The Effects of 3D and 2D Imaging on Brain Wave Activity in Laparoscopic Training


1
School of Big Data Management, Soochow University, Taipei City 111002, Taiwan
2
Department of Industrial Management, National Taiwan University of Science and Technology, Taipei City 106335, Taiwan
3
Department of Industrial Engineering and Management, Ming Chi University of Technology, New Taipei City 243303, Taiwan
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(2), 862; https://0-doi-org.brum.beds.ac.uk/10.3390/app11020862
Submission received: 15 December 2020
/
Revised: 13 January 2021
/
Accepted: 15 January 2021
/
Published: 18 January 2021
Abstract
:The current study tested the effects of a state-of-the-art stereoscopic three-dimensional (3D) display and a traditional two-dimensional (2D) display on performance and mental workload during simulated laparoscopic tasks with different levels of depth perception over a longer duration than in previous publications. Two different simulated laparoscopic tasks with depth perception, peg transfer, and circle-tracing were performed by 12 participants using 2D and 3D vision systems. The task performances (mean completion time and mean error frequency) and mental workload measures (gamma and alpha brain wave activity, blink frequency and NASA-TLX ratings) were recorded as dependent variables. The physiological mental workload measures were collected via a MUSE EEG headband. The 3D vision system had advantages in mean movement time and mean error frequency in the depth-perception peg transfer task. The mean completion time of the non-depth perception circle-tracing task was significantly lower for 2D than for 3D. For the peg transfer task, EEG alpha wave activity was significantly higher for 3D than for 2D. The EEG gamma wave activity for 2D was significantly higher than that for 3D in both tasks. A significantly higher blink frequency was found for both the peg transfer task and the 3D system. The overall NASA-TLX score of the 2D system was significantly higher. The findings of this research suggest that a 3D vision system could decrease stress, state of attentiveness, and mental workload compared with those of a 2D system, and it might reduce the completion time and increase the precision of depth-perception laparoscopic operations.
1. Introduction
The past two decades have seen the development of laparoscopy and improved outcomes in patients receiving surgeries due to the minimization of surgical trauma, acceleration of postoperative recovery, and abbreviation of hospital stays [1,2,3,4]. However, laparoscopic surgery is more challenging than open laparotomy due to the differences in the psychomotor skills required. One challenge is that the surgeons must complete tasks within three-dimensional (3D) spaces while depending on two-dimensional (2D) images [5,6]. The consequent lack of depth perception and spatial orientation increases the visual and cognitive loads of the tasks [7,8,9].
The overall goals of such a surgical procedure comprise two main components (i.e., a primary and a secondary task). The former is simply the performance of the physical steps of the procedure with instruments and visual feedback. The latter is more complicated, as it is the decision-making on the strategies to be used and steps to be executed. The primary task can be unusually difficult due to the extremely limited cognitive resources for overall monitoring and planning, which may delay the detection of an evolving problem until it becomes an emergency [10].
Increased workload is associated with inferior task performance and higher likelihood of errors [11]. One goal in training and instrument design is to ensure that the surgeon’s movements are both accurate and efficient. Another should be to decrease the mental workload of the surgeon performing the primary surgical task while maintaining acceptable performance levels [10].
3D laparoscopy was developed as an alternative to conventional 2D laparoscopy to overcome some of the challenges associated with laparoscopy [4,9,12,13]. In 3D laparoscopy, image magnification and direct illumination are combined to synthesize left- and right-eye images from a two-channel 3D laparoscope so as to approximate closely what a surgeon would see if they were positioned at the end of the laparoscope [14]. Stereoscopic 3D laparoscopy provides great advantages, particularly when surgery is being performed in areas such as the male pelvis, which can be difficult to visualize.
Compared to 2D laparoscopy, 3D laparoscopy has been reported to improve speed and reduce the number of performance errors, and it has resulted in significantly reduced surgical time, blood loss, perioperative complications, and hospital stays among patients who received abdominal surgery in simulated and clinical settings, respectively [14,15,16]. The stereoscopic vision provided by 3D laparoscopy improves task precision and reduces task performance time due to the simpler presentation of anatomical structures and greater depth perception. Using high-definition 3D vision during training, surgeons can quickly enhance their surgical skills, with the result that the learning curve in simulated settings can be greatly reduced [17]. In fact, for both experienced and inexperienced surgeons, training programs employing 3D systems provide improved task efficiency, error reduction, and accelerated acquisition of basic thoracoscopic and laparoscopic skills [18].
As above-mentioned, interest in the measurement of surgical skill and performance in laparoscopy has been increasing, especially as these are related to the evaluation of training [19,20,21]. Although the use of performance efficiency measures (speed, movement economy, errors) and ergonomic assessments are relatively well established, however, fewer systematic attempts have been made to develop standardized measures for evaluating the cognitive outcomes of technological innovations.
The most important benefit of using 3D vision systems is improved depth perception, which may reduce the surgeon’s mental workload [14,22]. Several recent studies have used the National Aeronautics and Space Administration Task Load Index (NASA-TLX) [23] to compare mental workload when using either 2D or 3D vision during laparoscopic surgery, and the results have been contradictory. Half of these trials reported a significantly reduced workload when using 3D vision [9,18,24,25], and the other half could not find any significant differences between the two vision systems [6,26,27,28]. Therefore, additional studies investigating the effects of 3D vision on mental workload need to be performed before any conclusions can be reached. Moreover, 3D vision was thought primarily to give surgeons an advantage during more complex laparoscopic operations or simulation tasks [2,9,28,29,30]. Nevertheless, studies have reported that 3D laparoscopy is also advantageous for non-complex tasks [6,22,31,32]. There is still a lack of systematic research comparing mental workloads between different depth-perception tasks. As noted above, the evaluation of newly-developed laparoscopic tools and displays, and that of the training procedures focused on them, should incorporate measures of mental workload. However, few researchers have engaged in systematic efforts to develop standardized measures of mental workload that can be used to judge the effectiveness of new surgical displays and similar technological innovations. If equipment and training procedures are to be evaluated, then multiple mental workload measures should be selected to ensure that the evaluation is both accurate and comprehensive [33]. For this reason, this study attempted to integrate physiological and subjective measures to develop standardized assessment measures for evaluating the effects of 2D and 3D vision systems on mental workload during the performance of different depth-perception laparoscopic tasks.
2. Methods
2.1. Ethics
The experiment was reviewed and approved by the Research Ethics Committee of National Taiwan University. All individual participants in this study gave written informed consent prior to their participation and were free to withdraw from the study without prejudice.
2.2. Participants
Twelve right-handed graduate students (six males and six females) were recruited from the National Taiwan University of Science and Technology to participate in this experiment. The mean age and standard deviation of the participants were 24.2 years and 0.58 years, respectively. All participants had normal or corrected-to-normal vision with no other physical impairments. None were from the medical school and thus none had any prior surgical experience.
2.3. Apparatus
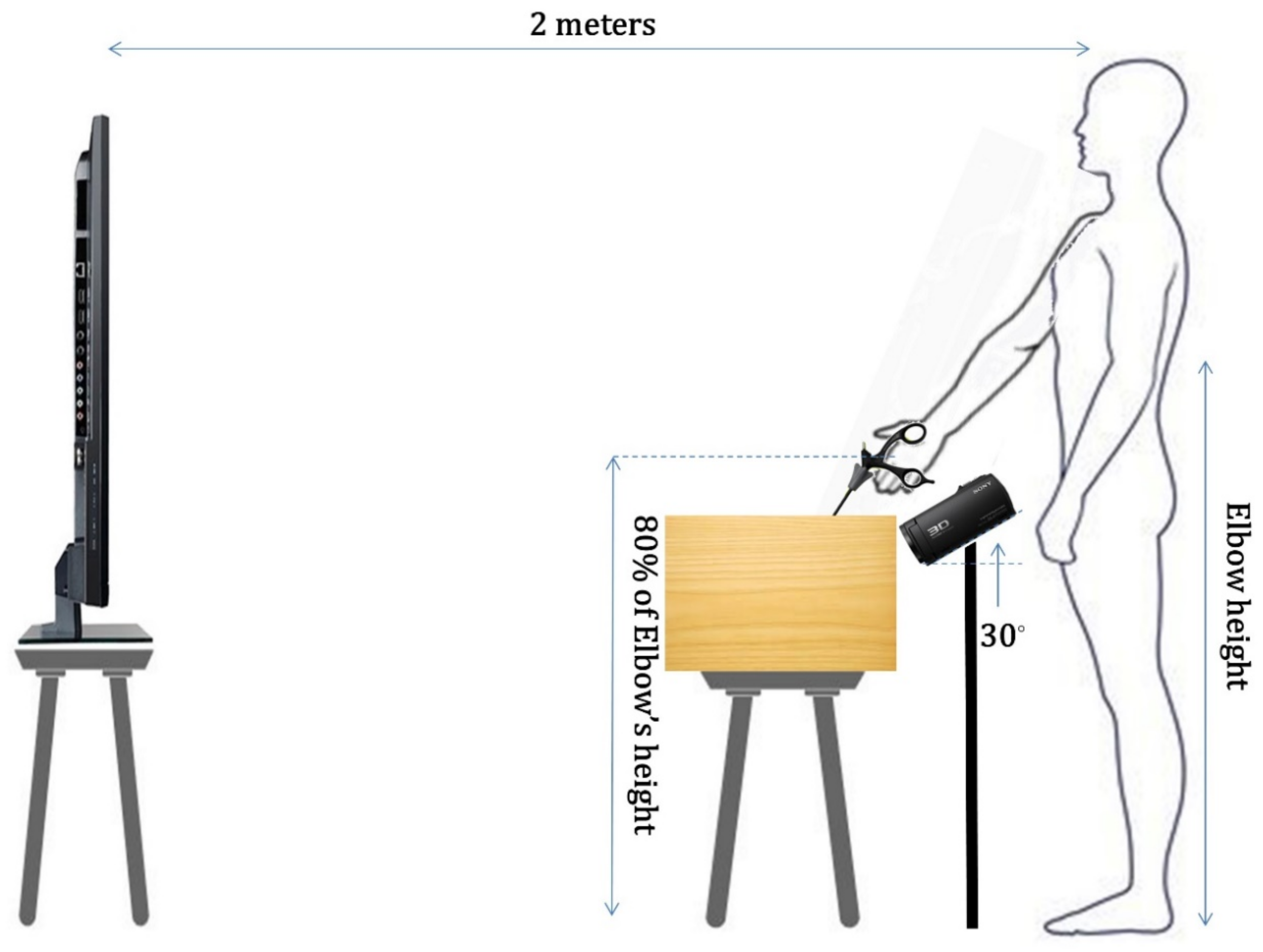
Both tasks were conducted in a laparoscopic simulation trainer (40 cm × 25 cm × 15 cm, length × width × height) developed for the present study. Simulated laparoscopic tasks were performed by holding a laparoscopic instrument passing through a rubber diaphragm representing the patient’ abdominal wall. The port of 10 mm in diameter was located at 5.7 cm and 135° from the center of the rubber diaphragm, and the fulcrum was located approximately halfway up the instrument shaft. The handle of the instrument was set at 80% of the participant’s elbow height, as suggested by Berquer et al. [34]. A horizontal occluding board was used to prevent direct vision of the instrument displacement during the tasks.
Many previous studies comparing 3D and 2D vision systems have failed to use appropriate controls that were identical in all respects except for the 2D or 3D viewing conditions [35]. To ensure that 2D and 3D viewing were the only variables in this experimental research comparing laparoscopic technical performance and mental workload in 2D and 3D, the display monitor and laparoscopic camera were kept identical by using one vision system that was able to display both 2D and 3D images with the same set-up. For both the 2D and 3D viewing conditions, the participants controlled the movement of the instrument based on visual feedback from a 3D TV (Sony KDL-55W800B 55-inch 3D LCD TV). A 3D digital recorder (Sony HDR-TD30V Full HD) was set at an angle of 30° from the horizontal plane to capture real-time displacement movement in the laparoscopic simulation trainer for synchronous display on the 3D TV. For the 3D viewing condition, the participants wore active 3D glasses (SONY TDG-BT400A) to view the stereoscopic 3D images.
Suboptimal viewing conditions caused by head tilt from the display elevation and acute eccentric viewing angles increase crosstalk due to incorrect orientation of the glasses relative to the display [36,37,38]. 3D perception is dramatically influenced by the distance between the viewer and the stereoscopic display in a way that is qualitatively different from the effect of viewing distance on the perception of a 2D display [35], and the best 3D images are obtained when the viewer is directly facing the display and the viewer’s eye level is the same as that of the center of the display [36]. To ensure fair comparisons between the 2D and 3D displays, the viewing conditions were standardized by adjusting the screen height according to each participant’s eye level and maintaining an eccentric viewing angle of 90° and a viewing distance of 2 m from the participant’s eyes, as shown in Figure 1.
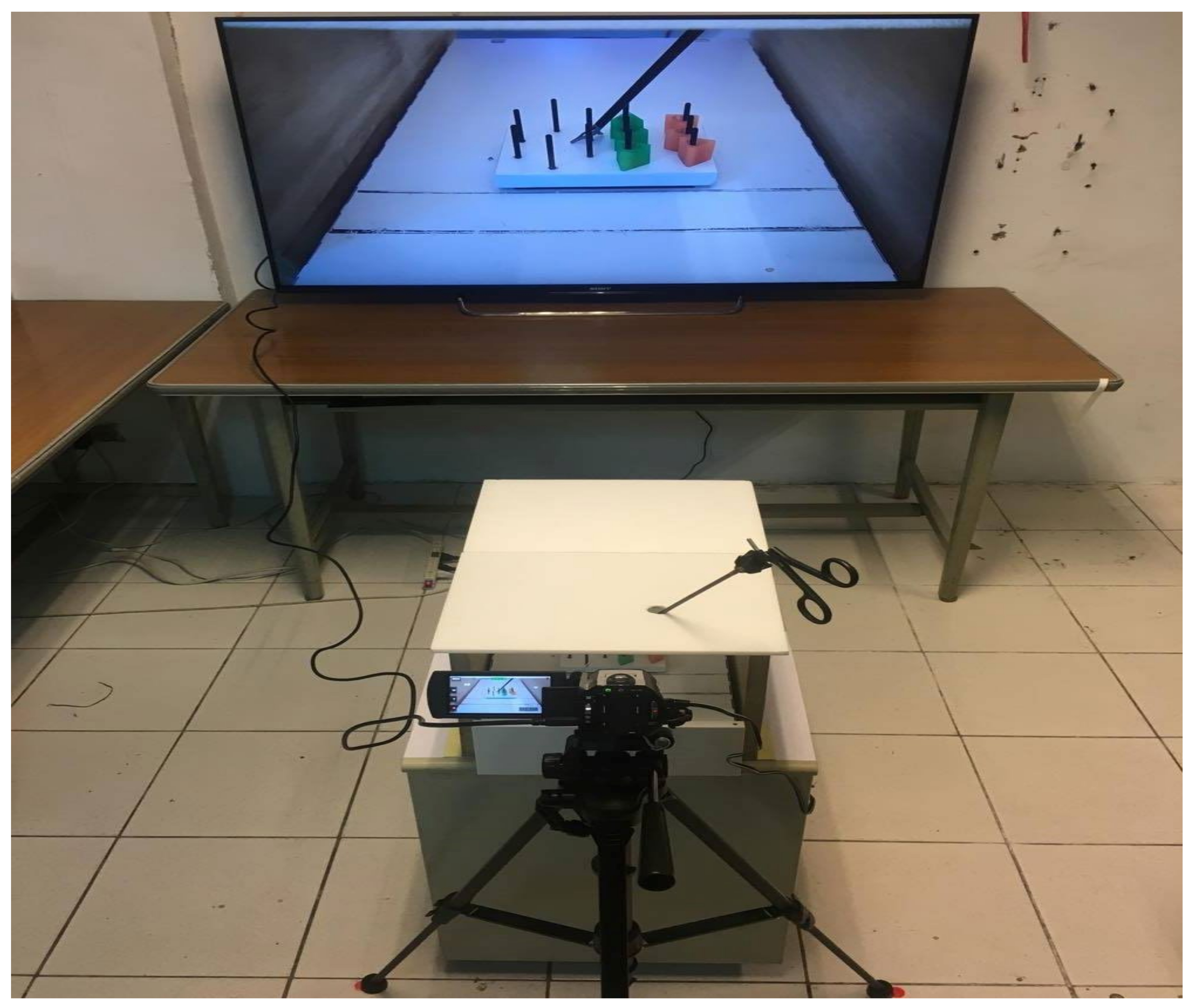
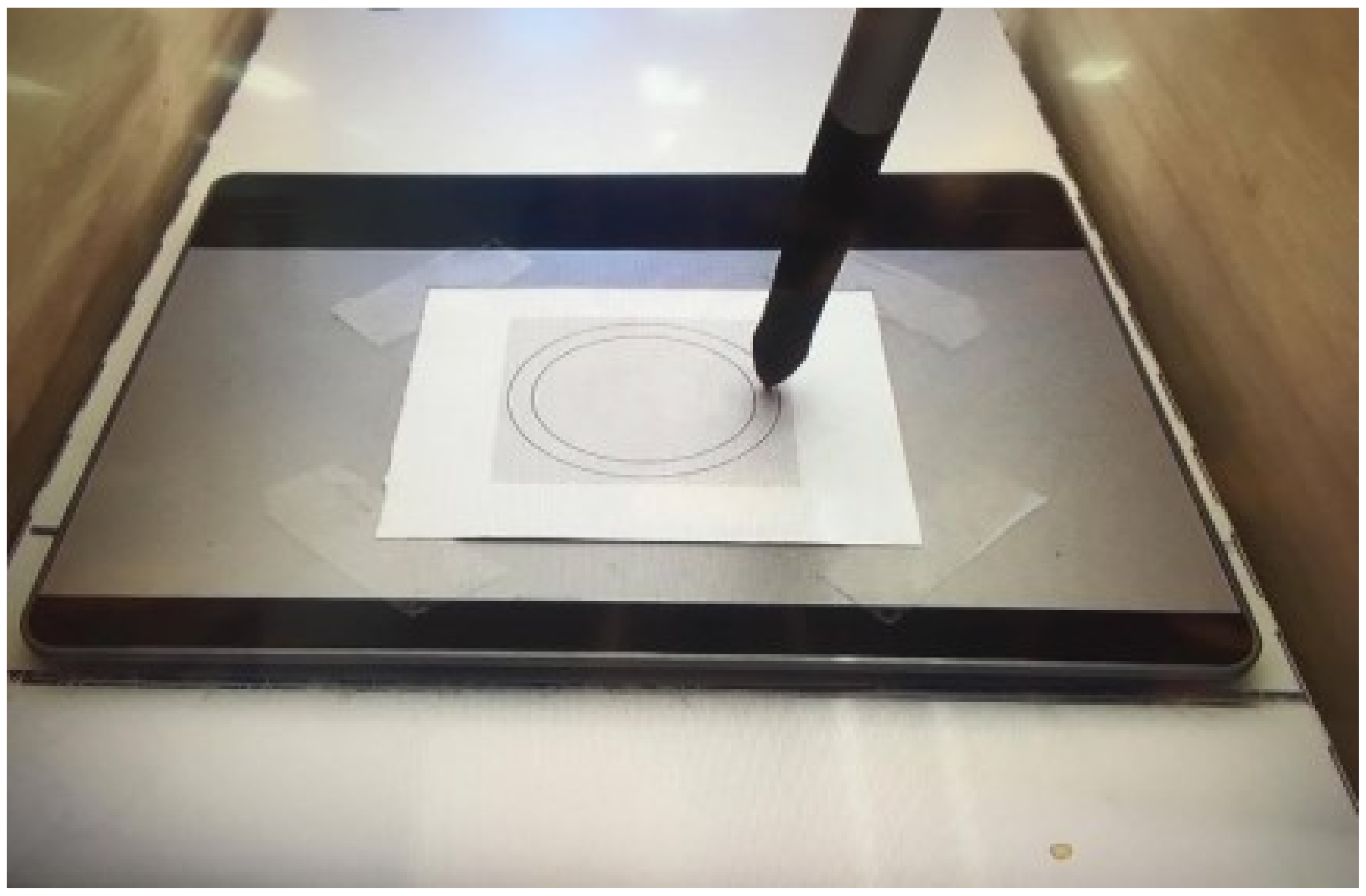
A pegboard and triangle set (Limb & Things, Product No. 50331) and a 5 mm curved dissector were used in the peg transfer task (shown in Figure 2). A digitizer tablet with a light and accurate pen (Wacom CTL-480) and a 10 mm Endo Babcock clamp were used for the circle-tracing task. As shown in Figure 3, the digitizer tablet was covered with a target paper with a pre-marked circular path, and the Endo Babcock clamp was modified by removing the clamp and attaching the digital pen to the rod of the instrument with a plastic tube.
The MUSETM headband (InteraXon Inc., Toronto, Canada), a commercially available and noninvasive wireless Electroencephalography (EEG) monitor, was used to collect brain waves and blinks at a sampling rate of 220 Hz. It is worn as a flexible, adjustable, lightweight headband with seven sensors—two forehead sensors, two ear sensors, and three reference sensors—and has been used in previous studies [39,40,41,42,43]. Participants wore the headset while performing the two tasks and the data were transmitted via Bluetooth to a laptop.
Once the simulated task was completed, the NASA TLX form was used to evaluate the subjective mental workload experienced by the participant. The NASA-TLX requires participants to rate their perceived levels of mental and physical workload, temporal demand, effort, performance, and frustration associated with a task on a scale of 20 points. The NASA-TLX has been used extensively in a variety of projects for assessing the mental workload experienced while performing both open and laparoscopic operations [10,28,44,45,46].
2.4. Tasks
Two simulated laparoscopic tasks with different depth perception conditions and dimensional operation were employed in this study. Task 1 was the peg transfer task, which is a Fundamentals of Laparoscopic Surgery (FLS) task designed to develop depth perception and 3D visual-spatial skills [47]. A series of six plastic triangles was picked up in turn with a curved dissector from a pegboard on the participant’s left and then placed around posts on the corresponding pegboard on the right. After all of the triangles were transferred from left to right, the process was reversed, requiring transfer from right to left. Task 2 was the circle-tracing task, which was simplified from another FLS task, pattern cutting, with two-dimensional operation. Participants were instructed to trace a 10-mm-wide circular path between two concentric circles (radiuses of 45 and 55 mm) using the tip of a modified Endo Babcock clamp with a digital pen. Both tasks were repeated for as many accurate transfers or tracings as possible within 900 s.
2.5. Experimental Design
A repeated-measures design analysis of variance (ANOVA) with a significance level of 0.05 was used to investigate the main effects of the two vision systems on task performance, psychophysiological measure, and subjective mental workload while performing 2D and 3D simulated laparoscopic tasks.
In terms of task performance analysis, a one-way repeated-measures design ANOVA with a significance level of 0.05 was used to investigate the main effects of the two vision systems on performance during both the circle-tracing and peg transfer tasks. The independent variable was vision system (two levels: 2D and 3D vision systems), and the dependent variables were mean completion time and mean error frequency. For the peg transfer task, the completion time began when the tip of the instrument touched the first plastic triangle, and time recording stopped when the participant placed the final plastic triangle on the designated peg. An error was recorded if a plastic triangle was dropped. For the circle-tracing task, the completion time, measured in seconds, was calculated as the interval between the start of one cycle and the start of the next cycle. An error was recorded whenever a participant’s trace strayed from the predefined path.
For the mental workload analysis, the present study used a 2 × 2 repeated-measures design ANOVA. The independent variables were vision system (two levels: 2D and 3D vision systems) and depth-perception simulated laparoscopic task (two levels: non-depth perception circle-tracing and depth-perception peg transfer tasks). The dependent variables were EEG alpha and gamma wave activity, blink frequency, and NASA-TLX subjective mental workload assessment. Gamma wave activity represents neurons linking up in a network to carry out a cognitive or motor function [48]. It represents the ability to concentrate and focus. Alpha wave activity is most closely linked to stress or mental exertion [49]. Changes in blink frequency are correlated with the moment of mental fatigue, lapsed attention, and stress overload [44,50,51]. The brain waves and blinks were collected with the MUSETM EEG headband for each participant and task. Using fast Fourier transformation (FFT), the time domain data were transferred into power values in the frequency domain for calculating the EEG alpha (between 8 and 13 Hz) and gamma (between 30 and 100 Hz) wave activity. EEG traces of both alpha and gamma waves were collected for each participant and task. The areas under the curve of four forehead and ear sensors, measured in Bel-Seconds, were summarized for the alpha and gamma wave activities. The unit of blink frequency was blinks per minute (blinks/min). Once the simulated task was completed, a web-based NASA-TLX questionnaire was used to evaluate the six independent components and overall mental workload experienced by the participant.
2.6. Procedure
Before starting each experiment, the objectives and procedures were explained to the participants, and each participant completed a consent form approved by the Research Ethics Committee of National Taiwan University and a simple demographics sheet. Afterward, participants were fitted carefully with the MUSE headset, and proper connectivity was checked before proceeding to the experimental phases. Wearing the MUSE headset, a participant stood in front of the laparoscopic simulation trainer and held the laparoscopic instrument in the dominant hand. The position of the instrument handle was adjusted to be close to 80% of the participant’s elbow height to minimize both discomfort and upper arm and shoulder muscle work [34]. The screen height was adjusted according to each participant’s eye level to maintain an eccentric viewing angle of 90° and ensure the best-quality 3D images [36]. The participants completed practice trials before performing the tasks so that they could become familiar with the apparatus and tasks. The order of the vision system and simulated task combinations was randomized. Then, the participants followed the procedures for each task and repeated each task for 900 s. Each participant performed only one task combination in one day. During the task, the EEG data and blinks were recorded with the MUSE headset with a software development kit (SDK) to further extract gamma and alpha wave activity. To avoid bias in eye measures, participants were not informed of the blink measurement during the data collection phase. Task performance, completion time, and error frequency were collected for subsequent calculations and analyses. After each condition was completed, the NASA-TLX was used to evaluate the subjective mental workload experienced by the participant.
3. Results
3.1. Performance
3.1.1. Peg Transfer Task
There were significant differences in completion time (F1,11 = 8.111, p = 0.016) and in error frequency (F1,11 = 31.150, p < 0.001) between the vision systems. The 3D vision system was associated with a shorter time to completion and improved task precision. The mean completion times (Standard Deviation) for the 2D and 3D vision systems were 84.04 (20.71) and 68.37 (18.17) seconds. The mean number of times a ring was dropped during each transfer was 0.23 (0.14) in 3D, compared with 0.55 (0.24) in 2D.
3.1.2. Circle-Tracing Task
The mean completion time was significantly lower for 2D than for 3D (F1,11 = 7.484, p = 0.019). The mean completion times and standard deviations for the 2D and 3D vision systems were 15.57 (4.78) and 19.46 (7.20) seconds, respectively. There were no significant differences in error frequency between image vision systems (F1,11 = 0.480, p = 0.503). The mean error rates and standard deviations were 4.01 (1.05) for 2D and 3.75 (0.93) for 3D.
3.2. Mental Workload
3.2.1. EEG Alpha Wave Activity
There were no significant differences in EEG alpha wave activity between the simulated laparoscopic tasks (F1,11 = 3.632, p = 0.083) and vision systems (F1,11 = 1.842, p = 0.202). The EEG alpha wave activities for the circle-tracing and peg transfer tasks were 1498.58 (410.10) and 1966.17 (429.89) Bel-Seconds, and for the 2D and 3D vision systems, 1505.67 (377.70) and 1692.08 (461.73) Bel-Seconds.
However, a significant interaction of simulated task × vision system (F1,11 = 11.072, p = 0.007) was found. For the interactions of the simulated task with EEG alpha wave activity and vision system, the results of one-way ANOVA indicated that in the peg transfer task, EEG alpha wave activity was significantly higher for 3D than for 2D (F1,11 = 7.989, p = 0.016).
3.2.2. EEG Gamma Wave Activity
There were no significant main effects of the tasks on EEG gamma wave activity (F1,11 = 0.243, p = 0.632). The EEG gamma wave activities were 1711.96 (758.40) Bel-Seconds for circle-tracing and 1649.38 (849.40) Bel-Seconds for peg transfer. In terms of vision systems, the EEG gamma wave activity was significantly higher for 2D than for 3D (F1,11 = 19.847, p = 0.001). The EEG gamma wave activity was 2027.75 (865.15) Bel-Seconds for 2D and 1333.58 (546.62) Bel-Seconds for 3D.
A significant interaction of simulated task × vision system (F1,11 = 6.205, p = 0.030) was found. For the interactions of task with EEG gamma wave activity and vision system, the results of one-way ANOVA indicated that EEG gamma wave activity was significantly higher in the 2D than in the 3D condition in both the circle-tracing (F1,11 = 7.585, p = 0.019) and peg transfer (F1,11 = 23.046, p = 0.001) tasks.
3.2.3. Blink Frequency
There were significant main effects of the tasks (F1,11 = 5.016, p = 0.047) and vision systems (F1,11 = 6.003, p = 0.032) on blink frequency. The blink frequencies for the circle-tracing and peg transfer tasks were 14.84 (10.83) and 12.56 (10.08), and those for the 2D and 3D vision systems were 10.50 (7.19) and 16.90 (12.19). No significant interaction effect of task × vision system was found.
3.2.4. National Aeronautics and Space Administration Task Load Index (NASA TLX)
The means, standard deviations, and Analysis of Variance (ANOVA) results of NASA-TLX for the simulated task and vision system are presented in Table 1. For the 2D vision system, the subjective rating scores on mental demand (F1,11 = 5.805, p = 0.035), performance (F1,11 = 6.152, p = 0.031), frustration (F1,11 = 10.073, p = 0.009), and overall mental workload (F1,11 = 13.231, p = 0.004) were significantly higher than those for the 3D vision system. There were no significant main effects of the simulated tasks on the six independent components or overall mental workload. Significant interactions of simulated task × vision system (F1,11 = 6.205, p = 0.030) were found for mental demand (F1,11 = 4.978, p = 0.047), performance (F1,11 = 8.772, p = 0.013), frustration (F1,11 = 5.530, p = 0.038), and overall mental workload (F1,11 = 24.991, p = 0.001). The results of one-way ANOVA indicated that in the peg transfer task, mental demand, temporal demand, performance, frustration, and overall mental workload were significantly higher in the 2D condition than in the 3D condition.
4. Discussion
Visual dimensions had a significant effect on both surgery-related parameters, namely, completion time and precision, in the two dimensional laparoscopic tasks in this study. In the depth-perception peg transfer task, the mean completion time was significantly shorter with the 3D vision system than with the 2D system. This result is in line with most of the studies published to date [14]. This finding suggests that, in tasks requiring depth perception, a modern 3D vision system that provides high-resolution images may improve task performance, even if the task requires much time to complete [28]. In contrast, in the circle-tracing task, which does not require depth perception, the mean completion time was significantly shorter with the 2D system than with the 3D system. Early studies reported that there were no significant differences in the completion times of this type of task when 2D and 3D systems were used [52], and recent research has indicated that the 3D system confers an operating time advantage even on easy tasks [14,53]. Therefore, the finding of a longer manipulation time in this study contradicts previous findings.
In the pegboard task, the 3D condition provided significantly better performance than the 2D condition in terms of mean error frequency. Previous studies have ascribed this increased precision to the better depth perception provided by the 3D system [14,54,55]. However, in the 2D circle-tracing task, there were no significant differences in mean error frequency between the image vision systems.
In this study, the MUSE headband with its EEG function was used as a direct measure of cortical activity during laparoscopic simulations. This is in stark contrast to previously mentioned surrogate measures, which, instead of directly measuring brain activity, require downstream extrapolations. Gamma waves are associated with concentration, thought, and listening, while alpha waves reflect a state of a calm and balanced psychological state [56]. The results of this study indicated no significant differences in EEG alpha wave activity between the simulated laparoscopic tasks or vision systems. However, a significant interaction of simulated task × vision system was found. In the peg transfer task, EEG alpha wave activity was significantly higher in the 3D condition than in the 2D condition. This finding implies that participants experienced less stress with the 3D vision system while performing a depth perception task. In terms of EEG gamma wave activity, there were no significant differences between the two tasks, but significant main effects of the vision systems and an interaction of simulated task × vision system were found. These findings demonstrated that participants maintained a higher state of attentiveness with the 2D vision system in both levels of the simulated laparoscopic tasks with depth perception.
A strong advantage of using the blink rate to assess surgeons’ mental workload is that this technology allows continuous monitoring of changes in the mental status of the surgeon during a surgical procedure [44]. Reduction of blink frequency is associated with higher levels of mental workload [44,50,51]. In the present study, participants perceived a higher mental workload with the 2D vision system than with the 3D system and when performing the depth-perception task, as indicated by the lower blink frequency.
The subjective workload experienced by the participants was significantly reduced in three of the six NASA TLX weightings, indicating that the 3D vision system was not only tolerated but was better tolerated than the standard 2D system in terms of mental demand, satisfaction with performance and frustration. These findings indicated that participants required more mental and perceptual activity (decision-making, memory, and searching) and experienced higher levels of effort on performance and greater frustration when completing the tasks with the 2D vision system. This may translate into a perceived reduction in workload demand and fatigue when performing extended complex minimally invasive surgical procedures using 3D displays. The overall mental workload was approximately 38% higher for the 2D vision system, at 62.71, than for the 3D system, at 45.42. Thus, the NASA-TLX data indicate that performing laparoscopic tasks induces higher levels of mental workload in 2D than in 3D.
Although the present study demonstrated some positive results to support the purposes and hypotheses, the major limitation of this study is that all results were based on two simulated laparoscopic tasks with different levels of depth perception. To sufficiently understand the effects of visual dimensions on mental workload measures for evaluating the effectiveness of new surgical displays, more maneuvers in actual laparoscopic surgeries such as cutting, knotting, and suturing should be examined in future research.
5. Conclusions
The current study tested the effects of vision systems on performance and mental workload during different simulated laparoscopic tasks with depth perception. Based on the results of the study, the following conclusions can be drawn. First, the 3D vision system reduced the completion time and increased the precision in the depth-perception task, even when the duration of the simulated task was prolonged far beyond those reported in previous studies. However, the 3D vision system seemed to increase the completion time in a simple non-depth-perception task. Second, the EEG results indicated that participants experienced less stress with the 3D vision system while performing a depth-perception task, and they maintained a higher state of attentiveness with the 2D vision system in both levels of simulated laparoscopic tasks with depth perception. Third, participants perceived a higher mental workload with the 2D vision system and when performing the depth-perception task, as indicated by the lower blink frequency. Finally, the NASA-TLX data indicated that laparoscopic tasks induce higher levels of subjective mental workload in 2D than in 3D.
Author Contributions
Conceptualization, H.-J.C. and C.J.L.; methodology, H.-J.C. and C.J.L.; software, Z.-H.G.; validation, H.-J.C., P.-H.L. and C.J.L.; formal analysis, H.-J.C.; investigation, H.-J.C. and P.-H.L.; resources, H.-J.C. and C.J.L.; data curation, Z.-H.G.; writing—original draft preparation, H.-J.C.; writing—review and editing, H.-J.C.; visualization, Z.-H.G.; supervision, H.-J.C.; project administration, H.-J.C.; funding acquisition, H.-J.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was subsidized and supported by a Grant from the Ministry of Science and Technology, Taiwan (Project No. MOST 105-2218-E-011-009-MY2).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of National Taiwan University (protocol code NTU-REC No.: 201302HS009 and approval date: 27 May 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Buchs, N.C.; Morel, P. Three-dimensional laparoscopy: A new tool in the surgeon’s armamentarium. Surg. Technol. Int. 2013, 23, 19–22. [Google Scholar] [PubMed]
- Wagner, O.; Hagen, M.; Kurmann, A.; Horgan, S.; Candinas, D.; Vorburger, S. Three-dimensional vision enhances task performance independently of the surgical method. Surg. Endosc. 2012, 26, 2961–2968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, L.; Stein, A.; Fachel, J.; Garry, R.; Furness, S. Laparoscopy versus laparotomy for benign ovarian tumor: A systematic review and meta-analysis. Int. J. Gynecol. Cancer 2008, 18, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Sahu, D.; Mathew, M.J.; Reddy, P.K. 3D Laparoscopy-help or hype; initial experience of a tertiary health centre. J. Clin. Diagn. Res. JCDR 2014, 8, NC01. [Google Scholar] [PubMed]
- Taffinder, N.; Smith, S.; Huber, J.; Russell, R.; Darzi, A. The effect of a second-generation 3D endoscope on the laparoscopic precision of novices and experienced surgeons. Surg. Endosc. 1999, 13, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, D.; Reiser, S.; Kohn, N.; Witte, M.; Leiner, U.; Mühlbach, L.; Ruschin, D.; Reiner, W.; Feussner, H. Comparative evaluation of HD 2D/3D laparoscopic monitors and benchmarking to a theoretically ideal 3D pseudodisplay: Even well-experienced laparoscopists perform better with 3D. Surg. Endosc. 2014, 28, 2387–2397. [Google Scholar] [CrossRef] [PubMed]
- Lusch, A.; Bucur, P.L.; Menhadji, A.D.; Okhunov, Z.; Liss, M.A.; Perez-Lanzac, A.; McDougall, E.M.; Landman, J. Evaluation of the impact of three-dimensional vision on laparoscopic performance. J. Endourol. 2014, 28, 261–266. [Google Scholar] [CrossRef]
- Kong, S.-H.; Oh, B.-M.; Yoon, H.; Ahn, H.S.; Lee, H.-J.; Chung, S.G.; Shiraishi, N.; Kitano, S.; Yang, H.-K. Comparison of two-and three-dimensional camera systems in laparoscopic performance: A novel 3D system with one camera. Surg. Endosc. 2010, 24, 1132–1143. [Google Scholar] [CrossRef]
- Smith, R.; Schwab, K.; Day, A.; Rockall, T.; Ballard, K.; Bailey, M.; Jourdan, I. Effect of passive polarizing three-dimensional displays on surgical performance for experienced laparoscopic surgeons. Br. J. Surg. 2014, 101, 1453–1459. [Google Scholar] [CrossRef]
- Carswell, C.M.; Clarke, D.; Seales, W.B. Assessing mental workload during laparoscopic surgery. Surg. Innov. 2005, 12, 80–90. [Google Scholar] [CrossRef]
- Yurko, Y.Y.; Scerbo, M.W.; Prabhu, A.S.; Acker, C.E.; Stefanidis, D. Higher mental workload is associated with poorer laparoscopic performance as measured by the NASA-TLX tool. Simul. Healthc. 2010, 5, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Falk, V.; Mintz, D.; Grunenfelder, J.; Fann, J.; Burdon, T. Influence of three-dimensional vision on surgical telemanipulator performance. Surg. Endosc. 2001, 15, 1282–1288. [Google Scholar] [CrossRef] [PubMed]
- Zdichavsky, M.; Schmidt, A.; Luithle, T.; Manncke, S.; Fuchs, J. Three-dimensional laparoscopy and thoracoscopy in children and adults: A prospective clinical trial. Minim. Invasive Ther. Allied Technol. 2015, 24, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, S.M.D.; Savran, M.M.; Konge, L.; Bjerrum, F. Three-dimensional versus two-dimensional vision in laparoscopy: A systematic review. Surg. Endosc. 2016, 30, 11–23. [Google Scholar] [CrossRef]
- Fergo, C.; Burcharth, J.; Pommergaard, H.-C.; Kildebro, N.; Rosenberg, J. Three-dimensional laparoscopy vs. 2-dimensional laparoscopy with high-definition technology for abdominal surgery: A systematic review. Am. J. Surg. 2017, 213, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Liang, W.; Lei, Z.; Liu, Z.; Wang, W.; He, J.; Zeng, Y.; Huang, W.; Wang, M.; Chen, Y. Three-Dimensional Versus Two-Dimensional Video-Assisted Endoscopic Surgery: A Meta-analysis of Clinical Data. World J. Surg. 2018, 42, 3658–3668. [Google Scholar] [CrossRef]
- Kyriazis, I.; Özsoy, M.; Kallidonis, P.; Vasilas, M.; Panagopoulos, V.; Liatsikos, E. Integrating three-dimensional vision in laparoscopy: The learning curve of an expert. J. Endourol. 2015, 29, 657–660. [Google Scholar] [CrossRef]
- Özsoy, M.; Kallidonis, P.; Kyriazis, I.; Panagopoulos, V.; Vasilas, M.; Sakellaropoulos, G.C.; Liatsikos, E. Novice surgeons: Do they benefit from 3D laparoscopy? Lasers Med. Sci. 2015, 30, 1325–1333. [Google Scholar] [CrossRef]
- Stylopoulos, N.; Cotin, S.; Maithel, S.; Ottensmeyer, M.; Jackson, P.; Bardsley, R.; Neumann, P.; Rattner, D.; Dawson, S. Computer-enhanced laparoscopic training system (CELTS): Bridging the gap. Surg. Endosc. Interv. Tech. 2004, 18, 782–789. [Google Scholar] [CrossRef]
- Chung, J.; Sackier, J. A method of objectively evaluating improvements in laparoscopic skills. Surg. Endosc. 1998, 12, 1111–1116. [Google Scholar] [CrossRef]
- Rosser, J.C.; Rosser, L.E.; Savalgi, R.S. Skill acquisition and assessment for laparoscopic surgery. Arch. Surg. 1997, 132, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Tanagho, Y.S.; Andriole, G.L.; Paradis, A.G.; Madison, K.M.; Sandhu, G.S.; Varela, J.E.; Benway, B.M. 2D versus 3D visualization: Impact on laparoscopic proficiency using the fundamentals of laparoscopic surgery skill set. J. Laparoendosc. Adv. Surg. Tech. 2012, 22, 865–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research. In Advances in Psychology; Elsevier: Amsterdam, The Netherlands, 1988; Volume 52, pp. 139–183. [Google Scholar]
- Foo, J.-L.; Martinez-Escobar, M.; Juhnke, B.; Cassidy, K.; Hisley, K.; Lobe, T.; Winer, E. Evaluating mental workload of two-dimensional and three-dimensional visualization for anatomical structure localization. J. Laparoendosc. Adv. Surg. Tech. 2013, 23, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, E.; Carrasco-Valiente, J.; Valero-Rosa, J.; Campos-Hernandez, J.; Anglada-Curado, F.; Carazo-Carazo, J.; Font-Ugalde, P.; Requena-Tapia, M. Impact of 3D vision on mental workload and laparoscopic performance in inexperienced subjects. Actas Urológicas Españolas (Engl. Ed.) 2015, 39, 229–235. [Google Scholar] [CrossRef]
- Marcus, H.J.; Hughes-Hallett, A.; Cundy, T.P.; Di Marco, A.; Pratt, P.; Nandi, D.; Darzi, A.; Yang, G.-Z. Comparative effectiveness of 3-dimensional vs 2-dimensional and high-definition vs standard-definition neuroendoscopy: A preclinical randomized crossover study. Neurosurgery 2013, 74, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buia, A.; Stockhausen, F.; Filmann, N.; Hanisch, E. 2D vs. 3D imaging in laparoscopic surgery—Results of a prospective randomized trial. Langenbeck’s Arch. Surg. 2017, 402, 1241–1253. [Google Scholar] [CrossRef]
- Lin, C.J.; Cheng, C.-F.; Chen, H.-J.; Wu, K.-Y. Training Performance of Laparoscopic Surgery in Two-and Three-Dimensional Displays. Surg. Innov. 2017, 24, 162–170. [Google Scholar] [CrossRef]
- Alaraimi, B.; El Bakbak, W.; Sarker, S.; Makkiyah, S.; Al-Marzouq, A.; Goriparthi, R.; Bouhelal, A.; Quan, V.; Patel, B. A randomized prospective study comparing acquisition of laparoscopic skills in three-dimensional (3D) vs. two-dimensional (2D) laparoscopy. World J. Surg. 2014, 38, 2746–2752. [Google Scholar] [CrossRef]
- Pietrabissa, A.; Scarcello, E.; Carobbi, A.; Mosca, F. Three-dimensional versus two-dimensional video system for the trained endoscopic surgeon and the beginner. Endosc. Surg. Allied Technol. 1994, 2, 315–317. [Google Scholar]
- Storz, P.; Buess, G.F.; Kunert, W.; Kirschniak, A. 3D HD versus 2D HD: Surgical task efficiency in standardised phantom tasks. Surg. Endosc. 2012, 26, 1454–1460. [Google Scholar] [CrossRef]
- Smith, R.; Day, A.; Rockall, T.; Ballard, K.; Bailey, M.; Jourdan, I. Advanced stereoscopic projection technology significantly improves novice performance of minimally invasive surgical skills. Surg. Endosc. 2012, 26, 1522–1527. [Google Scholar] [CrossRef] [PubMed]
- Nygren, T.E. Psychometric properties of subjective workload measurement techniques: Implications for their use in the assessment of perceived mental workload. Human Factors 1991, 33, 17–33. [Google Scholar] [CrossRef]
- Berquer, R.; Smith, W.D.; Davis, S. An ergonomic study of the optimum operating table height for laparoscopic surgery. Surg. Endosc. 2002, 16, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Sakata, S.; Watson, M.O.; Grove, P.M.; Stevenson, A.R. The conflicting evidence of three-dimensional displays in laparoscopy: A review of systems old and new. Ann. Surgery 2016, 263, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.J. Crosstalk in stereoscopic displays: A review. J. Electron. Imaging 2012, 21, 040902. [Google Scholar] [CrossRef]
- Lee, C.-T.; Lin, H.-Y.; Tsai, C.-H. Designs of broadband and wide-view patterned polarizers for stereoscopic 3D displays. Opt. Express 2010, 18, 27079–27094. [Google Scholar] [CrossRef]
- Salmimaa, M.; Järvenpää, T. 3-D crosstalk and luminance uniformity from angular luminance profiles of multiview autostereoscopic 3-D displays. J. Soc. Inf. Disp. 2008, 16, 1033–1040. [Google Scholar] [CrossRef]
- Krigolson, O.E.; Williams, C.C.; Norton, A.; Hassall, C.D.; Colino, F.L. Choosing MUSE: Validation of a low-cost, portable EEG system for ERP research. Front. Neurosci. 2017, 11, 109. [Google Scholar] [CrossRef] [Green Version]
- Abujelala, M.; Abellanoza, C.; Sharma, A.; Makedon, F. Brain-EE: Brain enjoyment evaluation using commercial EEG headband. In Proceedings of the 9th ACM International Conference on Pervasive Technologies Related to Assistive Environments, Corfu Island, Greece, 29 June–1 July 2016; p. 33. [Google Scholar]
- Viriyasiripong, S.; Lopez, A.; Mandava, S.H.; Lai, W.R.; Mitchell, G.C.; Boonjindasup, A.; Powers, M.K.; Silberstein, J.L.; Lee, B.R. Accelerometer measurement of head movement during laparoscopic surgery as a tool to evaluate skill development of surgeons. J. Surg. Educ. 2016, 73, 589–594. [Google Scholar] [CrossRef]
- Leape, C.; Fong, A.; Ratwani, R.M. Heuristic usability evaluation of wearable mental state monitoring sensors for healthcare environments. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; Sage: Los Angeles, CA, USA, 2016; pp. 583–587. [Google Scholar]
- Maddox, M.M.; Lopez, A.; Mandava, S.H.; Boonjindasup, A.; Viriyasiripong, S.; Silberstein, J.L.; Lee, B.R. Electroencephalographic Monitoring of Brain Wave Activity During Laparoscopic Surgical Simulation to Measure Surgeon Concentration and Stress: Can the Student Become the Master? J. Endourol. 2015, 29, 1329–1333. [Google Scholar] [CrossRef]
- Zheng, B.; Jiang, X.; Tien, G.; Meneghetti, A.; Panton, O.N.M.; Atkins, M.S. Workload assessment of surgeons: Correlation between NASA TLX and blinks. Surg. Endosc. 2012, 26, 2746–2750. [Google Scholar] [CrossRef] [PubMed]
- Stefanidis, D.; Haluck, R.; Pham, T.; Dunne, J.B.; Reinke, T.; Markley, S.; Korndorffer, J.R.; Arellano, P.; Jones, D.B.; Scott, D.J. Construct and face validity and task workload for laparoscopic camera navigation: Virtual reality versus videotrainer systems at the SAGES Learning Center. Surg. Endosc. 2007, 21, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Berguer, R.; Smith, W. An ergonomic comparison of robotic and laparoscopic technique: The influence of surgeon experience and task complexity. J. Surg. Res. 2006, 134, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Ritter, E.M.; Scott, D.J. Design of a proficiency-based skills training curriculum for the fundamentals of laparoscopic surgery. Surg. Innov. 2007, 14, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, E.; da Silva, F.L. Electroencephalography: Basic Principles, Clinical Applications, and Related Fields; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Pfurtscheller, G.; Da Silva, F.L. Event-related EEG/MEG synchronization and desynchronization: Basic principles. Clin. Neurophysiol. 1999, 110, 1842–1857. [Google Scholar] [CrossRef]
- Wilson, G.F. Air-to-ground training missions: A psychophysiological workload analysis. Ergonomics 1993, 36, 1071–1087. [Google Scholar] [CrossRef]
- Martins, R.; Carvalho, J. Eye blinking as an indicator of fatigue and mental load-a systematic review. In Occupational Safety and Hygiene III; CRC Press: Boca Raton, FL, USA, 2015; p. 10. [Google Scholar]
- Hofmeister, J.; Frank, T.G.; Cuschieri, A.; Wade, N.J. Perceptual aspects of two-dimensional and stereoscopic display techniques in endoscopic surgery: Review and current problems. In Seminars in Laparoscopic Surgery; Sage Publications: Thousand Oaks, CA, USA; pp. 12–24.
- Currò, G.; La Malfa, G.; Caizzone, A.; Rampulla, V.; Navarra, G. Three-dimensional (3D) versus two-dimensional (2D) laparoscopic bariatric surgery: A single-surgeon prospective randomized comparative study. Obes. Surg. 2015, 25, 2120–2124. [Google Scholar] [CrossRef]
- Van Beurden, M.H.; IJsselsteijn, W.A.; Juola, J.F. Effectiveness of stereoscopic displays in medicine: A review. 3D Res. 2012, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- McIntire, J.P.; Havig, P.R.; Geiselman, E.E. Stereoscopic 3D displays and human performance: A comprehensive review. Displays 2014, 35, 18–26. [Google Scholar] [CrossRef]
- Seo, S.-H.; Lee, J.-T. Stress and EEG. In Convergence and Hybrid Information Technologies; InTech: Vienna, Austria, 2010. [Google Scholar]
Figure 1.
Experimental environment.

Figure 2.
Peg transfer task.

Figure 3.
The digitizer tablet and modified Endo Babcock clamp with a digital pen used in the circle-tracing task.
Figure 3.
The digitizer tablet and modified Endo Babcock clamp with a digital pen used in the circle-tracing task.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Means, standard deviations (SDs), and Analysis of Variance (ANOVA) results of National Aeronautics and Space Administration Task Load Index (NASA-TLX) for the simulated task and vision system.
Table 1.
Means, standard deviations (SDs), and Analysis of Variance (ANOVA) results of National Aeronautics and Space Administration Task Load Index (NASA-TLX) for the simulated task and vision system.
| Performance | Factor | Level | Mean | SD | F1, 11 | p-Value |
|---|---|---|---|---|---|---|
| Mental demand | Simulated task | Circle-tracing | 61.88 | 21.25 | 0.057 | 0.816 |
| Peg transfer | 63.13 | 21.51 | ||||
| Vision system | 2D | 66.67 | 20.20 | 5.805 | 0.035 | |
| 3D | 58.33 | 21.70 | ||||
| Physical demands | Simulated task | Circle-tracing | 80.42 | 18.70 | 4.299 | 0.062 |
| Peg transfer | 68.75 | 19.90 | ||||
| Vision system | 2D | 76.25 | 19.01 | 0.413 | 0.534 | |
| 3D | 72.92 | 21.21 | ||||
| Temporal demand | Simulated task | Circle-tracing | 61.25 | 25.51 | 1.915 | 0.194 |
| Peg transfer | 48.75 | 23.37 | ||||
| Vision system | 2D | 57.71 | 27.58 | 3.733 | 0.080 | |
| 3D | 52.29 | 22.41 | ||||
| Performance | Simulated task | Circle-tracing | 45.63 | 19.69 | 0.001 | 0.972 |
| Peg transfer | 45.83 | 25.18 | ||||
| Vision system | 2D | 52.71 | 24.14 | 6.152 | 0.031 | |
| 3D | 38.75 | 18.37 | ||||
| Effort | Simulated task | Circle-tracing | 66.46 | 16.91 | 0.799 | 0.391 |
| Peg transfer | 70.83 | 15.72 | ||||
| Vision system | 2D | 71.04 | 14.22 | 1.431 | 0.257 | |
| 3D | 66.25 | 18.13 | ||||
| Frustration | Simulated task | Circle-tracing | 52.71 | 23.36 | 0.132 | 0.723 |
| Peg transfer | 55.42 | 24.58 | ||||
| Vision system | 2D | 62.71 | 22.21 | 10.073 | 0.009 | |
| 3D | 45.42 | 22.45 | ||||
| NASA-TLX scores | Simulated task | Circle-tracing | 66.40 | 15.45 | 0.395 | 0.542 |
| Peg transfer | 63.58 | 12.80 | ||||
| Vision system | 2D | 68.15 | 14.40 | 13.231 | 0.004 | |
| 3D | 61.83 | 13.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, H.-J.; Lin, C.J.; Lin, P.-H.; Guo, Z.-H. The Effects of 3D and 2D Imaging on Brain Wave Activity in Laparoscopic Training. Appl. Sci. 2021, 11, 862. https://0-doi-org.brum.beds.ac.uk/10.3390/app11020862
AMA Style
Chen H-J, Lin CJ, Lin P-H, Guo Z-H. The Effects of 3D and 2D Imaging on Brain Wave Activity in Laparoscopic Training. Applied Sciences. 2021; 11(2):862. https://0-doi-org.brum.beds.ac.uk/10.3390/app11020862
Chicago/Turabian StyleChen, Hung-Jen, Chiuhsiang Joe Lin, Po-Hung Lin, and Zong-Han Guo. 2021. "The Effects of 3D and 2D Imaging on Brain Wave Activity in Laparoscopic Training" Applied Sciences 11, no. 2: 862. https://0-doi-org.brum.beds.ac.uk/10.3390/app11020862
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.