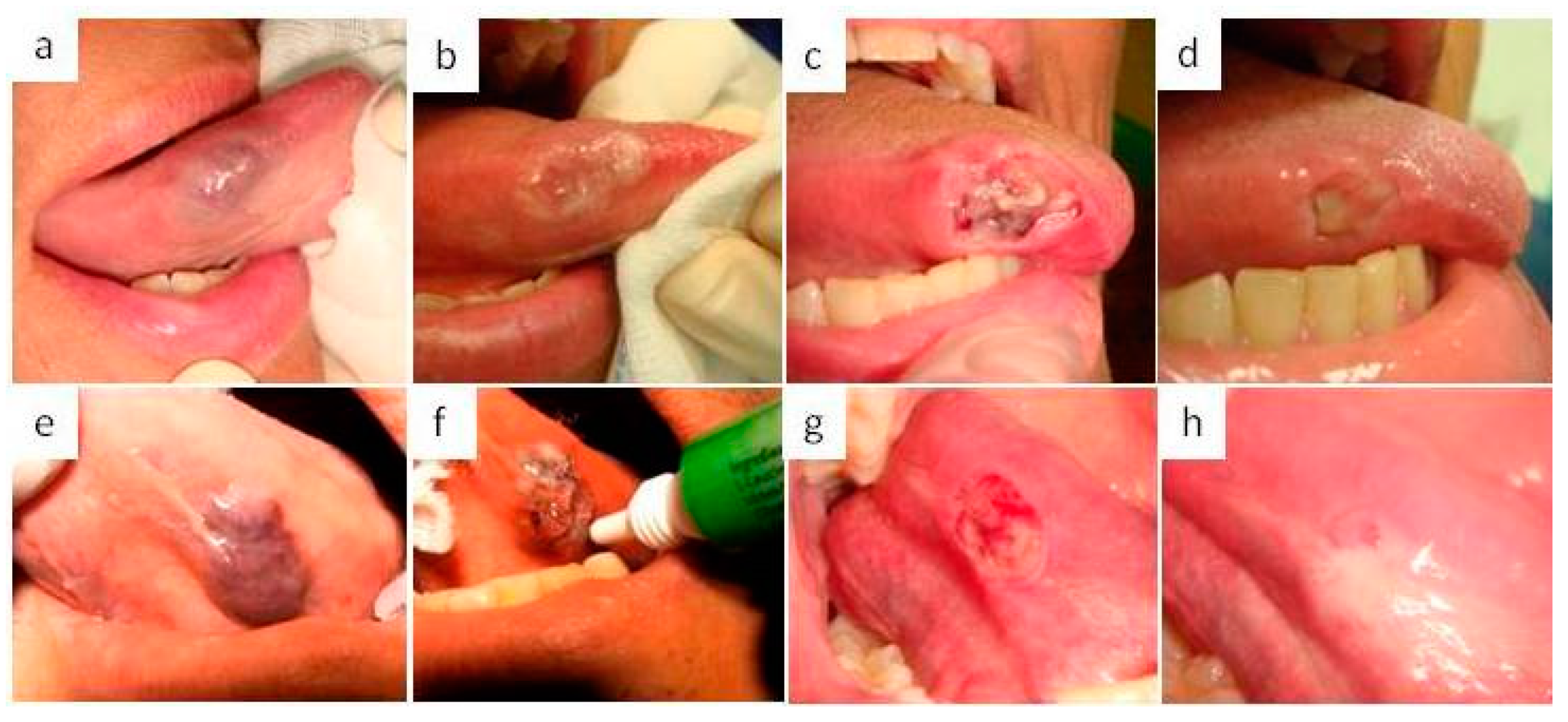
- Group E patients
- -
- Group F patients
- -
- Group G patients
- -
- Healing time evaluation after oral surgery
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Favia, G.; Mariggio, M.A.; Maiorano, F.; Cassano, A.; Capodiferro, S.; Ribatti, D. Accelerated wound healing of oral soft tissues and angiogenic effect induced by a pool of aminoacids combined to sodium hyaluronate (AMINOGAM). J. Biol. Regul. Homeost. Agents 2008, 22, 109–116. [Google Scholar] [PubMed]
- Cohn, I.K.; Diegelman, R.F.; Lindlab, W.J. (Eds.) Wound Healing: Biochemical and Clinical Aspects; WB Saunders: Philadelphia, PA, USA; London, UK, 1992. [Google Scholar]
- Brown, L.F.; Yeo, K.; Berse, B.; Yeo, T.K.; Senger, D.R.; Dvorak, H.F.; Van De Water, L. Expression of vascular permeability factor (vascular endothelial growth factor) by epidermal keratinocytes during wound healing. J. Exp. Med. 1992, 176, 1375–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stortelers, C.; Kerkhoven, R.; Moolenaar, W.H. Multiple actions of lysophosphatidic acid on fibroblasts revealed by transcriptional profiling. BMC Genom. 2008, 9, 387–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKay, D.; Miller, A. Nutritional support for wound healing. Altern. Med. Rev. 2003, 8, 359–377. [Google Scholar] [PubMed]
- Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med. 1999, 41, 738–746. [Google Scholar] [CrossRef] [PubMed]
- David-Raoudi, M.; Tranchepain, F.; Deschrevel, B.; Vincent, J.C.; Bogdanowicz, P.; Boumediene, K.; Pujol, J.P. Differential effects of hyaluronan and its fragments on fibroblasts: Relation to wound healing. Wound Repair Regen. 2008, 41, 274–287. [Google Scholar] [CrossRef] [PubMed]
- Dechert, T.A.; Ducale, A.E.; Ward, S.I.; Yager, D.R. Hyaluronan in human acute and chronic dermal wounds. Wound Repair Regen. 2006, 14, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Abatangelo, G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999, 7, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Fuhrman, M.P. Nutrients and wound healing: Still searching for the magic bullet. Nutr. Clin. Pract. 2005, 20, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Mariggiò, M.A.; Cassano, A.; Vinella, A.; Vincenti, A.; Fumarulo, R.; Lo Muzio, L.; Maiorano, E.; Ribatti, D.; Favia, G. Enhancement of fibroblast proliferation, collagen biosynthesis and production of growth factors as a result of combining sodium hyaluronate and aminoacids. Int. J. Immunopathol. Pharmacol. 2009, 22, 485–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, S.; Miccoli, S.; Limongelli, L.; Tempesta, A.; Favia, G.; Maiorano, E.; Favia, G. New Dimensional Staging of Bisphosphonate-Related Osteonecrosis of the Jaw Allowing a Guided Surgical Treatment Protocol: Long-Term Follow-Up of 266 Lesions in Neoplastic and Osteoporotic Patients from the University of Bari. Int. J. Dent. 2014, 2014, 935657. [Google Scholar] [CrossRef] [Green Version]
- Koray, M.; Ofluoglu, D.; Onal, E.A.; Ozgul, M.; Ersev, H.; Yaltirik, M.; Tanyeri, H. Efficacy of hyaluronic acid spray on swelling, pain, and trismus after surgical extraction of impacted mandibular third molars. Int. J. Oral Maxillofac. Surg. 2014, 43, 1399–1403. [Google Scholar] [CrossRef]
- Voinchet, V.; Vasseur, P.; Kern, J. Efficacy and safety of hyaluronic acid in the management of acute wounds. Am. J. Dermatol. 2006, 7, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Barbul, A. Proline precursors to sustain mammalian collagen synthesis. J. Nutr. 2008, 138, 2021–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEwan, P.A.; Scott, P.G.; Bishop, P.N.; Bella, J. Structural correlations in the family of small leucine-rich repeat Proteins and proteogiycans. J. Struct. Biol. 2006, 155, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Romeo, U.; Libotte, F.; Palaia, G.; Galanakis, A.; Gaimari, G.; Tenore, G.; Del Vecchio, A.; Polimeni, A. Oral soft tissue wound healing after laser surgery with or without a pool of amino acids and sodium hyaluronate: A randomized clinical study. Photomed. Laser Surg. 2014, 32, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Colella, G.; Cannavale, R.; Vicidomini, A.; Rinaldi, G.; Compilato, D.; Campisi, G. Efficacy of a spray compound containing a pool of collagen precursor synthetic aminoacids (l-proline, l-leucine, l-lysine and glycine) combined with sodium hyaluronate to manage chemo/radiotherapy-induced oral mucositis: Preliminary data of an open trial. Int. J. Immunopathol. Pharmacol. 2010, 23, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Cheng, Y.Y.; Koo, P.L.; Lee, K.M.; Qin, L.; Cheng, J.C.; Kumta, S.M. The effect of hyaluronan on osteoblast proliferation and differentiation in rat calvarial-derived cell cultures. J. Biomed. Mater. Res. A 2003, 66, 880–884. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | HT (Means ± SD) | p Value | |
|---|---|---|---|
| GROUP A: 120 teeth extractions (only inferior molars) | |||
| CASE | 60 | 10.10 ± 0.75 | |
| 60 | <0.001 | ||
| CONTROL | 14.20 ± 1.04 | ||
| GROUP B: 60 teeth extractions in patients taking BPs | |||
| CASE | 30 | 9.60 ± 1.38 | |
| <0.001 | |||
| CONTROL | 30 | 14.67 ± 0.48 | |
| GROUP C: 100 MRONJs with surgical resection of the necrotic bone | |||
| CASE | 50 | 17.90 ± 1.31 | |
| <0.001 | |||
| CONTROL | 50 | 25.30 ± 0.46 | |
| GROUP D: 80 endosseous implants | |||
| CASE | 40 | 6.93 ± 0.73 | |
| <0.001 | |||
| CONTROL | 40 | 10.58 ± 1.06 | |
| GROUP E: 140 diode laser excisions | |||
| CASE | 70 | 14.14 ± 1.00 | |
| <0.001 | |||
| CONTROL | 70 | 21.21 ± 1.43 | |
| GROUP F: 40 diode laser photocoagulations | |||
| CASE | 20 | 11.95 ± 0.69 | |
| <0.001 | |||
| CONTROL | 20 | 16.30±0.86 | |
| GROUP G: 40 bone surgery | |||
| CASE | 20 | 16.60 ± 1.05 | |
| <0.001 | |||
| CONTROL | 20 | 23.05 ± 0.76 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capodiferro, S.; Tempesta, A.; Bucci, S.; Maiorano, E.; Favia, G.; Limongelli, L. Aminogam® Gel Allows Faster Wound Healing after Oral Surgery by Formation of Mature Connective Tissue with Low Vascular Density and Reducing Inflammatory Infiltration. A Retrospective Study on 580 Cases with Histological and Confocal Laser Investigation. Appl. Sci. 2020, 10, 1105. https://0-doi-org.brum.beds.ac.uk/10.3390/app10031105
Capodiferro S, Tempesta A, Bucci S, Maiorano E, Favia G, Limongelli L. Aminogam® Gel Allows Faster Wound Healing after Oral Surgery by Formation of Mature Connective Tissue with Low Vascular Density and Reducing Inflammatory Infiltration. A Retrospective Study on 580 Cases with Histological and Confocal Laser Investigation. Applied Sciences. 2020; 10(3):1105. https://0-doi-org.brum.beds.ac.uk/10.3390/app10031105
Chicago/Turabian StyleCapodiferro, Saverio, Angela Tempesta, Sabina Bucci, Eugenio Maiorano, Gianfranco Favia, and Luisa Limongelli. 2020. "Aminogam® Gel Allows Faster Wound Healing after Oral Surgery by Formation of Mature Connective Tissue with Low Vascular Density and Reducing Inflammatory Infiltration. A Retrospective Study on 580 Cases with Histological and Confocal Laser Investigation" Applied Sciences 10, no. 3: 1105. https://0-doi-org.brum.beds.ac.uk/10.3390/app10031105