Automated Classification of Blood Loss from Transurethral Resection of the Prostate Surgery Videos Using Deep Learning Technique

Abstract
:1. Introduction
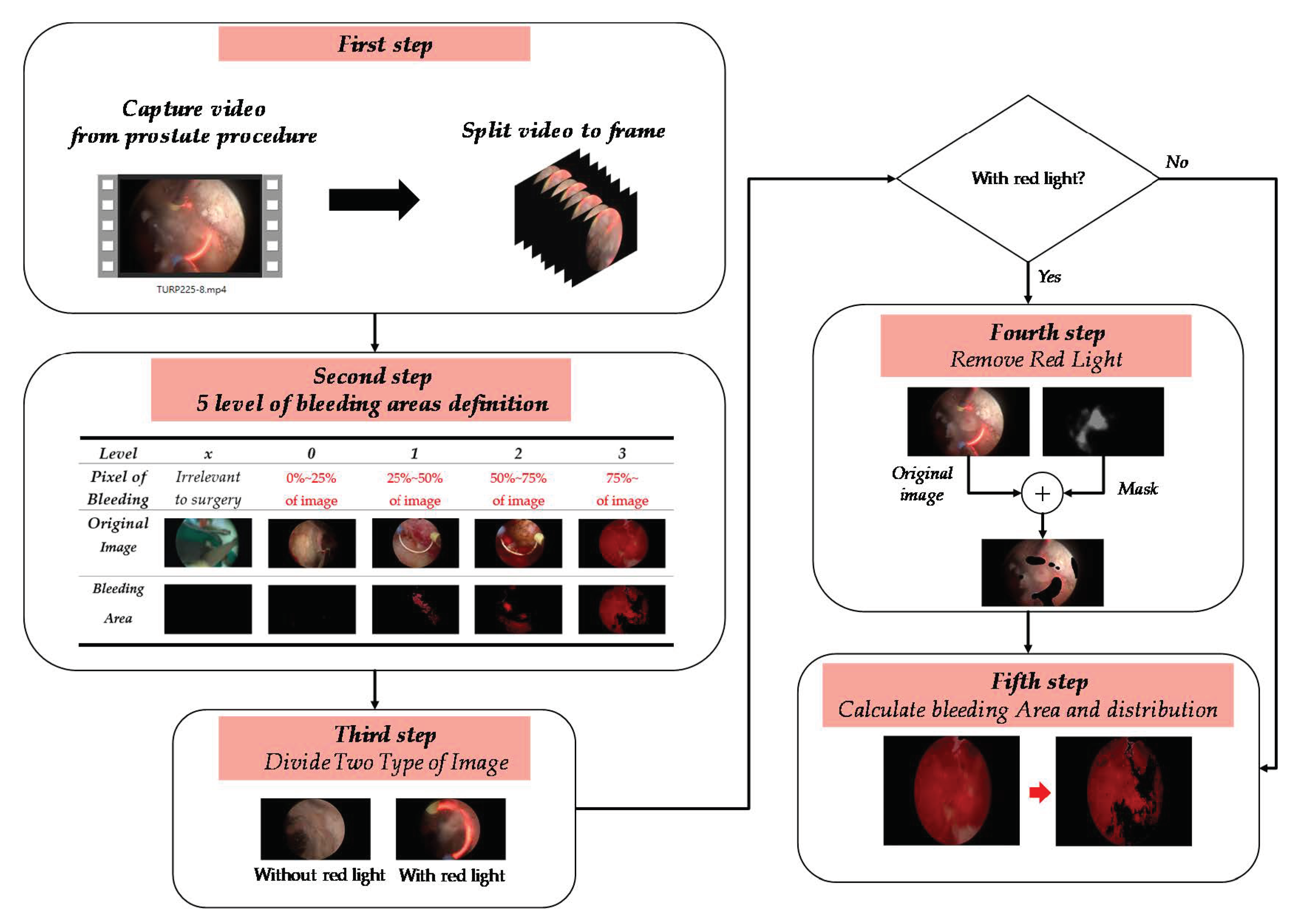
2. Materials and Methods
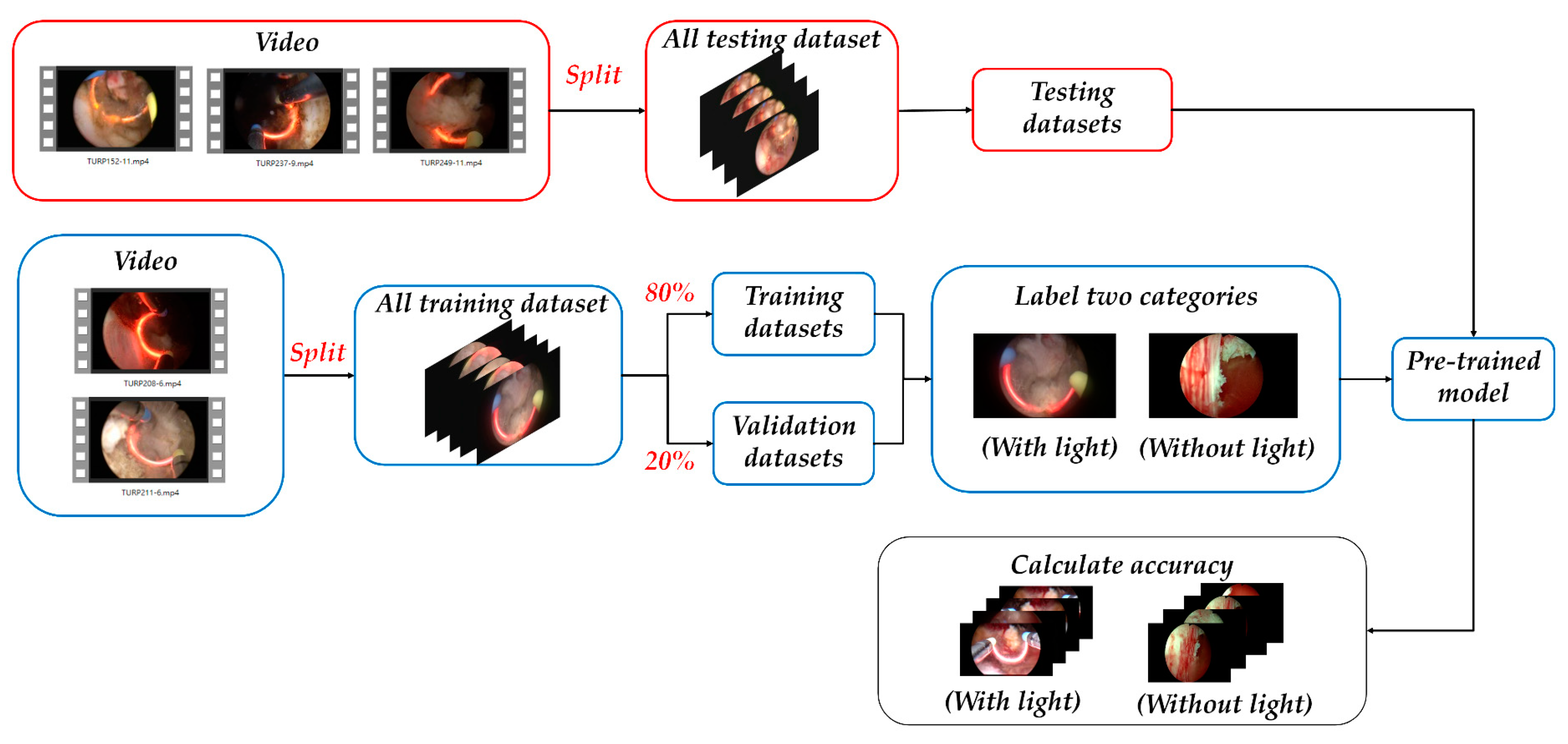
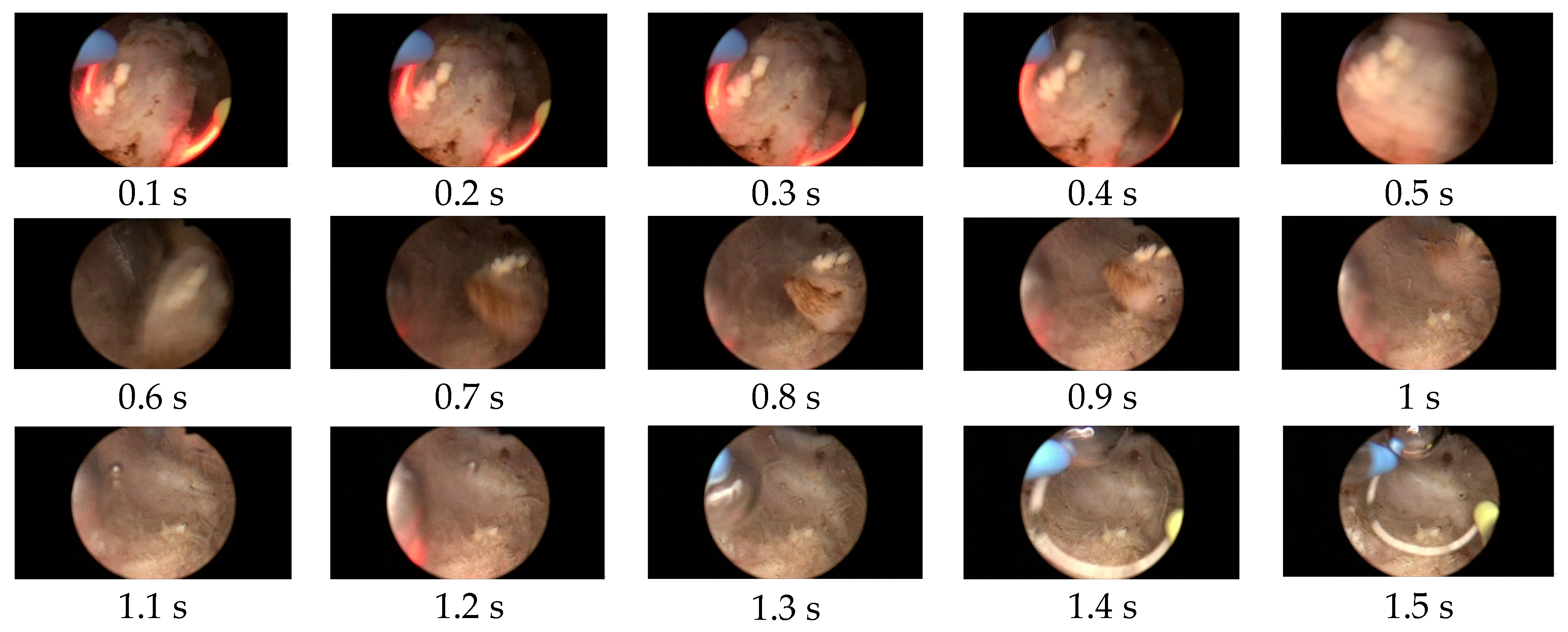
2.1. Detection of the Appearance of the Red Light Images Using the ResNet-50 Model
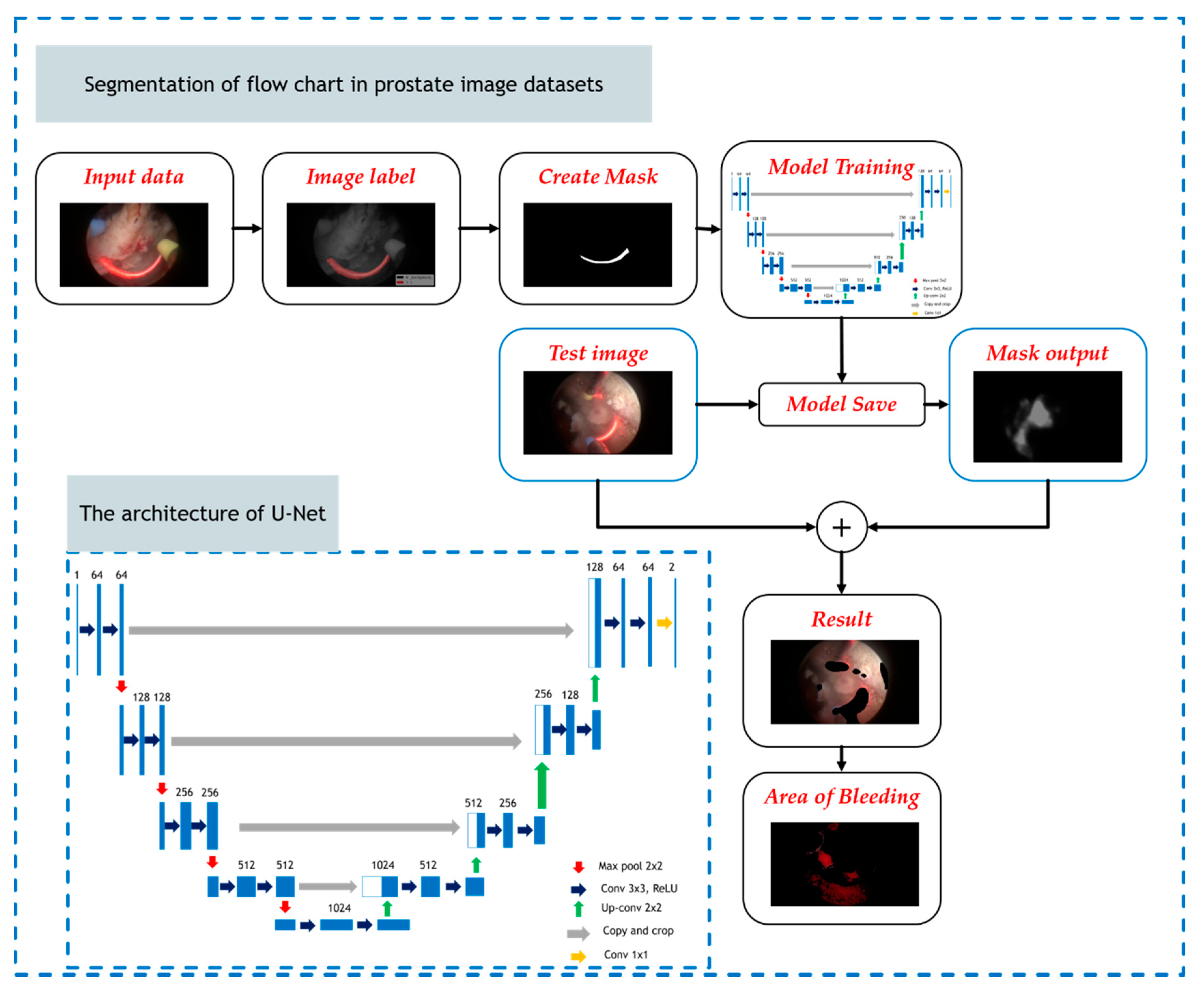
2.2. Extract Features of the Red Light Using the U-Net Model
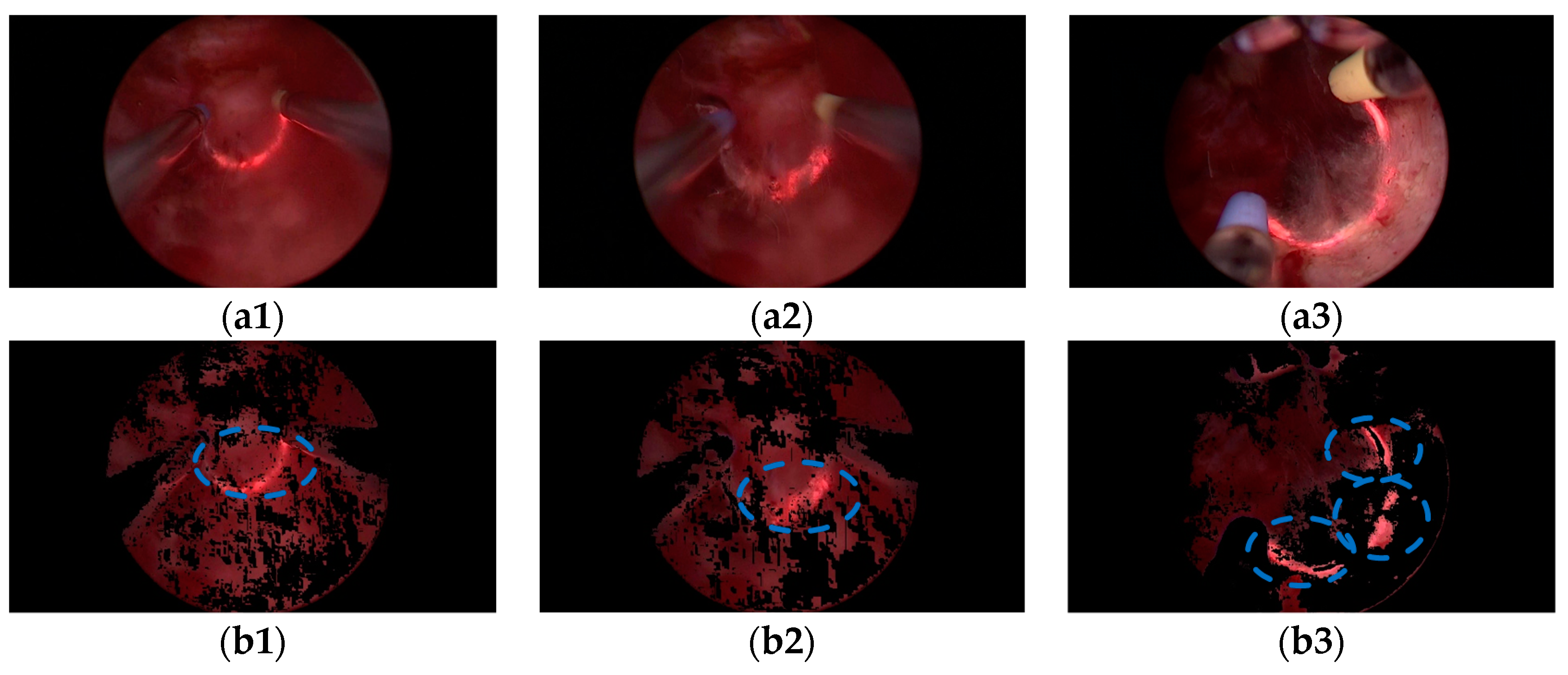
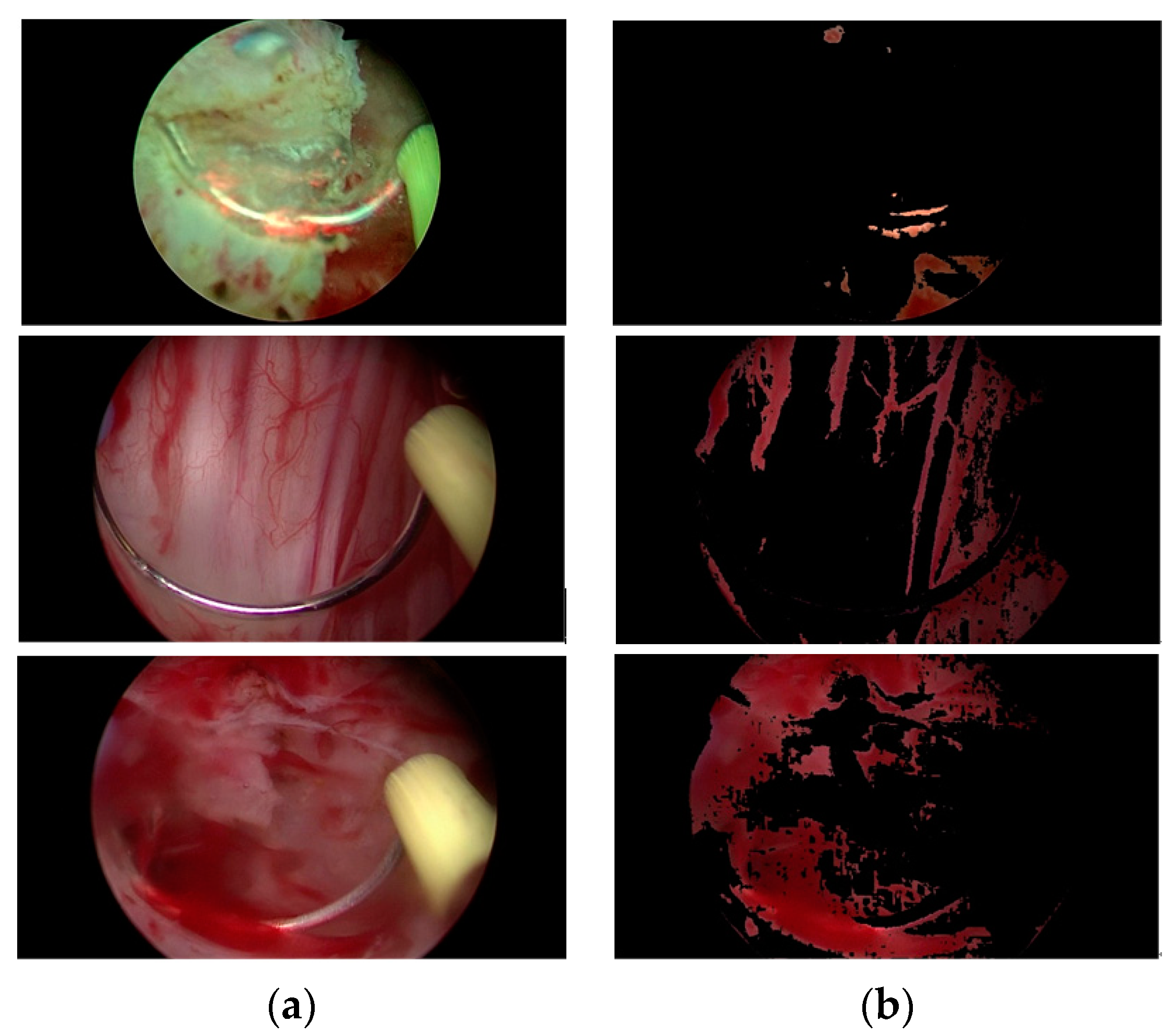
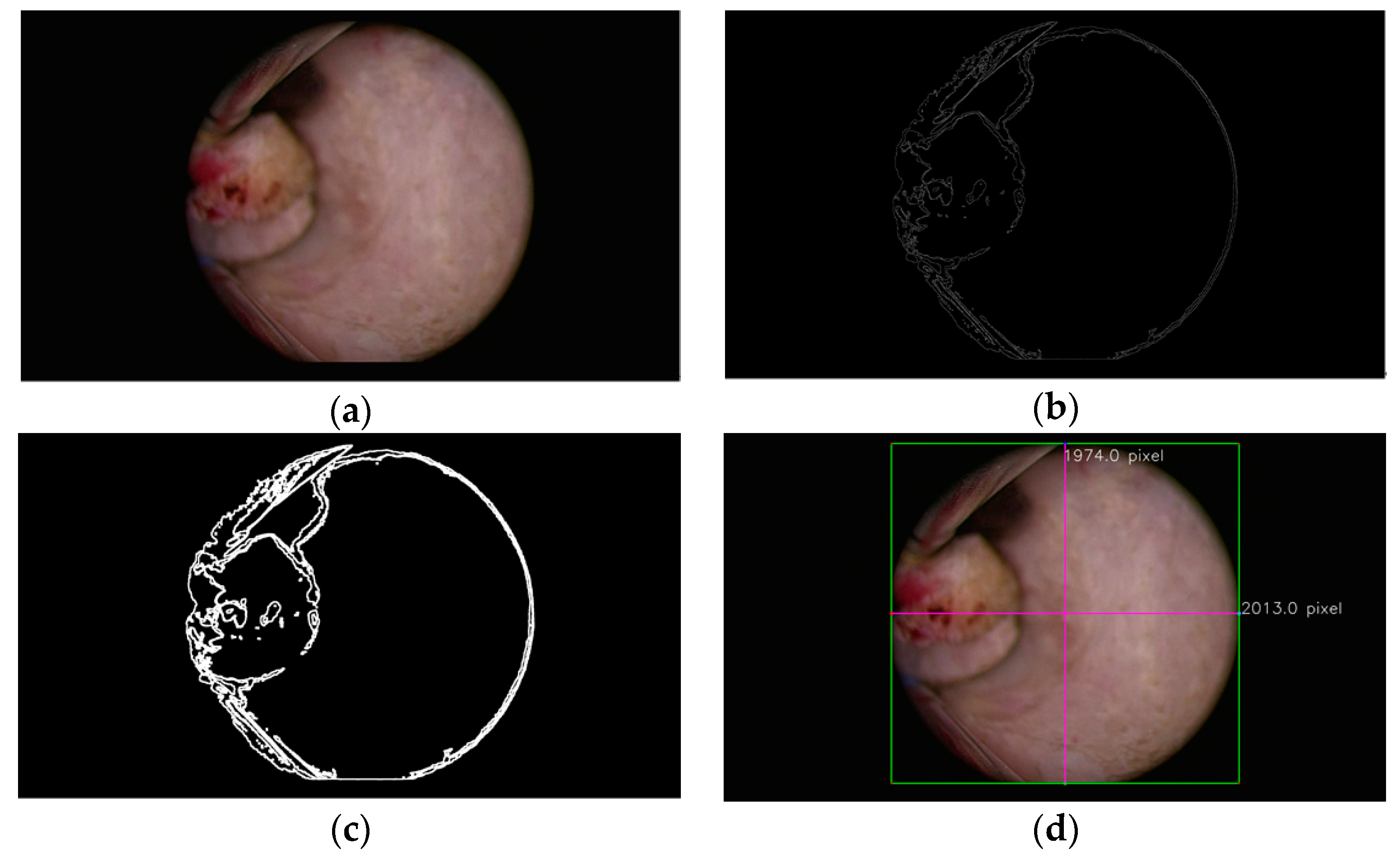
2.3. Level Classification of the Bleeding Regions Using the HSV Color Space Analysis Method
3. Experiments and Results
3.1. Preparation of Prostate Image Datasets for the ResNet-50 Classification Model
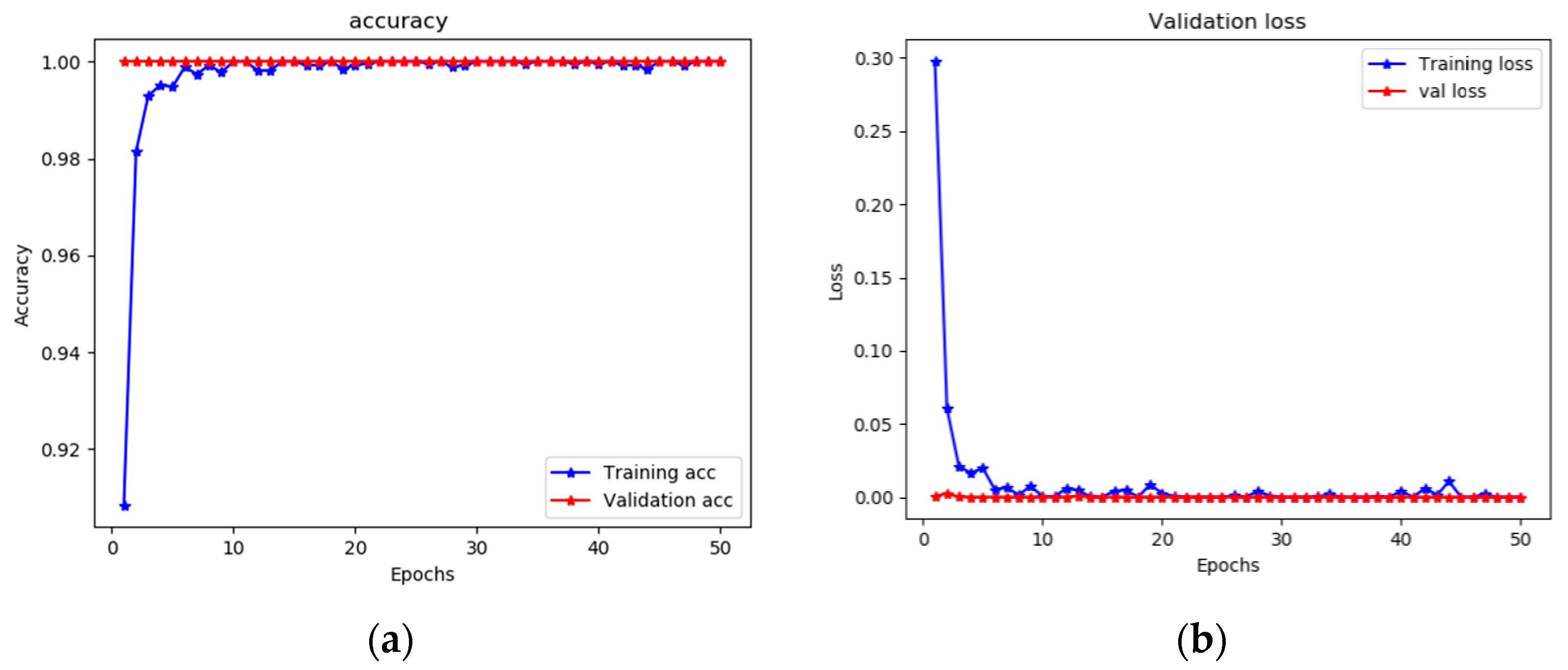
3.2. Performance of the ResNet-50 Classification Model
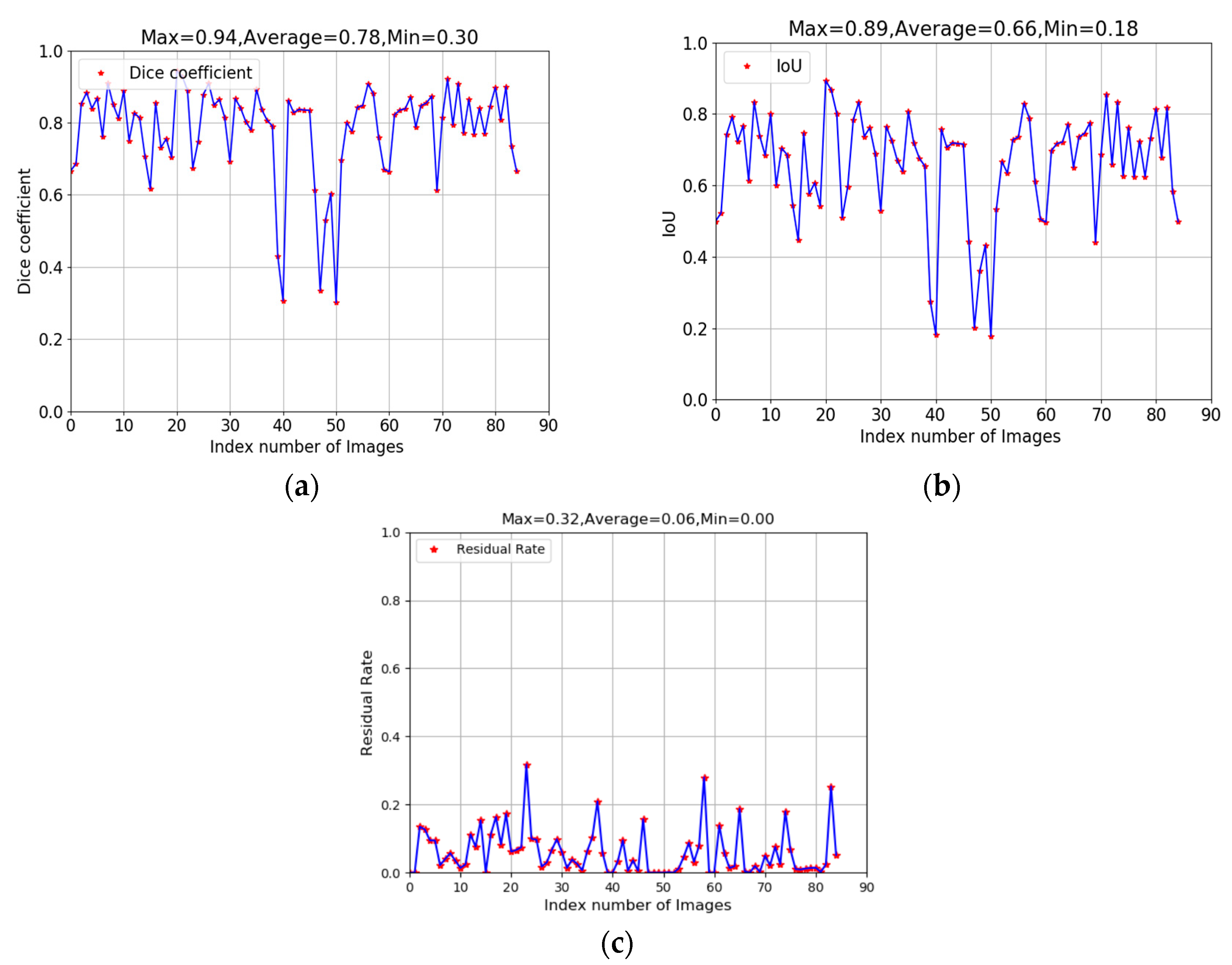
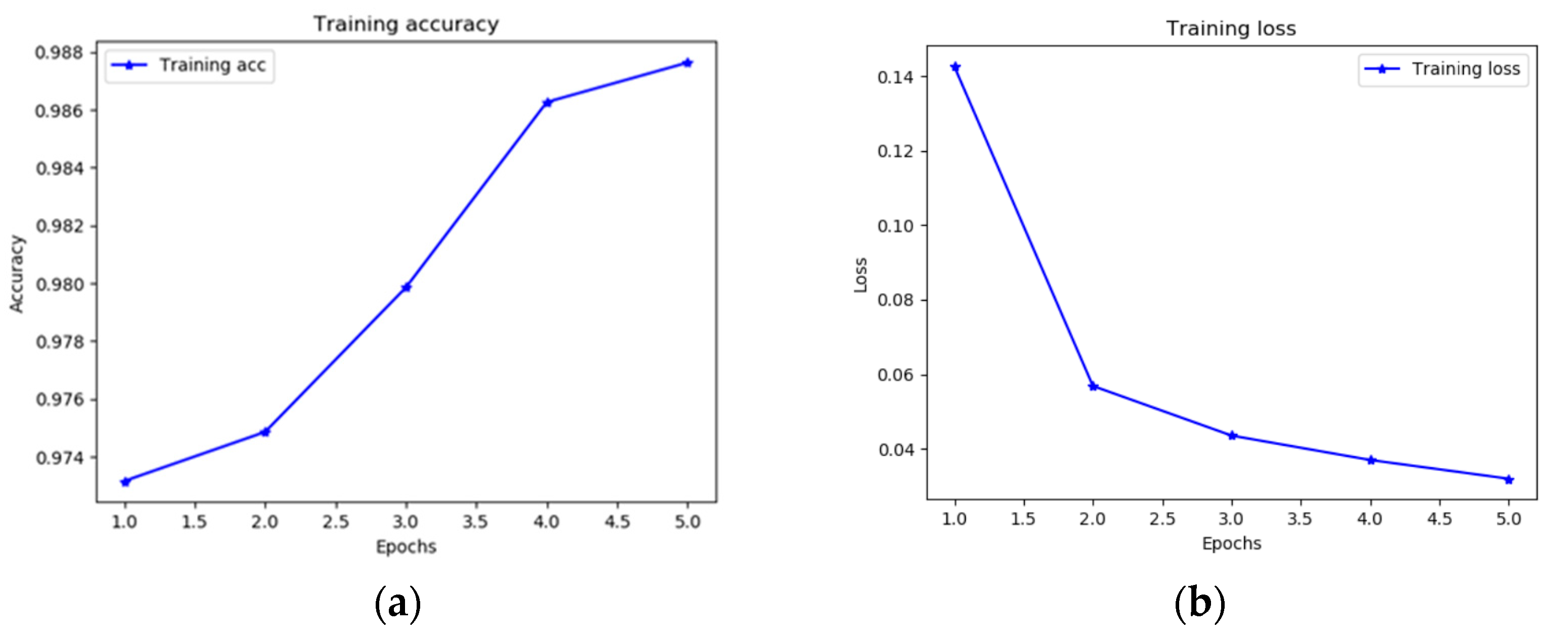
3.3. Performance of U-Net Segmentation and HSV Color Space Extraction
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Available online: https://www.health.harvard.edu/mens-health/the-growing-problem-of-an-enlarged-prostate-gland (accessed on 4 March 2020).
- Gravas, S.; Cornu, J.; Drake, M.; Gacci, M.; Gratzke, C.; Herrmann, T.; Mamoulakis, C.; Rieken, M.; Speakman, M.; Tikkinen, K.J.E.G. Management of Non-Neurogenic Male LUTS; EAU: Arnhem, The Netherlands, 2017. [Google Scholar]
- Wasson, J.H.; Reda, D.J.; Bruskewitz, R.C.; Elinson, J.; Keller, A.M.; Henderson, W.G. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. The veterans affairs cooperative study group on transurethral resection of the prostate. N. Engl. J. Med. 1995, 332, 75–79. [Google Scholar] [CrossRef]
- Ghalayini, I.F.; Al-Ghazo, M.A.; Pickard, R.S. A prospective randomized trial comparing transurethral prostatic resection and clean intermittent self-catheterization in men with chronic urinary retention. BJU Int. 2005, 96, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Abrams, P.; Donovan, J.L.; Neal, D.E.; Brookes, S.T.; Chacko, K.N.; Wright, M.J.; Timoney, A.G.; Peters, T.J. A prospective randomized trial comparing transurethral resection of the prostate and laser therapy in men with chronic urinary retention: The CLasP study. J. Urol. 2000, 164, 59–64. [Google Scholar] [CrossRef]
- Chughtai, B.; Te, A.E. Non-laser transurethral resection of the prostate. In Minimally Invasive Urology; Springer: Berlin/Heidelberg, Germany, 2015; pp. 195–203. [Google Scholar]
- Jansen, H.; Berseus, O.; Johansson, J.E. A simple photometric method for determination of blood loss during transurethral surgery. Scand. J. Urol. Nephrol. 1978, 12, 1–5. [Google Scholar]
- Fagerström, T.; Nyman, C.R.; Hahn, R.G. Bipolar transurethral resection of the prostate causes less bleeding than the monopolar technique: A single-centre randomized trial of 202 patients. BJU Int. 2010, 105, 1560–1564. [Google Scholar] [CrossRef]
- Aarnink, R.G.; Huynen, A.L.; Giesen, R.J.; de la Rosette, J.J.; Debruyne, F.M.; Wijkstra, H. Automated prostate volume determination with ultrasonographic imaging. J. Urol. 1995, 153, 1549–1554. [Google Scholar] [CrossRef] [Green Version]
- Crivianu-Gaita, D.; Miclea, F.; Gaspar, A.; Margineatu, D.; Holban, S. 3D reconstruction of prostate from ultrasound images. Int. J. Med. Inform. 1997, 45, 43–51. [Google Scholar] [CrossRef]
- Jiang, H.; Zhou, Y. Safety and efficacy of thulium laser prostatectomy versus transurethral resection of prostate for treatment of benign prostate hyperplasia: A meta-analysis. Low Urin. Tract Symptoms 2016, 8, 165–170. [Google Scholar] [CrossRef]
- Skinner, T.A.A.; Leslie, R.J.; Steele, S.S.; Nickel, J.C. Randomized, controlled trial of laser vs. bipolar plasma vaporization treatment of benign prostatic hyperplasia. Can. Urol. Assoc. J. 2017, 11, 194–198. [Google Scholar] [CrossRef] [Green Version]
- Sung, Y.S.; Kwon, H.J.; Park, B.W.; Cho, G.; Lee, C.K.; Cho, K.S.; Kim, J.K. Prostate cancer detection on dynamic contrast-enhanced MRI: Computer-aided diagnosis versus single perfusion parameter maps. AJR Am. J. Roentgenol. 2011, 197, 1122–1129. [Google Scholar] [CrossRef] [Green Version]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph 2007, 31, 198–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Piérola, L.B.F. Transanal resection of complicated rectal polyps using the urological resectoscope. Kirurgia 2005, 235, 2. [Google Scholar]
- Chang, Y.; Tsai, E.M.; Long, C.Y.; Lee, C.L.; Kay, N. Resectoscopic treatment combined with sonohysterographic evaluation of women with postmenstrual bleeding as a result of previous cesarean delivery scar defects. Am. J. Obstet. Gynecol. 2009, 200, 370–371. [Google Scholar] [CrossRef] [PubMed]
- Pantuck, A.J.; Baniel, J.; Kirkali, Z.; Klatte, T.; Zomorodian, N.; Yossepowitch, O.; Belldegrun, A.S. A novel resectoscope for transurethral resection of bladder tumors and the prostate. J. Urol. 2007, 178, 2331–2336. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, J.; Strand, J.; Kiesling, J.V.; Belville, W. Use of resectoscope for colon cancer. Urol. Clin. N. Am. 1990, 17, 63–66. [Google Scholar]
- Yap, M.H.; Pons, G.; Martí, J.; Ganau, S.; Sentís, M.; Zwiggelaar, R.; Davison, A.K.; Martí, R. Automated breast ultrasound lesions detection using convolutional neural networks. IEEE J. Biomed. Health Inform. 2017, 22, 1218–1226. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Chen, W.; Dong, X. Automatic classification of chinese herbal based on deep learning method. In Proceedings of the 2018 14th International Conference on Natural Computation, Fuzzy Systems and Knowledge Discovery (ICNC-FSKD), Huangshan, China, 28–30 July 2018; pp. 235–238. [Google Scholar]
- Dai, Y.; Tang, Z.; Wang, Y. Data driven intelligent diagnostics for Parkinson’s disease. IEEE Access 2019, 7, 106941–106950. [Google Scholar] [CrossRef]
- Huang, Y.J.; Dou, Q.; Wang, Z.X.; Liu, L.Z.; Wang, L.S.; Chen, H.; Heng, P.A.; Xu, R.H. HL-FCN: Hybrid loss guided FCN for colorectal cancer segmentation. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Omni, Shoreham Hotel, Washington, DC, USA, 4–7 April 2018; pp. 195–198. [Google Scholar]
- Xie, Y.; Xia, Y.; Zhang, J.; Song, Y.; Feng, D.; Fulham, M.; Cai, W. Knowledge-based collaborative deep learning for benign-malignant lung nodule classification on chest CT. IEEE Trans. Med. Imaging 2018, 38, 991–1004. [Google Scholar] [CrossRef]
- Zhang, R.; Zhao, L.; Lou, W.; Abrigo, J.M.; Mok, V.C.; Chu, W.C.; Wang, D.; Shi, L. Automatic segmentation of acute ischemic stroke from DWI using 3-D fully convolutional DenseNets. IEEE Trans. Med. Imaging 2018, 37, 2149–2160. [Google Scholar] [CrossRef]
- Zeng, Z.; Xie, W.; Zhang, Y.; Lu, Y. RIC-Unet: An improved neural network based on Unet for nuclei segmentation in histology images. IEEE Access 2019, 7, 21420–21428. [Google Scholar] [CrossRef]
- Sharma, N.; Aggarwal, L.M. Automated medical image segmentation techniques. J. Med. Phys. Assoc. Med. Phys. India 2010, 35, 3. [Google Scholar] [CrossRef] [PubMed]
- Milletari, F.; Navab, N.; Ahmadi, S.A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford University, Califonia, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Alom, M.Z.; Hasan, M.; Yakopcic, C.; Taha, T.M.; Asari, V.K. Recurrent residual convolutional neural network based on u-net (r2u-net) for medical image segmentation. arXiv 2018, arXiv:1802.06955. [Google Scholar]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.M.; Larochelle, H. Brain tumor segmentation with Deep Neural Networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, H.R.; Farag, A.; Lu, L.; Turkbey, E.B.; Summers, R.M. Deep convolutional networks for pancreas segmentation in CT imaging. In Proceedings of the Medical Imaging 2015: Image Processing, Orlando, Florida, FL, USA, 24–26 February 2015; p. 94131G. [Google Scholar]
- Jorge, F.P.; Juan, T.O.; Edgar, R.R.; Salvador, C.; Porfirio, J.L.; Jorge, H.V.; Juan, M.R.M. Fig plant segmentation from aerial images using a deep convolutional encoder-decoder network. Remote Sens. 2019, 11, 1157. [Google Scholar] [CrossRef] [Green Version]
- Mulham, F.; Ali, Y.; Domenico, D.B.; Alberto, P.; Daniele, N. Crop and Weeds Classification for Precision Agriculture using Context-Independent Pixel-Wise Segmentation. In Proceedings of the 2019 3th IEEE International Conference on Robotic Computing (IRC), Naples, Italy, 25–27 February 2019; pp. 146–152. [Google Scholar]
- Mohsen, H.; El-Dahshan, E.S.A.; El-Horbaty, E.S.M.; Salem, A.B.M. Classification using deep learning neural networks for brain tumors. Future Comput. Inform. J. 2018, 3, 68–71. [Google Scholar] [CrossRef]
- Cruz-Roa, A.; Gilmore, H.; Basavanhally, A.; Feldman, M.; Ganesan, S.; Shih, N.N.C.; Tomaszewski, J.; Gonzalez, F.A.; Madabhushi, A. Accurate and reproducible invasive breast cancer detection in whole-slide images: A Deep Learning approach for quantifying tumor extent. Sci. Rep. 2017, 7, 46450. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lei, B.; Ahmed, E.; Tan, E.L.; Wang, W.; Huang, F.; Gong, X.; Wang, T. Breast cancer image classification via multi-network features and dual-network orthogonal low-rank learning. IEEE Access 2020, 8, 27779–27792. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, G.; Li, H. Automatic cataract classification using deep neural network with discrete state transition. IEEE Trans. Med. Imaging 2020, 39, 436–446. [Google Scholar] [CrossRef]
- Guo, S.; Yang, Z. Multi-Channel-ResNet: An integration framework towards skin lesion analysis. Inform. Med. Unlocked 2018, 12, 67–74. [Google Scholar] [CrossRef]
- Ghosh, T.; Li, L.; Chakareski, J. Effective deep learning for semantic segmentation based bleeding zone detection in capsule endoscopy images. In Proceedings of the 2018 25th IEEE International Conference on Image Processing (ICIP), Athens, Greece, 7–10 October 2018; pp. 3034–3038. [Google Scholar]
- Ghosh, T.; Fattah, S.A.; Wahid, K.A. Automatic bleeding detection in wireless capsule endoscopy based on RGB pixel intensity ratio. In Proceedings of the 2014 International Conference on Electrical Engineering and Information & Communication Technology, Dhaka, Bangladesh, 10–12 April 2014; pp. 1–4. [Google Scholar]
- Ghosh, T.; Bashar, S.K.; Alam, M.S.; Wahid, K.; Fattah, S.A. A statistical feature based novel method to detect bleeding in wireless capsule endoscopy images. In Proceedings of the 2014 International Conference on Informatics, Electronics & Vision (ICIEV), Dhaka, Bangladesh, 23–24 May 2014; pp. 1–4. [Google Scholar]
- Sainju, S.; Bui, F.M.; Wahid, K. Bleeding detection in wireless capsule endoscopy based on color features from histogram probability. In Proceedings of the 2013 26th IEEE Canadian Conference on Electrical and Computer Engineering (CCECE), Regina, SK, Canada, 5–8 May 2013; pp. 1–4. [Google Scholar]
- Gonzalez, R.C.; Woods, R.E. Digital Image Processing, 3rd ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2008. [Google Scholar]
- Dilna, C.; Gopi, V.P. A novel method for bleeding detection in Wireless Capsule Endoscopic images. In Proceedings of the 2015 International Conference on Computing and Network Communications (CoCoNet), Trivandrum, Kerala, India, 16–19 December 2015; pp. 854–858. [Google Scholar]
- Ou, X.; Yan, P.; Zhang, Y.; Tu, B.; Zhang, G.; Wu, J.; Li, W. Moving object detection method via ResNet-18 with encoder–decoder structure in complex scenes. IEEE Access 2019, 7, 108152–108160. [Google Scholar] [CrossRef]
- Ding, Y.; Chen, F.; Zhao, Y.; Wu, Z.; Zhang, C.; Wu, D. A stacked multi-connection simple reducing net for brain tumor segmentation. IEEE Access 2019, 7, 104011–104024. [Google Scholar] [CrossRef]
- Yuan, Y.; Li, B.; Meng, M.Q.-H. Bleeding frame and region detection in the wireless capsule endoscopy video. IEEE J. Biomed. Health Inform. 2015, 20, 624–630. [Google Scholar] [CrossRef] [PubMed]
- He, J.Y.; Wu, X.; Jiang, Y.G.; Peng, Q.; Jain, R. Hookworm detection in wireless capsule endoscopy images with deep learning. IEEE Trans. Image Process. 2018, 27, 2379–2392. [Google Scholar] [CrossRef] [PubMed]
- Qummar, S.; Khan, F.G.; Shah, S.; Khan, A.; Shamshirband, S.; Rehman, Z.U.; Khan, I.A.; Jadoon, W. A Deep learning ensemble approach for diabetic retinopathy detection. IEEE Access 2019, 7, 150530–150539. [Google Scholar] [CrossRef]
- Lin, H.; Hu, Y.; Chen, S.; Yao, J.; Zhang, L. Fine-grained classification of cervical cells using morphological and appearance based convolutional neural networks. IEEE Access 2019, 7, 71541–71549. [Google Scholar] [CrossRef]
- Girish, G.; Thakur, B.; Chowdhury, S.R.; Kothari, A.R.; Rajan, J. Segmentation of intra-retinal cysts from optical coherence tomography images using a fully convolutional neural network model. IEEE J. Biomed. Health Inform. 2018, 23, 296–304. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Name | Output Size | Structure |
|---|---|---|
| Conv1 | 112 × 112 | 7 × 7, 64, stride 2 |
| Conv2_x | 56 × 56 | × 3 |
| Con3_x | 28 × 28 | × 4 |
| Conv4_x | 14 × 14 | × 6 |
| Conv5_x | 7 × 7 | × 3 |
| 1 × 1 | Average pooling, Fully Connected, Softmax |
| Level | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Pixel of Bleeding | 0%~25% of BAR | 25%~50% of BAR | 50%~75% of BAR | 75%~100% of BAR |
| Original Image |  |  |  |  |
| Bleeding Areas |  |  |  |  |
| Training/Validation | 10,410 images |
| Testing | 15,615 images |
| Actual Class Label | ||||
|---|---|---|---|---|
| Prediction Class Label | Yes | No | ||
| Yes | TP | FP | ||
| No | FN | TN | ||
| Sensitivity | Specificity | |||
| PREDICTED CLASS LABEL | |||
|---|---|---|---|
| ACTUAL CLASS LABEL | With Red Light | Without Red Light | |
| With Red Light | 1899 | 251 | |
| Without Red Light | 100 | 13,373 | |
| Dataset | Accuracy (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| Testing TURP surgery datasets | 97 | 98 | 94 |
| Index | Training Image | Ground Truth (GT) | Prediction | GT and Prediction |
|---|---|---|---|---|
| 1 |  |  |  |  |
| 2 |  |  |  |  |
| 3 |  |  |  |  |
| 4 |  |  |  |  |
| Index | Testing Images | Extraction Area | Segmentation |
|---|---|---|---|
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
| 5 |  |  |  |
| 6 |  |  |  |
| 7 |  |  |  |
| 8 |  |  |  |
| 9 |  |  |  |
| 10 |  |  |  |
| Index | Testing Image | Bleeding Area without Using U-Net Model | Bleeding Area with Using U-Net Model |
|---|---|---|---|
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
| 5 |  |  |  |
| 6 |  |  |  |
| 7 |  |  |  |
| 8 |  |  |  |
| 9 |  |  |  |
| 10 |  |  |  |
| Model | Mean Residual Coefficient (EPOCH = 50 LR = 0.00001) |
|---|---|
| Res-Unet model | 0.28 |
| Autoencoder model [31] | 0.63 |
| Segnet model [32] | 0.70 |
| Index | Testing Image | Res-Unet Model | Autoencoder Model | Segnet Model |
|---|---|---|---|---|
| 1 |  |  |  |  |
| 2 |  |  |  |  |
| 3 |  |  |  |  |
| 4 |  |  |  |  |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-W.; Lin, W.-J.; Lin, C.-Y.; Hung, C.-L.; Hou, C.-P.; Cho, C.-C.; Young, H.-T.; Tang, C.-Y. Automated Classification of Blood Loss from Transurethral Resection of the Prostate Surgery Videos Using Deep Learning Technique. Appl. Sci. 2020, 10, 4908. https://0-doi-org.brum.beds.ac.uk/10.3390/app10144908
Chen J-W, Lin W-J, Lin C-Y, Hung C-L, Hou C-P, Cho C-C, Young H-T, Tang C-Y. Automated Classification of Blood Loss from Transurethral Resection of the Prostate Surgery Videos Using Deep Learning Technique. Applied Sciences. 2020; 10(14):4908. https://0-doi-org.brum.beds.ac.uk/10.3390/app10144908
Chicago/Turabian StyleChen, Jian-Wen, Wan-Ju Lin, Chun-Yuan Lin, Che-Lun Hung, Chen-Pang Hou, Ching-Che Cho, Hong-Tsu Young, and Chuan-Yi Tang. 2020. "Automated Classification of Blood Loss from Transurethral Resection of the Prostate Surgery Videos Using Deep Learning Technique" Applied Sciences 10, no. 14: 4908. https://0-doi-org.brum.beds.ac.uk/10.3390/app10144908