
Intensive Rehabilitation Program in Arterial Occlusive Disease Patients

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject
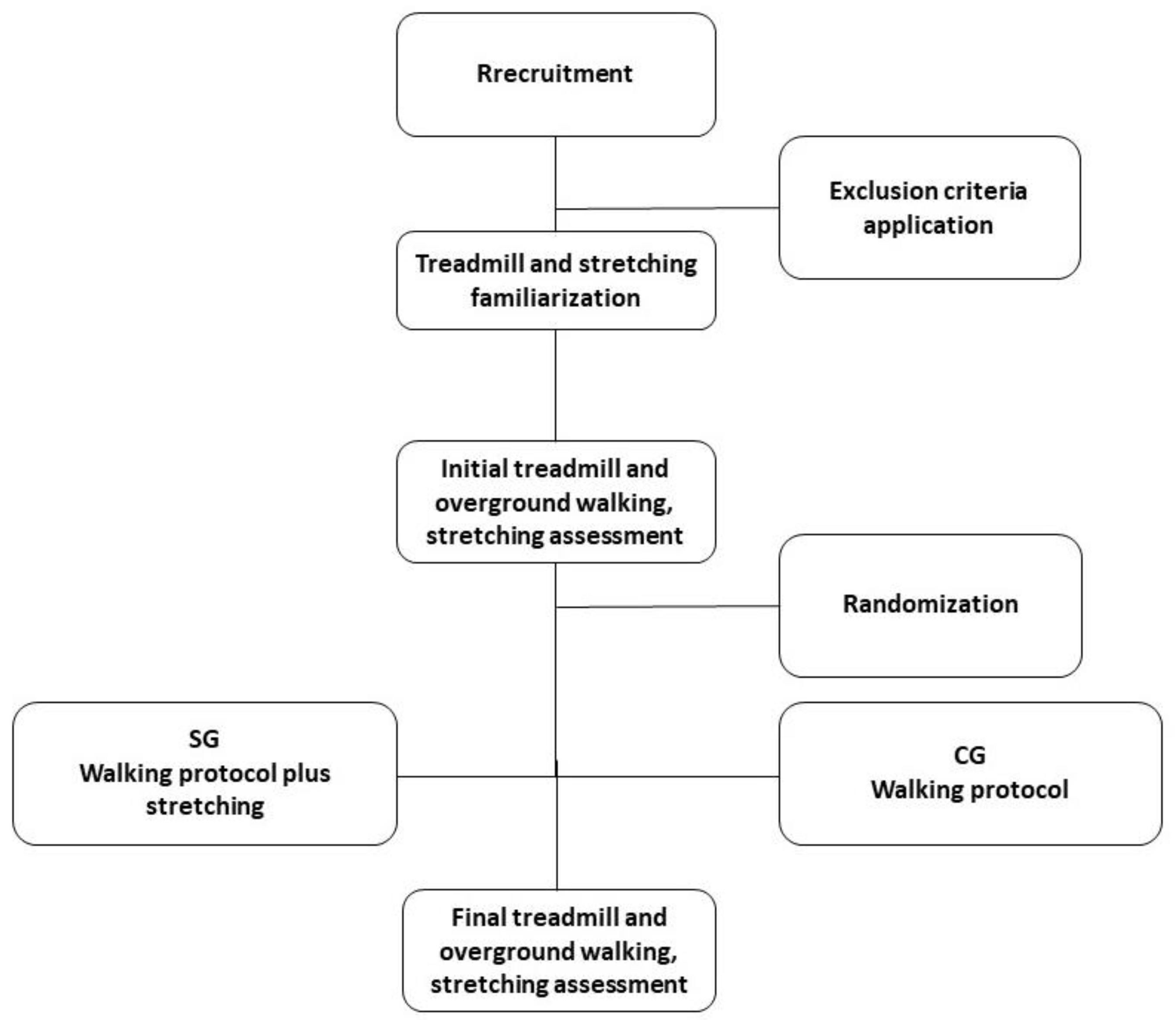
2.2. Procedure
2.3. Treadmill Test
2.4. Walking Test
2.5. Termination Test Criteria
2.6. Flexibility Test
Rehabilitation Protocol
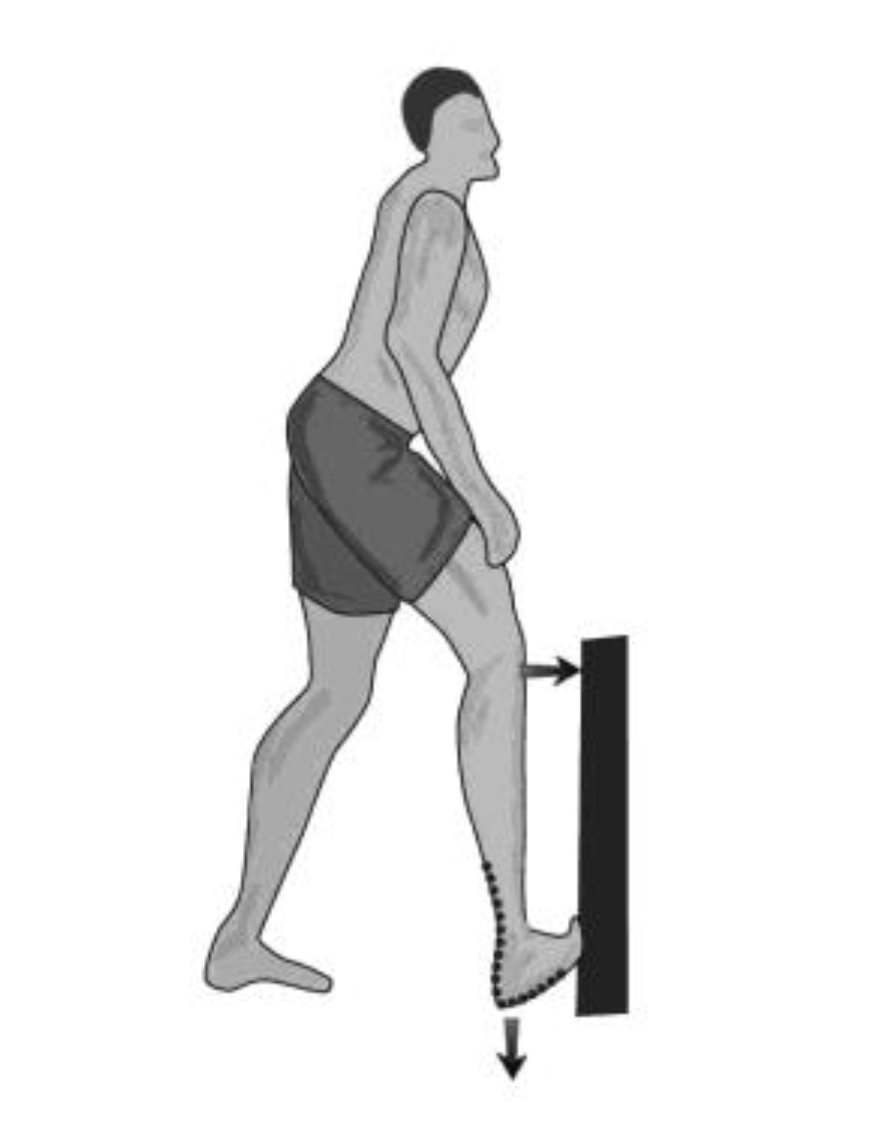
2.7. Stretching Protocol
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Muller, M.D.; Reed, A.B.; Leuenberger, U.A.; Sinoway, L.I. Physiology in Medicine: Peripheral arterial disease. J. Appl. Physiol. 2013, 115, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R.; Rutherford, R.B. Inter-Society Consensus for the management of peripheral arterial disease (TASC II). Int. Angiol. 2007, 26, 82–157. [Google Scholar] [CrossRef] [Green Version]
- Leng, G.C.; Lee, A.J.; Fowkes, F.G.R.; Whiteman, M.; Dunbar, J.; Housley, E.; Vaughan Ruckley, C. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int. J. Epidemiol. 1996, 25, 1172–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artigao-Rodenas, L.M.; Carbayo-Herencia, J.A.; Divisón-Garrote, J.A.; Gil-Guillén, V.F.; Massó-Orozco, J.; Simarro-Rueda, M.; Molina-Escribano, F.; Sanchis, C.; Carrión-Valero, L.; López de Coca, E.; et al. Framingham risk score for prediction of cardiovascular diseases: A population-based study from southern Europe. PLoS ONE 2013, 8, e73529. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.C.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): Executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vas. J. Am. Coll. Cardiol. 2006, 47, 1239–1312. [Google Scholar] [CrossRef] [Green Version]
- Cousin, A.; Popielarz, S.; Wieczorek, V.; Tiffreau, V.; Mounier-Vehier, C.; Thevenon, A. Impact of a rehabilitation program on muscular strength and endurance in peripheral arterial occlusive disease patients. Ann. Phys. Rehabil. Med. 2011, 54, 429–442. [Google Scholar] [CrossRef] [Green Version]
- Patterson, R.B.; Pinto, B.; Marcus, B.; Colucci, A.; Braun, T.; Roberts, M. Value of a supervised exercise program for the therapy of arterial claudication. J. Vasc. Surg. 1997, 25, 312–318, discussion 318-9. [Google Scholar] [CrossRef] [Green Version]
- Bendermacher, B.L.W.; Willigendael, E.M.; Teijink, J.A.W.; Prins, M.H. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst. Rev. 2006, CD005263. [Google Scholar] [CrossRef] [Green Version]
- Crowther, R.; Spinks, W.; Leicht, A.; Sangla, K.; Quigley, F.; Golledge, J. Effects of a long-term exercise program on lower limb mobility, physiological responses, walking performance, and physical activity levels in patients with peripheral arterial disease. JVS 2008, 47, 303–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gahier, M.; Hersant, J.; Hamel, J.F.; Sempore, Y.; Bruneau, A.; Henni, S.; Abraham, P. A Simple Scale for Screening Lower-Extremity Arterial Disease as a Possible Cause of Low Back Pain: A Cross-sectional Study Among 542 Subjects. J. Gen. Intern. Med. 2020, 35, 1963–1970. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Katzel, L.I.; Sorkin, J.D.; Bradham, D.D.; Hochberg, M.C.; Flinn, W.R.; Goldberg, A.P. Exercise rehabilitation improves functional outcomes and peripheral circulation in patients with intermittent claudication: A randomized controlled trial. J. Am. Geriatr. Soc. 2001, 49, 755–762. [Google Scholar] [CrossRef]
- Radford, J.A.; Burns, J.; Buchbinder, R.; Landorf, K.B.; Cook, C. Does stretching increase ankle dorsiflexion range of motion? A systematic review. Br. J. Sports Med. 2006, 40, 870–875, discussion 875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, R.; Nix, S.; Wholohan, A.; Bradhurst, R.; Reed, L. Interventions for increasing ankle joint dorsiflexion: A systematic review and meta-analysis. J. Foot Ankle Res. 2013, 6, 46. [Google Scholar] [CrossRef] [Green Version]
- Shephard, R.J.; Berridge, M.; Montelpare, W. On the generality of the “sit and reach” test: An analysis of flexibility data for an aging population. Res. Q. Exerc. Sport 1990, 61, 326–330. [Google Scholar] [CrossRef]
- Christiansen, C.L. The effects of hip and ankle stretching on gait function of older people. Arch. Phys. Med. Rehabil. 2008, 89, 1421–1428. [Google Scholar] [CrossRef]
- Watt, J.; Jackson, K.; Franz, J.; Dicharry, J.; Evans, J.; Kerringan, D. Effect of a supervised hip flexor stretching program on gait in frail elderly patients. PM&R 2011, 3, 330–335. [Google Scholar]
- Regensteiner, J.; Gardner, A.; Hiatt, W. Exercise testing and exercise rehabilitation for patients with peripheral arterial disease: Status in 1997. Vasc. Med. 1997, 2, 147–155. [Google Scholar] [CrossRef]
- Gibellini, R.; Ferrari, B.; Zambelli, M.; Fanello, M. La riabilitazione in Angiologia. Phlebologie-Paris 1997, 50, 455. [Google Scholar]
- Mayorga-Vega, D.; Merino-Marban, R.; Viciana, J. Criterion-Related Validity of Sit-and-Reach Tests for Estimating Hamstring and Lumbar Extensibility: A Meta-Analysis. J. Sports Sci. Med. 2014, 13, 1–14. [Google Scholar] [PubMed]
- Bohannon, R.; Tiberio, D.; Zito, M. Effect of five minute stretch on ankle dorsiflexion range of motion. J. Phys. Ther. Sci. 1994, 6, 1–8. [Google Scholar]
- Hamburg, N.M.; Balady, G.J. Exercise rehabilitation in peripheral artery disease: Functional impact and mechanisms of benefits. Circulation 2011, 123, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisconti, A.V.; Cè, E.; Longo, S.; Venturelli, M.; Coratella, G.; Limonta, E.; Doria, C.; Rampichini, S.; Esposito, F. Evidence for improved systemic and local vascular function after long-term passive static stretching training of the musculoskeletal system. J. Physiol. 2020, 598, 3645–3666. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Lesinski, M.; Gäbler, M.; VanSwearingen, J.M.; Malatesta, D.; Granacher, U. Effects of Three Types of Exercise Interventions on Healthy Old Adults’ Gait Speed: A Systematic Review and Meta-Analysis. Sport. Med. 2015, 45, 1627–1643. [Google Scholar] [CrossRef] [Green Version]
- Zakari, M.; Alsahly, M.; Koch, L.G.; Britton, S.L.; Katwa, L.C.; Lust, R.M. Are There Limitations to Exercise Benefits in Peripheral Arterial Disease? Front. Cardiovasc. Med. 2018, 5, 173. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Series N | Repetition n | Time (s) | Recovery (s) |
|---|---|---|---|
| 1 | 3 | 30 | 30 |
| 2 | 3 | 45 | 45 |
| 3 | 4 | 45 | 45 |
| 4 | 4 | 60 | 60 |
| 5 | 5 | 60 | 60 |
| SG | CG | |||
|---|---|---|---|---|
| Outcome | ||||
| WICP | 190.4 ± 97.5 | 302.7 ± 113.5 | 165.6 ± 77.1 | 222.8 ± 77.1 * |
| WACP | 292.6 ± 118.3 | 400.7 ± 135.3 * | 251.8 ± 113.1 | 355.7 ± 146.4 * |
| TICP | 188.0 ± 80.4 | 300.5 ± 100.5 * | 181.8 ± 63.3 | 314.2 ± 109.1 * |
| TACP | 283.9 ± 105.7 | 402.5 ± 113.9 * | 256.4 ± 82.2 | 408.9 ± 116.0 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, L.; Lovecchio, N.; Kawczynski, A.; Febbi, M.; Silvestri, D.; Pellino, V.C.; Gibellini, R.; Vandoni, M. Intensive Rehabilitation Program in Arterial Occlusive Disease Patients. Appl. Sci. 2021, 11, 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031184
Marin L, Lovecchio N, Kawczynski A, Febbi M, Silvestri D, Pellino VC, Gibellini R, Vandoni M. Intensive Rehabilitation Program in Arterial Occlusive Disease Patients. Applied Sciences. 2021; 11(3):1184. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031184
Chicago/Turabian StyleMarin, Luca, Nicola Lovecchio, Adam Kawczynski, Massimiliano Febbi, Dario Silvestri, Vittoria Carnevale Pellino, Raffaele Gibellini, and Matteo Vandoni. 2021. "Intensive Rehabilitation Program in Arterial Occlusive Disease Patients" Applied Sciences 11, no. 3: 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/app11031184