
Flabby Ridge, a Challenge for Making Complete Dentures

 , and
, and 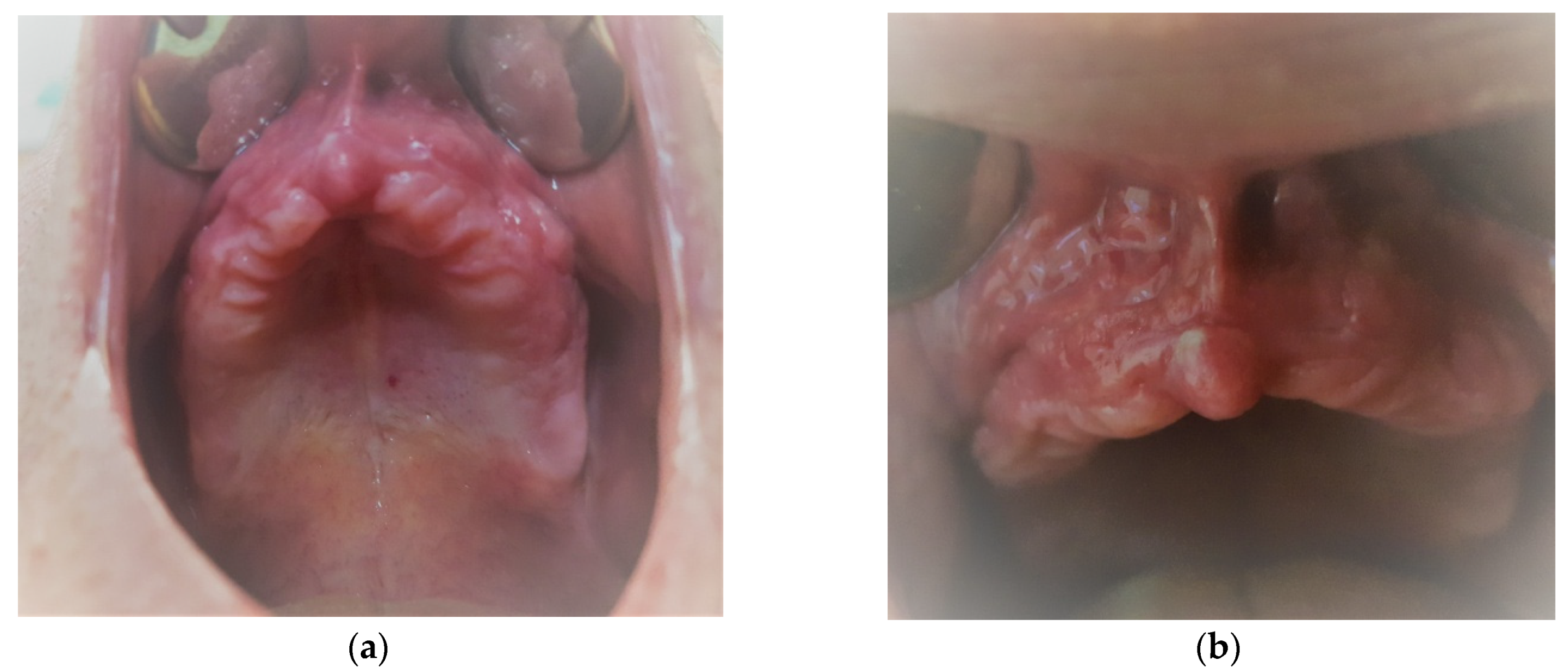{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- upper frontal edentulous ridge(very often)
- upper fronto-lateral edentulous ridge(often)
- maxillary tuberosity(rare)
- lower frontal edentulous ridge(very often)
- lower fronto-lateral edentulous ridge(rare)
- retromolar pad(often)
- Depending on the structure:
- hyperplasic, keratinized, with high antero-posterior and supero-inferior thickness
- atrophic, thin, small antero-posterior thickness and increased supero-inferior length
- apparently histological normal appearance at inspection, but with increased mobility in all directions.
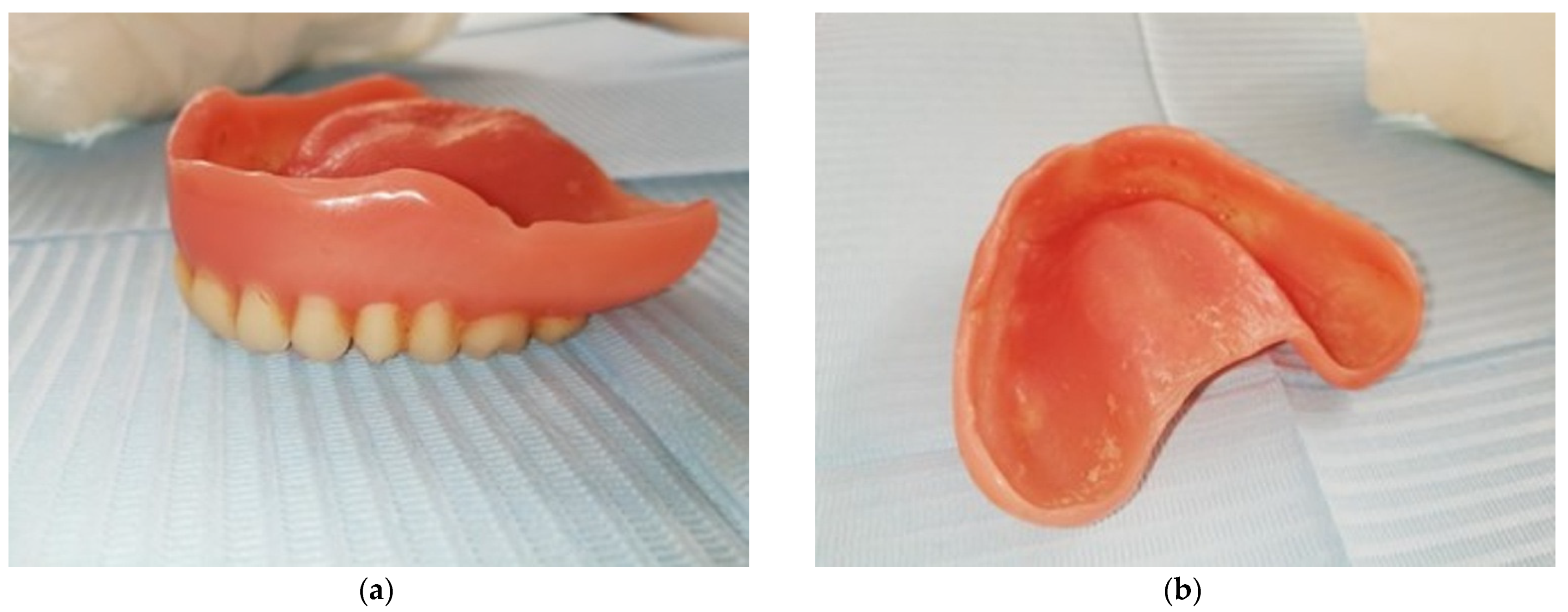
3. Results
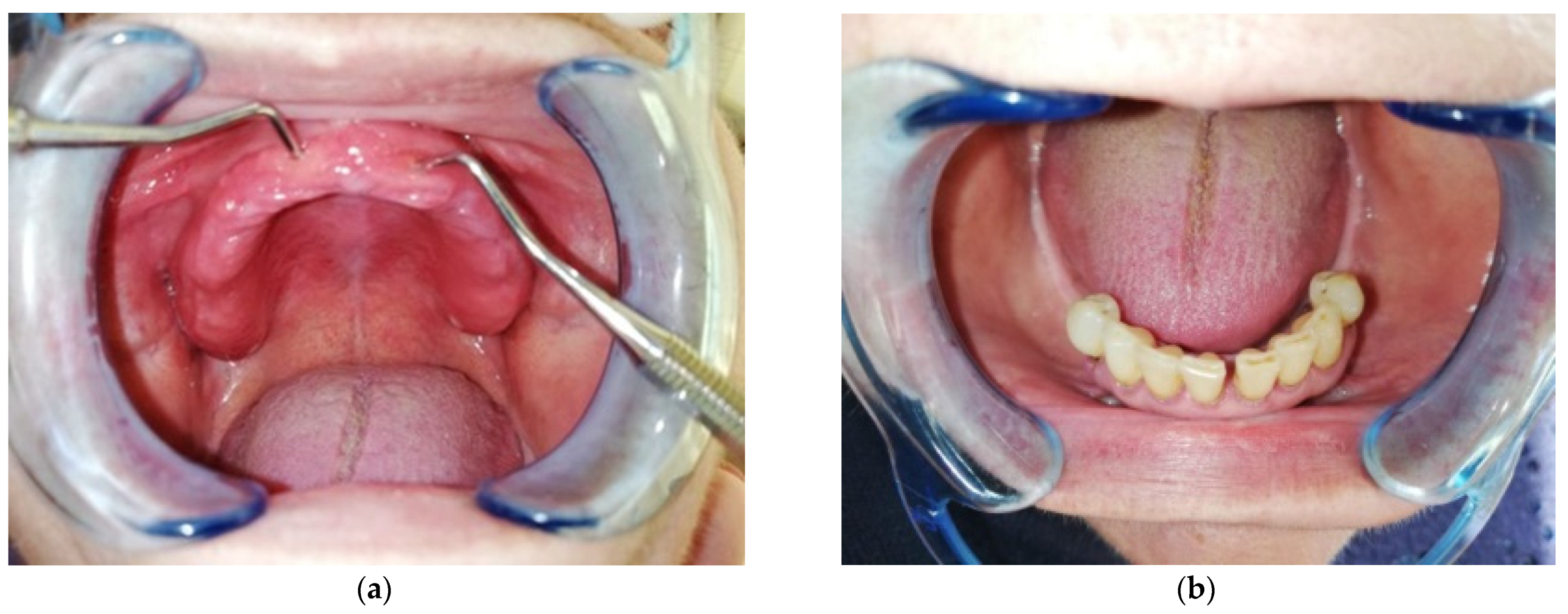
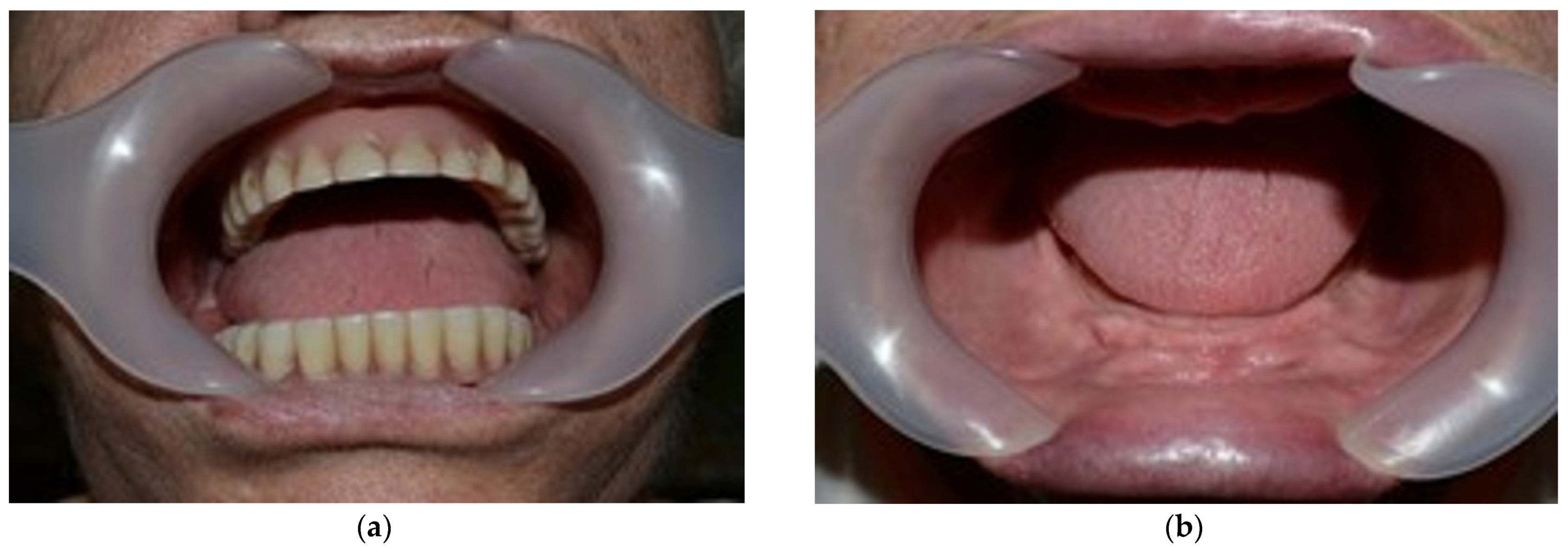
3.1. CASE REPORT 1
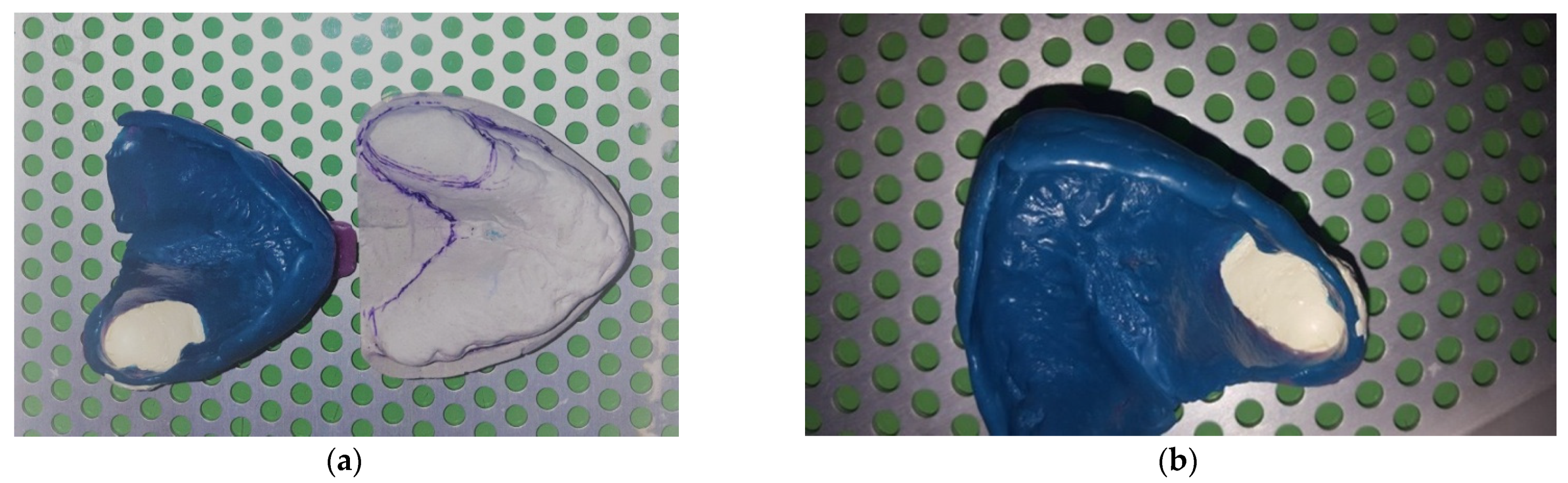
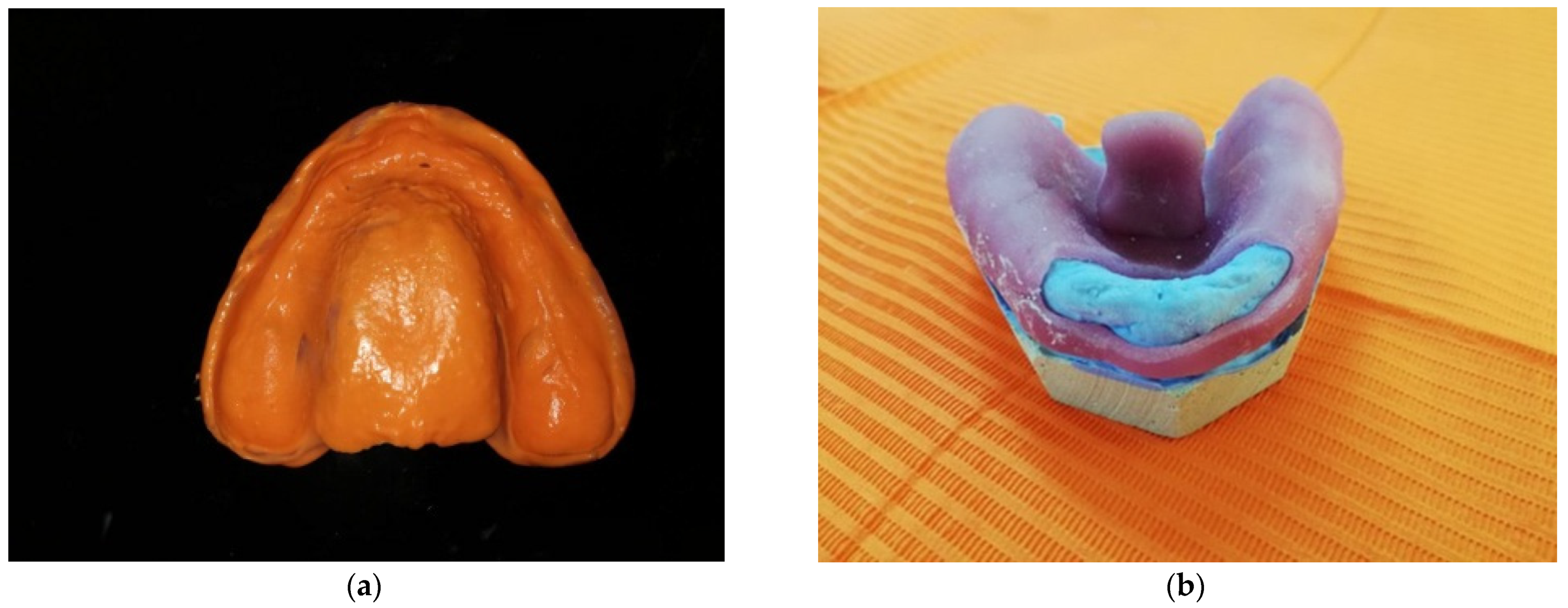
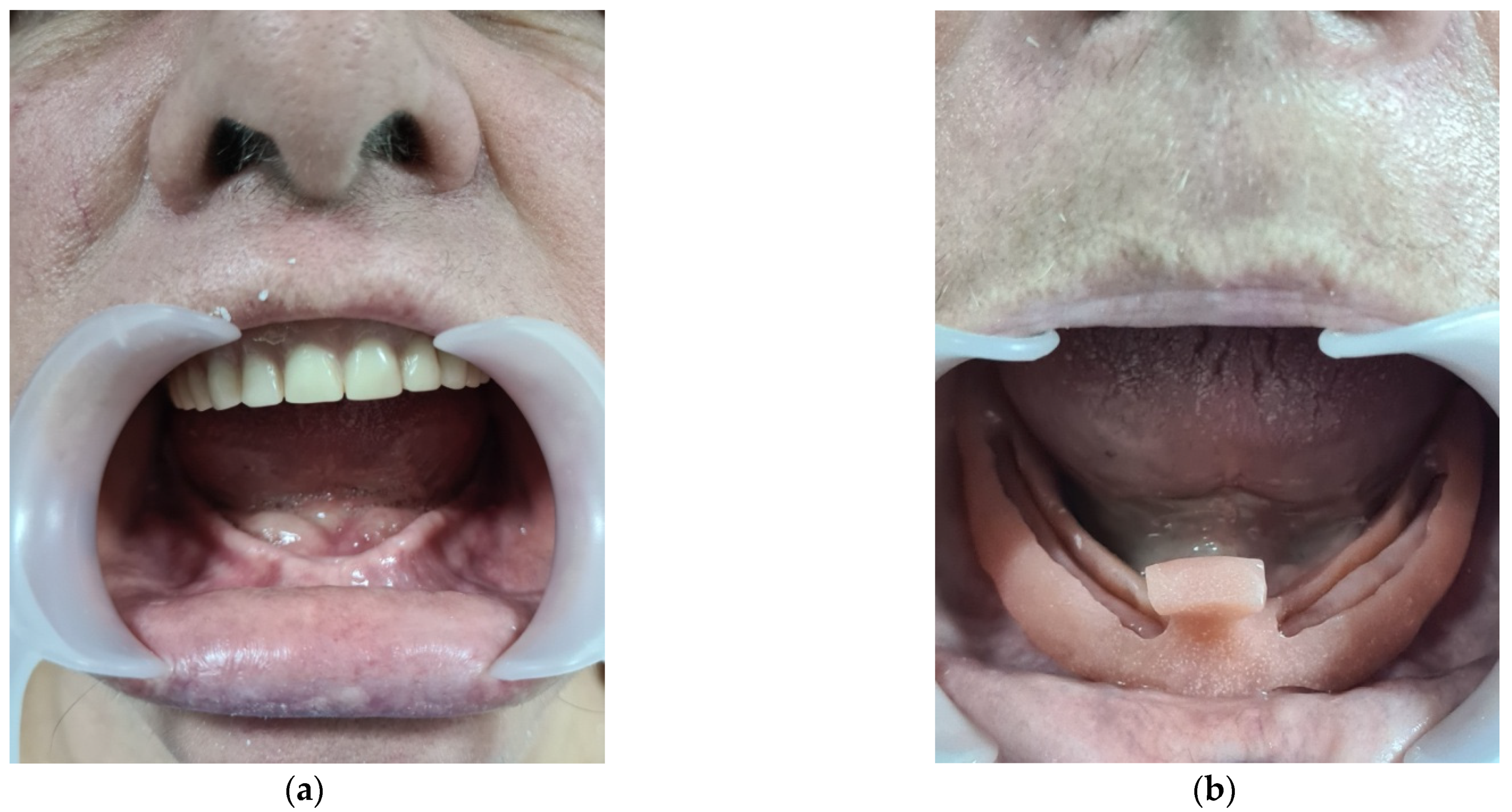
3.2. CASE REPORT 2
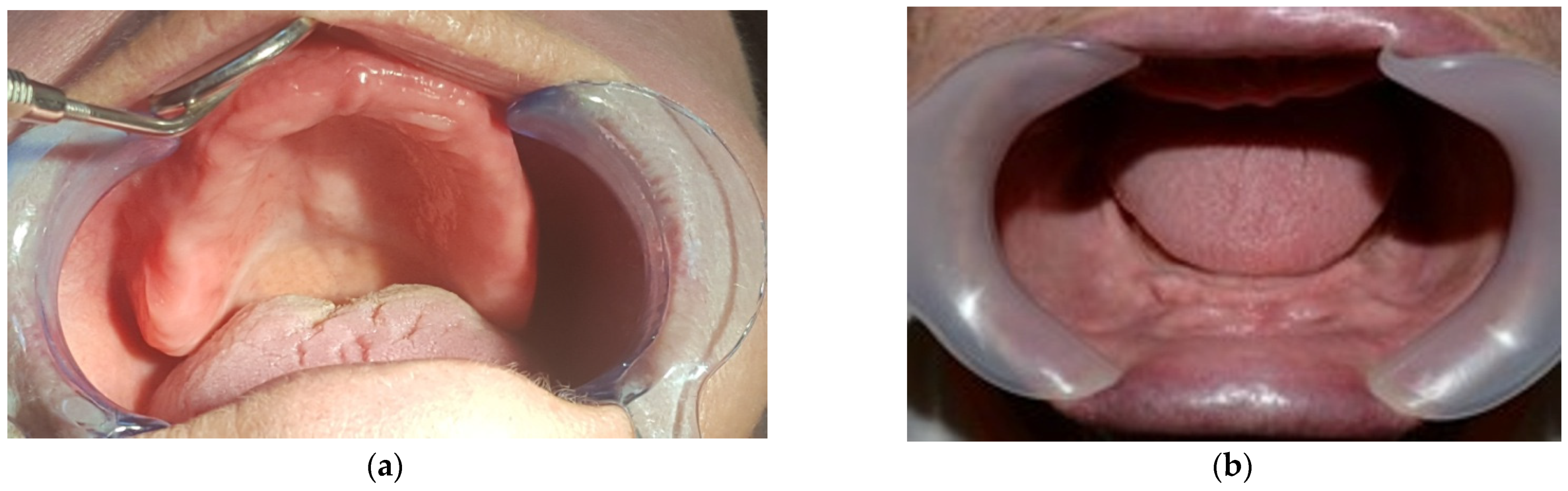
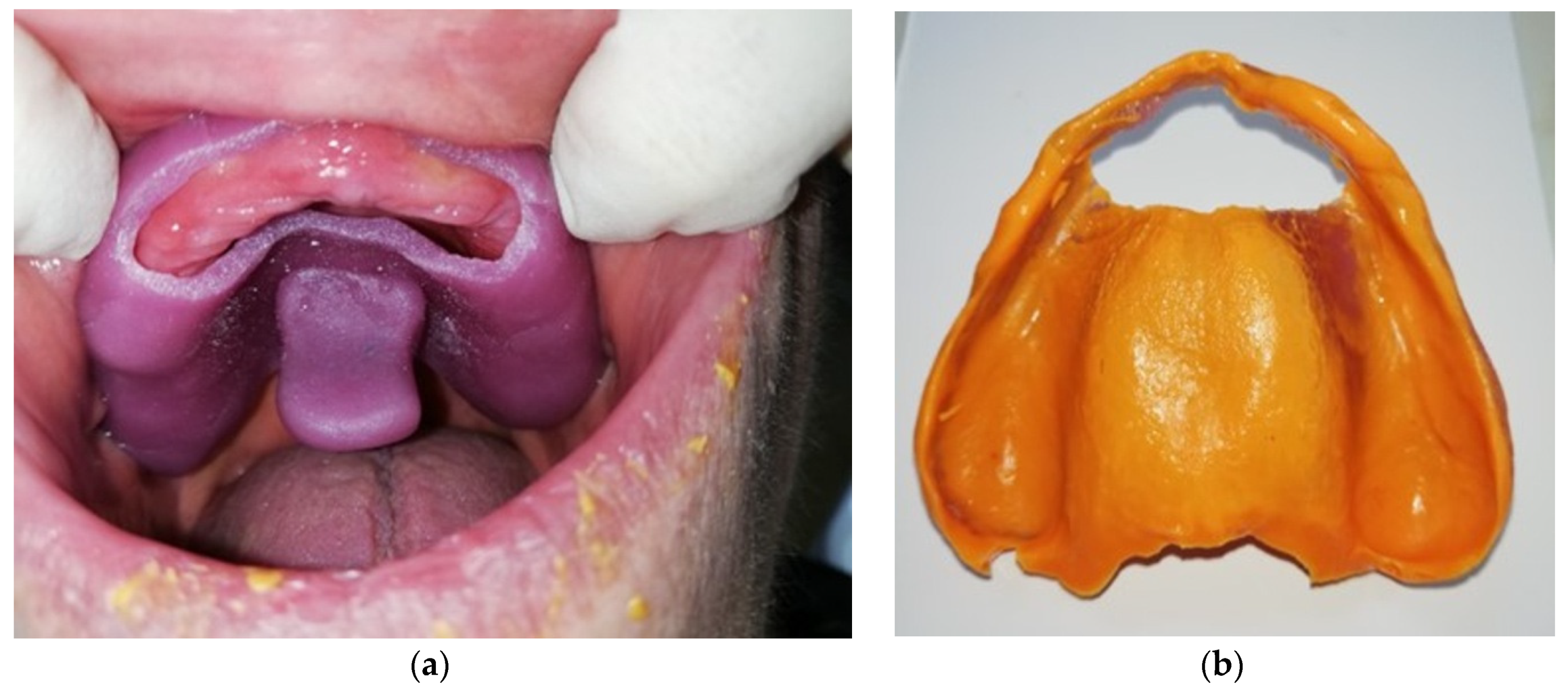
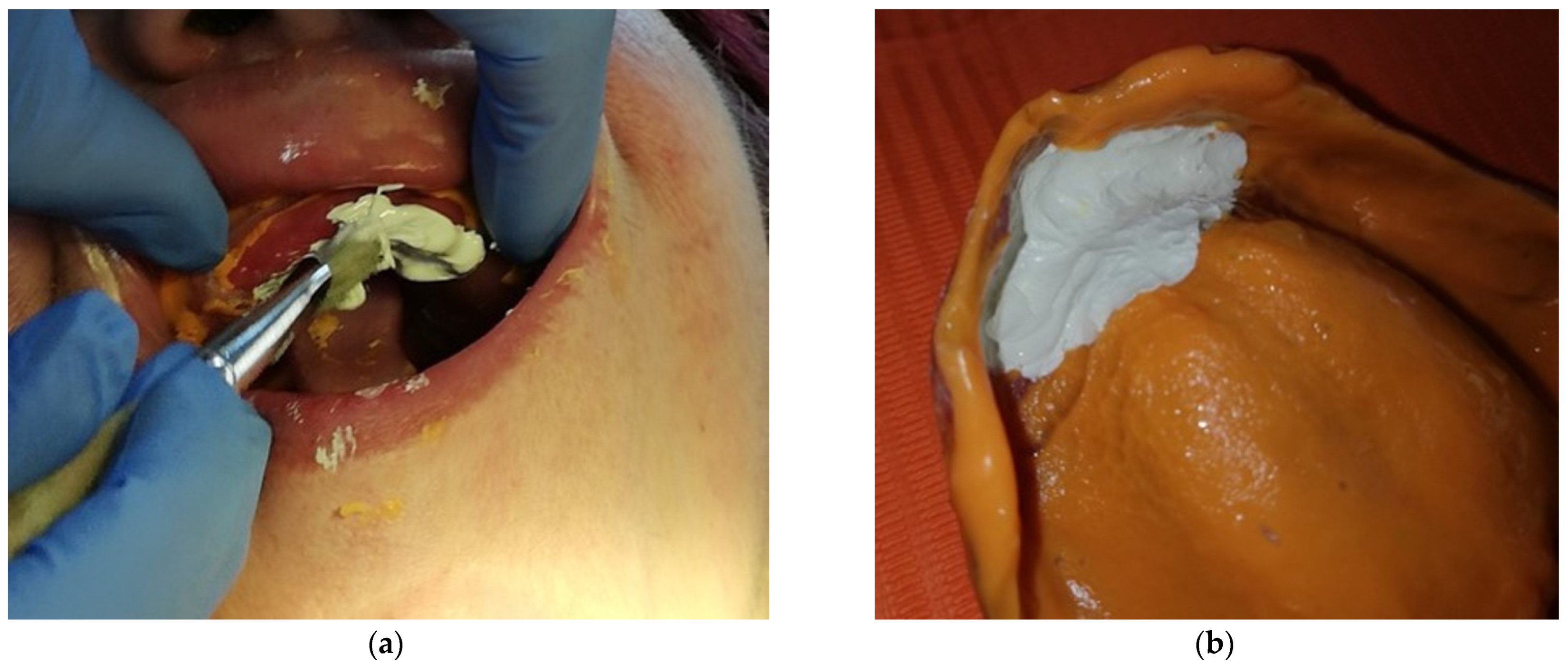
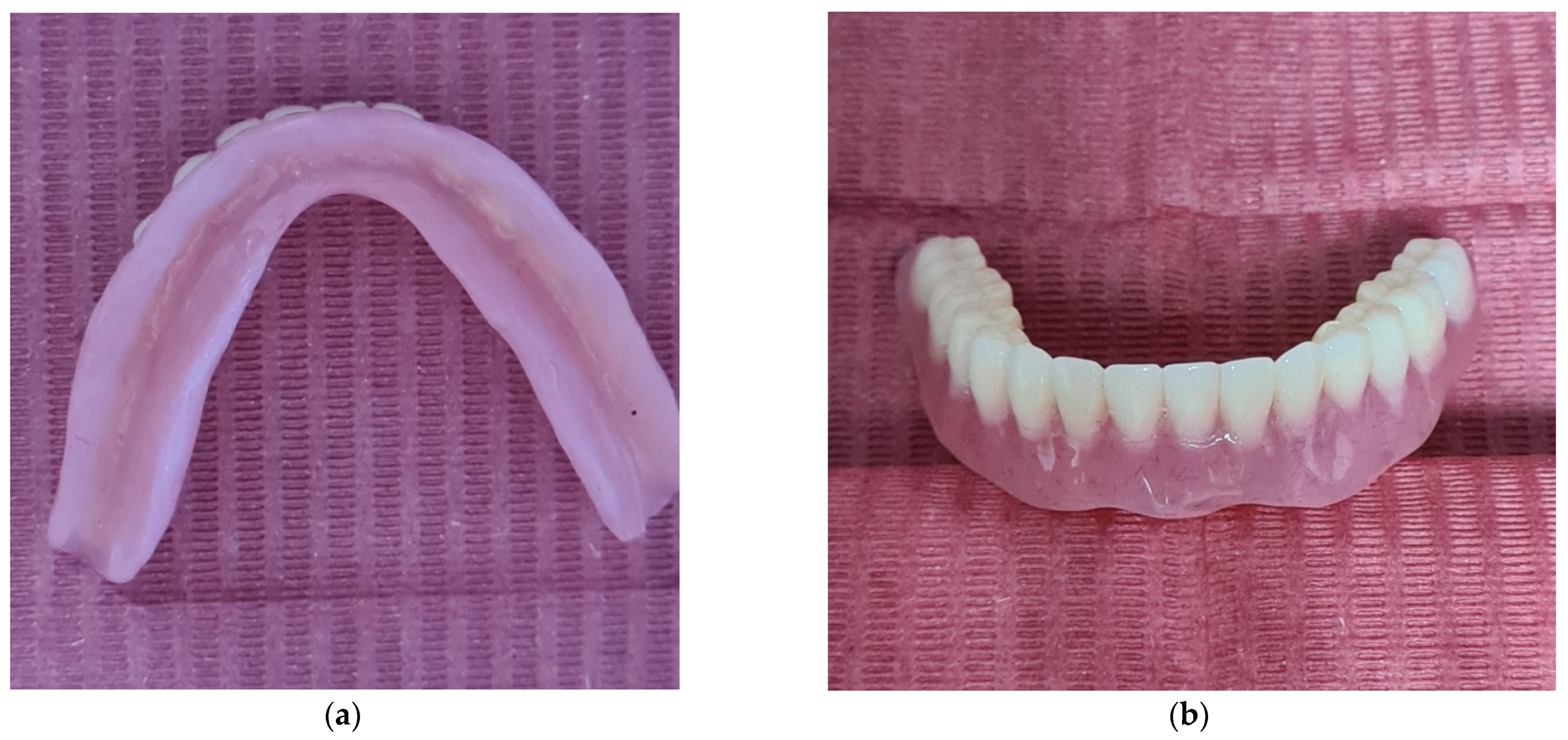
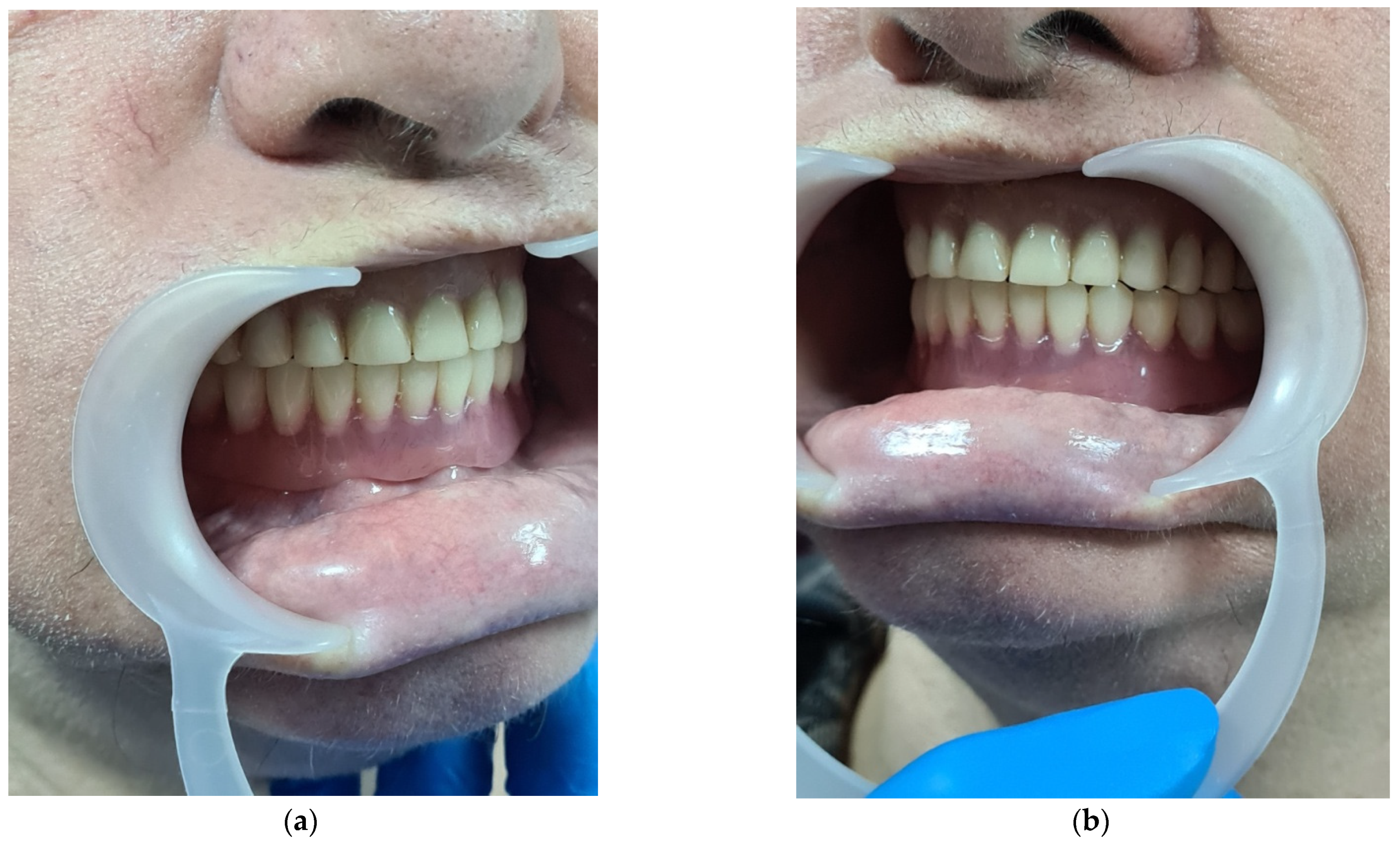
3.3. CASE REPORT 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, E. Changes caused by a mandibular removable partial denture opposing a maxillary complete denture. J. Prosthet. Dent. 1972, 27, 140–150. [Google Scholar] [CrossRef]
- Cristalli, M.P.; La Monaca, G.; Pranno, N.; Annibali, S.; Iezzi, G.; Vozza, I. Xeno-Hybrid Composite Scaffold Manufactured with CAD/CAM Technology for Horizontal Bone-Augmentation in Edentulous Atrophic Maxilla: A Short Communication. Appl. Sci. 2020, 10, 2659. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, P.; Kulkarni, R.S.; Shah, R.J.; Tomar, B. Mishmash impression technique for managing maxillary anterior fibrous ridge. J. Dent. Mater. Tech. 2018, 7, 63–68. [Google Scholar]
- Balwani, T.; Dubey, S.G.; Pande, S. Prosthodontic management of maxillary fabby ridge and the resorbed mandibular ridge. J. Datta Meghe Inst. Med. Sci. Univ. 2020, 15, 323–326. [Google Scholar] [CrossRef]
- Bindhoo, Y.A.; Trimurthy, V.R.; Anjana, K. Complete mucostatic impression: A new attempt. J. Prosthodont. 2012, 21, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Finbarr, A. Management of flabby ridge in complete denture construction. Dent. Update 2005, 32, 524–528. [Google Scholar]
- Benaiffer, A.; Surendra, A.; Anup, M. Management of flabby ridge: A case report. Ind. J. Dent. Sci. 2011, 3, 20–22. [Google Scholar]
- Liddelow, K.P. The prosthetic treatment of the elderly. Br. Dent. J. 1964, 117, 307–315. [Google Scholar]
- Osborne, J. Two impression methods for mobile fibrous ridges. Br. Dent. J. 1964, 117, 392–394. [Google Scholar]
- Watson, R.M. Impression technique for maxillary fibrous ridge. Br. Dent. J. 1970, 128, 552. [Google Scholar] [CrossRef]
- Arbree, N.S.; Fleck, S.; Askinas, S.W. The results of a brief survey of complete denture prosthodontic techniques in predoctoral programs in North American Dental Schools. J. Prosthodont. 1996, 5, 219–225. [Google Scholar] [CrossRef]
- Burton, M. Current trends in removable prosthodontics. J. Am. Dent. Assoc. 2000, 131, 52–56. [Google Scholar]
- Shum, M.H.C.; Pow, E.H.N. Management of excessive movable tissue: A modified impression technique. J. Prosthet. Dent. 2014, 112, 387–389. [Google Scholar] [CrossRef]
- Singh, D.K.; Dable, R.; Tandon, P.; Jain, A. Prosthodontics rehabilitation a maxillary fibrous ridge—A case report. TMU J. Dent. 2014, 4, 164–167. [Google Scholar]
- Muthukumar, B.; Deepak, K.; Ahila, S.C. Modified impression technique for a flabby maxilla—A clinical report. Univ. J. Dent. Sci. 2012, 3, 71–74. [Google Scholar]
- Jain, A.R.; Dhanraj, M. A clinical review of spacer design for conventional complete denture. Biol. Med. 2016, 8, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Rathee, M.; Jain, P.; Shetya, A.G.; Wakhure, P. Rehabilitation of an Edentulous Patient with Flabby Ridge Using Modifed Window Technique—A Case Report. J. Dent. Oral Disord. 2020, 6, 1149. [Google Scholar]
- Bratu, D.; Ieremia, L.; Uram-Ţuculescu, S. Bazele Clinice şi Tehnice ale Protezării Edentației Totale; Editura Medicală: Timișoara, Romania, 2005; p. 480. [Google Scholar]
- Cawood, J.I.; Howell, R.A. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef]
- Christopher, D.L.; Patrick, F.A. Management of the flabby ridge: Using contemporary materials to solve an old problem. BDJ 2005, 32, 558–561. [Google Scholar]
- Appelbaum, E.M.; Rivetti, H.C. Wax base development for complete denture impressions. J. Prosthet. Dent. 1985, 53, 663–667. [Google Scholar] [CrossRef]
- Bansal, R.; Kumar, M.; Garg, R.; Saini, R.; Kaushala, S. Prosthodontic rehabilitation of patient with flabby ridges with different impression techniques. Indian J. Dent. 2014, 5, 110–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, R.W.; Walmsleya, A.D. Review of prosthodontic management of fibrous ridges. Br. Dent. J. 2005, 199, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, R.P.; Tolman, D.E. Etiology and management of hypermobile mucosa overlying the residual alveolar ridge. J. Prosthet. Dent. 1974, 32, 619–638. [Google Scholar] [CrossRef]
- Devlin, H. A method for recording an impression for a patient with a fibrous maxillary alveolar ridge. Quint Int. 1985, 6, 395–397. [Google Scholar]
- Lynch, C.D.; Allen, P.F. Management of the flabby ridge: Re-visiting the principles of complete denture construction. Eur. J. Prosthet. Rest Dent. 2003, 11, 145–148. [Google Scholar]
- Ali, M.; Chaturvedi, S.; Shah, M. Innovative tunnel technique for mandibular flabby ridge. Int. J. Dent. Clin. 2012, 4, 74–76. [Google Scholar]
- Rohit, R.; Shajahan, P.A. Poornima Purushothaman. Prosthodontic management of flabby tissue using modified custom tray design and single impression technique. Int. J. Appl. Decis. Sci. 2019, 5, 50–53. [Google Scholar]
- Khurshid, A.; Mattoo Lakshya, K.; Shuja, R. Flabby Ridge Management Using Paint on Technique—Meticulous Review. J. Med. Sci. Clin. Res. 2019, 7, 518–521. [Google Scholar]
- Labban, N. Management of the flabby ridge using a modified window technique and polyvinylsiloxane impression material. J. Sdentj. 2018, 30, 89–93. [Google Scholar] [CrossRef]
















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ştefănescu, C.-L.; Zaharia, A.; Murineanu, R.M.; Puşcaşu, C.G.; Sachelarie, L.; Grigorian, M. Flabby Ridge, a Challenge for Making Complete Dentures. Appl. Sci. 2021, 11, 7386. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167386
Ştefănescu C-L, Zaharia A, Murineanu RM, Puşcaşu CG, Sachelarie L, Grigorian M. Flabby Ridge, a Challenge for Making Complete Dentures. Applied Sciences. 2021; 11(16):7386. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167386
Chicago/Turabian StyleŞtefănescu, Corina-Laura, Agripina Zaharia, Rodica Maria Murineanu, Cristina Gabriela Puşcaşu, Liliana Sachelarie, and Mircea Grigorian. 2021. "Flabby Ridge, a Challenge for Making Complete Dentures" Applied Sciences 11, no. 16: 7386. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167386