COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images

 , , , and
, , , and 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
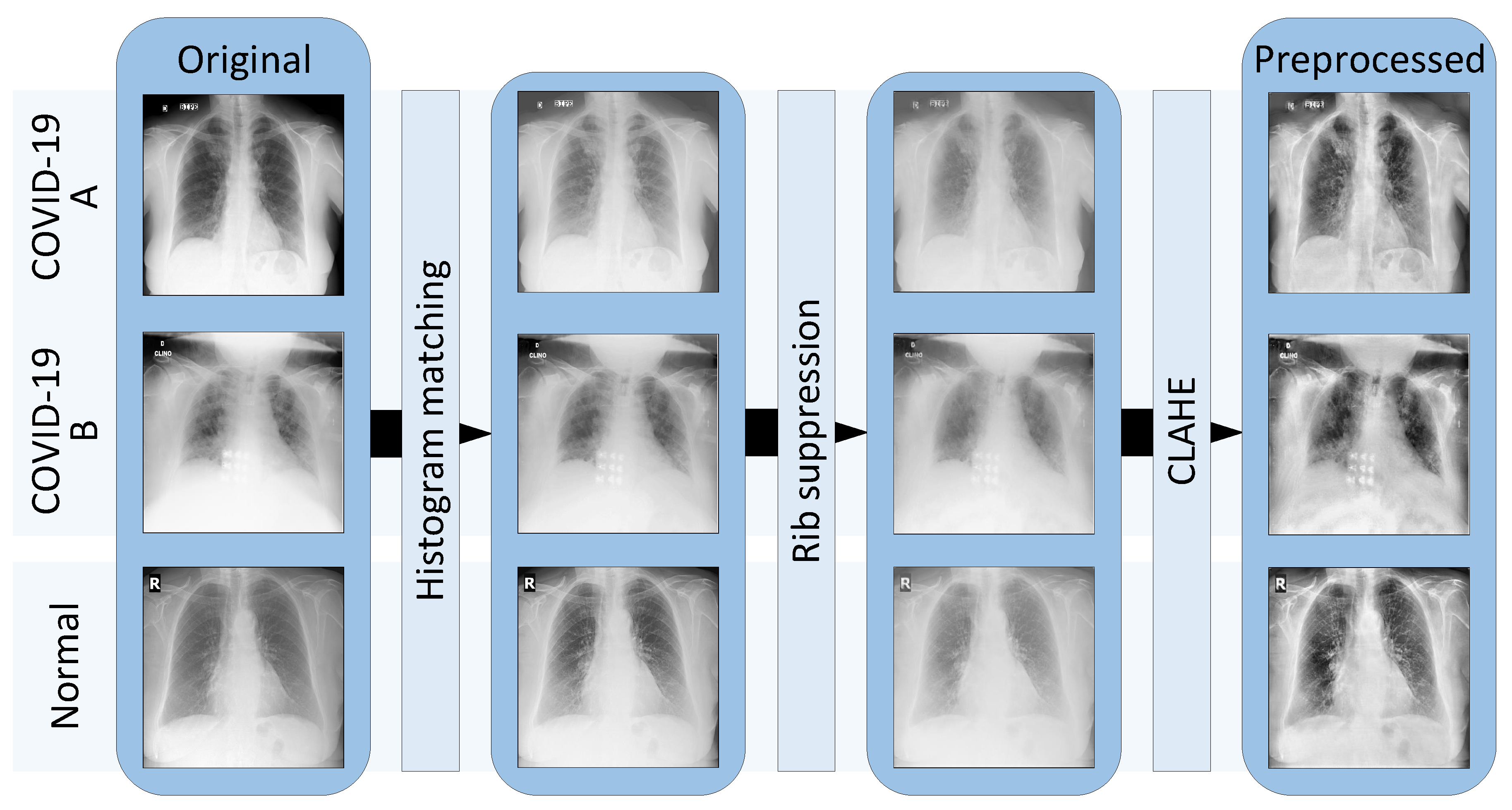
2.2.1. Preprocessing Step
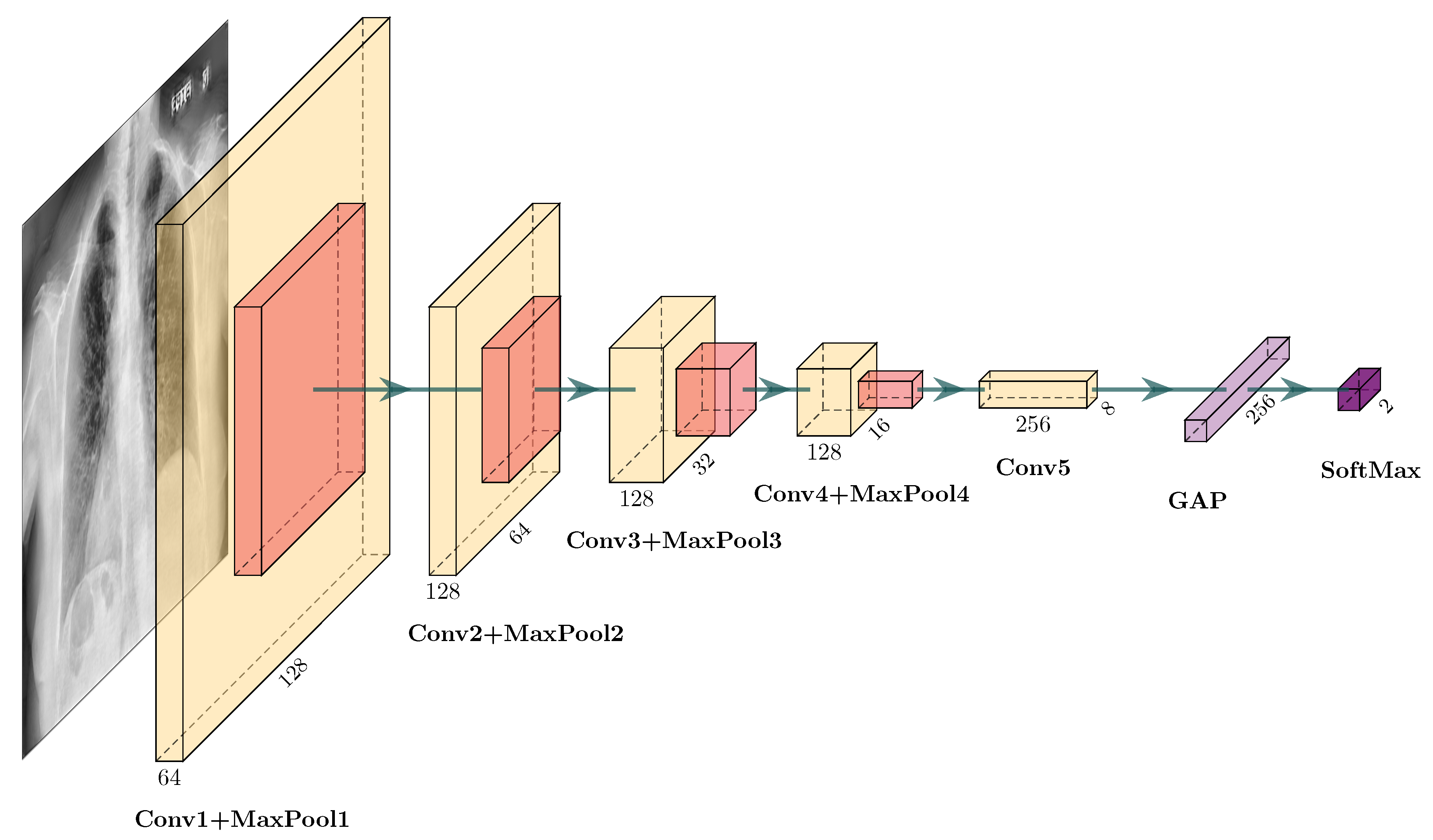
2.2.2. Convolutional Neural Network
2.2.3. Training and Testing the Network
2.2.4. Performance Metrics
2.2.5. Class Activation Maps
2.2.6. Post-Processing
3. Results and Discussion
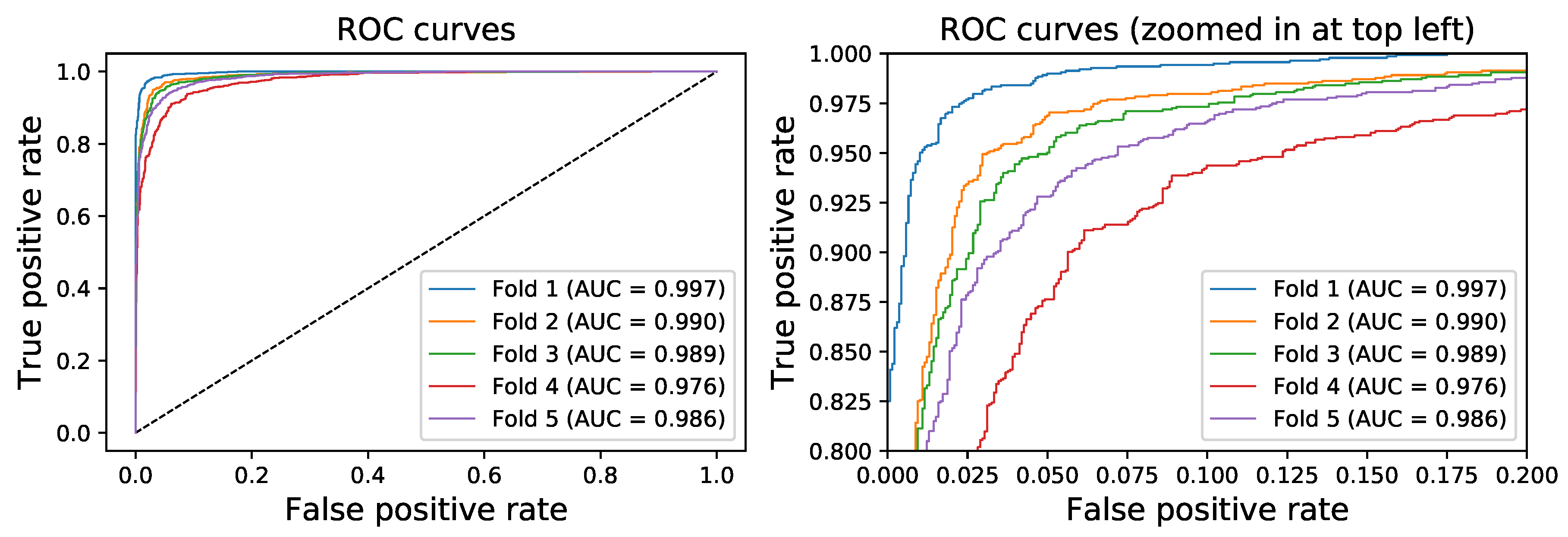
3.1. Quantitative Evaluation
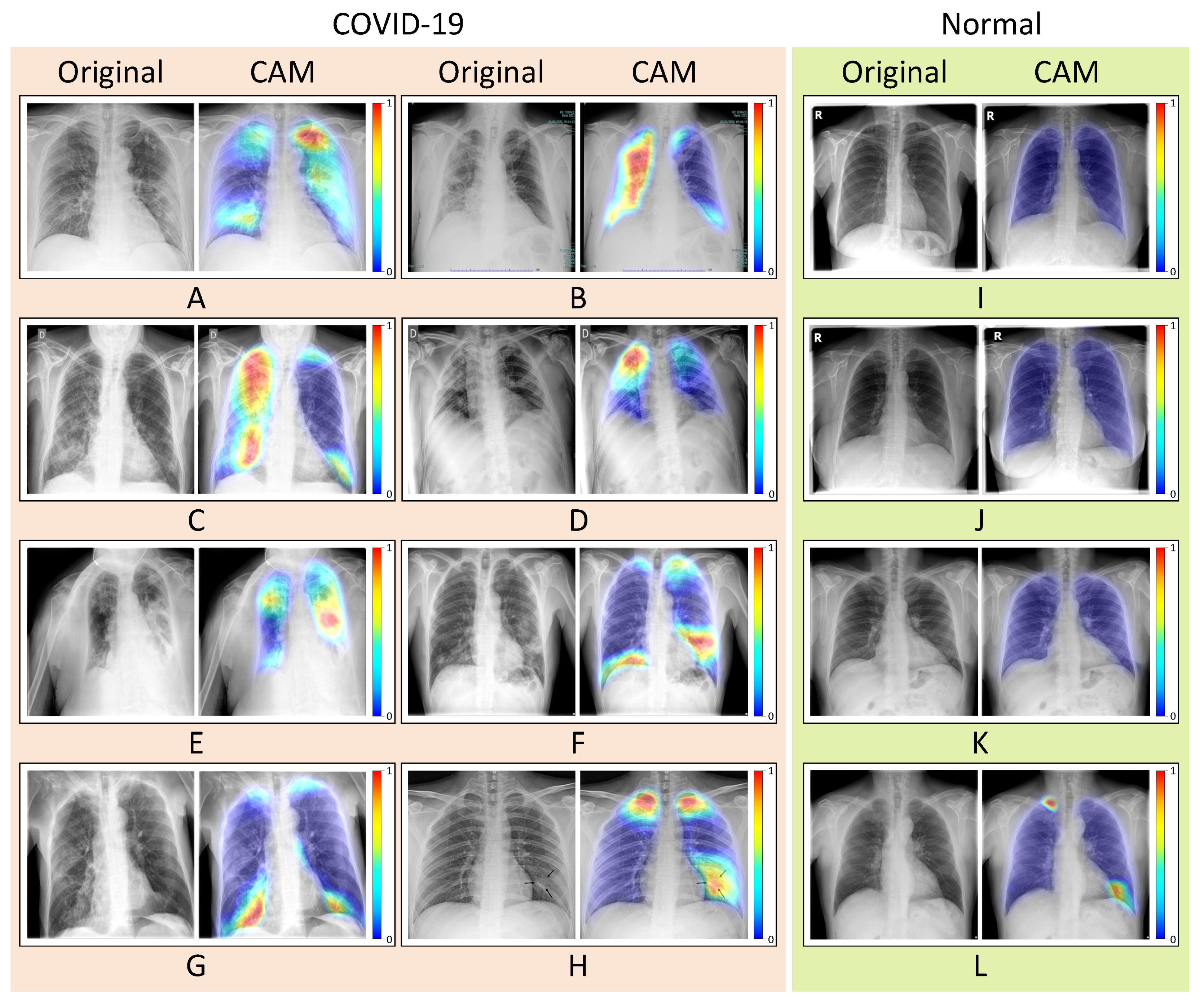
3.2. Qualitative Evaluation
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AP | Anteroposterior |
| AI | Artificial Intelligence |
| AUC | Area Under Curve |
| CAD | Computer-Aided Diagnosis |
| CAM | Class Activation Map |
| CLAHE | Contrast Limited Adaptive Histogram Equalization |
| CNN | Convolutional Neural Network |
| CoV | Coronavirus |
| COVID-19 | Coronavirus Disease 2019 |
| CT | Computer Tomography |
| DL | Deep Learning |
| GAP | Global Average Pooling |
| MERS | Middle East respiratory syndrome |
| PA | Posteroanterior |
| RSNA | Radiological Society of North America |
| ROC | Receiver Operating Characteristic |
| RT-LAMP | Reverse-Transcription Loop-Mediated Isothermal Amplification |
| RT-PCR | Reverse-Transcription Polymerase Chain Reaction |
| rRT-PCT | real-time RT-PCR |
| SARS | Severe Acute Respiratory Syndrome |
References
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 16 August 2020).
- Cui, J.; Li, F.; Shi, Z.L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Momattin, H.; Al-Ali, A.Y.; Al-Tawfiq, J.A. A Systematic Review of therapeutic agents for the treatment of the Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Travel Med. Infect. Dis. 2019, 30, 9–18. [Google Scholar] [CrossRef]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Kaler, J.; Tabrez, E.; Tabrez, S.; Tabrez, S.S. Novel COVID-19: A comprehensive review of transmission, manifestation, and pathogenesis. Cureus 2020, 12, e8184. [Google Scholar]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J. Med. Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 92, 200432. [Google Scholar] [CrossRef]
- Lin, E.C. Radiation risk from medical imaging. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2010; Volume 85, pp. 1142–1146. [Google Scholar]
- Lu, W.; Zhang, S.; Chen, B.; Chen, J.; Xian, J.; Lin, Y.; Shan, H.; Su, Z.Z. A clinical study of noninvasive assessment of lung lesions in patients with coronavirus disease-19 (COVID-19) by bedside ultrasound. Ultraschall Med. Eur. J. Ultrasound 2020, 41, 300–307. [Google Scholar] [CrossRef]
- Self, W.H.; Courtney, D.M.; McNaughton, C.D.; Wunderink, R.G.; Kline, J.A. High discordance of chest X-ray and computed tomography for detection of pulmonary opacities in ED patients: Implications for diagnosing pneumonia. Am. J. Emerg. Med. 2013, 31, 401–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Ratnapalan, S.; Bentur, Y.; Koren, G. Doctor, will that X-ray harm my unborn child? Cmaj 2008, 179, 1293–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Fang, C.; Huang, D.; Huang, L.Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Civit-Masot, J.; Luna-Perejón, F.; Domínguez Morales, M.; Civit, A. Deep Learning system for COVID-19 diagnosis aid using X-ray pulmonary images. Appl. Sci. 2020, 10, 4640. [Google Scholar] [CrossRef]
- Duran-Lopez, L.; Dominguez-Morales, J.P.; Conde-Martin, A.F.; Vicente-Diaz, S.; Linares-Barranco, A. PROMETEO: A CNN-based computer-aided diagnosis System for WSI prostate cancer detection. IEEE Access 2020, 8, 128613–128628. [Google Scholar] [CrossRef]
- Dominguez-Morales, J.P.; Jimenez-Fernandez, A.F.; Dominguez-Morales, M.J.; Jimenez-Moreno, G. Deep neural networks for the recognition and classification of heart murmurs using neuromorphic auditory sensors. IEEE Trans. Biomed. Circuits Syst. 2017, 12, 24–34. [Google Scholar] [CrossRef]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, B.; Tucker, A. Estimating uncertainty and interpretability in deep learning for coronavirus (COVID-19) detection. arXiv 2020, arXiv:2003.10769. [Google Scholar]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. arXiv 2020, arXiv:2003.10849. [Google Scholar]
- Zhang, J.; Xie, Y.; Li, Y.; Shen, C.; Xia, Y. COVID-19 screening on chest X-ray images using deep learning based anomaly detection. arXiv 2020, arXiv:2003.12338. [Google Scholar]
- Wang, L.; Wong, A. Covid-net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. arXiv 2020, arXiv:2003.09871. [Google Scholar]
- Vayá, M.D.L.I.; Saborit, J.M.; Montell, J.A.; Pertusa, A.; Bustos, A.; Cazorla, M.; Galant, J.; Barber, X.; Orozco-Beltrán, D.; Garcia, F.; et al. BIMCV COVID-19+: A large annotated dataset of RX and CT images from COVID-19 patients. arXiv 2020, arXiv:2006.01174. Available online: https://bimcv.cipf.es/bimcv-projects/bimcv-covid19/ (accessed on 16 August 2020).
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 image data collection. arXiv 2020, arXiv:2003.11597. Available online: https://github.com/ieee8023/covid-chestxray-dataset (accessed on 16 August 2020).
- Bustos, A.; Pertusa, A.; Salinas, J.M.; de la Iglesia-Vayá, M. Padchest: A large chest X-ray image dataset with multi-label annotated reports. arXiv 2019, arXiv:1901.07441. Available online: https://bimcv.cipf.es/bimcv-projects/padchest/ (accessed on 16 August 2020).
- Gonzales, R.C.; Woods, R.E. Digital Image Processing; Prentice Hall: Upper Saddle River, NJ, USA, 2002. [Google Scholar]
- Qin, C.; Yao, D.; Shi, Y.; Song, Z. Computer-aided detection in chest radiography based on artificial intelligence: A survey. Biomed. Eng. Online 2018, 17, 113. [Google Scholar] [CrossRef] [Green Version]
- Soleymanpour, E.; Pourreza, H.R. Fully automatic lung segmentation and rib suppression methods to improve nodule detection in chest radiographs. J. Med. Signals Sens. 2011, 1, 191. [Google Scholar] [CrossRef] [Green Version]
- Oda, S.; Awai, K.; Suzuki, K.; Yanaga, Y.; Funama, Y.; MacMahon, H.; Yamashita, Y. Performance of radiologists in detection of small pulmonary nodules on chest radiographs: Effect of rib suppression with a massive-training artificial neural network. Am. J. Roentgenol. 2009, 193, W397–W402. [Google Scholar] [CrossRef] [Green Version]
- Gordienko, Y.; Gang, P.; Hui, J.; Zeng, W.; Kochura, Y.; Alienin, O.; Rokovyi, O.; Stirenko, S. Deep learning with lung segmentation and bone shadow exclusion techniques for chest X-ray analysis of lung cancer. In Advances in Intelligent Systems and Computing, Proceedings of the International Conference on Computer Science, Engineering and Education Applications, Kiev, Ukraine, 18–20 January 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 638–647. [Google Scholar]
- Gusarev, M.; Kuleev, R.; Khan, A.; Rivera, A.R.; Khattak, A.M. Deep learning models for bone suppression in chest radiographs. In Proceedings of the 2017 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), Manchester, UK, 23–25 August 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–7. [Google Scholar]
- Reza, A.M. Realization of the contrast limited adaptive histogram equalization (CLAHE) for real-time image enhancement. J. VLSI Signal Process. Syst. Signal Image Video Technol. 2004, 38, 35–44. [Google Scholar] [CrossRef]
- Zeiler, M.D. Adadelta: An adaptive learning rate method. arXiv 2012, arXiv:1212.5701. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Object detectors emerge in deep scene CNNs. arXiv 2014, arXiv:1412.6856. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning deep features for discriminative localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Lecture Notes in Computer Science, Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fold Test | Actual Classes | Predicted Classes | Sensitivity | Specificity | Precision | F1-Score | AUC | Balanced Accuracy | |
|---|---|---|---|---|---|---|---|---|---|
| Normal | COVID-19 | ||||||||
| 1st fold | Normal | 851 | 16 | 96.71% | 98.15% | 96.89% | 96.8% | 0.997 | 97.43% |
| 98.15% | 1.85% | ||||||||
| COVID-19 | 17 | 499 | |||||||
| 3.29% | 96.71% | ||||||||
| 2nd fold | Normal | 839 | 28 | 94.00% | 96.77% | 94.54% | 94.27% | 0.990 | 95.38% |
| 96.77% | 3.23% | ||||||||
| COVID-19 | 31 | 485 | |||||||
| 6% | 94% | ||||||||
| 3rd fold | Normal | 834 | 33 | 93.02% | 96.19% | 93.57% | 93.29% | 0.989 | 94.61% |
| 96.19% | 3.81% | ||||||||
| COVID-19 | 36 | 480 | |||||||
| 6.98% | 93.02% | ||||||||
| 4th fold | Normal | 815 | 52 | 88.95% | 94.00% | 89.82% | 89.39% | 0.976 | 91.48% |
| 94% | 6% | ||||||||
| COVID-19 | 57 | 459 | |||||||
| 11.05% | 88.95% | ||||||||
| 5th fold | Normal | 839 | 30 | 90% | 96.55% | 93.98% | 91.94% | 0.986 | 93.27% |
| 96.55% | 3.45% | ||||||||
| COVID-19 | 52 | 468 | |||||||
| 10% | 90% | ||||||||
| Average | Normal | 96.33% | 3.67% | 92.53% | 96.33% | 93.76% | 93.14% | 0.988 | 94.43% |
| COVID-19 | 7.47% | 92.53% | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duran-Lopez, L.; Dominguez-Morales, J.P.; Corral-Jaime, J.; Vicente-Diaz, S.; Linares-Barranco, A. COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images. Appl. Sci. 2020, 10, 5683. https://0-doi-org.brum.beds.ac.uk/10.3390/app10165683
Duran-Lopez L, Dominguez-Morales JP, Corral-Jaime J, Vicente-Diaz S, Linares-Barranco A. COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images. Applied Sciences. 2020; 10(16):5683. https://0-doi-org.brum.beds.ac.uk/10.3390/app10165683
Chicago/Turabian StyleDuran-Lopez, Lourdes, Juan Pedro Dominguez-Morales, Jesús Corral-Jaime, Saturnino Vicente-Diaz, and Alejandro Linares-Barranco. 2020. "COVID-XNet: A Custom Deep Learning System to Diagnose and Locate COVID-19 in Chest X-ray Images" Applied Sciences 10, no. 16: 5683. https://0-doi-org.brum.beds.ac.uk/10.3390/app10165683