Application of a Prediction Model for Ambient Noise Levels and Acoustical Capacity for Living Rooms in Nursing Homes Hosting Older People with Dementia

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Theoretical Background
3. Methods
4. Results
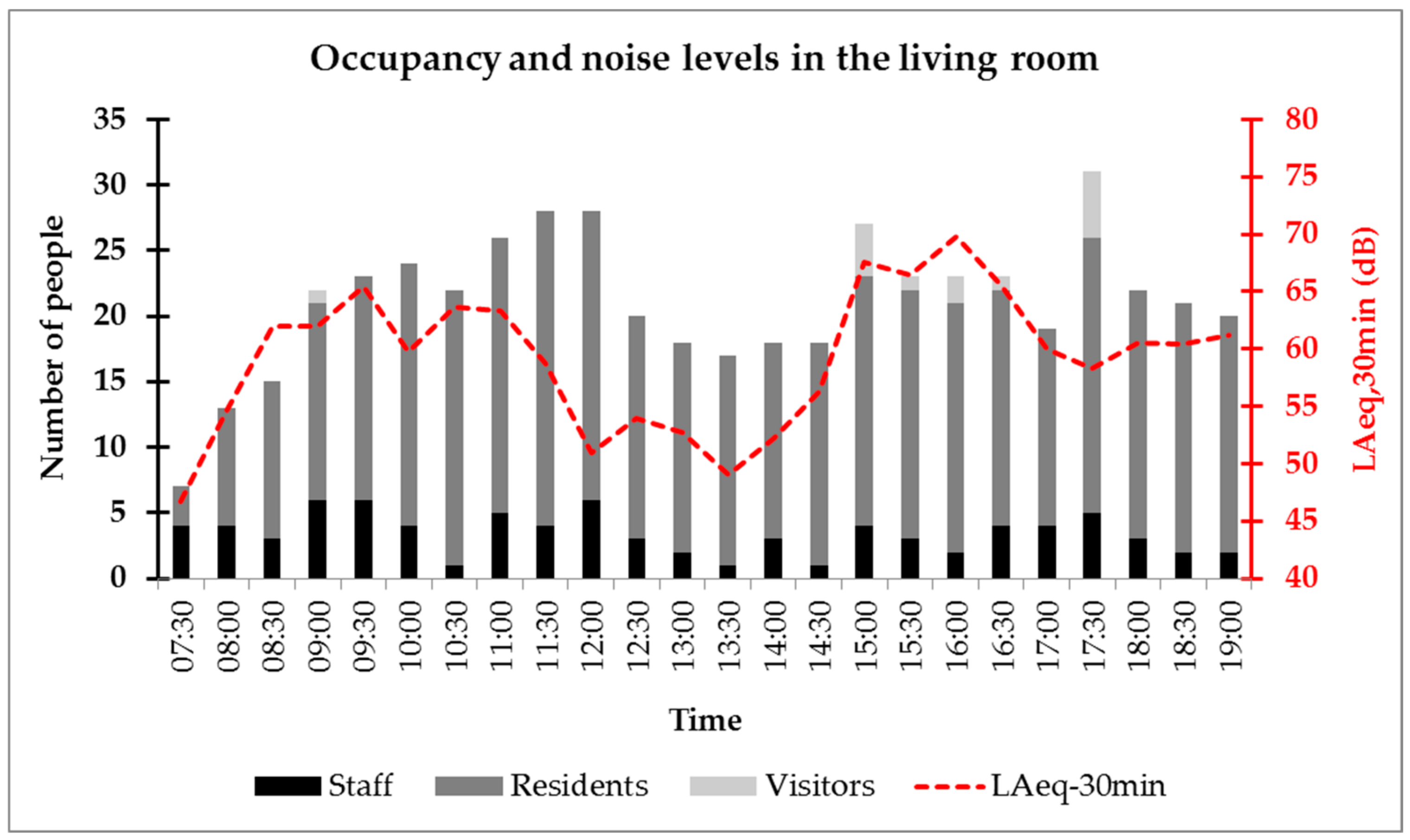
4.1. Acoustic and Occupancy Data in the NH Living Room
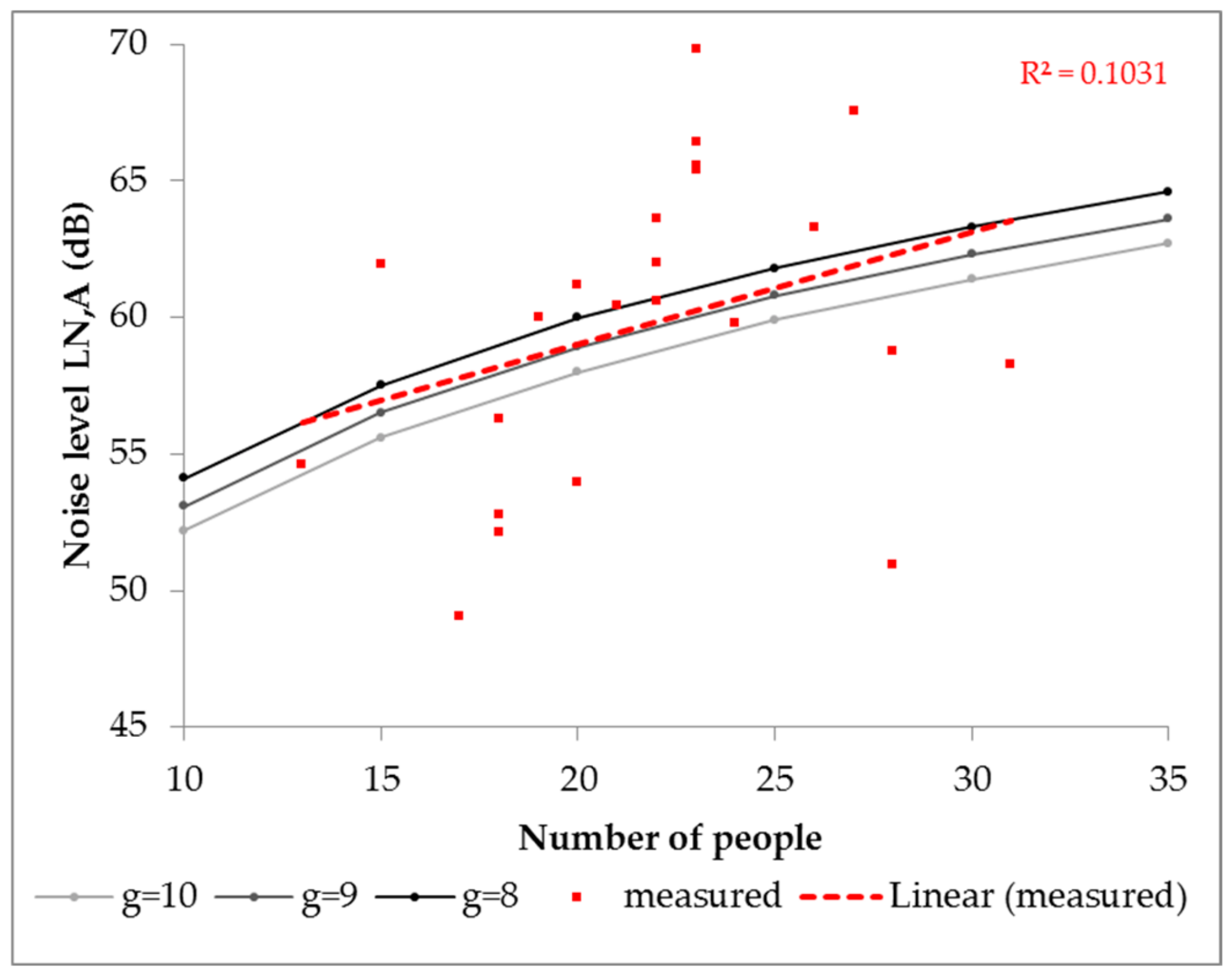
4.2. Optimization of the g Value for Prediction of Ambient Noise Levels
4.3. Acoustical Capacity Pre- and Post-Intervention
5. Discussion
6. Conclusions
- In the living room of a nursing home hosting people with BPSD, the prediction model gave the best results with a set of parameters that deviates considerably from those proposed for other eating establishments; namely, c = 0.5 dB/dB, Ap = 0.2 m2 and g = 9;
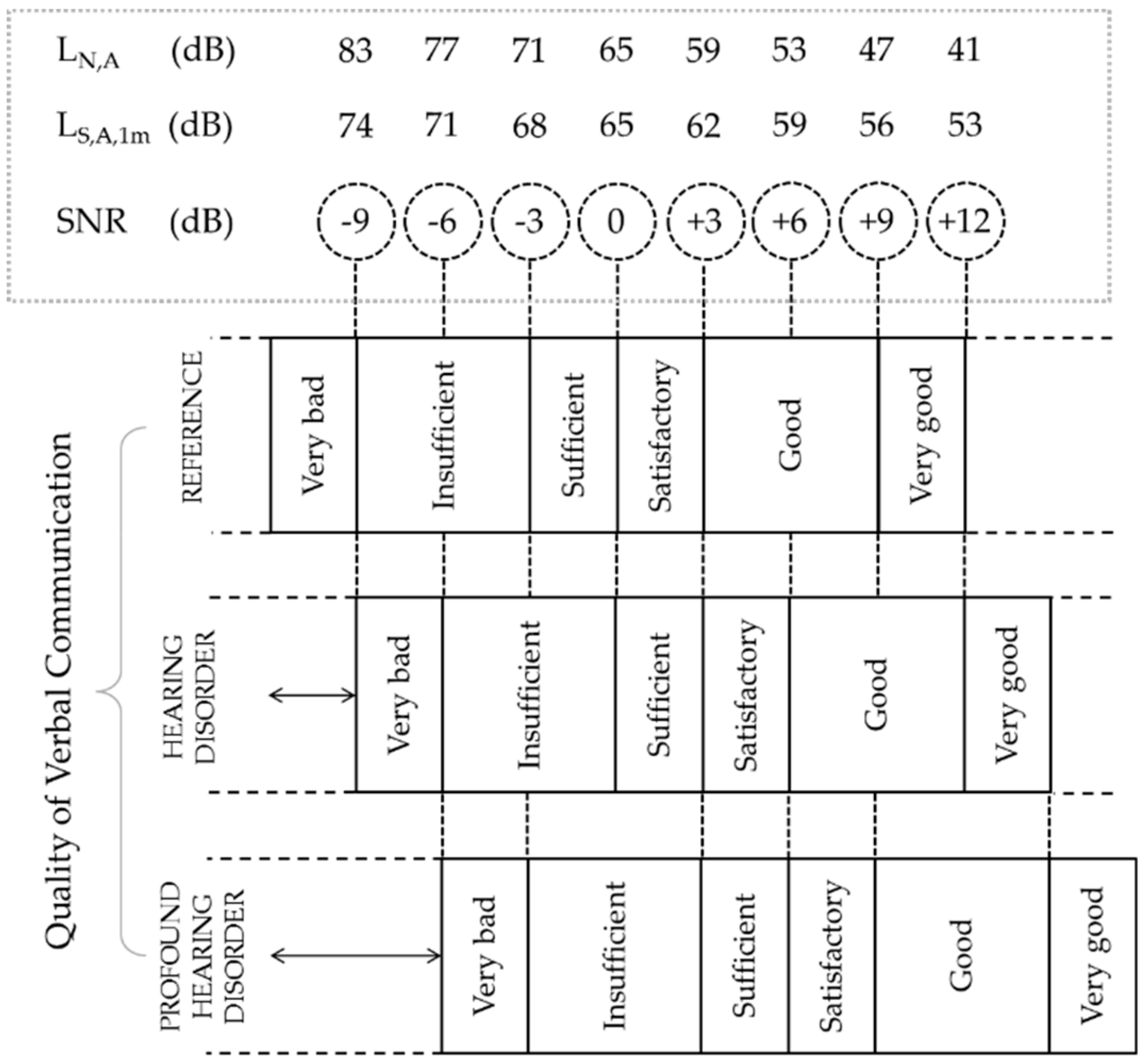
- The admissible ambient noise level used as reference in determining the threshold for sufficient quality of verbal communication had to be adjusted to LN,A = 59 dB to return realistic values of acoustical capacity for the living room;
- The acoustical retrofit intervention implemented in the living room of the AcustiCare case study increased the acoustical capacity of the space by 27 people, leading to a much lower occupancy saturation ratio under normal functioning conditions and an improved quality of verbal communication from “insufficient” to “satisfactory”.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van den Bosch, K.A. Safe and Sound: Soundscape Research in Special Needs Care; University of Groningen: Groningen, The Netherlands, 2015. [Google Scholar]
- Brown, J.; Fawzi, W.; Shah, A.; Joyce, M.; Holt, G.; McCarthy, C.; Solomon-Ayeh, K. Low stimulus environments: Reducing noise levels in continuing care. BMJ Open Qual. 2016, 5, u207447. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Zeng, Y.; Zhao, L.; Zeng, J. An investigation of acoustical environments in the elderly care facilities. Appl. Acoust. 2018, 137, 45–50. [Google Scholar] [CrossRef]
- Sanford, A.M.; Orrell, M.; Tolson, D.; Abbatecola, A.M.; Arai, H.; Bauer, J.M.; Goel, A. An International Definition for “Nursing Home”. J. Am. Med Dir. Assoc. 2015, 16, 181–184. [Google Scholar] [CrossRef]
- United Nations. World Population Ageing: 1950–2050; Department of Economic and Social Affairs—Population Division, United Nations Publications: New York, NY, USA, 2001. [Google Scholar]
- Van den Bosch, K.A.; Andringa, T.C.; Başkent, D.; Vlaskamp, C. The Role of Sound in Residential Facilities for People With Profound Intellectual and Multiple Disabilities. J. Policy Pract. Intellect. Disabil. 2016, 13, 61–68. [Google Scholar] [CrossRef]
- Aletta, F.; Botteldooren, D.; Thomas, P.; Vander Mynsbrugge, T.; De Vriendt, P.; Van de Velde, D.; Devos, P. Monitoring Sound Levels and Soundscape Quality in the Living Rooms of Nursing Homes: A Case Study in Flanders (Belgium). Appl. Sci. 2017, 7, 874. [Google Scholar] [CrossRef] [Green Version]
- Aletta, F.; Vander Mynsbrugge, T.; Van de Velde, D.; De Vriendt, P.; Thomas, P.; Filipan, K.; Devos, P. Awareness of 'sound' in nursing homes: A large-scale soundscape survey in Flanders (Belgium). Build. Acoust. 2018, 25, 43–59. [Google Scholar] [CrossRef]
- Van den Bosch, K.A.; Andringa, T.C.; Post, W.J.; Ruijssenaars, W.A.; Vlaskamp, C. The relationship between soundscapes and challenging behavior: A small-scale intervention study in a healthcare organization for individuals with severe or profound intellectual disabilities. Build. Acoust. 2018, 25, 123–135. [Google Scholar] [CrossRef]
- Hayne, M.J.; Fleming, R. Acoustic design guidelines for dementia care facilities. In Proceedings of the Internoise 2014 Conference, Melbourne, Australia, 16–19 November 2014. [Google Scholar]
- Fleming, R.; Purandare, N. Long-term care for people with dementia: Environmental design guidelines. Int. Psychogeriatr. 2010, 22, 1084–1096. [Google Scholar] [CrossRef] [Green Version]
- Devos, P.; Aletta, F.; Thomas, P.; Petrovic, M.; Vander Mynsbrugge, T.; Van de Velde, D.; Botteldooren, D. Designing Supportive Soundscapes for Nursing Home Residents with Dementia. Int. J. Environ. Res. Public Health 2019, 16, 4904. [Google Scholar] [CrossRef] [Green Version]
- Thomas, P.; Aletta, F.; Filipan, K.; Vander Mynsbrugge, T.; De Geetere, L.; Dijckmans, A.; Devos, P. Noise environments in nursing homes: An overview of the literature and a case study in Flanders with quantitative and qualitative methods. Appl. Acoust. 2020, 159, 107103. [Google Scholar] [CrossRef]
- Milisen, K.; Abraham, I.; Siebens, K.; Darras, E.; Dierckx de Casterlé, B. Work environment and workforce problems: A cross-sectional questionnaire survey of hospital nurses in Belgium. Int. J. Nurs. Stud. 2006, 43, 745–754. [Google Scholar] [CrossRef]
- Xie, H.; Kang, J.; Mills, G.H. Clinical review: The impact of noise on patients' sleep and the effectiveness of noise reduction strategies in intensive care units. Crit. Care 2009, 13, 208. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.; Kang, J. The acoustic environment of intensive care wards based on long period nocturnal measurements. Noise Health 2012, 14, 230–236. [Google Scholar]
- Gopinath, B.; Thiagalingam, A.; Teber, E.; Mitchell, P. Exposure to workplace noise and the risk of cardiovascular disease events and mortality among older adults. Prev. Med. 2011, 53, 390–394. [Google Scholar] [CrossRef]
- Passchier-Vermeer, W.; Passchier, W.F. Noise exposure and public health. Environ. Health Perspectve 2000, 108, 123–131. [Google Scholar]
- World Health Organization. Burden of Disease from Environmental Noise; WHO Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Śliwińska-Kowalska, M.; Zaborowski, K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Permanent Hearing Loss and Tinnitus. Int. J. Environ. Res. Public Health 2017, 14, 1139. [Google Scholar] [CrossRef]
- Department of Health. Health Technical Memorandum 08-01: Acoustics; Specialist Services; Department of Health: London, UK, 2013. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/144248/HTM_08-01.pdf (accessed on 12 May 2020).
- Graham, M.E. Re-socialising sound: Investigating sound, selfhood and intersubjectivity among people living with dementia in long-term care. Sound Stud. 2018. [Google Scholar] [CrossRef]
- Devos, P.; Aletta, F.; Vander Mynsbrugge, T.; Thomas, P.; Filipan, K.; Petrovic, M.; Botteldooren, D. Soundscape Design for Management of Behavioral Disorders: A Pilot Study among Nursing Home Residents with Dementia. In Proceedings of the Internoise 2018 Conference, Chicago, IL, USA, 26–29 August 2018. [Google Scholar]
- Rindel, J.H. Verbal communication and noise in eating establishments. Appl. Acoust. 2010, 71, 1156–1161. [Google Scholar] [CrossRef]
- Devos, P.; Thomas, P.; Aletta, F.; Vander Mynsbrugge, T.; De Vriendt, P.; Van de Velde, D.; Botteldooren, D. Towards understanding healthy and supportive acoustic environments: The case of a nursing home. In Proceedings of the International Conference on Acoustics ICA 2019, Aachen, Germany, 9–13 September 2019. [Google Scholar]
- Van Hout, N.H.; Hak, C.C.; Suren, S.; Kort, H.S. Acoustic measurements of sound levels in common rooms and sleeping rooms of care facilities for older adults. Gerontechnology 2014, 13, 86–87. [Google Scholar]
- Wiratha, M.S.; Tsaih, L. Acoustic comfort in long-term care facilities based on listening impressions from normal hearing individuals. Proc. Meet. Acoust. 2015, 25, 015003. [Google Scholar] [CrossRef] [Green Version]
- Rindel, J.H. The acoustics of places for social gatherings. In Proceedings of the Euronoise 2015 Conference, Maastricht, The Netherlands, 31 May–3 June 2015; pp. 2429–2436. [Google Scholar]
- Rindel, J.H. Acoustical capacity as a means of noise control in eating establishments. In Proceedings of the Joint Baltic-Nordic Acoustic Meeting BNAM 2012, Odense, Denmark, 18–20 June 2012. [Google Scholar]
- Hodgson, M.; Steininger, G.; Razavi, Z. Measurement and prediction of speech and noise levels and the Lombard effect in eating establishments. J. Acoust. Soc. Am. 2007, 121, 2023–2033. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 3382-2:2008 Acoustics—Measurement of Room Acoustic Parameters—Part 2: Reverberation Time in Ordinary Rooms; ISO: Geneva, Switzerland, 2008. [Google Scholar]
- Fernandez-Prieto, J.A.; Cañada-Bago, J.; Gadeo-Martos, M.A. Wireless Acoustic Sensor Nodes for Noise Monitoring in the City of Linares (Jaén). Sensors 2020, 20, 124. [Google Scholar] [CrossRef] [Green Version]
- Alías, F.; Alsina-Pagès, R.M. Review of Wireless Acoustic Sensor Networks for Environmental Noise Monitoring in Smart Cities. J. Sens. 2019, 7634860. [Google Scholar] [CrossRef] [Green Version]
- Van Renterghem, T.; Thomas, P.; Dominguez, F.; Dauwe, S.; Touhafi, A.; Dhoedt, B.; Botteldooren, D. On the ability of consumer electronics microphones for environmental noise monitoring. J. Environ. Monit. 2011, 13, 544–552. [Google Scholar] [CrossRef]
- Picaut, J.; Can, A.; Fortin, N.; Ardouin, J.; Lagrange, M. Low-Cost Sensors for Urban Noise Monitoring Networks—A Literature Review. Sensors 2020, 20, 2256. [Google Scholar] [CrossRef]
- Flemish Government. Eindrapport Ontwikkeling Van Specifieke Energieprestatie-Indicatoren Voor Rusthuizen; Department of Welfare, Public Health and Family: Brussels, Belgium, 2010. [Google Scholar]
- Lazarus, H. Prediction of Verbal Communication is Noise—A review: Part 1. Appl. Acoust. 1986, 19, 439–464. [Google Scholar] [CrossRef]
- Lazarus, H. Prediction of verbal communication in noise—A development of generalized SIL curves and the quality of communication (Part 2). Appl. Acoust. 1987, 20, 245–261. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 9921:2003 Ergonomics—Assessment of Speech Communication; ISO: Geneva, Switzerland, 2003. [Google Scholar]
- Mosnier, I.; Bebear, J.P.; Marx, M.; Fraysse, B.; Truy, E.; Lina-Granade, G.; Mondain, M.; Sterkers-Artières, F.; Bordure, P.; Robier, A.; et al. Improvement of Cognitive Function After Cochlear Implantation in Elderly Patients. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 442–450. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| c (dB/dB) | Average Deviation (dB) | ||
|---|---|---|---|
| Group Size, g | |||
| 8 | 9 | 10 | |
| 0.4 | 1.8 | 2.7 | 3.4 |
| 0.5 | −0.8 | 0.3 | 1.2 |
| 0.6 | −4.6 | −3.3 | −2.2 |
| 0.7 | −11.1 | −9.4 | −7.9 |
| Ap (m2) | Average Deviation (dB) | ||
|---|---|---|---|
| Group Size, g | |||
| 8 | 9 | 10 | |
| 0.2 | −0.8 | 0.3 | 1.2 |
| 0.3 | −0.6 | 0.4 | 1.4 |
| 0.4 | −0.4 | 0.6 | 1.5 |
| 0.5 | −0.3 | 0.8 | 1.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devos, P.; Aletta, F.; Thomas, P.; Vander Mynsbrugge, T.; Petrovic, M.; Van de Velde, D.; De Vriendt, P.; Botteldooren, D. Application of a Prediction Model for Ambient Noise Levels and Acoustical Capacity for Living Rooms in Nursing Homes Hosting Older People with Dementia. Appl. Sci. 2020, 10, 4205. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124205
Devos P, Aletta F, Thomas P, Vander Mynsbrugge T, Petrovic M, Van de Velde D, De Vriendt P, Botteldooren D. Application of a Prediction Model for Ambient Noise Levels and Acoustical Capacity for Living Rooms in Nursing Homes Hosting Older People with Dementia. Applied Sciences. 2020; 10(12):4205. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124205
Chicago/Turabian StyleDevos, Paul, Francesco Aletta, Pieter Thomas, Tara Vander Mynsbrugge, Mirko Petrovic, Dominique Van de Velde, Patricia De Vriendt, and Dick Botteldooren. 2020. "Application of a Prediction Model for Ambient Noise Levels and Acoustical Capacity for Living Rooms in Nursing Homes Hosting Older People with Dementia" Applied Sciences 10, no. 12: 4205. https://0-doi-org.brum.beds.ac.uk/10.3390/app10124205