1. Introduction
The age of a living subject can be determined by applying a number of different methods. The most utilized are skeletal and dental methods, most of which are based on X-rays examinations. According to the clinically estimated age of the subject, a particular set of methods is selected. Some methods could be employed only when evaluating a restricted age span, while other methods have a different degree of precision according to the different age of the analyzed subject. Furthermore, each method is characterized by a different degree of accuracy, i.e., the difference between estimated dental age (DA) and chronological age (CA), reliability, which is defined as its ability to produce stable and consistent results when the same subject is evaluated by different evaluators, and invasiveness. For these reasons, sometime different methods are normally combined, in order to obtain a more accurate age estimation.
Age estimation is a relevant issue in different public health situations, especially when dealing with young subjects because of the important consequences at the juridical level related with different particular turning-point age, which could vary according to different national legislations. For example, in the recent years, refugee, asylum seeker, and migrant flow towards the Mediterranean Sea and Eastern European countries increased the need for a standardized, reliable and sustainable—in terms of time, instrumentations needed, and costs—method for age estimation over or under the limit of 18 years. Being an adult entails important implication in determining the administrative procedures to be followed, in particular with economic migrants. Another common issue is related with young criminals, who could not be considered imputable or could go to a juvenile instead of an adult detention center, according to their particular age and depending on the legislation of the country where the crime is perpetrated [
1].
Dental age estimation methods utilized with young subjects are fundamentally based on the analysis of teeth anatomy, evaluated by means of pre-defined stages or with special algorithms specifically ideated for this aim. Teeth maturation is frequently studied using panoramic X-rays that allow the simultaneous visualization of all teeth, despite not erupted yet, with their respective roots, if already formed. One limitation of this radiologic technique is the image deformation that occurs when a tooth is malpositioned, leading sometimes to some incertitude in the developmental stage definition or even to the impossibility to evaluate it.
Cone Beam Computed Tomography (CBCT) is a three-dimensional (3D) radiological technique recently introduced in dentistry for the study of the maxillofacial region for surgical and orthodontic reasons, especially in cases when two-dimensional (2D) radiological techniques are not able to provide enough information in order to establish a correct diagnosis. CBCT employs a reduced dose of radiations compared to the traditional Multi Slice Computed Tomography (MSCT), but higher if compared to classic 2D exams. Consequently, a careful clinical exam and a well-pondered risk-benefit assessment are necessary before opting for this kind of 3D radiological imaging [
2,
3,
4].
The aim of this systematic review was to compare the accuracy and reliability of CBCT vs. Panoramic radiography in age determination, considering also ethical aspects.
2. Materials and Methods
This systematic review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [
5] and CRD (Centre for Reviews and Dissemination, University of York) statements.
A computerized systematic literature search of studies published up to January 2020 was conducted without language restrictions in the following electronic databases: Scopus, ISI Web of Knowledge, and Medline (via PubMed). The strategies illustrated in
Table 1,
Table 2 and
Table 3 were used.
A hand search for additional articles was then thoroughly performed in the authors’ personal libraries and in the references lists of all previously selected articles.
A limited gray literature search was finally conducted through the websites of more important and pertinent international dental congresses held during the last five years. When posters and oral communications, which were presented at those congresses, were not followed by a full manuscript publication, authors were contacted by e-mail in order to obtain pertinent missing data, if necessary.
Inclusion criteria were: articles comparing CBCT vs. panoramic radiography in dental anatomy evaluation; articles evaluating the accuracy of dental methods for age estimation, both with CT and panoramic radiography exams; articles comparing CBCT vs. panoramic radiography in terms of radiation dose. Exclusion criteria were: study protocols; case reports; author debates; review articles.
Study selection was independently performed by two of the authors and, in case of disagreement, a discussion with a third senior author was conducted in order to obtain a consensus between the two. Pertinent information that answered the research questions was independently extracted from the selected articles by the same two investigators and a customized data extraction form was filled out including the following items: first author’ name and year of publication, study design, origin of studied population, argument (comparison between CBCT and orthopantomography (OPG) in terms of dental anatomy evaluation, radiation dose, and accuracy of dental methods for age estimation), and main results of the study.
The same two authors who selected the studies, applying the appropriate scale based on the different type of study to be evaluated, independently assessed the quality of the selected articles. In case of disagreement, a consensus was again reached after discussion with a third expert author.
3. Results
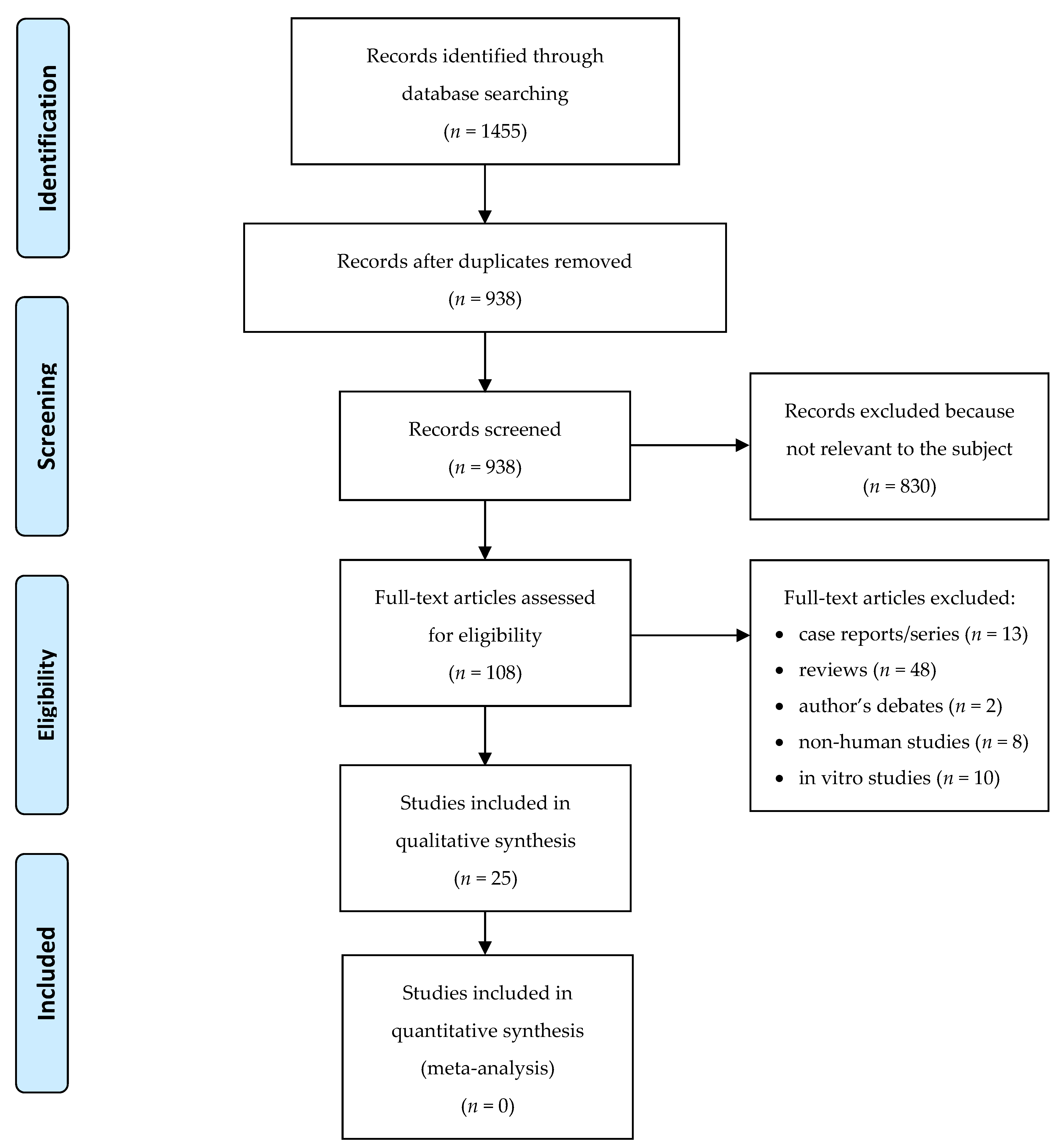
The article selection process is illustrated through the PRISMA flow diagram presented in the
Figure 1.
The electronic databases search yielded 1455 articles. After overlapping data among the databases identification and duplicates removal, 938 papers were screened. After titles and abstracts screening, 108 articles were selected for full-article review. A total of 43 articles met the inclusion criteria and, after application of exclusion criteria, 25 were selected for analysis. Ten articles compared CBCT vs. OPG in dental anatomy evaluation, five articles evaluated the accuracy of dental methods for age estimation, both with CT and OPG exams, and the remining 10 compared CBCT vs. OPG in terms of radiation dose.
CBCT was found to be more accurate than OPG in dental anatomy evaluation, because of the absence of distortion and superimpositions of different structures. Several dental methods were used for age evaluation, each one with a different degree of reliability depending also on the age to be evaluated. When analyzing young adults, an estimation error of two years is considered forensically acceptable. The radiologic dose of a CBCT exam is higher compared to an OPG exam; with small Field Of View (FOV) and low-resolution protocols, the difference is not so marked.
Data extracted from more significant manuscripts are summarized in
Table 4,
Table 5 and
Table 6 [
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28].
A simplified version of the NIH (National Institutes of Health) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [
29] was adopted to evaluate the risk of bias and the methodological quality of the included papers, because they presented the results of cross-sectional studies. When it was not possible to evaluate one of the questionnaire items due to lack of information into the manuscript, a “Cannot Determine” (CD) judgement was reported for that specific item. Quality of studies scoring more than five out of eight “Yes” was considered “Good,” quality of studies which ranged from three to five “Yes” was considered “Fair,” and quality of studies with less than three “Yes” was considered “Poor.”
Following these criteria, one of the studies regarding dental anatomy evaluation was rated as “Poor” and the remaining nine were rated as “Fair” (
Table 7), while all five studies regarding the accuracy of dental methods for age estimation (
Table 8) and all 10 studies regarding radiation dose evaluation (
Table 9) were rated as “Fair.”
4. Discussion
CBCT use in dentistry was introduced more than 15 years ago, and since then, it has spread exponentially from big hospitals and clinics to small private practices, also thanks to the introduction into the market of small size sensors that helped, together with an increased diffusion of this technology, to make the economic cost of a scanner more affordable.
The possibility for the clinician to see orthogonal sections of a Region Of Interest (ROI) in virtually all the desired directions is an obvious advantage for the diagnosis. This could be really useful not only in implantology, when bone thickness and height must be exactly measured before placing a dental implant, or in oral surgery, when the proximity of sensible structures to the area of the intervention must be carefully evaluated, but also in other dental fields such as orthodontics, periodontology, restorative dentistry, endodontics, and gnathology [
30,
31,
32,
33,
34].
CBCT images quality is mainly influenced by their resolution, the presence of noise, and the presence of artefacts. These, in turn, are controlled by equipment parameters such as Field Of View (FOV) dimension, milliamperage seconds (mAs), peak tube voltage (KVp), reconstruction algorithm, scanning time, frame rate, speed of sensor rotation, arc of sensor trajectory, and type of detector.
In the last two decades, various types of detectors have been developed: image intensifiers coupled to a charge-coupled device (CCD), amorphous silicon (α-Si) flat panels (FP), and complementary metal-oxide semiconductor (CMOS) FP. Amorphous silicon and CMOS flat panels are used in many of the CBCT machines available today. CMOS has several useful characteristics: it requires low power to operate, has high-speed readout, is capable of on-chip integration of electronic circuitry, and produces digital signals without external converters. Compared with α-Si flat panels, it has the advantage of a smaller pixel size, resulting in higher resolution, and it does not suffer from image lag, a residual charge left behind in the sensor that degrades overall image quality. A disadvantage of CMOS flat panel sensors is the size of the active detection area, which makes it difficult to produce a single CMOS chip in a large size, unlike α-Si flat panels: a common technique to overcome this issue is tiling multiple CMOS chips to form a larger mosaic [
35,
36].
Several studies focused on the comparison between CBCT and OPG, and also between CBCT and MSCT, in the diagnostic process of a wide range of different pathologies [
37,
38].
From a therapeutic point of view, the recent digitalization of dental lab procedures, coupled with the guided surgical protocol based on the patient bones 3D reconstruction obtained from CBCT images, gave the last push to the diffusion of this radiologic technology also in small practices. Small practices are finally able to “close the circle,” exploiting the availability of in-office Computer Aided Design—Computer Aided Manufacturing (CAD-CAM) systems conceived for delivering chair-side restorations to the dental patient [
39].
The MSCT scanners would also make this theoretically possible, but because of the anisotropic nature of their voxel, the accuracy of the re-formatted bone reconstructions was not as reliable as with the isotropic voxel that characterize CBCT scanners. Furthermore, the higher X-rays dose administered to the patient by MSCT compared to CBCT scanners limited the utilization of this technique only to more severe cases; the biological cost-benefit ratio was in favor of this more invasive radiologic technique. The over-prescription of MSCT would contrast the public health mission to protect population health avoiding unjustified radiologic exposures, and would lead to inappropriate expenses.
Loubele et al. [
40] compared the effective dose levels, according to the ICRP 103 (2007) guidelines, of three CBCT scanners for maxillofacial applications with those of three MSCT scanners. They measured values ranging from 13 to 82 μSv for CBCT and from 474 to 1160 μSv for MSCT. Despite dose levels for CBCT imaging remained far below those of clinical MSCT protocols, they concluded recommending that—considering the wide dose span even using the same type of scanner—it is of outmost importance to buy the appropriate equipment needed for a specific practice, to justify the selection of each of these imaging protocols, and to optimize the radiation dose while achieving a sufficient image quality.
Horner et al. [
41], combining a literature review with the expert opinion of senior members of the European Academy of Dento-maxillo-facial radiology (EADMFR) and of the Dental X-ray Protection Services of the UK Health Protection Agency (HPA), tried to give specific indications regarding remedial and suspension levels in different dental CBCT equipment. The analysis of these two values is useful when selecting the CBCT scanner to be installed in a specific dental primary care facility. Remedial levels, i.e., when the margin of deviation from the standard requires action to rectify it, were available for operating potential accuracy and precision, tube output consistency, Half-value layer (HVL), and Hounsfield value (CT number) uniformity. Suspension levels, i.e., when the margin of deviation from the standard is substantial and equipment are no longer fit to use, were available for image noise, image density values, computed tomography dose index (CTDI) free in air, radiation field size, radiation output repeatability and reproducibility, operating potential, and Dose-Area-Product (DAP). Due to the limited information available, at that time, from large-scale audits of equipment in clinical use, and taking into account the continuing developments in equipment, they took a pragmatic approach and concluded that suspension levels for dental CBCT should be continuously kept under review in the light of growing experience of testing equipment in practice. Furthermore, they pointed out the importance of periodical revision of acceptability criteria for dental CBCT also because of its usual location in primary care facilities, where quality assurance and maintenance of equipment may not be optimal.
Recently, Erdelyi and Duma [
42] discussed the patient’s risk in dental radiography presenting their experience in dose optimization when exposing dental patients to intraoral, panoramic, and CBCT X-rays. They concluded that if a proper optimization of the instruments’ settings and of the patient’s positioning are made, it is possible to stay in a reasonable range of radiological exposure ensuring at the same time a good resolution of the acquired images.
Focusing on forensic medicine, it is possible to notice that since 10 years ago, CBCT was used with different purposes, such as, for example, in forensic identification through facial soft tissues thickness measurement and craniofacial reconstruction, and frontal sinus, mandibular lingual canals or teeth superimposition; for bite marks analysis; for sex determination identifying a possible dimorphism of the mandibular body, the foramen magnum, and the maxillary of frontal sinus; and of course for age estimation [
43,
44,
45,
46,
47,
48,
49,
50,
51,
52,
53,
54].
Age estimation through CBCT images focused on different craniofacial structures: cervical vertebrae shape; spheno-occipital synchondrosis ossification; mandibular condyle cortication; structural changes of teeth and buccal alveolar bone level; pulp–tooth volume ratio; and dental maturation.
Rhee et al. [
55] used cervical vertebrae shape analysis to build bone and forensic age estimation regression models and they found that there was no significant difference between form space and shape space in both age estimation models even if, for gender comparison, this two age estimation models had a higher explanatory power for males. In their study, the narrowest prediction intervals among the multivariate regression models were 19.63 for bone age and 2.99 for forensic age: the latter interval gives an idea of the incertitude of a forensic age estimation elaborated through this method. Sinanoglu et al. [
56] focused on the analysis of spheno-occipital synchondrosis, and they found that the mean ages for its complete fusion were 18 and 20 years of age for females and males, respectively, with an interobserver agreement ranging between substantial and perfect and an intraobserver substantial agreement. Therefore, they concluded that the spheno-occipital synchondrosis ossification stage evaluation has a value for age estimation around the age of 18 years. Bayrak et al. [
57] investigated the effectiveness of using the condylar cortication as a new method of age estimation, and they found three different stages around 14.14 ± 2.3 years, 16.11 ± 3.18 years, and 19.39 ± 3.96 years for males, approximately one year less for females, that are all important age turning points from a public system perspective. It must be considered they also found that the type of cortication in the right and left condyle might be different for the same individual. All these methods are based on maxillofacial structures that are easily visualized with a CBCT, but compared to dental methods, they normally require a bigger FOV and they are also closer, especially in young subjects, to radiologic sensible developing structures: they should then be considered as secondary exams in the case of wide incertitude when utilizing a dental method for age estimation.
Koh et al. [
58] focused on the structural changes of teeth and buccal alveolar bone level described by Gustafson [
59]; namely, attrition, secondary dentine formation, and periodontal recession, which occur progressively during the aging process, and therefore, are less useful compared with other methods when analyzing young subjects. This is also partially true for studies focusing on pulp–tooth volume ratio evaluation. Pinchi et al. [
60], for example, found that their original method, based on the geometric approximation of the different parts of the tooth (the root and the pulp were assimilated to elliptical based cones and the crown to an elliptical based truncated cone), showed the highest accuracy in age prediction for the age cohorts between 30 to 59 years, while for other age cohorts, the estimation error was similar to what was reported by applying other dental methods. Asif et al. [
61] found that the volumetric analysis of the pulp chamber/crown ratio (up to cemento-enamel junction) is a valuable gender-independent technique for age evaluation, and it is quicker and equally reliable compared to the analysis of pulp cavity/tooth ratio. Gulsahi et al. [
62] confirmed the ratio of pulp volume to tooth volume is not gender-dependent, and they also found that it is more reliable when measured on maxillary central incisors than on other teeth. Of course, in all these studies, teeth with caries, filling or crown restorations, periapical pathologies or pulps that could not be identified were excluded, because they interfere with the physiological processes normally occurring in healthy teeth. Dealing with dental maturation evaluation, Cantekin et al. [
63] found that third molar evaluation on CT images is clinically useful for the accurate and reliable estimation of dental ages of children and youth. Findings by Bassed et al. [
64] confirmed these results. Furthermore, they also compared the CT images to conventional radiographs to assess the developmental scoring agreement between the two and they found that the agreement of Demirjian [
65] scores between the two imaging modalities was excellent and that the third molar is not a precise tool for age estimation in the ranges of 3–8 years; however, it is a useful tool for discriminating the adult/child transition age of 18 years. Opposite results were obtained by Marroquin Penaloza et al. [
66] after applying the Kvaal [
67] method, based on pulp and root width measurement, to bucco-lingual and mesio-distal CBCT sections of a tooth. They found that it was outside an acceptable range for forensic application (±10.00 years), and that it was also more time consuming than the original approach based on dental radiographs [
68,
69,
70,
71,
72,
73,
74,
75,
76,
77,
78,
79,
80,
81,
82,
83,
84,
85].
A final consideration must be made taking into account opinions that do not support the radiological age estimation methods due to radiation exposure, even if the ALARA (As Low As Reasonably Achievable) or ALADA (As Low As Diagnostically Acceptable) radioprotection principles are followed [
86].
Any radiological exposure is free from stochastic effects, such as, for example, cancer induction and radiation-induced hereditary effects, which occur by chance. Nevertheless, in some situations—as discussed above—the benefit of obtaining a more precise age estimation overweight this kind of risk, which must be individually evaluated, case by case, following general rules and guidelines.
Theoretically, a 2D method should be preferred and a 3D method should be used only in difficult or uncertain cases, due to anatomical or tooth morphological reasons. Unfortunately, this approach involves the administration of two exams, with a cumulative effect of dose exposure. Considering that nowadays several CBCT scanners implemented ultra-low dose protocols and small size FOV able to expose the patient to an effective dose compared to a digital OPG, the use of 3D radiological images only as a second step exam should be carefully evaluated [
87,
88,
89,
90,
91].

 ,
, 


{kind=link}