Vesicular Emulgel Based System for Transdermal Delivery of Insulin: Factorial Design and in Vivo Evaluation

 ,
,  , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
2.1. Materials
2.2. Preparation of Niosome Emulgel
2.3. Experimental Design
2.4. Evaluation
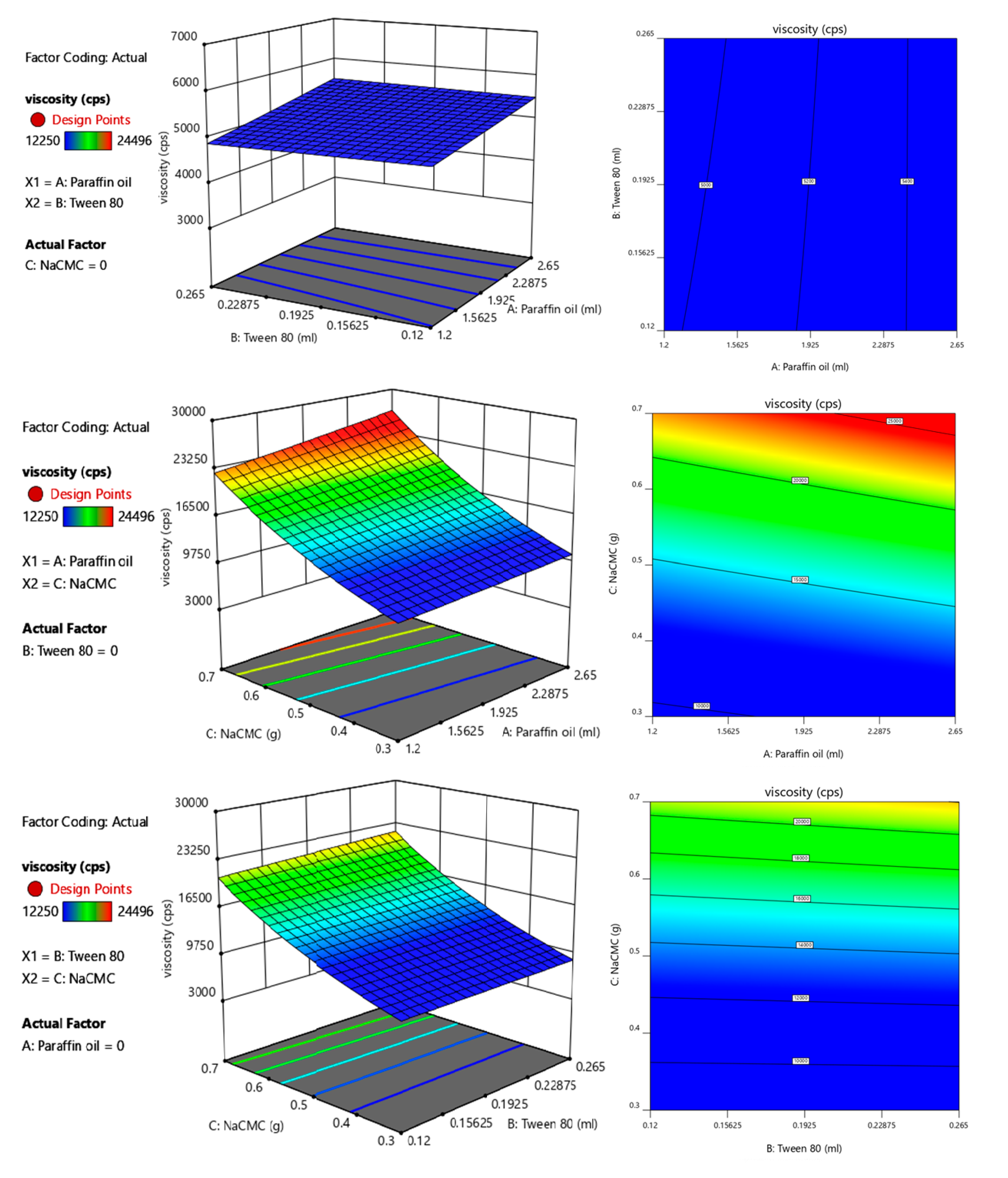
2.4.1. Viscosity
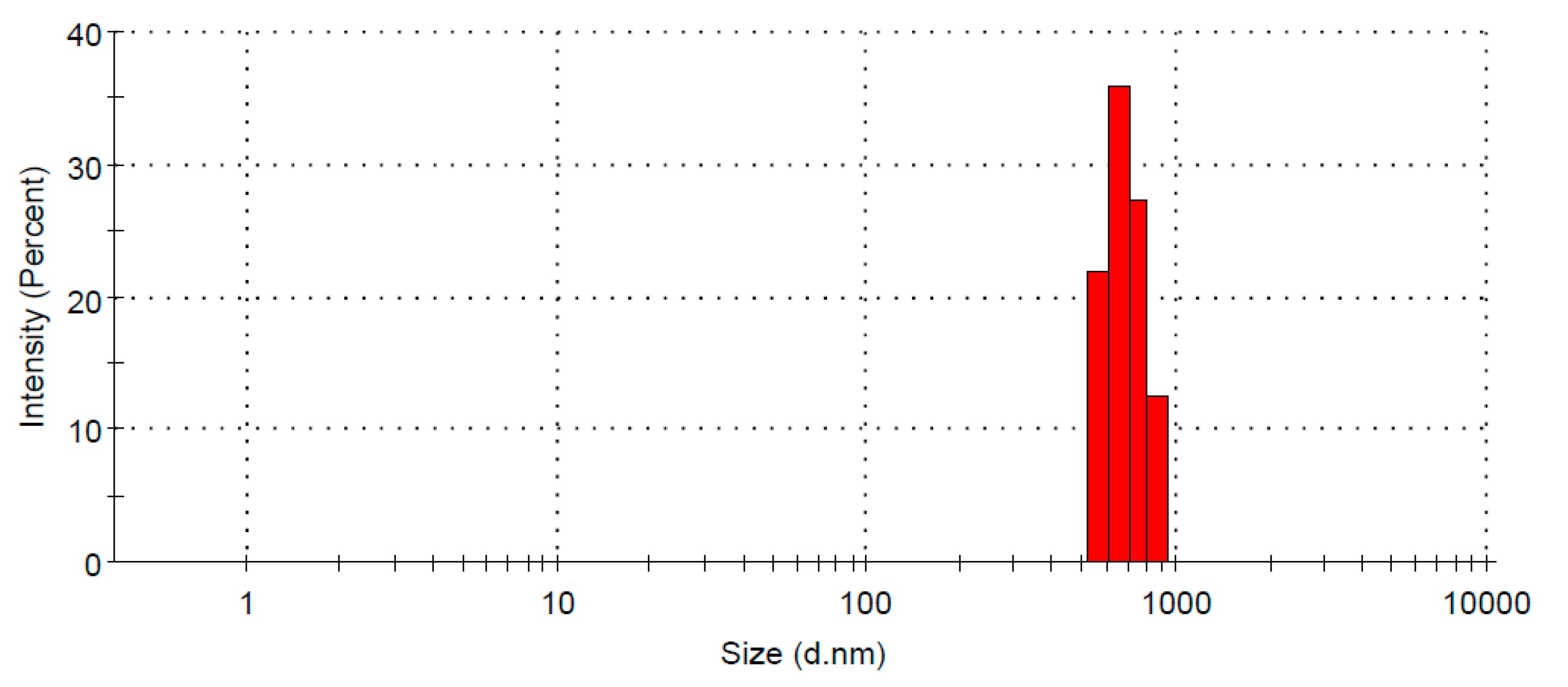
2.4.2. Particle Size
2.4.3. Entrapment Efficiency
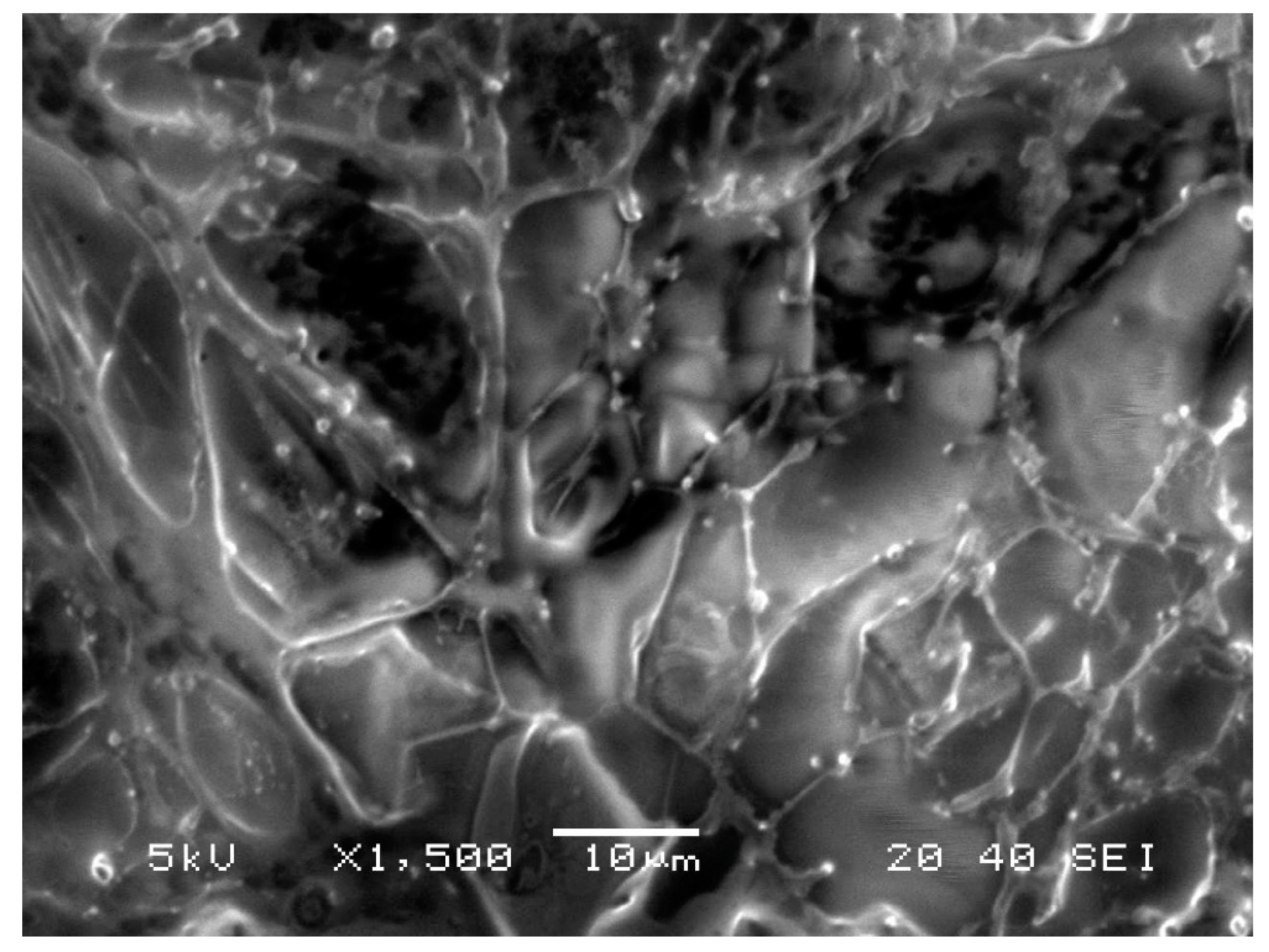
2.4.4. Scanning Electron Microscopy
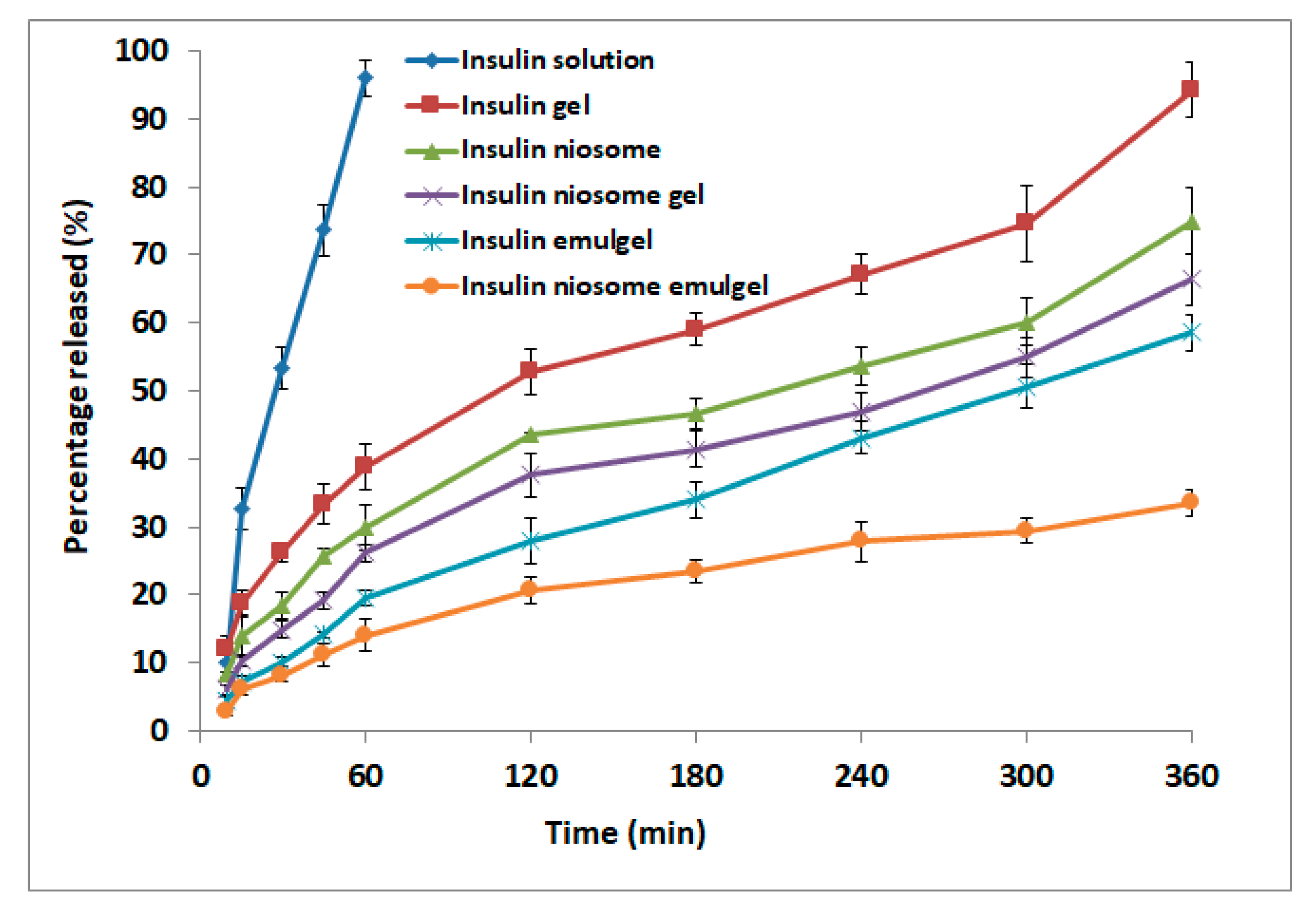
2.5. Drug Release and Kinetics
2.6. Preparation of Rat Skin
2.7. Permeation of Insulin
2.8. In Vivo Antidiabetic Activity
2.8.1. Animals
2.8.2. Antidiabetic Study
2.9. Statistics
3. Results and Discussion
3.1. Physical Characteristics of the Prepared Formulations
3.2. Analysis of 23 Factorial Design
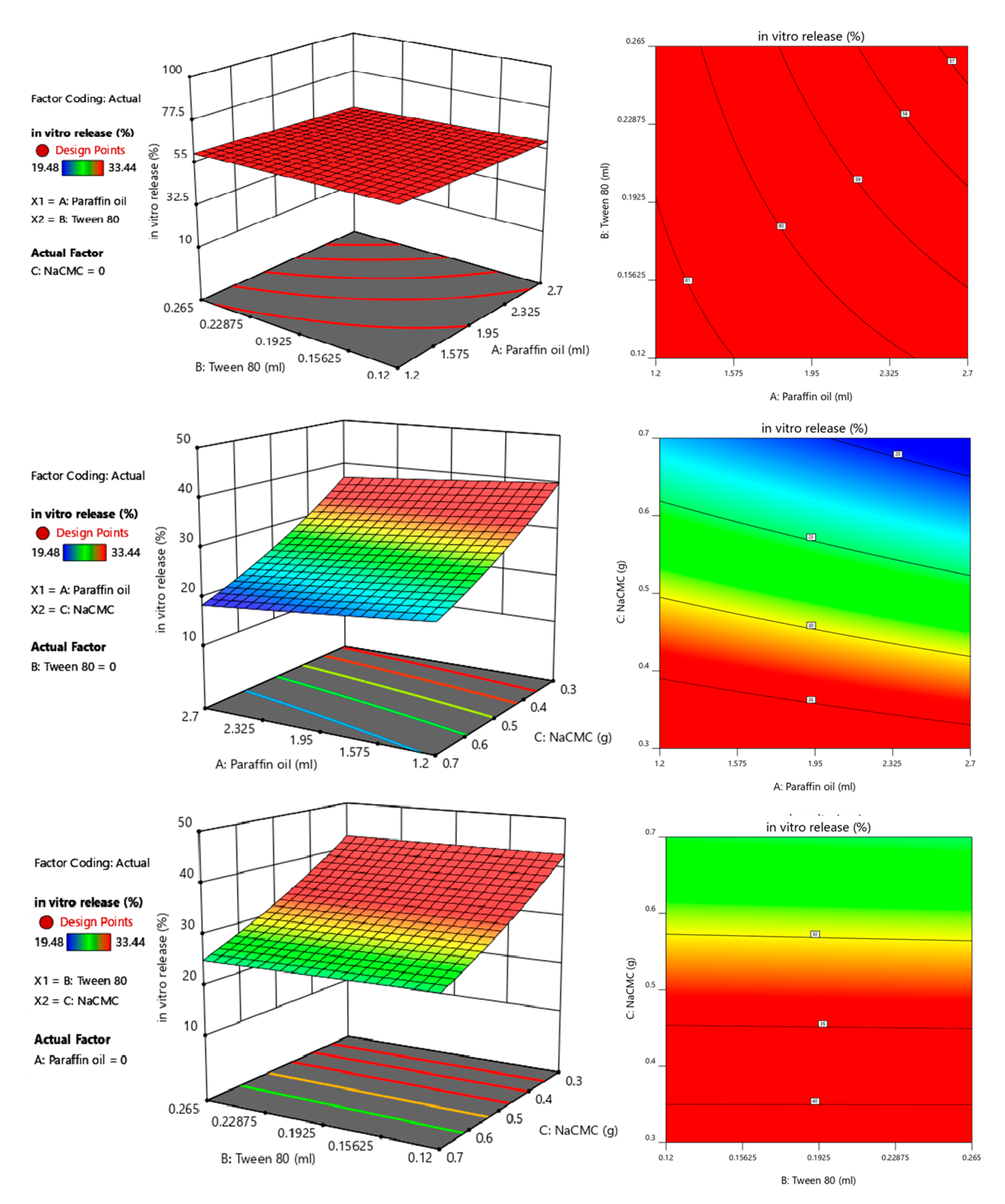
3.3. Effect of Independent Variables on Viscosity and In Vitro Release Studies
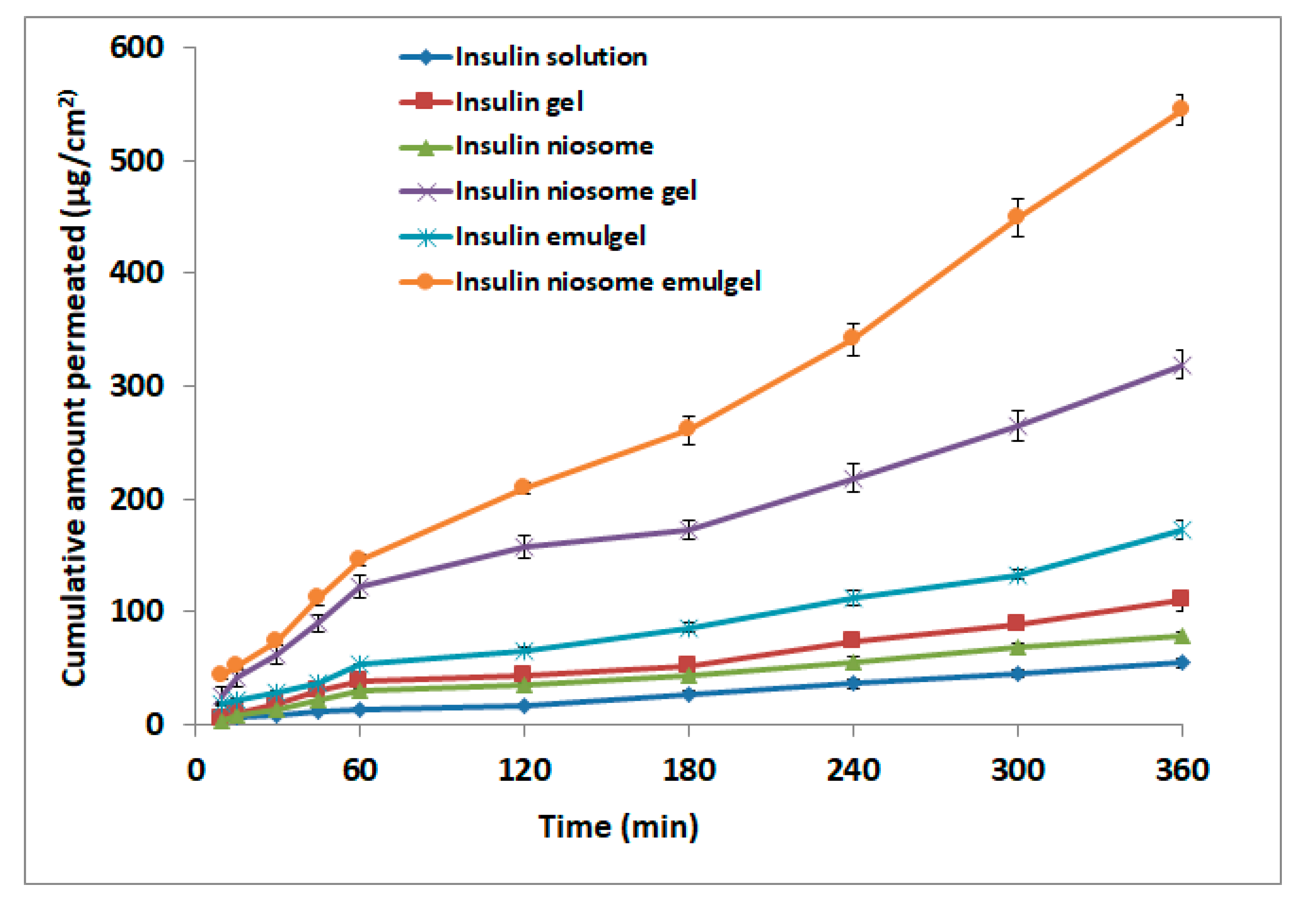
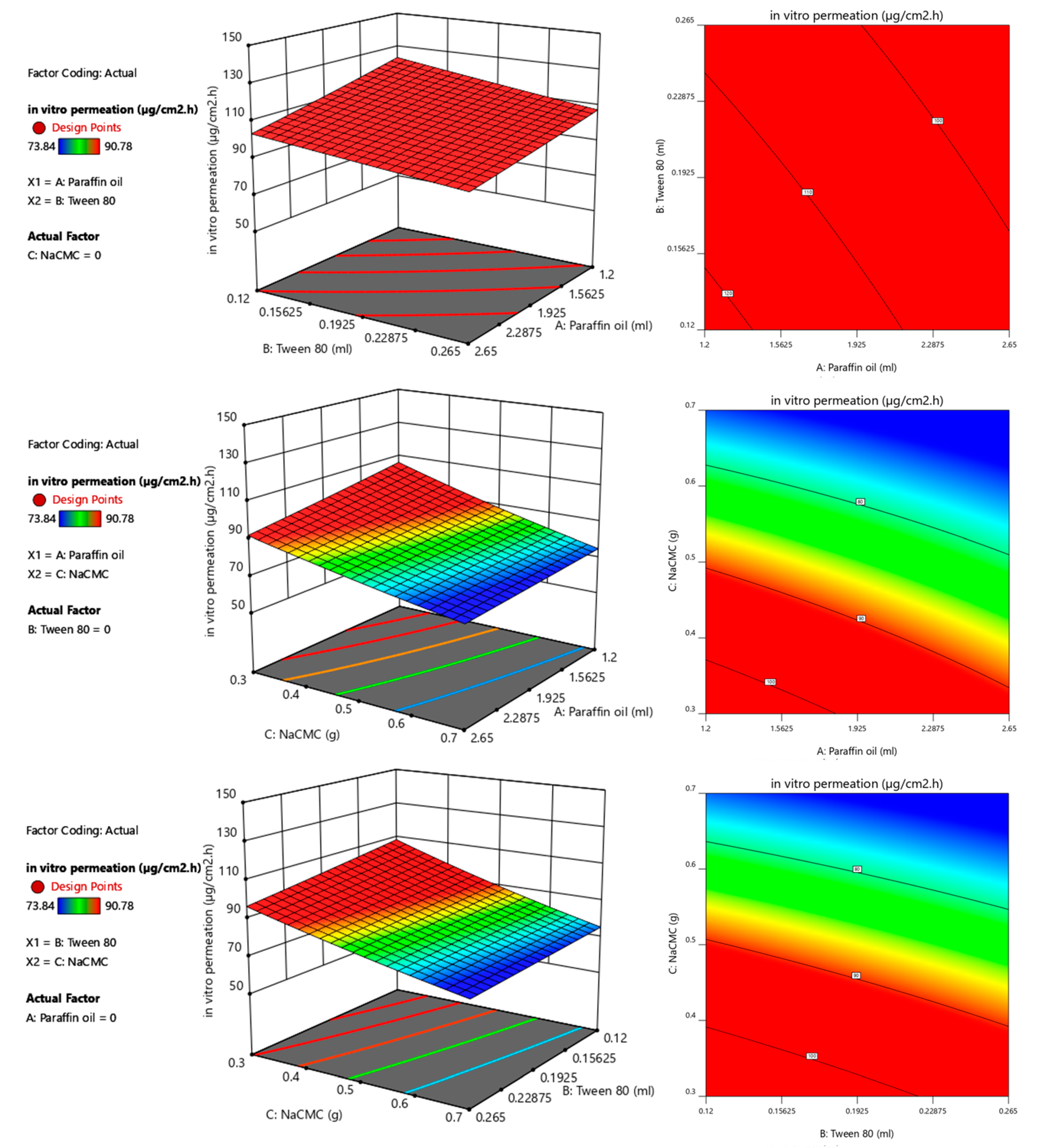
3.4. Permeation
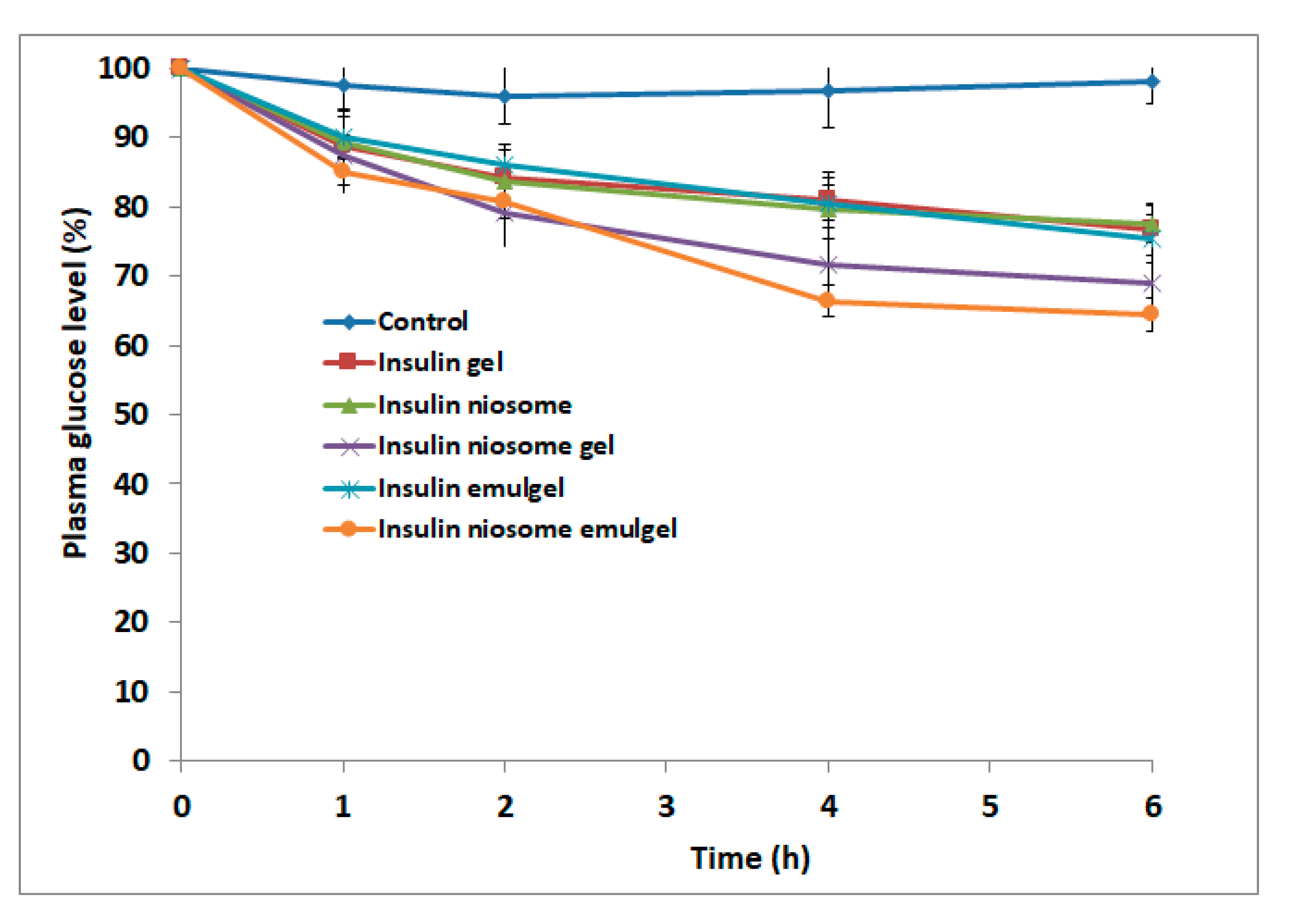
3.5. In Vivo
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nair, A.B.; Shah, J.; Aljaeid, B.M.; Al-Dhubiab, B.E.; Jacob, S. Gellan gum-based hydrogel for the transdermal delivery of nebivolol: Optimization and evaluation. Polymers 2019, 11, 1699. [Google Scholar] [CrossRef] [Green Version]
- Wen, H.; Jung, H.; Li, X. Drug delivery approaches in addressing clinical pharmacology-related issues: Opportunities and challenges. AAPS J. 2015, 17, 1327–1340. [Google Scholar] [CrossRef]
- Nair, A.B.; Gupta, S.; Al-Dhubiab, B.E.; Jacob, S.; Shinu, P.; Shah, J.; Morsy, M.A.; SreeHarsha, N.; Attimarad, M.; Venugopala, K.N.; et al. Effective therapeutic delivery and bioavailability enhancement of pioglitazone using drug in adhesive transdermal patch. Pharmaceutics 2019, 11, 359. [Google Scholar] [CrossRef]
- Nair, A.; Jacob, S.; Al-Dhubiab, B.; Attimarad, M.; Harsha, S. Basic considerations in the dermatokinetics of topical formulations. Braz. J. Pharm. Sci. 2013, 49, 423–434. [Google Scholar] [CrossRef] [Green Version]
- Pino, C.J.; Gutterman, J.U.; Vonwil, D.; Mitragotri, S.; Shastri, V.P. Glycosylation facilitates transdermal transport of macromolecules. Proc. Natl. Acad. Sci. USA 2012, 109, 21283–21288. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.M.; Shehata, T.M. The enhancement of transdermal permeability of water soluble drug by niosome-emulgel combination. J. Drug Deliv. Sci. Technol. 2012, 22, 353–359. [Google Scholar] [CrossRef]
- Nastiti, C.M.R.R.; Ponto, T.; Abd, E.; Grice, J.E.; Benson, H.A.E.; Roberts, M.S. Topical nano and microemulsions for skin delivery. Pharmaceutics 2017, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Gil’deeva, G.N.; Yurkov, V.I. Microemulsions as Potential bases for formulating modern transdermal therapeutics. Pharm. Chem. J. 2018, 52, 550–552. [Google Scholar] [CrossRef]
- Muzzalupo, R.; Tavano, L. Niosomal drug delivery for transdermal targeting: Recent advances. Res. Rep. Transdermal Drug Deliv. 2015, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- Pradhan, M.; Srivastava, S.; Singh, D.; Saraf, S.; Saraf, S.; Singh, M.R. Perspectives of lipid-based drug carrier systems for transdermal delivery. Crit. Rev. Ther. Drug Carr. Syst. 2018, 35, 331–367. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, H.; Banga, A.K. Transdermal delivery of proteins. AAPS PharmSciTech 2011, 12, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Alkilani, A.Z.; McCrudden, M.T.C.; Donnelly, R.F. Transdermal drug delivery: Innovative pharmaceutical developments based on disruption of the barrier properties of the stratum corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rai, S.; Pandey, V.; Rai, G. Transfersomes as versatile and flexible nano-vesicular carriers in skin cancer therapy: The state of the art. Nano Rev. Exp. 2017, 8, 1325708. [Google Scholar] [CrossRef] [PubMed]
- Aziz, D.E.; Abdelbary, A.A.; Elassasy, A.I. Implementing central composite design for developing transdermal diacerein-loaded niosomes: Ex vivo permeation and in vivo deposition. Curr. Drug Deliv. 2018, 15, 1330–1342. [Google Scholar] [CrossRef]
- Jacob, S.; Nair, A.B.; Al-Dhubiab, B.E. Preparation and evaluation of niosome gel containing acyclovir for enhanced dermal deposition. J. Liposome Res. 2017, 27, 283–292. [Google Scholar] [CrossRef]
- Upadhyay, R.K. Drug delivery systems, CNS protection, and the blood brain barrier. BioMed Res. Int. 2014, 2014, 869269. [Google Scholar] [CrossRef] [Green Version]
- Shah, H.; Nair, A.B.; Shah, J.; Bharadia, P.; Al-Dhubiab, B.E. Proniosomal gel for transdermal delivery of lornoxicam: Optimization using factorial design and in vivo evaluation in rats. DARU J. Pharm. Sci. 2019, 27, 59–70. [Google Scholar] [CrossRef]
- Jacob, S.; Morsy, M.A.; Nair, A. An overview on the insulin preparations and devices. Indian J. Pharm. Educ. Res. 2018, 52, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Gilroy, C.A.; Luginbuhl, K.M.; Chilkoti, A. Controlled release of biologics for the treatment of type 2 diabetes. J. Control. Release Off. J. Control. Release Soc. 2016, 240, 151–164. [Google Scholar] [CrossRef] [Green Version]
- Ng, L.C.; Gupta, M. Transdermal drug delivery systems in diabetes management: A review. Asian J. Pharm. Sci. 2020, 15, 13–25. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J.; Kahkoska, A.R.; Wang, J.; Buse, J.B.; Gu, Z. Advances in transdermal insulin delivery. Adv. Drug Deliv. Rev. 2019, 139, 51–70. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.C.; Shukla, S.; Skoog, S.A.; Boehm, R.D.; Narayan, R.J. Current advancements in transdermal biosensing and targeted drug delivery. Sensors 2019, 19, 1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.M.; Shehata, T.M. Tramadol HCl encapsulated niosomes for extended analgesic effect following oral administration. J. Drug Deliv. Sci. Technol. 2018, 46, 14–18. [Google Scholar] [CrossRef]
- Al-Dhubiab, B.E.; Nair, A.B.; Kumria, R.; Attimarad, M.; Harsha, S. Development and evaluation of buccal films impregnated with selegiline-loaded nanospheres. Drug Deliv. 2016, 23, 2154–2162. [Google Scholar] [CrossRef] [Green Version]
- Malakar, J.; Sen, S.O.; Nayak, A.K.; Sen, K.K. Formulation, optimization and evaluation of transferosomal gel for transdermal insulin delivery. Saudi Pharm. J. 2012, 20, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Morsy, M.A.; Nair, A.B. Prevention of rat liver fibrosis by selective targeting of hepatic stellate cells using hesperidin carriers. Int. J. Pharm. 2018, 552, 241–250. [Google Scholar] [CrossRef]
- Shah, J.; Nair, A.B.; Jacob, S.; Patel, R.K.; Shah, H.; Shehata, T.M.; Morsy, M.A. Nanoemulsion based vehicle for effective ocular delivery of moxifloxacin using experimental design and pharmacokinetic study in rabbits. Pharmaceutics 2019, 11, 230. [Google Scholar] [CrossRef] [Green Version]
- Morsy, M.A.; Abdel-Latif, R.G.; Nair, A.B.; Venugopala, K.N.; Ahmed, A.F.; Elsewedy, H.S.; Shehata, T.M. Preparation and evaluation of atorvastatin-loaded nanoemulgel on wound-healing efficacy. Pharmaceutics 2019, 11, 609. [Google Scholar] [CrossRef] [Green Version]
- Anroop, B.; Ghosh, B.; Parcha, V.; Kumar, A.; Khanam, J. Synthesis and comparative skin permeability of atenolol and propranolol esters. J. Drug Deliv. Sci. Technol. 2005, 15, 187–190. [Google Scholar] [CrossRef]
- Vora, B.; Khopade, A.J.; Jain, N.K. Proniosome based transdermal delivery of levonorgestrel for effective contraception. J. Control. Release 1998, 54, 149–165. [Google Scholar] [CrossRef]
- Pillai, O.; Panchagnula, R. Transdermal delivery of insulin from poloxamer gel: Ex vivo and in vivo skin permeation studies in rat using iontophoresis and chemical enhancers. J. Control. Release 2003, 89, 127–140. [Google Scholar] [CrossRef]
- Nair, A.B.; Jacob, S.; Al-Dhubiab, B.E.; Alhumam, R.N. Influence of skin permeation enhancers on the transdermal delivery of palonosetron: An in vitro evaluation. J. Appl. Biomed. 2018, 16, 192–197. [Google Scholar] [CrossRef]
- Escudero, I.; Geanta, R.M.; Ruiz, M.O.; Benito, J.M. Formulation and characterization of Tween 80/cholestherol niosomes modified with tri-n-octylmethylammonium chloride (TOMAC) for carboxylic acids entrapment. Colloids Surf A Physicochem. Eng. Asp. 2014, 461, 167–177. [Google Scholar] [CrossRef]
- Mohammed, F.A. Topical permeation characteristics of diclofenac sodium from NaCMC gels in comparison with conventional gel formulations. Drug Dev. Ind. Pharm. 2001, 27, 1083–1097. [Google Scholar] [CrossRef]
- Nair, A.; Reddy, C.; Jacob, S. Delivery of a classical antihypertensive agent through the skin by chemical enhancers and iontophoresis. Ski. Res. Technol. 2009, 15, 187–194. [Google Scholar] [CrossRef]
- Agarwal, R.; Katare, O.P.; Vyas, S.P. Preparation and in vitro evaluation of liposomal/niosomal delivery systems for antipsoriatic drug dithranol. Int. J. Pharm. 2001, 228, 43–52. [Google Scholar] [CrossRef]
- Torin Huzil, J.; Sivaloganathan, S.; Kohandel, M.; Foldvari, M. Drug delivery through the skin: Molecular simulations of barrier lipids to design more effective noninvasive dermal and transdermal delivery systems for small molecules, biologics, and cosmetics. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2011, 3, 449–462. [Google Scholar] [CrossRef]
- Shah, J.; Nair, A.B.; Shah, H.; Jacob, S.; Shehata, T.M.; Morsy, M.A. Enhancement in antinociceptive and anti-inflammatory effects of tramadol by transdermal proniosome gel. Asian J. Pharm. Sci. 2019. [Google Scholar] [CrossRef]
- Som, I.; Bhatia, K.; Yasir, M. Status of surfactants as penetration enhancers in transdermal drug delivery. J. Pharm. Bioallied Sci. 2012, 4, 2–9. [Google Scholar] [CrossRef]
- Shokri, J.; Azarmi, S.; Fasihi, Z.; Hallaj-Nezhadi, S.; Nokhodchi, A.; Javadzadeh, Y. Effects of various penetration enhancers on percutaneous absorption of piroxicam from emulgels. Res. Pharm. Sci. 2012, 7, 225–234. [Google Scholar]
- Nair, A.; Morsy, M.A.; Jacob, S. Dose translation between laboratory animals and human in preclinical and clinical phases of drug development. Drug Dev. Res. 2018, 79, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, N.S.; Shobha Rani, R.H. Physicochemical and pharmacokinetic parameters in drug selection and loading for transdermal drug delivery. Indian J. Pharm. Sci. 2008, 70, 94–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Insulin Gel | Insulin Niosome | Insulin Niosome Gel | Insulin Emulgel | Insulin Niosome Emulgel |
|---|---|---|---|---|---|
| Insulin (mL) * | 4 | 0 | 0 | 4 | 0 |
| Sodium carboxymethyl cellulose (g) | 0.4 | – | 0.4 | 0.4 | 0.4 |
| Liquid paraffin (mL) | 0 | 0 | 0 | 1.25 | 1.25 |
| Tween 80 (mL) | 0 | 0 | 0 | 0.125 | 0.125 |
| Niosomes-loaded insulin (mL) * | 0 | 4 | 4 | 0 | 4 |
| Buffer pH 7.4 Q.S. to (g) | 10 | 10 | 10 | 10 | 10 |
| Independent Variables in Coded and Actual Values | ||||||
|---|---|---|---|---|---|---|
| Formulation No. | X1 (Conc. of Paraffin Oil (mL)) | X2 (Conc. of Paraffin Oil (mL)) | X3 (Conc. of Sodium Carboxymethyl Cellulose (g)) | |||
| Coded | Actual | Coded | Actual | Coded | Actual | |
| F1 | 1 | 2.5 | −1 | 0.125 | −1 | 0.4 |
| F2 | −1 | 1.25 | −1 | 0.125 | 1 | 0.6 |
| F3 | 1 | 2.5 | 1 | 0.25 | −1 | 0.4 |
| F4 | −1 | 1.25 | 1 | 0.25 | −1 | 0.4 |
| F5 | 1 | 2.5 | 1 | 0.25 | 1 | 0.6 |
| F6 | −1 | 1.25 | −1 | 0.125 | −1 | 0.4 |
| F7 | 1 | 2.5 | −1 | 0.125 | 1 | 0.6 |
| F8 | −1 | 1.25 | 1 | 0.25 | 1 | 0.6 |
| Property | Insulin Gel | Insulin Niosome | Insulin Niosome Gel | Insulin Emulgel | Insulin Niosome Emulgel |
|---|---|---|---|---|---|
| Viscosity (cP) | 6550 ± 50 | 2150 ± 75 | 8220 ± 80 | 11,050 ± 50 | 12,250 ± 70 |
| Check Point Batch | Responses | |||||
|---|---|---|---|---|---|---|
| In Vitro Release (%) | Viscosity (cP) | Cumulative Amount Permeated (µg/cm2) | ||||
| Predicted | Observed | Predicted | Observed | Predicted | Observed | |
| F9 | 26.79 | 27.38 | 18,397 | 18,529 | 82.85 | 83.43 |
| Formulation | Zero Order (R2) | First-Order (R2) | Higuchi Model (R2) | Order |
|---|---|---|---|---|
| Insulin solution | 0.9819 | 0.7157 | 0.9130 | Zero |
| Insulin gel | 0.9242 | 0.4780 | 0.9896 | Higuchi |
| Insulin niosome | 0.9282 | 0.5246 | 0.9850 | Higuchi |
| Insulin niosome gel | 0.9421 | 0.5786 | 0.9866 | Higuchi |
| Insulin emulgel | 0.9482 | 0.6694 | 0.9838 | Higuchi |
| Insulin niosome emulgel | 0.9236 | 0.6288 | 0.9918 | Higuchi |
| Time | Insulin Solution | Insulin Gel | Insulin Niosome | Insulin Niosome Gel | Insulin Emulgel | Insulin Niosome Emulgel |
|---|---|---|---|---|---|---|
| SSTF (µg/cm2/h) | 9.06 | 18.39 | 13.17 | 53.11 | 28.72 | 90.78 |
| ER | 1.00 | 2.03 | 1.45 | 5.86 | 3.17 | 10.02 |
| Mechanism | Zero | Zero | Higuchi | Higuchi | Zero | Zero |
| R2 | 0.986 | 0.967 | 0.973 | 0.976 | 0.982 | 0.989 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shehata, T.M.; Nair, A.B.; Al-Dhubiab, B.E.; Shah, J.; Jacob, S.; Alhaider, I.A.; Attimarad, M.; Elsewedy, H.S.; Ibrahim, M.M. Vesicular Emulgel Based System for Transdermal Delivery of Insulin: Factorial Design and in Vivo Evaluation. Appl. Sci. 2020, 10, 5341. https://0-doi-org.brum.beds.ac.uk/10.3390/app10155341
Shehata TM, Nair AB, Al-Dhubiab BE, Shah J, Jacob S, Alhaider IA, Attimarad M, Elsewedy HS, Ibrahim MM. Vesicular Emulgel Based System for Transdermal Delivery of Insulin: Factorial Design and in Vivo Evaluation. Applied Sciences. 2020; 10(15):5341. https://0-doi-org.brum.beds.ac.uk/10.3390/app10155341
Chicago/Turabian StyleShehata, Tamer M., Anroop B. Nair, Bandar E. Al-Dhubiab, Jigar Shah, Shery Jacob, Ibrahim A. Alhaider, Mahesh Attimarad, Heba S. Elsewedy, and Mahmoud M. Ibrahim. 2020. "Vesicular Emulgel Based System for Transdermal Delivery of Insulin: Factorial Design and in Vivo Evaluation" Applied Sciences 10, no. 15: 5341. https://0-doi-org.brum.beds.ac.uk/10.3390/app10155341