
Efficacy of TENS in Cervical Pain Syndromes: An Umbrella Review of Systematic Reviews

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
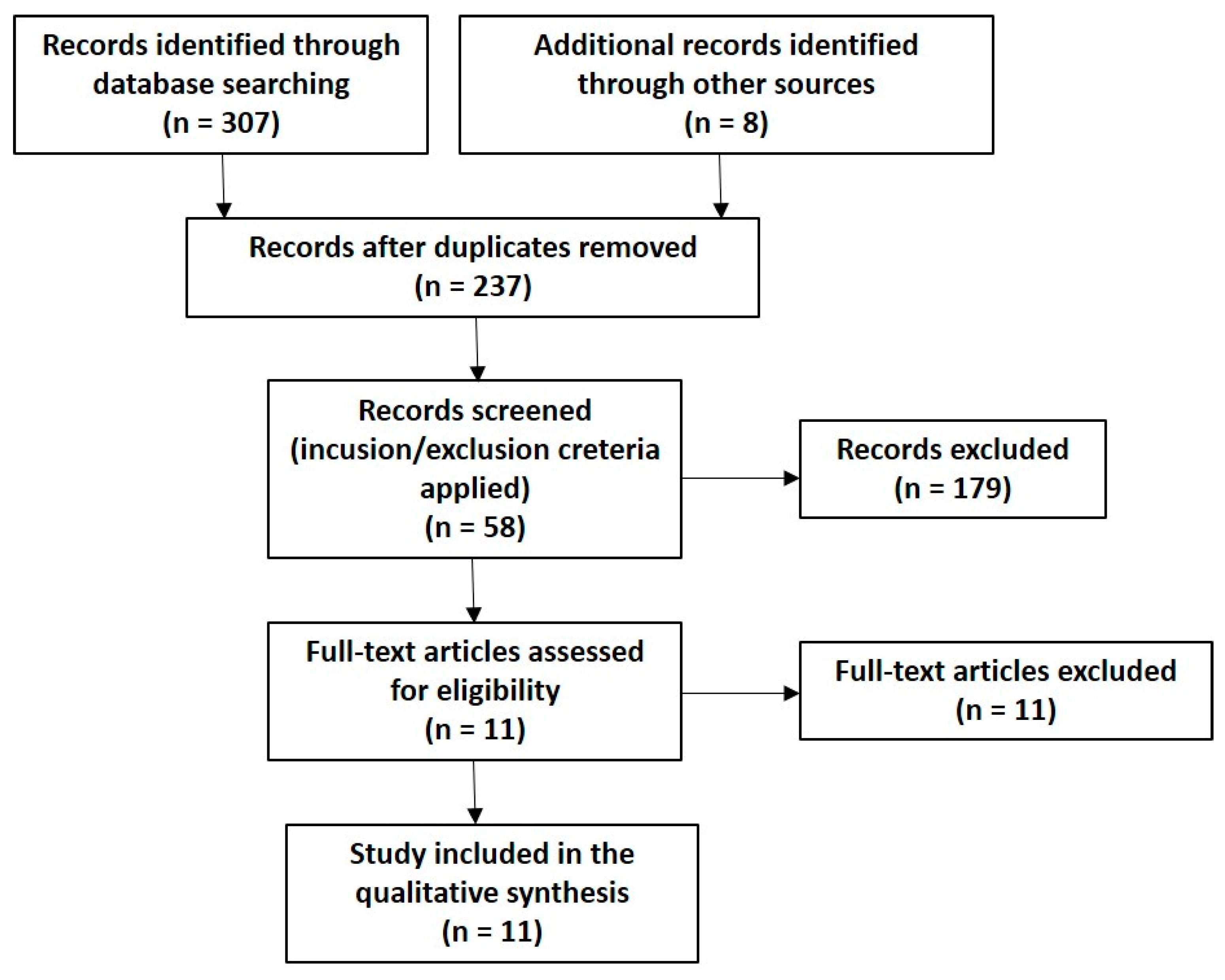
2.1. Research Strategy
2.2. P.I.C.O.
2.3. Inclusion/Exclusion Criteria
2.4. Quality of Study Evaluation
3. Results
4. Discussion
Implications for Future Research and Clinical Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, S.P. Epidemiology, Diagnosis, and Treatment of Neck Pain. Mayo Clin. Proc. 2015, 90, 284–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangone, M.; Paoloni, M.; Procopio, S.; Venditto, T.; Zucchi, B.; Santilli, V.; Paolucci, T.; Agostini, F.; Bernetti, A. Sagittal spinal alignment in patients with ankylosing spondylitis by rasterstereographic back shape analysis: An observational retrospective study. Eur. J. Phys. Rehabil. Med. 2020, 56, 191–196. [Google Scholar] [CrossRef]
- Mangone, M.; Bernetti, A.; Agostini, F.; Paoloni, M.; De Cicco, F.A.; Capobianco, S.V.; Bai, A.V.; Bonifacino, A.; Santilli, V.; Paolucci, T. Changes in Spine Alignment and Postural Balance After Breast Cancer Surgery: A Rehabilitative Point of View. Biores Open Access 2019, 8, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gimigliano, F.; De Sire, A.; Gastaldo, M.; Maghini, I.; Paoletta, M.; Pasquini, A.; Boldrini, P.; Selb, M.; Prodinger, B.; SIMFER Residents Section Group. Use of the International Classification of Functioning, Disability and Health Generic-30 Set for the characterization of outpatients: Italian Society of Physical and Rehabilitative Medicine Residents Section Project. Eur. J. Phys. Rehabil. Med. 2019, 55, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; Agostini, F.; De Sire, A.; Mangone, M.; Tognolo, L.; Di Cesare, A.; Ruiu, P.; Paolucci, T.; Invernizzi, M.; Paoloni, M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics 2021, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Côté, P.; Cassidy, D.J.; Carroll, L.J.; Kristman, V. The annual incidence and course of neck pain in the general population: A population-based cohort study. Pain 2004, 112, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Damiani, C.; Mangone, M.; Paoloni, M.; Goffredo, M.; Franceschini, M.; Servidio, M.; Pournajaf, S.; Santilli, V.; Agostini, F.; Bernetti, A. Trade-Offs with rehabilitation Effectiveness (REs) and Efficiency (REy) in a sample of Italian disabled persons in a in post-acuity rehabilitation unit. Ann. Ig. 2020, 32, 327–335. [Google Scholar] [PubMed]
- Liu, R.; Kurihara, C.; Tsai, H.T.; Silvestri, P.J.; Bennett, M.I.; Pasquina, P.F.; Cohen, S.P. Classification and Treatment of Chronic Neck Pain: A Longitudinal Cohort Study. Reg. Anesth. Pain Med. 2017, 42, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; Di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief. 2020, 30, 105419. [Google Scholar] [CrossRef]
- Montemurro, N.; Perrini, P.; Mangini, V.; Galli, M.; Papini, A. The Y-shaped trabecular bone structure in the odontoid process of the axis: A CT scan study in 54 healthy subjects and biomechanical considerations. J. Neurosurg. Spine 2019, 30, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Jaumard, N.V.; Udupa, J.K.; Welch, W.C.; Winkelstein, B.A. Kinematic magnetic resonance imaging to define the cervical facet joint space for the spine in neutral and torsion. Spine 2014, 39, 664–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanaugh, J.M.; Lu, Y.; Chen, C.; Kallakuri, S. Pain generation in lumbar and cervical facet joints. J. Bone Joint. Surg Am. 2006, 88 (Suppl. 2), 63–67. [Google Scholar] [PubMed]
- Masiero, S.; Litwocenko, S.; Agostini, F.; On behalf section of Rehabilitation in Environ-mental Thermal for Italian Society of Physical Medicine and Rehabilitation. Rehabilitation in an Italian thermal setting: A new therapeutic strategy for patients with musculoskeletal disability-the results of an Italian survey. Int. J. Biometeorol. 2020, 64, 951–954. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Agostini, F.; Lippi, L.; Mangone, M.; Marchese, S.; Cisari, C.; Bernetti, A.; Invernizzi, M. Oxygen-Ozone Therapy in the Rehabilitation Field: State of the Art on Mechanisms of Action, Safety and Effectiveness in Patients with Musculoskeletal Disorders. Biomolecules 2021, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; Cardarola, A.; Colonnelli, P.; Ferracuti, G.; Gonnella, R.; Murgia, M.; Santilli, V.; Paoloni, M.; Bernetti, A.; Agostini, F.; et al. Give me a kiss! An integrative rehabilitative training program with motor imagery and mirror therapy for recovery of facial palsy. Eur. J. Phys. Rehabil. Med. 2020, 56, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Vernon, H.T.; Humphreys, B.K.; Hagino, C.A. A systematic review of conservative treatments for acute neck pain not due to whiplash. J. Manip. Physiol. Ther. 2005, 28, 443–448. [Google Scholar] [CrossRef]
- Haines, T.; Gross, A.R.; Burnie, S.; Goldsmith, C.H.; Perry, L.; Graham, N. Cervical Overview Group (COG). A Cochrane review of patient education for neck pain. Spine J. 2009, 9, 859–871. [Google Scholar] [CrossRef]
- Rickards, L.D. The effectiveness of non-invasive treatments for active myofascial trig-ger point pain: A systematic review of the literature. Int. J. Osteopath. Med. 2006, 9, 120–136. [Google Scholar] [CrossRef]
- Leaver, A.M.; Refshauge, K.M.; Maher, C.G.; McAuley, J.H. Conservative interventions provide short-term relief for non-specific neck pain: A systematic review. J. Physiother. 2010, 56, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Passos Nunes, A.M.; Azinheira Martins Moita, J.P. Effectiveness of physical and rehabilitation techniques in reducing pain in chronic trapezius myalgia: A systematic review and meta-analysis. Int. J. Osteopath. Med. 2015, 18, 189–206. [Google Scholar] [CrossRef]
- Kroeling, P.; Gross, A.R.; Goldsmith, C.H. Cervical Overview Group. A Cochrane review of electrotherapy for mechanical neck disorders. Spine 2005, 30, E641–E648. [Google Scholar] [CrossRef] [PubMed]
- Damgaard, P.; Bartels, E.M.; Ris, I.; Christensen, R.; Juul-Kristensen, B. Evidence of Physiotherapy Interventions for Patients with Chronic Neck Pain: A Systematic Review of Randomised Controlled Trials. ISRN Pain 2013, 2013, 567175. [Google Scholar] [CrossRef]
- Resende, L.; Merriwether, E.; Rampazo, É.P.; Dailey, D.; Embree, J.; Deberg, J.; Liebano, R.E.; Sluka, K.A. Meta-analysis of transcutaneous electrical nerve stimulation for relief of spinal pain. Eur. J. Pain 2018, 22, 663–678. [Google Scholar] [CrossRef]
- Gross, A.; Langevin, P.; Burnie, S.J.; Bédard-Brochu, M.S.; Empey, B.; Dugas, E.; Faber-Dobrescu, M.; Andres, C.; Graham, N.; Goldsmith, C.H.; et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst. Rev. 2015, 9, CD004249. [Google Scholar] [CrossRef] [PubMed]
- Kroeling, P.; Gross, A.; Graham, N.; Burnie, S.J.; Szeto, G.; Goldsmith, C.H.; Haines, T.; Forget, M. Electrotherapy for neck pain. Cochrane Database Syst. Rev. 2013, 8, CD004251. [Google Scholar]
- Martimbianco, A.L.C.; Porfírio, G.J.; Pacheco, R.L.; Torloni, M.R.; Riera, R. Transcutaneous electrical nerve stimulation (TENS) for chronic neck pain. Cochrane Database Syst. Rev. 2019, 12, CD011927. [Google Scholar] [CrossRef]
- Nordemar, R.; Thörner, C. Treatment of acute cervical pain-a comparative group study. Pain 1981, 10, 93–101. [Google Scholar] [CrossRef]
- Söderlund, A.; Lindberg, P. Cognitive behavioural components in physiotherapy management of chronic whiplash associated disorders (WAD)—A randomised group study. G Ital. Med. Lav. Ergon. 2007, 29 (Suppl. A), A5–A11. [Google Scholar] [CrossRef]
- Vitiello, A.L.; Bonello, R.; Pollard, H. The effectiveness of ENAR for the treatment of chronic neck pain in Australian adults: A preliminary single-blind, randomised controlled trial. Chiropr. Osteopat. 2007, 15, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardiç, F.; Sarhus, M.; Topuz, O. Comparison of two different techniques of electrotherapy on myofascial pain. J. Back Musculoskelet Rehabil. 2002, 16, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.T.; Hui-Chan, C.W.; Chein, G. A randomized clinical trial of TENS and exercise for patients with chronic neck pain. Clin. Rehabil. 2005, 19, 850–860. [Google Scholar] [CrossRef]
- Smania, N.; Corato, E.; Fiaschi, A.; Pietropoli, P.; Aglioti, S.M.; Tinazzi, M. Repetitive magnetic stimulation: A novel therapeutic approach for myofascial pain syndrome. J. Neurol. 2005, 252, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Sahin, N.; Albayrak, I.; Ugurlu, H. Effect of different transcutaneous electrical stimulation modalities on cervical myofascial pain syndrome. J. Musculoskelet Pain 2011, 19, 18–23. [Google Scholar] [CrossRef]
- Li, C.; Zhang, X.L.; Ding, H.; Tao, Y.Q.; Zhan, H.S. Comparative study on effects of manipulation treatment and transcutaneous electrical nerve stimulation on patients with cervi-cogenic headache. Zhong Xi Yi Jie He Xue Bao 2007, 5, 403–406. (In Chinese) [Google Scholar] [PubMed] [Green Version]
- Escortell-Mayor, E.; Riesgo-Fuertes, R.; Garrido-Elustondo, S.; Asúnsolo-Del Barco, A.; Díaz-Pulido, B.; Blanco-Díaz, M.; Bejerano-Álvarez, E. TEMA-TENS Group. Primary care randomized clinical trial: Manual therapy effectiveness in comparison with TENS in patients with neck pain. Man. Ther. 2011, 16, 66–73. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Cleland, J.A.; Huijbregts, P.; Palomeque-Del-Cerro, L.; González-Iglesias, J. Repeated Applications of Thoracic Spine Thrust Manipulation do not Lead to Tolerance in Patients Presenting with Acute Mechanical Neck Pain: A Secondary Analysis. J. Man. Manip. Ther. 2009, 17, 154–162. [Google Scholar] [CrossRef] [Green Version]
- González-Iglesias, J.; Fernández-de-las-Peñas, C.; Cleland, J.A.; Gutiérrez-Vega Mdel, R. Thoracic spine manipulation for the management of patients with neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2009, 39, 20–27. [Google Scholar] [CrossRef] [Green Version]
- González-Iglesias, J.; Fernández-de-las-Peñas, C.; Cleland, J.A.; Alburquerque-Sendín, F.; Palomeque-del-Cerro, L.; Méndez-Sánchez, R. Inclusion of thoracic spine thrust manipula-tion into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: A randomized clinical trial. Man. Ther. 2009, 14, 306–313. [Google Scholar] [CrossRef]
- Curatolo, M.; Petersen-Felix, S.; Arendt-Nielsen, L.; Giani, C.; Zbinden, A.M.; Radanov, B.P. Central hypersensitivity in chronic pain after whiplash injury. Clin. J. Pain. 2001, 17, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Haldeman, S.; Carroll, L.; Cassidy, J.D.; Schubert, J.; Nygren, Å. The Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Eur. Spine J. 2008, 17 (Suppl. 1), 5–7. [Google Scholar] [CrossRef]
- Guzman, J.; Hurwitz, E.L.; Carroll, L.J.; Haldeman, S.; Côté, P.; Carragee, E.J.; Peloso, P.M.; van der Velde, G.; Holm, L.W.; Hogg-Johnson, S.; et al. Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. A new conceptual model of neck pain: Linking onset, course, and care: The Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine 2008, 33 (Suppl. 4), S14–S23. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, S.M.; van Tulder, M. A best-evidence review of diagnostic procedures for neck and low-back pain. Best Pract. Res. Clin. Rheumatol. 2008, 22, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Carroll, L.J.; Hogg-Johnson, S.; van der Velde, G.; Haldeman, S.; Holm, L.W.; Carragee, E.J.; Hurwitz, E.L.; Côté, P.; Nordin, M.; Peloso, P.M.; et al. Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Course and prognostic factors for neck pain in the general population: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine 2008, 33 (Suppl. 4), S75–S82. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.A.; Costantini, R.; Affaitati, G.; Fabrizio, A.; Lapenna, D.; Tafuri, E.; Mezzetti, A. Viscero-visceral hyperalgesia: Characterization in different clinical models. Pain 2010, 151, 307–322. [Google Scholar] [CrossRef]
- Gelhorn, H.L.; Sexton, C.C.; Classi, P.M. Patient preferences for treatment of major depressive disorder and the impact on health outcomes: A systematic review. Prim. Care Companion CNS Disord. 2011, 13, PCC.11r01161. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year | Type | TENS Study | Evaluation | Results | Limits | AMSTAR Score |
|---|---|---|---|---|---|---|
| Vernon et al., 2005 [18] | SR | Nordemar et al., 1981 [29] | Amsterdam-Maastricht Consensus List | There is limited evidence of the efficacy of TENS in patients suffering from acute neck pain not associated with whiplash | The number of included studies and participants is low; no study achieves a high-quality score, only one study talks about TENS | 6/11 |
| Haines et al., 2009 [19] | SR | Soderlund et al., 2001 [30] | The Methodological Quality criteria Van Tulder et al. | There is no evidence of the superiority of educational strategies over TENS | Low methodological quality of the included studies; only one study talks about TENS | 8/11 |
| Leaver et al., 2010 [21] | SR | Vitiello et al., 2007 [31] | PEDro scale | There is sparse evidence regarding the various forms of TENS, with only one study in this review reporting insignificant results, in general few investigated interventions have shown better long-term effects than placebo | Only one study included in the review talks about TENS | 7/11 |
| Passos Nunes et al., 2015 [22] | SR and MA | Ardic et al., 2002 [32] | Score developed by Cochrane Back Review Group (CBRG) | There is very low-quality evidence that TENS is effective in chronic trapezius muscle pain. This review found no evidence of an effective treatment to reduce pain in the medium to long term | The quality of the evidence varies from low to very low in the short term; there is no evidence of the effectiveness of the treatment in the medium and long term; low methodological quality of the included studies; only one study talks about TENS | 8/11 |
| Damgaard et al., 2013 [24] | SR | Chiu et al., 2005 [33]; Smania et al., 2005 [34]; Soderlund et al., 2001 [30] | Cochrane Collaboration’s tool | TENS appears to be effective in chronic nonspecific neck pain, however there is insufficient evidence for the application of a specific physiotherapy intervention in a specific subgroup of patients | Many studies are characterized by a high risk of bias, in some of them the risk of bias is unclear; the various interventions are complex, multifaceted, and with various interventions; the various interventions have been administered to you in different ways and in different contexts | 7/11 |
| Resende et al., 2018 [25] | SR and MA | Sahin et al., 2011 [35] | Cochrane Collaborations tool | The effects of TENS in chronic neck pain are unclear | Low number of RCTs included low quality of RCTs included; heterogeneity of included studies; only one study speaks of TENS in chronic neck pain | 10/11 |
| Authors, Year | Type | Evaluation | Results | Limits | AMSTAR Score |
|---|---|---|---|---|---|
| Rickards, 2006 [20] | SR | Critical evaluation list of methodological quality (20 items) | TENS seems to have an immediate effect in reducing the intensity of myofascial pain in the neck and in the upper back area, however there is insufficient data to determine the effectiveness of TENS beyond the immediate post-treatment | Heterogeneity of included studies; small intervention and comparison groups; the strength of the evidence is limited in most cases | 6/11 |
| Kroeling et al., 2005 [23] | SR | Jadad et al.’s criteria | No definitive declarations can be issued regarding the efficacy of TENS in mechanical disorders of the cervical spine. Current evidence is lacking, limited, and conflicting | Lack of studies; low quality included studies; heterogeneity of subtypes of cervical disorders and of the methods used | 7/11 |
| Gross et al., 2015 [26] | SR | Cochrane handbook for systematic re-views of interventions criteria | In patients with chronic headache of cervicogenic origin, TENS appears to be less effective than cervical manipulation in reducing pain in the short term. In patients suffering from chronic and subacute neck pain, TENS appears to produce the same effects as cervical mobilization with regard to the improvement of pain, function, quality of life, and patient satisfaction up to an intermediate follow-up period | Many studios are small in size; lack of blinding of participants and therapists in most of the included studies; high risk of “detection bias”; there are no long-term follow-up studies | 10/11 |
| Kroeling et al., 2013 [27] | SR and MA | Criteria recommended by the Cochrane Collaboration and the Cochrane Back Review Group | It is not possible to issue definitive statements on the efficacy of TENS and its clinical use in cervical pain | Small size of the studios; heterogeneity of the populations analyzed, interventions and outcomes; 70% of the studies were not conducted properly | 10/11 |
| Martimbianco et al., 2019 [28] | SR | Cochrane criteria Handbook for Systematic Reviews of Interventions | This systematic review reported very low-quality evidence regarding the difference between TENS and sham TENS in pain relief. There is insufficient evidence regarding the use of TENS in people with chronic neck pain | Lack of data on the outcomes of interest; quality of the included studies limited by the lack of “blinding” and the lack of allocation concealment; estimated effects influenced by different degrees of “publication bias”; very low certainty of evidence for all outcomes analyzed within each comparison; heterogeneity of the analyzed outcomes; small number of participants in each study | 11/11 |
| Authors, Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Vernon et al., 2005 [18] | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✕ |
| Haines et al., 2009 [19] | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✕ |
| Rickards, 2006 [20] | ✓ | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✕ |
| Leaver et al., 2010 [21] | ✓ | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ | ✕ | ✓ | ✕ | ✓ |
| Passos Nunes et al., 2015 [22] | ✓ | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ |
| Kroeling et al., 2005 [23] | ✓ | ✓ | ✓ | ✕ | x | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ |
| Damgaard et al., 2013 [24] | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✕ | ✕ | ✕ | ✓ |
| Resende et al., 2018 [25] | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Gross et al., 2015 [26] | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Kroeling et al., 2013 [27] | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Martimbianco et al., 2019 [28] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Authors, Year | Frequency | Intensity | Pulse Duration | Session Duration | Sessions | Treatment Duration | Follow-Up |
|---|---|---|---|---|---|---|---|
| Vernon et al., 2005 [18] | / | / | / | / | 6 | 2 weeks | / |
| Haines et al., 2009 [19] | / | / | / | / | 12 | / | 3 months |
| Rickards, 2006 [20] | 100 Hz | / | 250 µs | / | / | / | Immediately in the post-treatment (3–5 min) |
| Leaver et al., 2010 [21] | 60–100 Hz | <10 mA | 50–100 µs | 15 min | 12 | 6 weeks | / |
| Passos Nunes et al., 2015 [22] | / | / | / | 20 min | 14 | 2 weeks | 3 months |
| Kroeling et al., 2005 [23] | 0.5–160 Hz | Modulable between “below the sensory threshold” (0.3 mA) and “just below the nociceptive threshold “ | / | 10–30 min | 1–15 | 1 day–3 months | 6 weeks–12 months |
| Damgaard et al., 2013 [24] | 80–100 Hz | Modulable from “below the local sensory threshold” to “antioxidant sensation” | 150–250 µs | 30 min. | 4–12 | 2–6 weeks | Post treatment–6 months |
| Resende et al., 2018 [25] | 2–100 Hz | Modulable from “low intensity” to “high intensity” | 40–250 µs | 15–60 min | 19 | 2–5 weeks | / |
| Gross et al., 2015 [26] | 10–100 Hz | / | 250 ns–<150 µs | 20–30 min | 5–10 | 3 weeks–1 month | Immediately in the post-treatment–6 months |
| Kroeling et al., 2013 [27] | 4–143 Hz | Modulable from “low intensity” to “high intensity” | 40 µs–150 ms | 14–30 min | 1–12 | 1 gg–6 months | 6 weeks–6 months |
| Martimbianco et al., 2019 [28] | 2–100 Hz | <70 mA | 50–250 µs | 15–60 min | 1–60 | 1 gg–6 weeks | 1 week–6 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paolucci, T.; Agostini, F.; Paoloni, M.; de Sire, A.; Verna, S.; Pesce, M.; Ribecco, L.; Mangone, M.; Bernetti, A.; Saggini, R. Efficacy of TENS in Cervical Pain Syndromes: An Umbrella Review of Systematic Reviews. Appl. Sci. 2021, 11, 3423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083423
Paolucci T, Agostini F, Paoloni M, de Sire A, Verna S, Pesce M, Ribecco L, Mangone M, Bernetti A, Saggini R. Efficacy of TENS in Cervical Pain Syndromes: An Umbrella Review of Systematic Reviews. Applied Sciences. 2021; 11(8):3423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083423
Chicago/Turabian StylePaolucci, Teresa, Francesco Agostini, Marco Paoloni, Alessandro de Sire, Simone Verna, Mirko Pesce, Luca Ribecco, Massimiliano Mangone, Andrea Bernetti, and Raoul Saggini. 2021. "Efficacy of TENS in Cervical Pain Syndromes: An Umbrella Review of Systematic Reviews" Applied Sciences 11, no. 8: 3423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083423