Total Serum Calcium and Recovery after Rehabilitation in Patients with Stroke

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
2.2. Rehabilitation Intervention
2.3. Rehabilitation Outcome
2.4. Biochemical Analyses
2.5. Statistical Analysis
3. Results
3.1. Demographics, Clinical Characteristics, and Biochemical Status
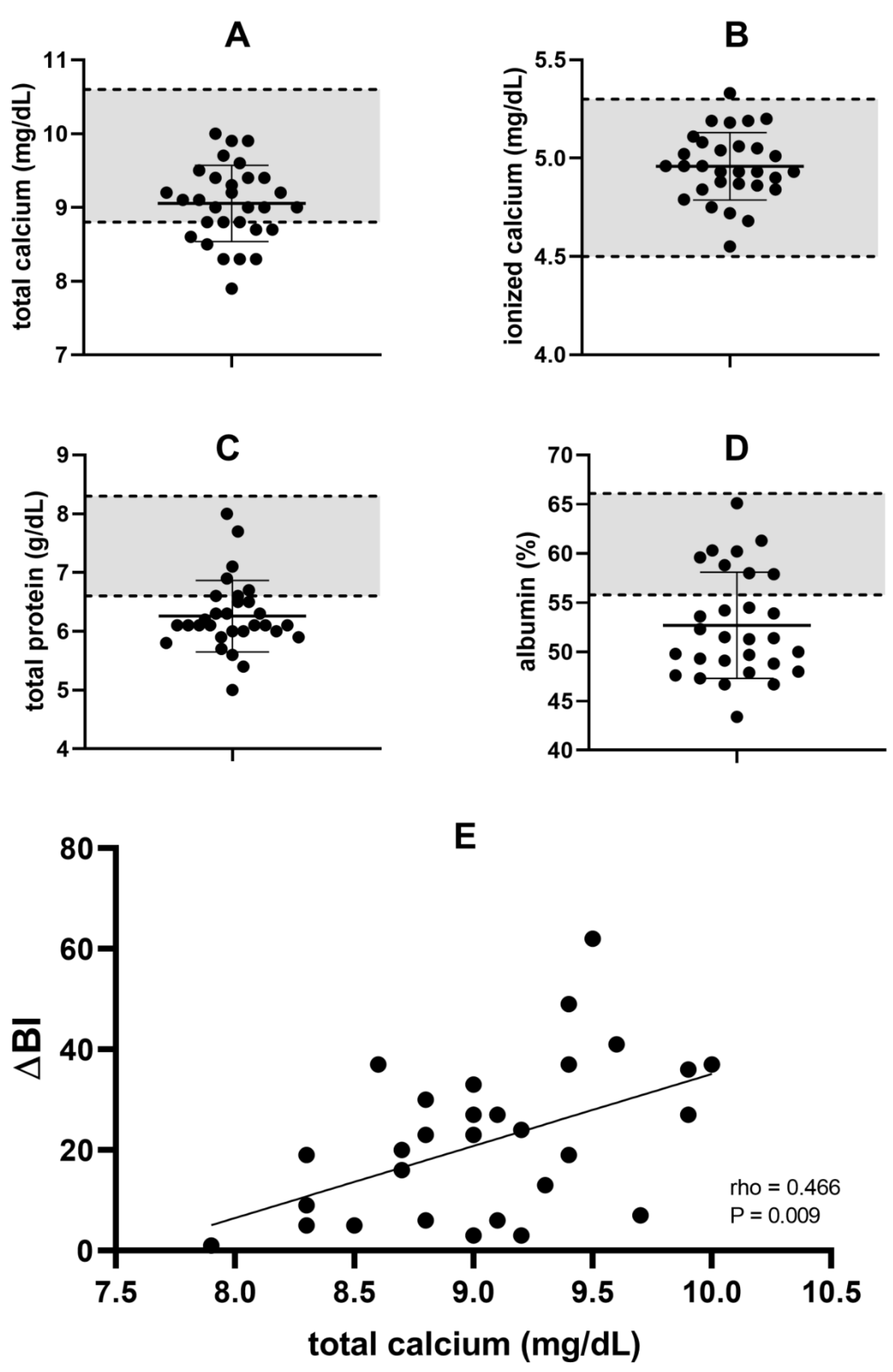
3.2. Relationship between Biochemical Status and Rehabilitation Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Executive Summary: Heart Disease and Stroke Statistics—2014 Update. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, S.; Zarahn, E.; Riley, C.; Speizer, A.; Chong, J.Y.; Lazar, R.M.; Marshall, R.S.; Krakauer, J.W. Inter-individual Variability in the Capacity for Motor Recovery After Ischemic Stroke. Neurorehabil. Neural Repair 2008, 22, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Li, Y.; Fang, J.; Lu, Q.; He, L. Risk factors for malnutrition in stroke patients: A meta-analysis. Clin. Nutr. 2019, 38, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Choue, R. Impact of nutritional status and dietary quality on stroke: Do we need specific recommendations? Eur. J. Clin. Nutr. 2013, 67, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Beto, J.A. The Role of Calcium in Human Aging. Clin. Nutr. Res. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F. The Vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Shiue, H.; Ivanov, M.; Kunze, K.; Sands, K. Low Serum Calcium and Clinical Outcomes Following Systemic Thrombolysis in Acute Ischemic Stroke. Neurology 2020, 94 (Suppl. 15), 2858. [Google Scholar]
- Ovbiagele, B.; Starkman, S.; Teal, P.; Lyden, P.; Kaste, M.; Davis, S.M.; Hacke, W.; Fierus, M.; Slaver, J.; VISTA Investigators. Serum Calcium as Prognosticator in Ischemic Stroke. Stroke 2008, 39, 2231–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Michaylova, V.; Ilkova, P. Photometric determination of micro amounts of calcium with arsenazo III. Anal. Chim. Acta 1971, 53, 194–198. [Google Scholar] [CrossRef]
- Pfitzenmeyer, P.; Martin, I.; d’Athis, P.; Grumbach, Y.; Delmestre, M.C.; Blondé-Cynober, F.; Derycke, B.; Brondel, L. A new formula for correction of total calcium level into ionized serum calcium values in very elderly hospitalized patients. Arch. Gerontol. Geriatr. 2007, 45, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Keren, D.F. Protein Electrophoresis in Clinical Diagnosis; Hodder Arnold: London, UK, 2003; pp. 1–14. ISBN 0340-81213-3. [Google Scholar]
- Ovbiagele, B.; Liebeskind, D.S.; Starkman, S.; Sanossian, N.; Kim, D.; Razinia, T.; Saver, J.L. Are elevated admission calcium levels associated with better outcomes after ischemic stroke? Neurology 2006, 67, 170–173. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, J.F.; Xiong, Z.G.; Jackson, M.F. Paradox of Ca2+ signaling, cell death and stroke. Trends Neurosci. 2006, 29, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Buck, B.H.; Liebeskind, D.S.; Saver, J.L.; Bang, O.Y.; Starkman, S.; Ali, L.K.; Kim, D.; Villablanca, J.P.; Salamon, N.; Yun, S.W.; et al. Association of higher serum calcium levels with smaller infarct volumes in acute ischemic stroke. Arch. Neurol. 2007, 64, 1287–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Wang, J.; Xu, Z. Prognostic utility of serum 25-hydroxyvitamin D in patients with stroke: A meta-analysis. J. Neurol. 2019, 267, 3177–3186. [Google Scholar] [CrossRef] [PubMed]
- Siotto, M.; Santoro, M.; Aprile, I. Vitamin D and Rehabilitation after Stroke: Status of Art. Appl. Sci. 2020, 10, 1973. [Google Scholar] [CrossRef] [Green Version]
- Gariballa, S.E.; Parker, S.G.; Taub, N.; Castleden, C.M. Influence of nutritional status on clinical outcome after acute stroke. Am. J. Clin. Nutr. 1998, 68, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Rabadi, M.H.; Coar, P.L.; Lukin, M.; Lesser, M.; Blass, J.P. Intensive nutritional supplements can improve outcomes in stroke rehabilitation. Neurology 2008, 71, 1856–1861. [Google Scholar] [CrossRef]
- Ramasamy, D.K.; Dutta, T.; Kannan, V.; Chandramouleeswaran, V. Amino acids in post-stroke rehabilitation. Nutr. Neurosci. 2019, 20, 1–6. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | Mean (±SD) or n (%) |
|---|---|
| Age (years) | 66.4 ± 12.2 |
| Sex | |
| Men | 18 (60.0%) |
| Women | 12 (40.0%) |
| Index stroke type | |
| Ischemic | 21 (70.0%) |
| Hemorrhagic | 9 (30.0%) |
| Affected side | |
| Right | 12 (40.0%) |
| Left | 18 (60.0%) |
| Comorbidities | |
| Hypertension | 22 (73.3%) |
| Type 2 Diabetes | 10 (33.3%) |
| Dislipidemia | 6 (10%) |
| Hearth disease | 7 (23.3%) |
| Dysphagia | 7 (23.3%) |
| Language impairment | 7 (23.3%) |
| Neglect syndrome | 6 (20.0%) |
| Days from index stroke to enrollment | 90.5 ± 41.2 |
| Modified Barthel Index (0-100) | 25.3 ± 15.3 |
| Biochemical Variables | ΔBI | |
|---|---|---|
| Spearman’s rho | p-Value | |
| Total calcium | 0.466 | 0.009 |
| Ionized calcium | 0.278 | 0.137 |
| Total protein | 0.278 | 0.136 |
| Albumin | -0.095 | 0.623 |
| Independent Variables | Unstardardized Coefficients | Stardardized Coefficients | t | p-Value | |
|---|---|---|---|---|---|
| B | SE | Beta | |||
| Total calcium | 10.989 | 5.298 | 0.366 | 2.074 | 0.049 |
| Time since stroke | −0.031 | 0.072 | −0.083 | −0.435 | 0.667 |
| Age | −0.412 | 0.225 | −0.325 | −1.833 | 0.079 |
| Type of stroke | 7.504 | 6.201 | 0.226 | 1.210 | 0.238 |
| Barthel Index (baseline) | −0.316 | 0.161 | −0.314 | −1.961 | 0.062 |
| Constant | −41.947 | 57.915 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siotto, M.; Germanotta, M.; Santoro, M.; Di Blasi, C.; Loreti, C.; Mastropaolo, S.; Aprile, I. Total Serum Calcium and Recovery after Rehabilitation in Patients with Stroke. Appl. Sci. 2020, 10, 7893. https://0-doi-org.brum.beds.ac.uk/10.3390/app10217893
Siotto M, Germanotta M, Santoro M, Di Blasi C, Loreti C, Mastropaolo S, Aprile I. Total Serum Calcium and Recovery after Rehabilitation in Patients with Stroke. Applied Sciences. 2020; 10(21):7893. https://0-doi-org.brum.beds.ac.uk/10.3390/app10217893
Chicago/Turabian StyleSiotto, Mariacristina, Marco Germanotta, Massimo Santoro, Chiara Di Blasi, Claudia Loreti, Simona Mastropaolo, and Irene Aprile. 2020. "Total Serum Calcium and Recovery after Rehabilitation in Patients with Stroke" Applied Sciences 10, no. 21: 7893. https://0-doi-org.brum.beds.ac.uk/10.3390/app10217893