
Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review

 , , , , , and
, , , , , and
Abstract
:1. Introduction
- Paresthesia—An abnormal sensation, whether spontaneous or evoked.
- Anesthesia—Complete absence of perception of stimuli including touch.
- Dysesthesia—An unpleasant abnormal sensation, whether spontaneous or evoked.
- Hyperalgesia—Increased pain from a stimulus that normally provokes pain.
- Allodynia—Pain due to a stimulus that does not normally provoke pain.
- Hypoesthesia—Decreased sensitivity to stimulation, excluding the special senses.
- Hyperesthesia—Increased sensitivity to stimulation, excluding the special senses.
- The injury to the lingual nerve may also affect taste perception on the same side.
- Ageusia—Loss of taste perception.
- Dysgeusia—Altered taste perception.
2. Materials and Methods
2.1. PICO Question
- Population (P): Patients suffering nerve injuries at the inferior alveolar/facial nerve after oral surgery procedures.
- Interventions (I): Microsurgical nerve regeneration approach with type I collagen devices.
- Comparison (C): Nihil.
- Outcomes (O): Nerve injuries regeneration assessed with patient’s self-reported scale and/or standardized scales.
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria for Study Selection
2.4. Inclusion Criteria for Study Selection
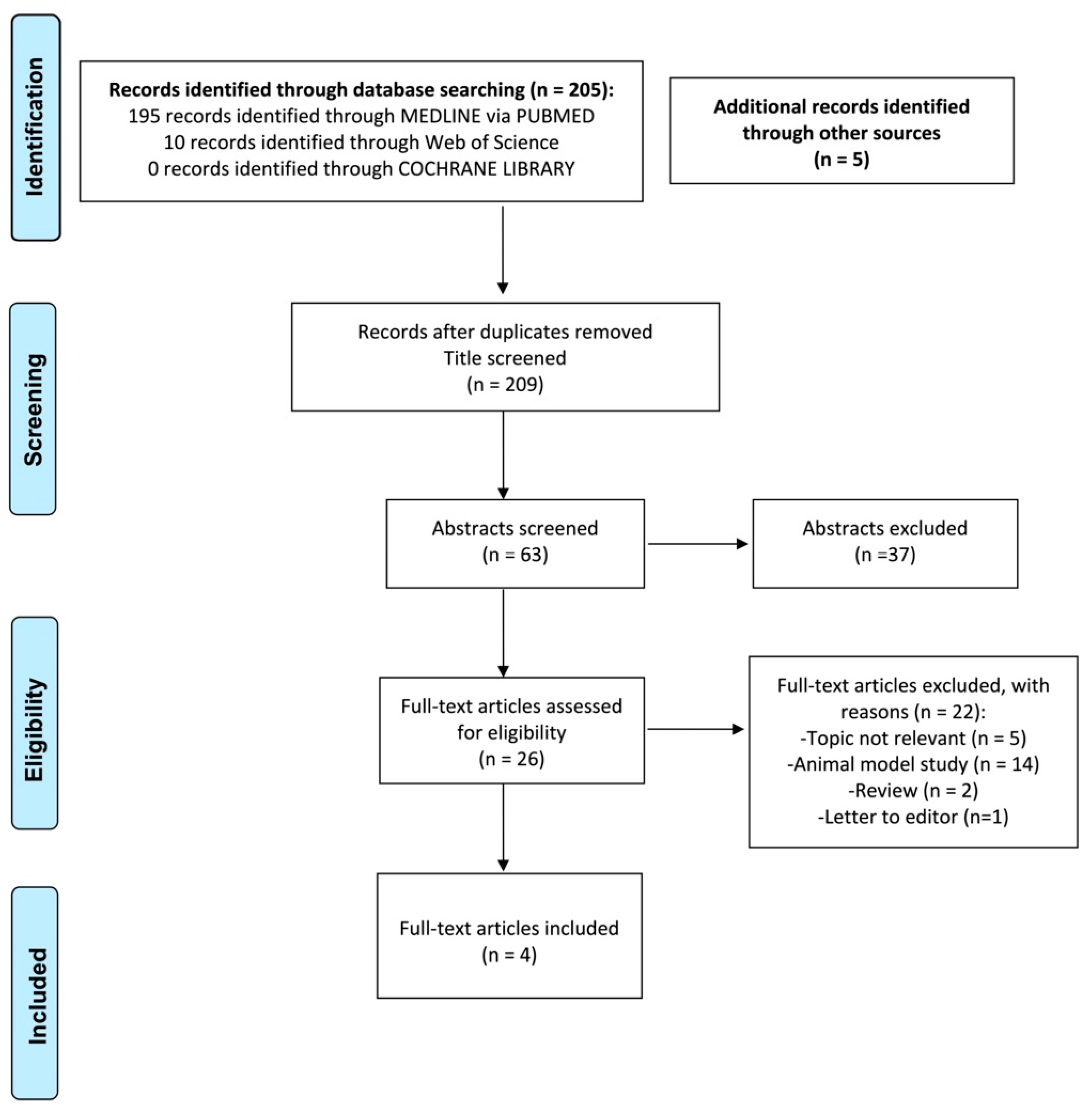
2.5. Study Selection
2.6. Data Extraction Process
2.7. Quality Assessment of the Level of Evidence
2.8. Data Synthesis
3. Results
3.1. Study Design, Patients’ Characteristics, Cause and Location of Nerve Injury
3.2. Time Interval between Injury and Repair and Type I Collagen Membrane Characteristics
3.3. Nerve Recovering Outcomes and Overall Assessment of the Quality of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kipp, D.P.; Goldstein, B.H.; Weiss, W.W., Jr. Dysesthesia after mandibular third molar surgery: A retrospective study and analysis of 1,377 surgical procedures. J. Am. Dent. Assoc. 1980, 100, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Glera-Suárez, P.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Patient morbidity after impacted third molar extraction with different flap designs. A systematic review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e233–e239. [Google Scholar] [CrossRef]
- Cheung, L.K.; Leung, Y.Y.; Chow, L.K.; Wong, M.C.; Chan, E.K.; Fok, Y.H. Incidence of neurosensory deficits and recovery after lower third molar surgery: A prospective clinical study of 4338 cases. Int. J. Oral Maxillofac. Surg. 2010, 39, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Sukegawa, S.; Yokota, K.; Kanno, T.; Manabe, Y.; Sukegawa-Takahashi, Y.; Masui, M.; Furuki, Y. What are the risk factors for postoperative infections of third molar extraction surgery: A retrospective clinical study? Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e123–e129. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.S.; Benton, J.A.; Yates, J.M. Risk of inferior alveolar nerve injury with coronectomy vs surgical extraction of mandibular third molars-A comparison of two techniques and review of the literature. J. Oral Rehabil. 2018, 45, 250–257. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Nhembe, F.; Gudka, D.; Shah, P.; Abbas, S.; McCarthy, E.; Patel, S.; Mahil, J.; Hopper, C. Experience in third molar surgery: An update. Br. Dent. J. 2010, 209, E1. [Google Scholar] [CrossRef] [PubMed]
- Queral-Godoy, E.; Figueiredo, R.; Valmaseda-Castellón, E.; Berini-Aytés, L.; Gay-Escoda, C. Frequency and evolution of lingual nerve lesions following lower third molar extraction. J. Oral Maxillofac. Surg. 2006, 64, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Deppe, H.; Mücke, T.; Wagenpfeil, S.; Kesting, M.; Linsenmeyer, E.; Tölle, T. Trigeminal nerve injuries after mandibular oral surgery in a university outpatient setting--a retrospective analysis of 1,559 cases. Clin. Oral Investig. 2015, 19, 149–157. [Google Scholar] [CrossRef]
- Coulthard, P.; Bailey, E.; Esposito, M.; Furness, S.; Renton, T.F.; Worthington, H.V. Surgical techniques for the removal of mandibular wisdom teeth. Cochrane Database Syst. Rev. 2014, 7, CD004345. [Google Scholar] [CrossRef] [Green Version]
- Kushnerev, E.; Yates, J.M. Evidence-based outcomes following inferior alveolar and lingual nerve injury and repair: A systematic review. J. Oral Rehabil. 2015, 42, 786–802. [Google Scholar] [CrossRef]
- Jones, R.H. Microsurgical repair of nerves injured during third molar surgery. Aust. Dent. J. 1992, 37, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Rath, E.M. Skeletal muscle autograft for repair of the human inferior alveolar nerve: A case report. J. Oral Maxillofac. Surg. 2002, 60, 330–334. [Google Scholar] [CrossRef] [PubMed]
- American Association of Oral and Maxillofacial Surgeons. Parameters and pathways: Clinical practice guidelines for oral and maxillofacial surgery (AAOMS ParPath 01), version 3.0. J. Oral Maxillofac. Surg. 2001, 59 (Suppl. S1). [Google Scholar]
- Pogrel, M.A.; Maghen, A. The use of autogenous vein grafts for inferior alveolar and lingual nerve reconstruction. J. Oral. Maxillofac. Surg. 2001, 59, 985–988. [Google Scholar] [CrossRef] [PubMed]
- Crawley, W.A.; Dellon, A.L. Inferior alveolar nerve reconstruction with a polyglycolic acid bioabsorbable nerve conduit. Plast. Reconstr. Surg. 1992, 90, 300–302. [Google Scholar] [CrossRef]
- Pitta, M.C.; Wolford, L.M.; Mehra, P.; Hopkin, J. Use of Gore-Tex tubing as a conduit for inferior alveolar and lingual nerve repair: Experience with 6 cases. J. Oral Maxillofac. Surg. 2001, 59, 493–497. [Google Scholar] [CrossRef]
- Seo, K.; Inada, Y.; Terumitsu, M.; Nakamura, T.; Horiuchi, K.; Inada, I.; Someya, G. One year outcome of damaged lingual nerve repair using a PGA-collagen tube: A case report. J. Oral Maxillofac. Surg. 2008, 66, 1481–1484. [Google Scholar] [CrossRef]
- Kehoe, S.; Zhang, X.F.; Boyd, D. FDA approved guidance conduits and wraps for peripheral nerve injury: A review of materials and efficacy. Injury 2012, 43, 553–572. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Farole, A.; Jamal, B.T. A bioabsorbable collagen nerve cuff (NeuraGen) for repair of lingual and inferior alveolar nerve injuries: A case series. J. Oral Maxillofac. Surg. 2008, 66, 2058–2062. [Google Scholar] [CrossRef]
- Bagheri, S.C.; Meyer, R.A.; Khan, H.A.; Kuhmichel, A.; Steed, M.B. Retrospective review of microsurgical repair of 222 lingual nerve injuries. J. Oral Maxillofac. Surg. 2010, 68, 715–723. [Google Scholar] [CrossRef]
- Erakat, M.S.; Chuang, S.K.; Shanti, R.M.; Ziccardi, V.B. Interval between injury and lingual nerve repair as a prognostic factor for success using type I collagen conduit. J. Oral Maxillofac. Surg. 2013, 71, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.T.; Chuang, S.K.; Ziccardi, V.B. Lingual Nerve Microsurgery Outcomes Using 2 Different Conduits: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2017, 75, 609–615. [Google Scholar] [CrossRef]
- Susarla, S.M.; Kaban, L.B.; Donoff, R.B.; Dodson, T.B. Does early repair of lingual nerve injuries improve functional sensory recovery? J. Oral Maxillofac. Surg. 2007, 65, 1070–1076. [Google Scholar] [CrossRef]
- Rutner, T.W.; Ziccardi, V.B.; Janal, M.N. Long-term outcome assessment for lingual nerve microsurgery. J. Oral Maxillofac. Surg. 2005, 63, 1145–1149. [Google Scholar] [CrossRef]
- Lam, N.P.; Donoff, R.B.; Kaban, L.B.; Dodson, T.B. Patient satisfaction after trigeminal nerve repair. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 538–543. [Google Scholar] [CrossRef]
- Gregg, J.M. Studies of traumatic neuralgia in the maxillofacial region: Symptom complexes and response to microsurgery. J. Oral Maxillofac. Surg. 1990, 48, 135–141. [Google Scholar] [CrossRef]
- Ichihara, S.; Inada, Y.; Nakamura, T. Artificial nerve tubes and their application for repair of peripheral nerve injury: An update of current concepts. Injury 2008, 39 (Suppl. S4), 29–39. [Google Scholar] [CrossRef] [PubMed]
- Ashley, W.W., Jr.; Weatherly, T.; Park, T.S. Collagen nerve guides for surgical repair of brachial plexus birth injury. J. Neurosurg. 2006, 105 (Suppl. S6), 452–456. [Google Scholar] [CrossRef]
- Lundborg, G.; Dahlin, L.B.; Danielsen, N. Ulnar nerve repair by the silicone chamber technique. Case report. Scand. J. Plast. Reconstr. Surg. Hand. Surg. 1991, 25, 79–82. [Google Scholar] [CrossRef]
- Chen, Y.S.; Hsieh, C.L.; Tsai, C.C.; Chen, T.H.; Cheng, W.C.; Hu, C.L.; Yao, C.H. Peripheral nerve regeneration using silicone rubber chambers filled with collagen, laminin and fibronectin. Biomaterials 2000, 21, 1541–1547. [Google Scholar] [CrossRef]
- Konofaos, P.; Ver Halen, J.P. Nerve repair by means of tubulization: Past, present, future. J. Reconstr. Microsurg. 2013, 29, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Shin, R.H.; Friedrich, P.F.; Crum, B.A.; Bishop, A.T.; Shin, A.Y. Treatment of a segmental nerve defect in the rat with use of bioabsorbable synthetic nerve conduits: A comparison of commercially available conduits. J. Bone Joint Surg. Am. 2009, 91, 2194–2204. [Google Scholar] [CrossRef]
- Thomsen, L.; Bellemere, P.; Loubersac, T.; Gaisne, E.; Poirier, P.; Chaise, F. Treatment by collagen conduit of painful post-traumatic neuromas of the sensitive digital nerve: A retrospective study of 10 cases. Chir. Main. 2010, 29, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Wangensteen, K.J.; Kalliainen, L.K. Collagen tube conduits in peripheral nerve repair: A retrospective analysis. Hand 2010, 5, 273–277. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Parisi, T.J.; Friedrich, P.F.; Bishop, A.T.; Shin, A.Y. Does the addition of a nerve wrap to a motor nerve repair affect motor outcomes? Microsurgery 2014, 34, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Rbia, N.; Bulstra, L.F.; Saffari, T.M.; Hovius, S.; Shin, A.Y. Collagen Nerve Conduits and Processed Nerve Allografts for the Reconstruction of Digital Nerve Gaps: A Single-Institution Case Series and Review of the Literature. World Neurosurg. 2019, 127, e1176–e1184. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| (“molar, third”[MeSH Terms]) and (“mandibular nerve”[MeSH Terms] or “lingual nerve”[MeSH Terms]) and (“mandibular nerve injuries”[All Fields]) and (“trigeminal nerve”[MeSH Terms]) or (“lingual nerve Injuries”[All Fields]) or (“trigeminal nerve injuries”[MeSH Terms]) and (“nerve regeneration”[MeSH Terms]) or (“nerve”[All Fields] and (“regeneration”[All Fields]) or “nerve regeneration”[All Fields]) and (“collagen”[MeSH Terms]) and (“Humans”[MeSH Terms]) |
| ((“molar, third”[MeSH Terms]) and (“mandibular nerve”[MeSH Terms] or “lingual nerve”[MeSH Terms]) and (“mandibular nerve injuries”[All Fields]) and (“trigeminal nerve”[MeSH Terms]) or (“lingual nerve Injuries”[All Fields]) or (“trigeminal nerve injuries”[MeSH Terms]) and (“nerve regeneration”[MeSH Terms]) or (“nerve”[All Fields] and (“regeneration”[All Fields]) or “nerve regeneration”[All Fields]) and (“collagen”[MeSH Terms]) and (“Humans”[MeSH Terms])) |
| (molar, third) and (mandibular nerve or lingual nerve) and (mandibular nerve injuries) and (trigeminal nerve or lingual nerve Injuries or trigeminal nerve injuries) and (nerve regeneration or nerve regeneration or nerve regeneration) and (collagen) and (Humans) |
| Inclusion Criteria |
|---|
|
Exclusion Criteria |
|
| Author/Year | Type of Study | Patients (n) | Surgical Procedure | Nerve Injury Site | Nerve Disturbances | Collagen Conduit | Therapy | Time interval between Injury and Repair | Follow-up | Outcome | Recovering Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Farole A. 2008 [19] | Case series | 8 | 3rd molar extractions | 3 IAN 6 LN | 3 les. dysesthesia absent 3. les dysesthesia | Collagen type I conduit (NeuraGen Integra LifeSciences, Plainsboro, NJ, USA), | External neurolysis, primary neurorrhaphy, and excision of neuroma (if present), | 3 to 7 months | 4 pat. at least 12 montths. 4 pat. 30 months. | 4 les. Good improvement 4 les. Some recovering 1 les. No improvement | Pogrel classification |
| Bagheri et al. 2010 [20] | Retrospective study | 8 | 3rd molar extraction (NCM) | 8 LN | Numbness, Numbness with pain, Pain (NCM) | Collagen cuff (Neuroflex; Collagen Matrix, Franklin Lakes, NJ, USA) | External decompression and neurolysis | 6 months to 12 months | At least 12 months | Complete return of sensation (90.5%)/no or inadequate improvement (9.5%) (NCM) | MRC scale |
| Erakat et al. 2013 [21] | Retrospective cohort study | 21 | 3rd molar extraction | 22 LN | complete hypoesthesia | Collagen type I conduit (NeuraGen Integra LifeSciences, Plainsboro, NJ, USA), | External neurolysis 4 External/internal neurolysis 8 Microrepair 10 | 3 to 9 months | 12 months | Return to successful functional sensory recover in 100% of cases | MRC scale |
| Wilson et al. 2016 [22] | Retrospective cohort study | 28 | 3rd molar extraction. | 28 LN | 10 neurotmesis 8 axonotmesis | Collagen type I conduit NeuraGen Integra LifeSciences, Plainsboro, NJ, USA), | External or internal neurolysis, neuroma excision and direct primary neurorrhaphy. | 2 to 36 months | 3 to 18 months | Mean functional sensory recover of S3+.grade in the MRC scale (Superficial pain and touch without Hyperesthesia/ good stimulus localization; static discrimination of 7–15 mm | Testing responses to hot, cold, wisp, Brush, pinprick/testing 2-point discrimination and fine touch with von Frey fibers and MRC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roccuzzo, A.; Molinero-Mourelle, P.; Ferrillo, M.; Cobo-Vázquez, C.; Sanchez-Labrador, L.; Ammendolia, A.; Migliario, M.; de Sire, A. Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review. Appl. Sci. 2021, 11, 3927. https://0-doi-org.brum.beds.ac.uk/10.3390/app11093927
Roccuzzo A, Molinero-Mourelle P, Ferrillo M, Cobo-Vázquez C, Sanchez-Labrador L, Ammendolia A, Migliario M, de Sire A. Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review. Applied Sciences. 2021; 11(9):3927. https://0-doi-org.brum.beds.ac.uk/10.3390/app11093927
Chicago/Turabian StyleRoccuzzo, Andrea, Pedro Molinero-Mourelle, Martina Ferrillo, Carlos Cobo-Vázquez, Luis Sanchez-Labrador, Antonio Ammendolia, Mario Migliario, and Alessandro de Sire. 2021. "Type I Collagen-Based Devices to Treat Nerve Injuries after Oral Surgery Procedures. A Systematic Review" Applied Sciences 11, no. 9: 3927. https://0-doi-org.brum.beds.ac.uk/10.3390/app11093927