Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pre-Surgical Procedures
2.2. Surgical Procedures
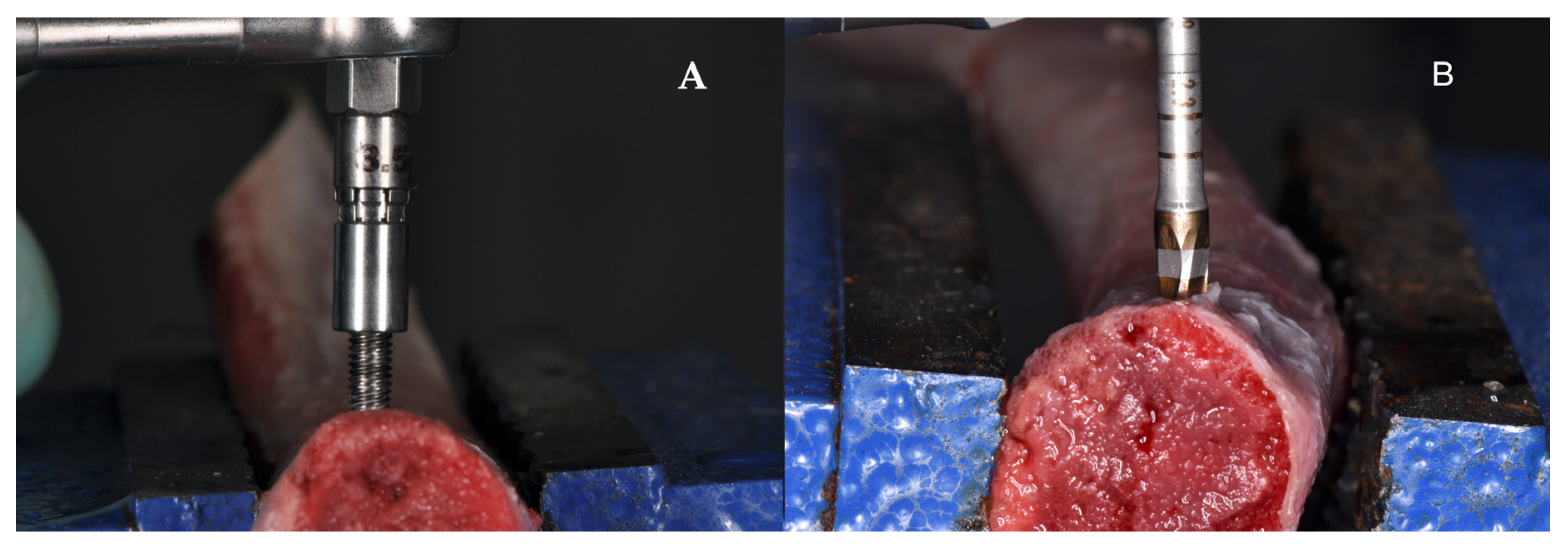
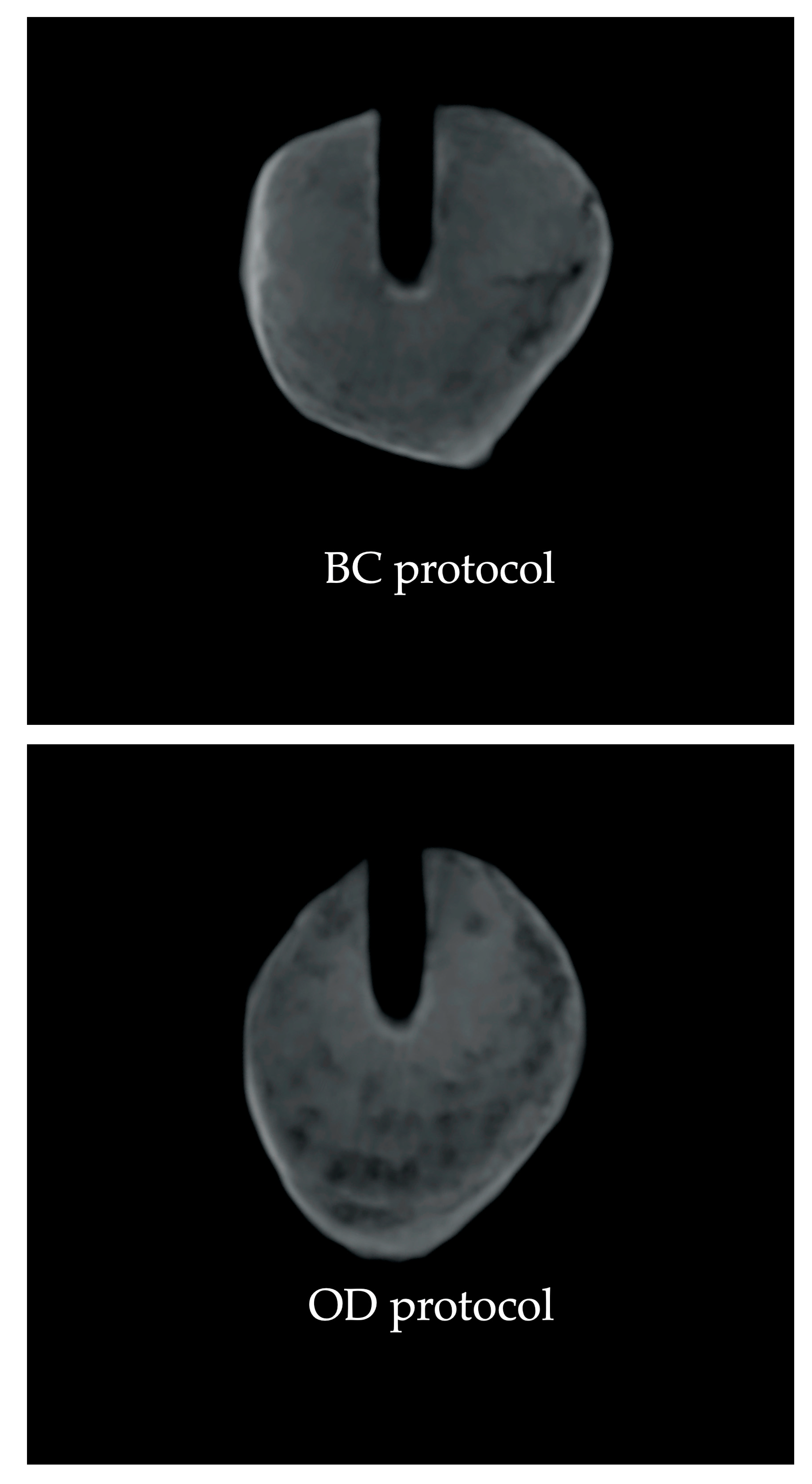
2.2.1. Bone Compaction Implant Site Preparation
2.2.2. Osseodensification Implant Site Preparation
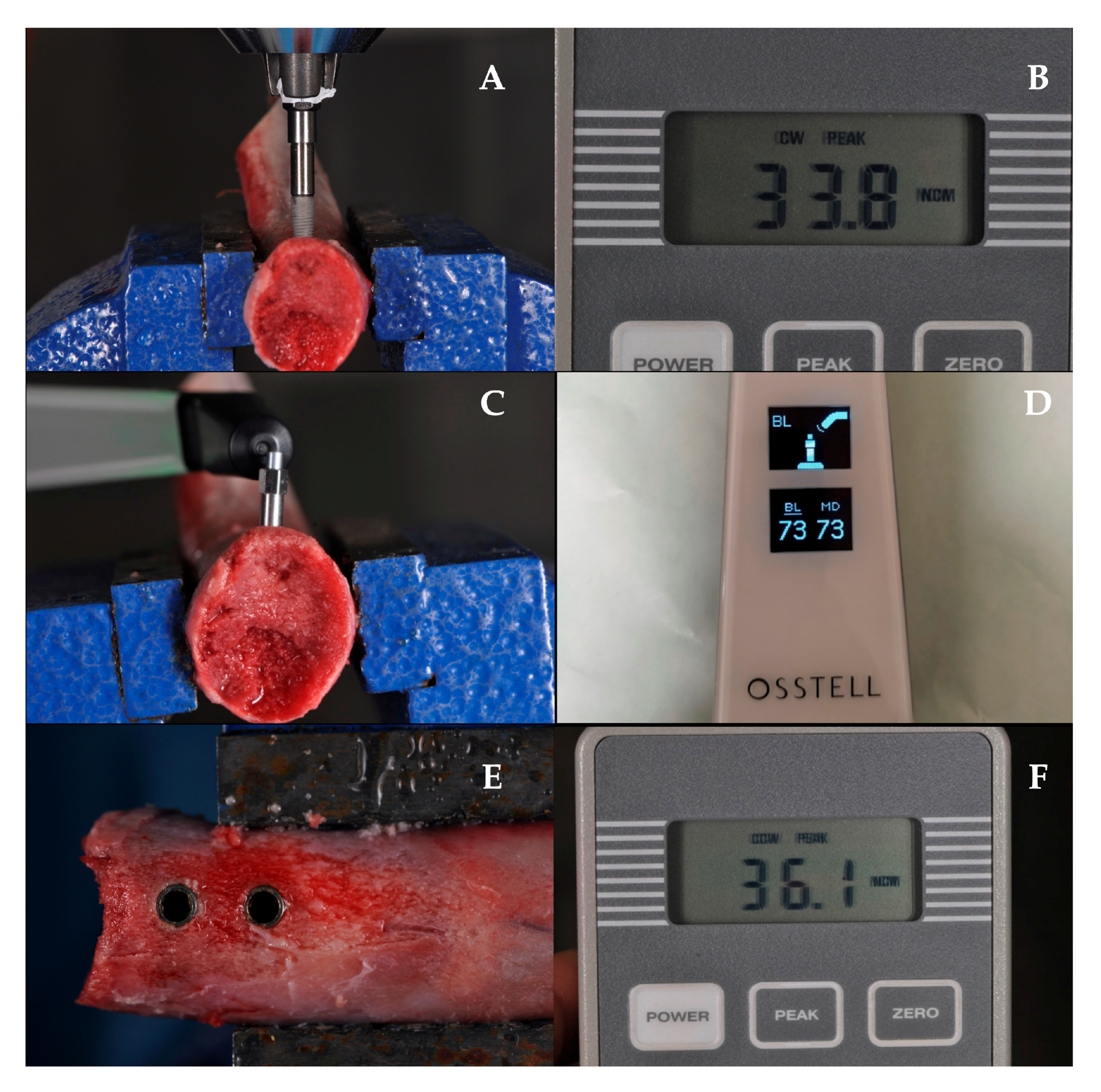
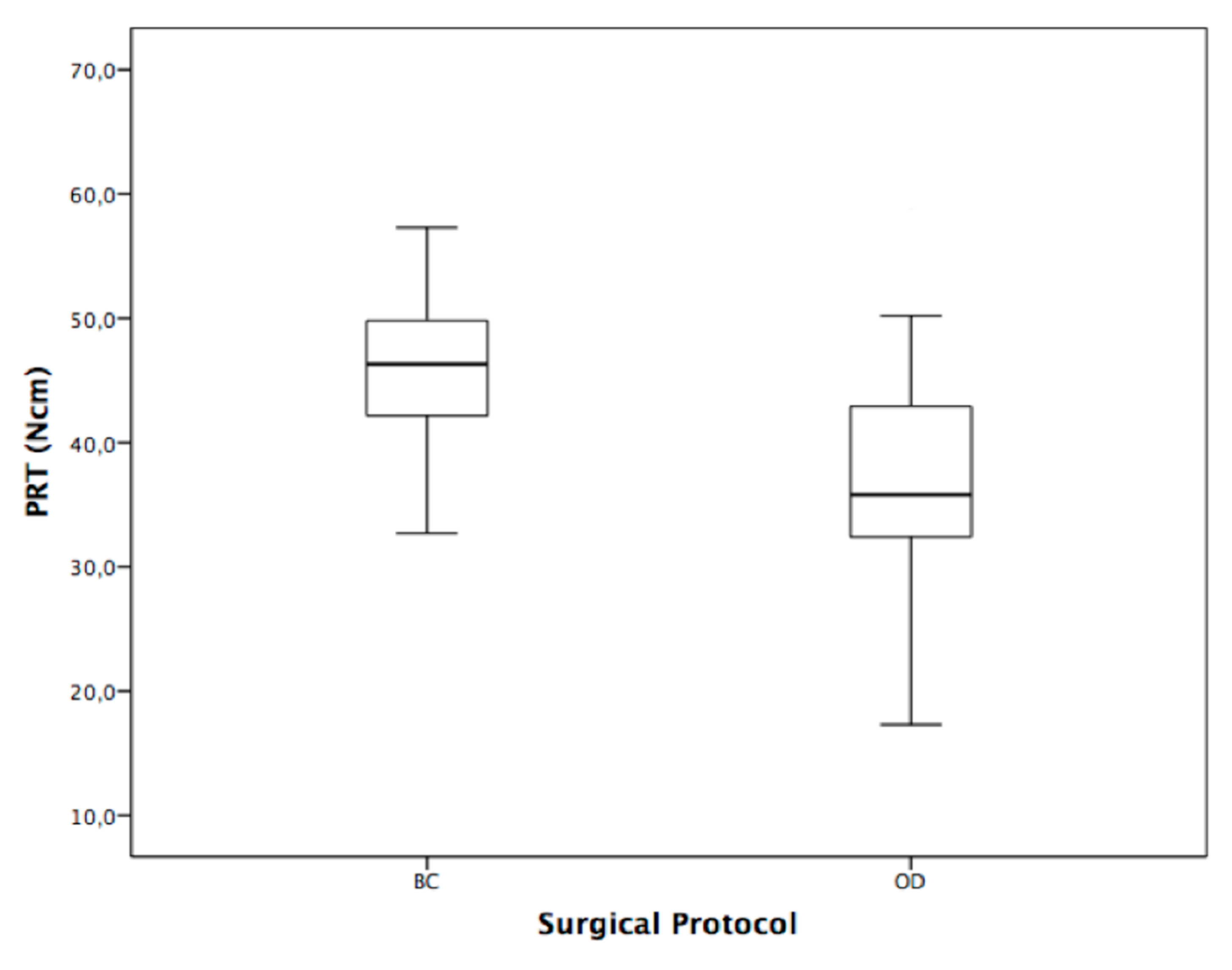
2.3. Primary Implant Stability Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| OD | Osseodensification drills |
| BC | Bone compactors |
| PS | Primary implant stability |
| PIT | Peak insertion torque |
| RFA | Resonance frequency analysis |
| ISQ | Implant stability quotient |
| PRT | Peak removal torque |
References
- Makary, C.; Menhall, A.; Zammarie, C.; Lombardi, T.; Lee, S.Y.; Stacchi, C.; Park, K.B. Primary Stability Optimization by Using Fixtures with Different Thread Depth According to Bone Density: A Clinical Prospective Study on Early Loaded Implants. Materials 2019, 12, 2398. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; Ravidà, A.; Wang, H.L.; Helms, J.A.; Brunski, J.B. Relationship between Primary/Mechanical and Secondary/Biological Implant Stability. Int. J. Oral Maxillofac. Implant. 2019, 34, s7–s23. [Google Scholar] [CrossRef]
- Huwais, S.; Meyer, E.G. A Novel Osseous Densification Approach in Implant Osteotomy Preparation to Increase Biomechanical Primary Stability, Bone Mineral Density, and Bone-to-Implant Contact. Int. J. Oral Maxillofac. Implant. 2017, 32, 27–36. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Arosio, P.; Perrotti, V.; Iezzi, G.; Scarano, A.; Piattelli, A. Correlation between Implant Geometry, Bone Density, and the Insertion Torque/Depth Integral: A Study on Bovine Ribs. Dent. J. 2019, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Duttenhoefer, F.; Fuessinger, M.A.; Beckmann, Y.; Schmelzeisen, R.; Groetz, K.A.; Boeker, M. Dental implants in immunocompromised patients: A systematic review and meta-analysis. Int. J. Implant. Dent. 2019, 5, 43. [Google Scholar] [CrossRef]
- Guazzo, R.; Sbricoli, L.; Ricci, S.; Bressan, E.; Piattelli, A.; Iaculli, F. Medication-Related Osteonecrosis of the Jaw and Dental Implants Failures: A Systematic Review. J. Oral Implantol. 2017, 43, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Barone, S.; Diodati, F.; Antonelli, A.; Nocini, R.; Cristofaro, M.G. Can Surgical Management Improve Resolution of Medication-Related Osteonecrosis of the Jaw at Early Stages? A Prospective Cohort Study. J. Oral Maxillofac. Surg. 2020, 78, 1986–1999. [Google Scholar] [CrossRef] [PubMed]
- Simonpieri, A.; Gasparro, R.; Pantaleo, G.; Mignogna, J.; Riccitiello, F.; Sammartino, G. Four-year post-loading results of full-arch rehabilitation with immediate placement and immediate loading implants: A retrospective controlled study. Quintessence Int. 2017, 48, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Barone, S.; Muraca, D.; Averta, F.; Diodati, F.; Antonelli, A.; Fortunato, L. Can Teledentistry Improve the Monitoring of Patients during the Covid-19 Dissemination? A Descriptive Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 3399. [Google Scholar] [CrossRef]
- Trisi, P.; Perfetti, G.; Baldoni, E.; Berardi, D.; Colagiovanni, M.; Scogna, G. Implant micromotion is related to peak insertion torque and bone density. Clin. Oral Implant. Res. 2009, 20, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, I.; Lekholm, U.; Holm, S.; Kultje, C. Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. Int. J. Oral Maxillofac. Implant. 2005, 20, 220–230. [Google Scholar]
- Stacchi, C.; Spinato, S.; Lombardi, T.; Bernardello, F.; Bertoldi, C.; Zaffe, D.; Mevins, M. Minimally Invasive Management of Implant-Supported Rehabilitation in the Posterior Maxilla, Part, I.I. Surgical Techniques and Decision Tree. Int. J. Periodontics Restor. Dent. 2020, 40, e95–e102. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; De Biasi, M.; Torelli, L.; Robiony, M.; Di Lenarda, R.; Angerame, D. Primary Stability of Short Implants Inserted Using Piezoelectric or Drilling Systems: An In Vitro Comparison. J. Oral Implantol. 2019, 45, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Pérez-Albacete Martínez, C.; Piattelli, A.; Shibli, J.A.; Markovic, A.; Calvo Guirado, J.L. The influence of three different apical implant designs at stability and osseointegration process: Experimental study in rabbits. Clin. Oral Implant. Res. 2017, 28, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Assenza, B.; Inchingolo, F.; Mastrangelo, F.; Lorusso, F. New Implant Design with Midcrestal and Apical Wing Thread for Increased Implant Stability in Single Postextraction Maxillary Implant. Case Rep. Dent. 2019, 2019, 9529248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanali, S.; Tumedei, M.; Pignatelli, P.; Inchingolo, F.; Pennacchietti, P.; Pace, G.; Piattelli, A. Implant primary stability with an osteocondensation drilling protocol in different density polyurethane blocks. Comput. Methods Biomech. Biomed. Eng. 2020, 25, 1–7. [Google Scholar] [CrossRef]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Wagner, F.; Fortunato, L.; Traxler, H. Influence of clinician’s skill on primary implant stability with conventional and piezoelectric preparation techniques: An ex-vivo study. J. Biol. Regul. Homeost. Agents 2020, 34, 739–745. [Google Scholar] [CrossRef]
- Michael, R.N.; Carole, G. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implant. Res. 2001, 12, 79–84. [Google Scholar]
- Lekholm, U. Patient Selection and Preparation. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Publishing: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Merheb, J.; Temmerman, A.; Rasmusson, L.; Kübler, A.; Thor, A.; Quirynen, M. Influence of Skeletal and Local Bone Density on Dental Implant Stability in Patients with Osteoporosis. Clin. Implant. Dent. Relat. Res. 2016, 18, 253–260. [Google Scholar] [CrossRef]
- Figliuzzi, M.M.; Giudice, A.; Pileggi, S.; Pacifico, D.; Marrelli, M.; Tatullo, M.; Fortunato, L. Implant-Prosthetic Rehabilitation in Bilateral Agenesis of Maxillary Lateral Incisors with a Mini Split Crest. Case Rep. Dent. 2016, 2016, 3591321. [Google Scholar] [CrossRef] [Green Version]
- Holahan, C.M.; Wiens, J.L.; Weaver, A.; Assad, D.; Koka, S. Relationship between systemic bone mineral density and local bone quality as effectors of dental implant survival. Clin. Implant. Dent. Relat. Res. 2011, 13, 29–33. [Google Scholar] [CrossRef]
- Vervaeke, S.; Collaert, B.; Cosyn, J.; Deschepper, E.; De Bruyn, H. A multifactorial analysis to identify predictors of implant failure and peri-implant bone loss. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 1), e298–e307. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Lombardi, T.; Colombo, J.; Cervino, G.; Perinetti, G.; Di Lenarda, R.; Stacchi, C. Correlation between Insertion Torque and Implant Stability Quotient in Tapered Implants with Knife-Edge Thread Design. Biomed. Res. Int. 2018, 2018, 7201093. [Google Scholar] [CrossRef]
- Stacchi, C.; Bassi, F.; Troiano, G.; Rapani, A.; Lombardi, T.; Jokstad, A.; Sennerby, L.; Schierano, G. Piezoelectric bone surgery for implant site preparation compared with conventional drilling techniques: A systematic review, meta-analysis and trial sequential analysis. Int. J. Oral Implantol. 2020, 13, 141–158. [Google Scholar]
- Degidi, M.; Daprile, G.; Piattelli, A. Influence of underpreparation on primary stability of implants inserted in poor quality bone sites: An in vitro study. J. Oral Maxillofac. Surg. 2015, 73, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Berardini, M.; Falco, A.; Podaliri Vulpiani, M. New Osseodensification Implant Site Preparation Method to Increase Bone Density in Low-Density Bone: In Vivo Evaluation in Sheep. Implant. Dent. 2016, 25, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coyac, B.R.; Leahy, B.; Salvi, G.; Hoffmann, W.; Brunski, J.B.; Helms, J.A. A preclinical model links osseo-densification due to misfit and osseo-destruction due to stress/strain. Clin. Oral Implant. Res. 2019, 30, 1238–1249. [Google Scholar] [CrossRef] [PubMed]
- Slete, F.B.; Olin, P.; Prasad, H. Histomorphometric Comparison of 3 Osteotomy Techniques. Implant. Dent. 2018, 27, 424–428. [Google Scholar] [CrossRef]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2000 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Padhye, N.M.; Padhye, A.M.; Bhatavadekar, N.B. Osseodensification—A systematic review and qualitative analysis of published literature. J. Oral Biol. Craniofac. Res. 2020, 10, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Elsayyad, A.A.; Osman, R.B. Osseodensification in Implant Dentistry: A Critical Review of the Literature. Implant. Dent. 2019, 28, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Lahens, B.; Neiva, R.; Tovar, N.; Alifarag, A.M.; Jimbo, R.; Bonfante, E.A.; Bowers, M.M.; Cuppini, M.; Freitas, H.; Witek, L.; et al. Biomechanical and histologic basis of osseodensification drilling for endosteal implant placement in low density bone. An experimental study in sheep. J. Mech. Behav. Biomed. Mater. 2016, 63, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Alifarag, A.M.; Lopez, C.D.; Neiva, R.F.; Tovar, N.; Witek, L.; Coelho, P.G. Atemporal osseointegration: Early biomechanical stability through osseodensification. J. Orthop Res. 2018, 36, 2516–2523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutouzis, T.; Huwais, S.; Hasan, F.; Trahan, W.; Waldrop, T.; Neiva, R. Alveolar Ridge Expansion by Osseodensification-Mediated Plastic Deformation and Compaction Autografting: A Multicenter Retrospective Study. Implant. Dent. 2019, 28, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, C.D.; Alifarag, A.M.; Torroni, A.; Tovar, N.; Diaz-Siso, J.R.; Witek, L.; Rodriguez, E.D.; Coelho, P.G. Osseodensification for enhancement of spinal surgical hardware fixation. J. Mech. Behav. Biomed. Mater. 2017, 69, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Huwais, S.; Mazor, Z.; Ioannou, A.L.; Gluckman, H.; Neiva, R. A Multicenter Retrospective Clinical Study with Up-to-5-Year Follow-up Utilizing a Method that Enhances Bone Density and Allows for Transcrestal Sinus Augmentation Through Compaction Grafting. Int. J. Oral Maxillofac. Implant. 2018, 33, 1305–1311. [Google Scholar] [CrossRef] [Green Version]
- Tanello, B.; Huwais, S.; Tawil, I.; Rosen, P.; Neiva, R. Osseodensification protocols for enhancement of primary and secondary implant stability–A retrospective 5-year follow-up multi-center study. Clin. Oral Implant. Res. 2019, 30, 414. [Google Scholar] [CrossRef]
- Gaspar, J.; Esteves, T.; Gaspar, R.; Rua, J.; João Mendes, J. Osseodensification for implant site preparation in the maxilla-a prospective study of 97 implants. Clin. Oral Implant. Res. 2018, 29, 163. [Google Scholar] [CrossRef] [Green Version]
- Kumar, B.; Narayan, V. Minimally invasive crestal approach sinus floor elevation using Densah burs, and hydraulic lift utilizing putty graft in cartridge delivery. Clin. Oral Implant. Res. 2017, 28 (Suppl. 14), 203. [Google Scholar]
- Vercellotti, T.; Troiano, G.; Oreglia, F.; Lombardi, T.; Gregorig, G.; Morella, E.; Rapani, A.; Stacchi, C. Wedge-Shaped Implants for Minimally Invasive Treatment of Narrow Ridges: A Multicenter Prospective Cohort Study. J. Clin. Med. 2020, 9, 3301. [Google Scholar] [CrossRef] [PubMed]
- Meredith, N.; Book, K.; Friberg, B.; Jemt, T.; Sennerby, L. Resonance frequency measurements of implant stability in vivo. A cross-sectional and longitudinal study of resonance frequency measurements on implants in the edentulous and partially dentate maxilla. Clin. Oral Implant. Res. 1997, 8, 226–233. [Google Scholar] [CrossRef]
- Anitua, E.; Murias-Freijo, A.; Alkhraisat, M.H. Conservative Implant Removal for the Analysis of the Cause, Removal Torque, and Surface Treatment of Failed Nonmobile Dental Implants. J. Oral Implant. 2016, 42, 69–77. [Google Scholar] [CrossRef]
- Stacchi, C.; Lombardi, T.; Baldi, D.; Bugea, C.; Rapani, A.; Perinetti, G.; Itri, A.; Carpita, D.; Audenino, G.; Bianco, G.; et al. Immediate Loading of Implant-Supported Single Crowns after Conventional and Ultrasonic Implant Site Preparation: A Multicenter Randomized Controlled Clinical Trial. Biomed. Res. Int. 2018, 2018, 6817154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cozzani, M.; Nucci, L.; Lupini, D.; Dolatshahizand, H.; Fazeli, D.; Barzkar, E.; Naeini, E.; Jamilian, A. The ideal insertion angle after immediate loading in Jeil, Storm, and Thunder miniscrews: A 3D-FEM study. Int. Orthod. 2020, 18, 503–508. [Google Scholar] [CrossRef]
- Minervini, G.; Romano, A.; Petruzzi, M.; Maio, C.; Serpico, R.; Lucchese, A.; Candotto, V.; Di Stasio, D. Telescopic overdenture on natural teeth: Prosthetic rehabilitation on (OFD) syndromic patient and a review on available literature. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. 1), 131–134. [Google Scholar]
- Ikar, M.; Grobecker-Karl, T.; Karl, M.; Steiner, C. Mechanical stress during implant surgery and its effects on marginal bone: A literature review. Quintessence Int. 2020, 51, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Witek, L.; Alifarag, A.M.; Tovar, N.; Lopez, C.D.; Gil, L.F.; Gorbonosov, M.; Hannan, K.; Neiva, R.; Coelho, P.G. Osteogenic parameters surrounding trabecular tantalum metal implants in osteotomies prepared via osseodensification drilling. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e764–e769. [Google Scholar] [CrossRef]
- González-García, R.; Monje, F.; Moreno-García, C. Predictability of the resonance frequency analysis in the survival of dental implants placed in the anterior non-atrophied edentulous mandible. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e664–e669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischof, M.; Nedir, R.; Szmukler-Moncler, S.; Bernard, J.P.; Samson, J. Implant stability measurement of delayed and immediately loaded implants during healing. Clin. Oral Implants Res. 2004, 15, 529–539. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. Implant Insertion Torque: Its Role in Achieving Primary Stability of Restorable Dental Implants. Compend. Contin. Educ. Dent. 2017, 38, 88–95. [Google Scholar] [PubMed]
- Lages, F.S.; Douglas-de Oliveira, D.W.; Costa, F.O. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant. Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Piattelli, A. Determination of primary stability: A comparison of the surgeon’s perception and objective measurements. Int. J. Oral Maxillofac. Implants 2010, 25, 558–561. [Google Scholar] [PubMed]
- Yao, C.J.; Ma, L.; Mattheos, N. Can resonance frequency analysis detect narrow marginal bone defects around dental implants? An ex vivo animal pilot study. Aust. Dent. J. 2017, 62, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Di Fiore, A.; Sivolella, S.; Stocco, E.; Favero, V.; Stellini, E. Experimental Analysis of Temperature Differences during Implant Site Preparation: Continuous Drilling Technique Versus Intermittent Drilling Technique. J. Oral Implantol. 2018, 44, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Fugito Junior, K.; Cortes, A.R.; de Carvalho Destro, R.; Yoshimoto, M. Comparative Study on the Cutting Effectiveness and Heat Generation of Rotary Instruments Versus Piezoelectric Surgery Tips Using Scanning Electron Microscopy and Thermal Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 345–350. [Google Scholar] [CrossRef]
- Marenzi, G.; Sammartino, J.C.; Scherillo, F.; Rengo, C.; Rosa, A.D.; Graziano, V.; Spagnuolo, G. Comparative Analysis of the Chemical Composition and Microstructure Conformation Between Different Dental Implant Bone Drills. Materials 2019, 12, 1866. [Google Scholar] [CrossRef] [Green Version]
- Marenzi, G.; Sammartino, J.C.; Quaremba, G.; Graziano, V.; Hassanin, A.E.; Qorri, M.E.; Sammartino, G.; Iorio-Siciliano, V. Clinical Influence of Micromorphological Structure of Dental Implant Bone Drills. Biomed. Res. Int. 2018, 2018, 8143962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Möhlhenrich, S.C.; Abouridouane, M.; Heussen, N.; Hölzle, F.; Klocke, F.; Modabber, A. Thermal evaluation by infrared measurement of implant site preparation between single and gradual drilling in artificial bone blocks of different densities. Int. J. Oral Maxillofac. Surg. 2016, 45, 1478–1484. [Google Scholar] [CrossRef]
- Scarano, A.; Lorusso, F.; Noumbissi, S. Infrared Thermographic Evaluation of Temperature Modifications Induced during Implant Site Preparation with Steel vs. Zirconia Implant Drill. J. Clin. Med. 2020, 9, 148. [Google Scholar] [CrossRef] [Green Version]
- Vercellotti, T.; Stacchi, C.; Russo, C.; Rebaudi, A.; Vincenzi, G.; Pratella, U.; Baldi, D.; Mozzati, M.; Monagheddu, C.; Sentineri, R.; et al. Ultrasonic implant site preparation using piezosurgery: A multicenter case series study analyzing 3579 implants with a 1- to 3-year follow-up. Int. J. Periodontics Restor. Dent. 2014, 34, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Lamas Pelayo, J.; Peñarrocha Diago, M.; Martí Bowen, E.; Peñarrocha Diago, M. Intraoperative complications during oral implantology. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E239–E243. [Google Scholar] [PubMed]
- Brancaccio, Y.; Antonelli, A.; Barone, S.; Bennardo, F.; Fortunato, L.; Giudice, A. Evaluation of local hemostatic efficacy after dental extractions in patients taking antiplatelet drugs: A randomized clinical trial. Clin. Oral Investig. 2021, 25, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
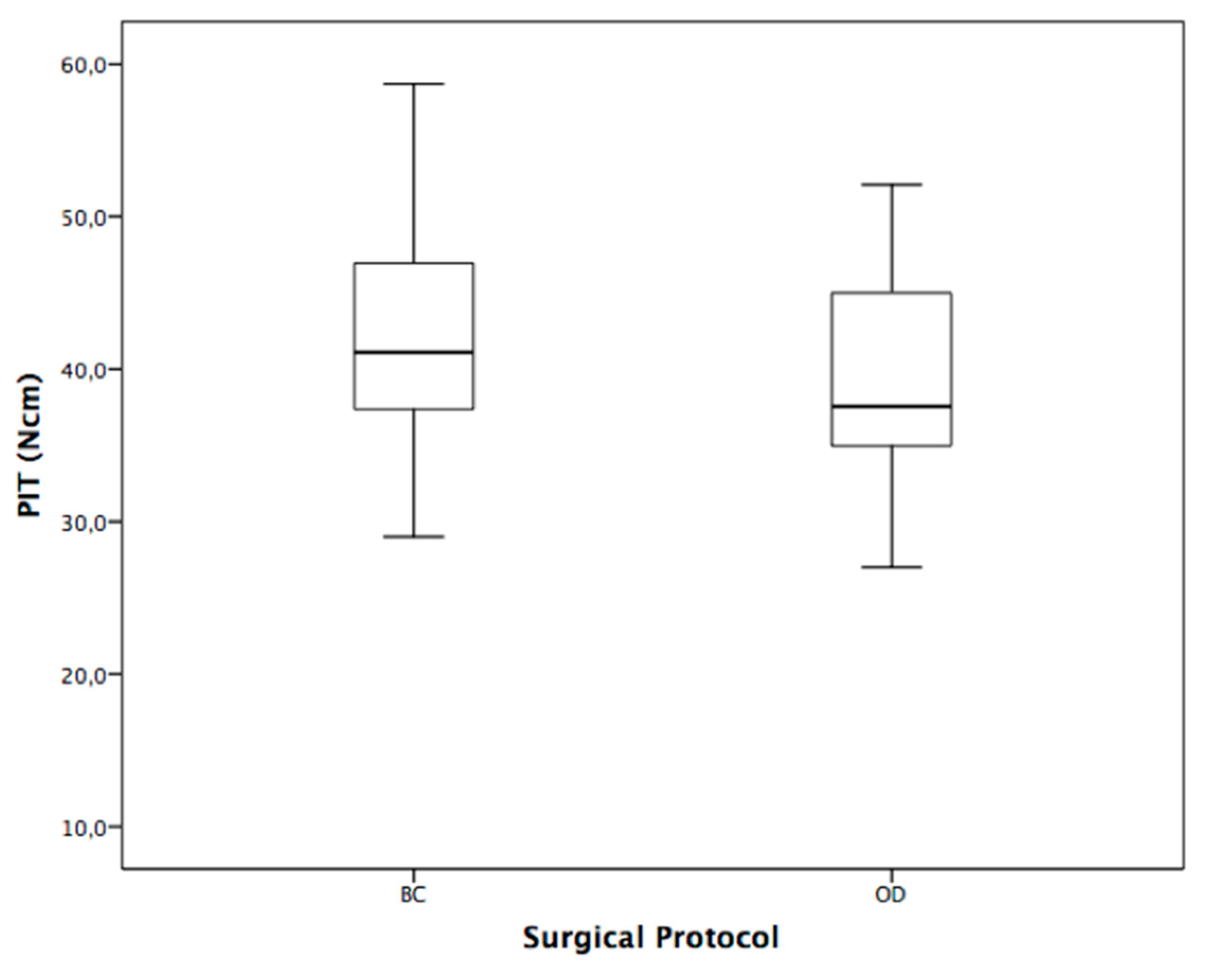
| PIT (Insertion Torque) (Ncm) | Sample Size | Mean | SD |
|---|---|---|---|
| BC | 20 | 41.55 | 9.12 |
| OD | 20 | 38.91 | 7.76 |
| p-value | 0.33 | ||
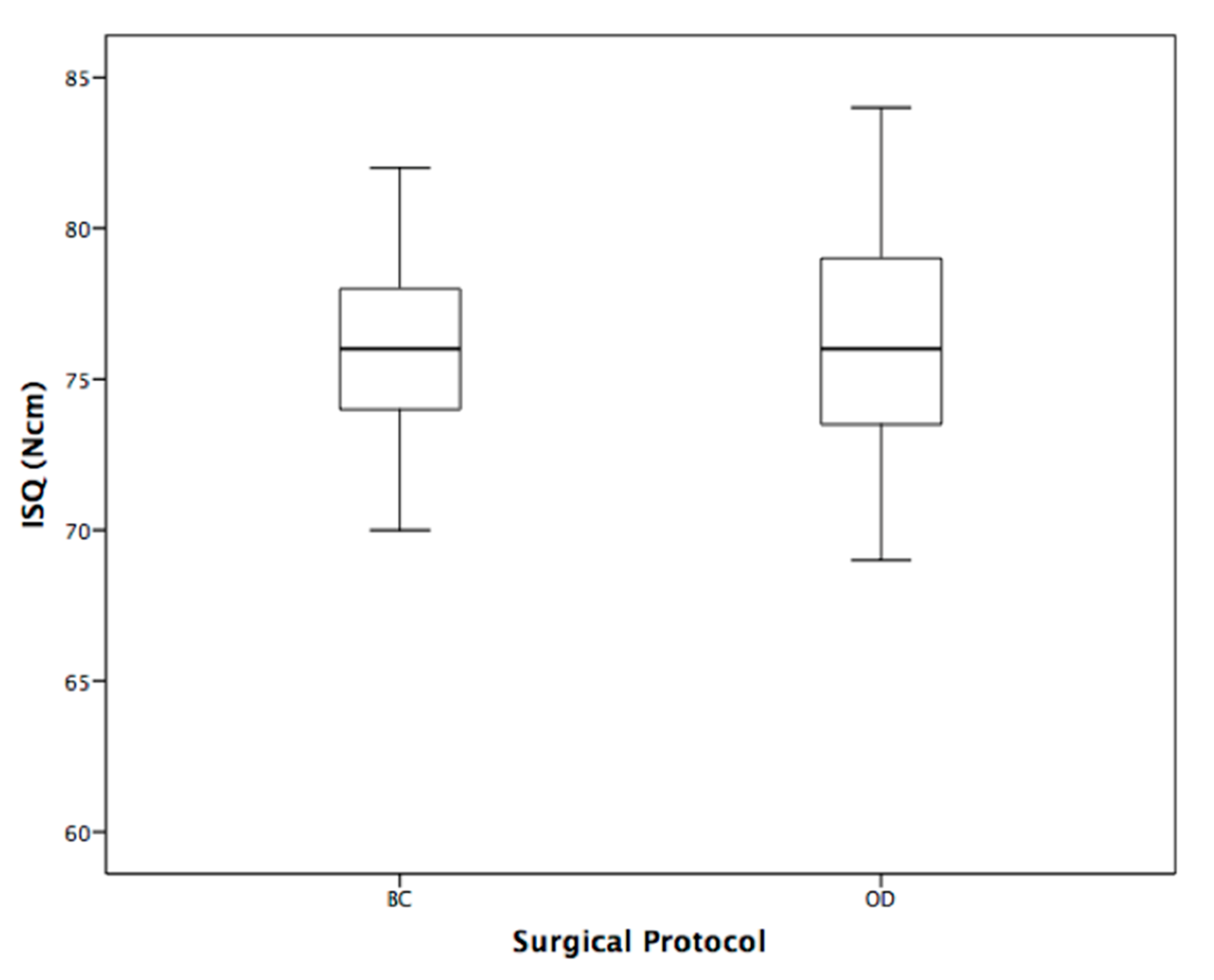
| ISQ (Implant stability quotient) | Sample size | Mean | SD |
| BC | 20 | 75.5 | 3.89 |
| OD | 20 | 75.55 | 5.76 |
| p-value | 0.97 | ||
| PRT (Removal Torque) (Ncm) | Sample size | Mean | SD |
| BC | 20 | 45.37 | 7.8 |
| OD | 20 | 36.7 | 9.82 |
| p-value | 0.009 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonelli, A.; Bennardo, F.; Brancaccio, Y.; Barone, S.; Femiano, F.; Nucci, L.; Minervini, G.; Fortunato, L.; Attanasio, F.; Giudice, A. Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique. Appl. Sci. 2020, 10, 8623. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238623
Antonelli A, Bennardo F, Brancaccio Y, Barone S, Femiano F, Nucci L, Minervini G, Fortunato L, Attanasio F, Giudice A. Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique. Applied Sciences. 2020; 10(23):8623. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238623
Chicago/Turabian StyleAntonelli, Alessandro, Francesco Bennardo, Ylenia Brancaccio, Selene Barone, Felice Femiano, Ludovica Nucci, Giuseppe Minervini, Leonzio Fortunato, Ferdinando Attanasio, and Amerigo Giudice. 2020. "Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique" Applied Sciences 10, no. 23: 8623. https://0-doi-org.brum.beds.ac.uk/10.3390/app10238623