
Cytokine-Related Effect of Buccal-Delivered Collagen Peptide Incorporated in Mucoadhesive Films to Improve Female Skin Conditions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Collagen Peptide Buccal Delivery Film
2.2. Permeation of the Collagen Peptide Buccal Delivery Film
2.3. Study Design and Ethical Aspects
2.4. Study Volunteers and Study Schedule
2.5. Test Product and Placebo
2.6. Measurements
2.6.1. Skin Hydration
2.6.2. Skin Elasticity
2.6.3. Skin Roughness
2.6.4. Questionnaire
2.7. Cytokine Test
2.7.1. Cell Line
2.7.2. Bradford, Peroxynitrite (ONOO−), and Interleukin-1α (IL-1α) Assay
2.8. Statistical Analysis
3. Results
3.1. Permeation of the Collagen Peptide Buccal Delivery Film
3.2. Characteristics of Volunteers
3.3. Skin Hydration
3.4. Skin Elasticity
3.5. Skin Roughness
3.6. Questionnaire
3.7. Cytokine Results
3.7.1. Bradford Assay
3.7.2. Peroxynitrite (ONOO−) and Interleukin-1α
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sorushanova, A.; Delgado, L.M.; Wu, Z.; Shologu, N.; Kshirsagar, A.; Raghunath, R.; Mullen, A.M.; Bayon, Y.; Pandit, A.; Raghunath, M.; et al. The collagen suprafamily: From bio-synthesis to advanced biomaterial development. Adv. Mater. 2019, 31, e1801651. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, M.I.A.; Barroso, L.G.R.; Sánchez, M.L. Collagen: A review on its sources and potential cosmetic applications. J. Cosmet. Dermatol. 2017, 17, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Rizk, M.A.; Mostafa, N.Y. Extraction and characterization of collagen from buffalo skin for bio-medical applications. Orient. J. Chem. 2016, 32, 1601–1609. [Google Scholar] [CrossRef]
- Blackburn, N.J.; Sofrenovic, T.; Kuraitis, D.; Ahmadi, A.; McNeill, B.; Deng, C.; Rayner, K.; Zhong, Z.; Ruel, M.; Suuronen, E.J. Timing underpins the benefits associated with injectable collagen biomaterial therapy for the treatment of myocardial infarction. Biomaterials 2014, 39, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.L.; Marques, A.L.P.; Martins, E.; Silva, T.H.; Reis, R.L. Cosmetic Potential of Marine Fish Skin Collagen. Cosmetics 2017, 4, 39. [Google Scholar] [CrossRef] [Green Version]
- Guillerme, J.-B.; Couteau, C.; Coiffard, L. Applications for Marine Resources in Cosmetics. Cosmetics 2017, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Xhauflaire-Uhoda, E.; Fontaine, K.; Piérard, G. Kinetics of moisturizing and firming effects of cosmetic formulations. Int. J. Cosmet. Sci. 2008, 30, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Yamada, S.; Ikeda, T.; Yanagiguchi, K. Marine Cosmeceuticals: Trends and Prospects; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Morgantii, P.; Randazzo, S.; Cardilloi, A. Role of insoluhle and soluhle collagen as skin moisturizer. J. Appl. Cosmetol. 1986, 4, 141–152. [Google Scholar]
- Fluhr, J.W.; Elsner, P.; Berardesca, E.; Maibach, H.I. Bioengineering of the Skin: Water and the Stratum Corneum; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Peng, Y.; Glattauer, V.; Werkmeister, J.A.; Ramshaw, J.A.M. Evaluation for collagen products for cosmetic application. Int. J. Cosmet. Sci. 2004, 26, 313. [Google Scholar] [CrossRef]
- Nikolaeva, T.I.; Laurinavichus, K.S.; Kaptsov, V.V.; Molchanov, M.V.; Shekhovtsov, P.V. Development of Low-Molecular Weight Collagen Peptide Complex with Glycosaminoglycan Components. Bull. Exp. Biol. Med. 2018, 165, 629–634. [Google Scholar] [CrossRef]
- Koo, J.; Lee, S.; Yeo, S.; Kim, D.; Park, M.; Nam, T.S.; Lee, J. Viscosity Effects of Hydrophilic Polymers on Transport of Collagen Hydrolysate Across Reconstructed Human Buccal Tissue. Bull. Korean Chem. Soc. 2020, 41, 290–295. [Google Scholar] [CrossRef]
- Kiela, P.R.; Ghishan, F.K. Physiology of Intestinal Absorption and Secretion. Best Pr. Res. Clin. Gastroenterol. 2016, 30, 145–159. [Google Scholar] [CrossRef] [Green Version]
- Martin, L.; Wilson, C.G.; Koosha, F.; Uchegbu, I.F. Sustained buccal delivery of the hydrophobic drug denbufylline using physically cross-linked palmitoyl glycol chitosan hydrogels. Eur. J. Pharm. Biopharm. 2003, 55, 35–45. [Google Scholar] [CrossRef]
- Siddiqui, M.; Garg, G.; Sharma, P.K. A short review on “A novel approach in oral fast dissolving drug delivery system and their patents”. Adv. Biol. Res. 2011, 5, 291–303. [Google Scholar]
- Castro, P.M.; Baptista, P.; Madureira, A.R.; Sarmento, B.; Pintado, M.E. Combination of PLGA nanoparticles with mucoadhesive guar-gum films for buccal delivery of antihypertensive peptide. Int. J. Pharm. 2018, 547, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Metia, P.K.; Bandyopadhyay, A.K. In vitro and in vivo evaluation of a novel mucoadhesive buccal oxytocin tablet prepared with Dillenia indica fruit mucilage. Die Pharm. Int. J. Pharm. Sci. 2008, 270–274. [Google Scholar] [CrossRef]
- Langoth, N.; Bernkop-Schnürch, A.; Kurka, P. In Vitro Evaluation of Various Buccal Permeation Enhancing Systems for PACAP (Pituitary Adenylate Cyclase-Activating Polypeptide). Pharm. Res. 2005, 22, 2045–2050. [Google Scholar] [CrossRef]
- Bird, A.P.; Faltinek, J.R.; Shojaei, A.H. Transbuccal peptide delivery: Stability and in vitro per-meation studies on endomorphin-1. J. Control. Release 2001, 73, 31–36. [Google Scholar] [CrossRef]
- Bolke, L.; Schlippe, G.; Gerß, J.; Voss, W. A Collagen Supplement Improves Skin Hydration, Elasticity, Roughness, and Density: Results of a Randomized, Placebo-Controlled, Blind Study. Nutrients 2019, 11, 2494. [Google Scholar] [CrossRef] [Green Version]
- Faocd, D.O.; Kathy, L.A. Clinical Evidence of the Anti-Aging Effects of a Collagen Peptide Nutraceutical Drink on the Skin. J Drugs Dermatol. 2020, 19, s5–s10. [Google Scholar]
- Anonymous International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use ICH Harmonised Guideline: Integrated addendum to ICH E6; Clinical Practice, European Medicines Agency: London, UK, 2016; R1: Guideline for Good, E6(R2).
- Stroumza, N.; Bosc, R.; Hersant, B.; Hermeziu, O.; Meningaud, J.P. Benefits of using the cut-ometer to evaluate the effectiveness of skin treatments in plastic and maxillofacial surgery. Rev. Stomatol. Chir. Maxillo-Faciale Chir. Orale 2015, 116, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Willy, K.; Girndt, M.; Voelkl, J.; Fiedler, R.; Martus, P.; Storr, M.; Schindler, R.; Zickler, D. Expanded haemodialysis therapy of chronic haemodialysis patients prevents calcification and apoptosis of vascular smooth muscle cells in vitro. Blood Purif. 2018, 45, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Inoue, N.; Sugihara, F.; Wang, X. Ingestion of bioactive collagen hydrolysates enhance facial skin moisture and elasticity and reduce facial ageing signs in a randomised double-blind placebo-controlled clinical study. J. Sci. Food Agric. 2016, 96, 4077–4081. [Google Scholar] [CrossRef] [PubMed]
- Asserin, J.; Lati, E.; Shioya, T.; Prawitt, J. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: Evidence from an ex vivo model and randomized, placebo-controlled clinical trials. J. Cosmet. Dermatol. 2015, 14, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Proksch, E.; Schunck, M.; Zague, V.; Segger, D.; Degwert, J.; Oesser, S. Oral Intake of Specific Bioactive Collagen Peptides Reduces Skin Wrinkles and Increases Dermal Matrix Synthesis. Ski. Pharmacol. Physiol. 2014, 27, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Proksch, E.; Segger, D.; Degwert, J.; Schunck, M.; Zague, V.; Oesser, S. Oral Supplementation of Specific Collagen Peptides Has Beneficial Effects on Human Skin Physiology: A Double-Blind, Placebo-Controlled Study. Ski. Pharmacol. Physiol. 2014, 27, 47–55. [Google Scholar] [CrossRef]
- Zague, V.; de Freitas, V.; da Costa Rosa, M.d.C.; de Castro, G.Á; Jaeger, R.G.; Machado-Santelli, G.M. Collagen hydrolysate intake increases skin collagen expression and suppresses matrix metalloproteinase 2 activity. J. Med. Food 2011, 14, 618–624. [Google Scholar] [CrossRef]
- Iwai, K.; Hasegawa, T.; Taguchi, Y.; Morimatsu, F.; Sato, K.; Nakamura, Y.; Higashi, A.; Kido, Y.; Nakabo, Y.; Ohtsuki, K. Identification of Food-Derived Collagen Peptides in Human Blood after Oral Ingestion of Gelatin Hydrolysates. J. Agric. Food Chem. 2005, 53, 6531–6536. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, S.; Morifuji, M.; Ohara, H.; Matsumoto, H.; Takeuchi, Y.; Sato, K. Hydroxypro-line-containing dipeptides and tripeptides quantified at high concentration in human blood after oral administration of gelatin hydrolysate. Int. J. Food Sci. Nutr. 2010, 61, 52–60. [Google Scholar] [CrossRef]
- Dubey, V.; Mishra, D.; Asthana, A.; Jain, N.K. Transdermal delivery of a pineal hormone: Melatonin via elastic liposomes. Biomaterials 2006, 27, 3491–3496. [Google Scholar] [CrossRef] [PubMed]
- Asai, T.T.; Oikawa, F.; Yoshikawa, K.; Inoue, N.; Sato, K. Food-derived collagen peptides, prolyl-hydroxyproline (Pro–Hyp), and hydroxyprolyl-glycine (Hyp–Gly) enhance growth of primary cultured mouse skin fibroblast using fetal bovine serum free from hydroxyprolyl peptide. Int. J. Mol. Sci. 2019, 21, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeley, B.M.; Denton, A.B.; Ahn, M.S.; Maas, C.S. Effect of homeopathic Arnica montana on bruising in face-lifts: Results of a randomized, double-blind, placebo-controlled clinical trial. Arch. Facial Plast. Surg. 2006, 8, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldschmidt, M.; Clemow, J.B. Neuromodulators (Botox). In Applied Head and Neck Anatomy for the Facial Cosmetic Surgeon; Springer: Berlin/Heidelberg, Germany, 2021; pp. 123–129. [Google Scholar]
- Boilard, E.; Nigrovic, P.A.; Larabee, K.; Watts, G.; Coblyn, J.S.; Weinblatt, M.E.; Massarotti, E.M.; Remold-O’Donnell, E.; Farndale, R.W.; Ware, J.; et al. Platelets Amplify Inflammation in Arthritis via Collagen-Dependent Microparticle Production. Science 2010, 327, 580–583. [Google Scholar] [CrossRef] [Green Version]
- Yamanishi, Y.; Boyle, D.L.; Pinkoski, M.J.; Mahboubi, A.; Lin, T.; Han, Z.; Zvaifler, N.J.; Green, D.; Firestein, G.S. Regulation of Joint Destruction and Inflammation by p53 in Collagen-Induced Arthritis. Am. J. Pathol. 2002, 160, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Lubberts, E.; Joosten, L.A.B.; Oppers, B.; Bersselaar, L.V.D.; Roo, C.J.J.C.-D.; Kolls, J.K.; Schwarzenberger, P.; Van De Loo, F.A.J.; Berg, W.B.V.D. IL-1-Independent Role of IL-17 in Synovial Inflammation and Joint Destruction During Collagen-Induced Arthritis. J. Immunol. 2001, 167, 1004–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, Y.J.; Lee, D.G.; Lee, S.B. Late-onset migrated inflammatory granuloma after collagen-containing filler injection. J. Korean Ophthalmol. Soc. 2008, 49, 1330–1334. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.S.; Han, H. Anti-inflammatory activity Effects of Mori Folium Water Extraction IL-1α, IL-6 and IL-10 on mouse macrophages. J. Digit. Converg. 2018, 16, 613–620. [Google Scholar]
- Chung, H.Y.; Kim, H.J.; Kim, K.W.; Choi, J.S.; Yu, B.P. Molecular inflammation hypothesis of aging based on the anti-aging mechanism of calorie restriction. Microsc. Res. Tech. 2002, 59, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Soung, D.; Kim, A.; Choi, H.; Kim, H.; Choi, J.; Yang, R.; Lee, K.; Yu, B. Generation, toxicity and scavenging of ONOO−: Its involvement in the aging process. Kor. J. Gerontol. 2000, 10, 46–59. [Google Scholar]
- Kweon, Y.; Jeong, J. Peroxynitrite scavenging activity of Sabohwanin lipopolysaccha-ride-induced oxidatively-stressed mice. J. Intern. Korean Med. 2007, 28, 80–91. [Google Scholar]
- Kato, Y.; Ogino, Y.; Aoki, T.; Uchida, K.; Kawakishi, S.; Osawa, T. Phenolic Antioxidants Prevent Peroxynitrite-Derived Collagen Modification in Vitro. J. Agric. Food Chem. 1997, 45, 3004–3009. [Google Scholar] [CrossRef]
- Evans, L.C.; Liu, H.; Pinkas, G.A.; Thompson, L.P. Chronic hypoxia increases peroxynitrite, MMP9 expression, and collagen accumulation in fetal guinea pig hearts. Pediatr. Res. 2011, 71, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Dooley, A.; Gao, B.; Shi-Wen, X.; Abraham, D.J.; Black, C.M.; Jacobs, M.; Bruckdorfer, K.R. Effect of nitric oxide and peroxynitrite on type I collagen synthesis in normal and scleroderma dermal fibroblasts. Free. Radic. Biol. Med. 2007, 43, 253–264. [Google Scholar] [CrossRef]
- Tingstrom, A.; Heldin, C.; Rubin, K. Regulation of fibroblast-mediated collagen gel contraction by platelet-derived growth factor, interleukin-1 alpha and transforming growth factor-beta 1. J. Cell Sci. 1992, 102, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Poole, A.R. A fibronectin fragment induces type II collagen degradation by colla-genase through an interleukin-1—mediated pathway. Arthritis Rheum. 2002, 46, 138–148. [Google Scholar] [CrossRef]


 ), and max–min whiskers (I). The changes were significantly different between the control and test groups, and before and after intake, with p < 0.001 (***).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, and before and after intake, with p < 0.001 (***).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, and before and after intake, with p < 0.001 (***).
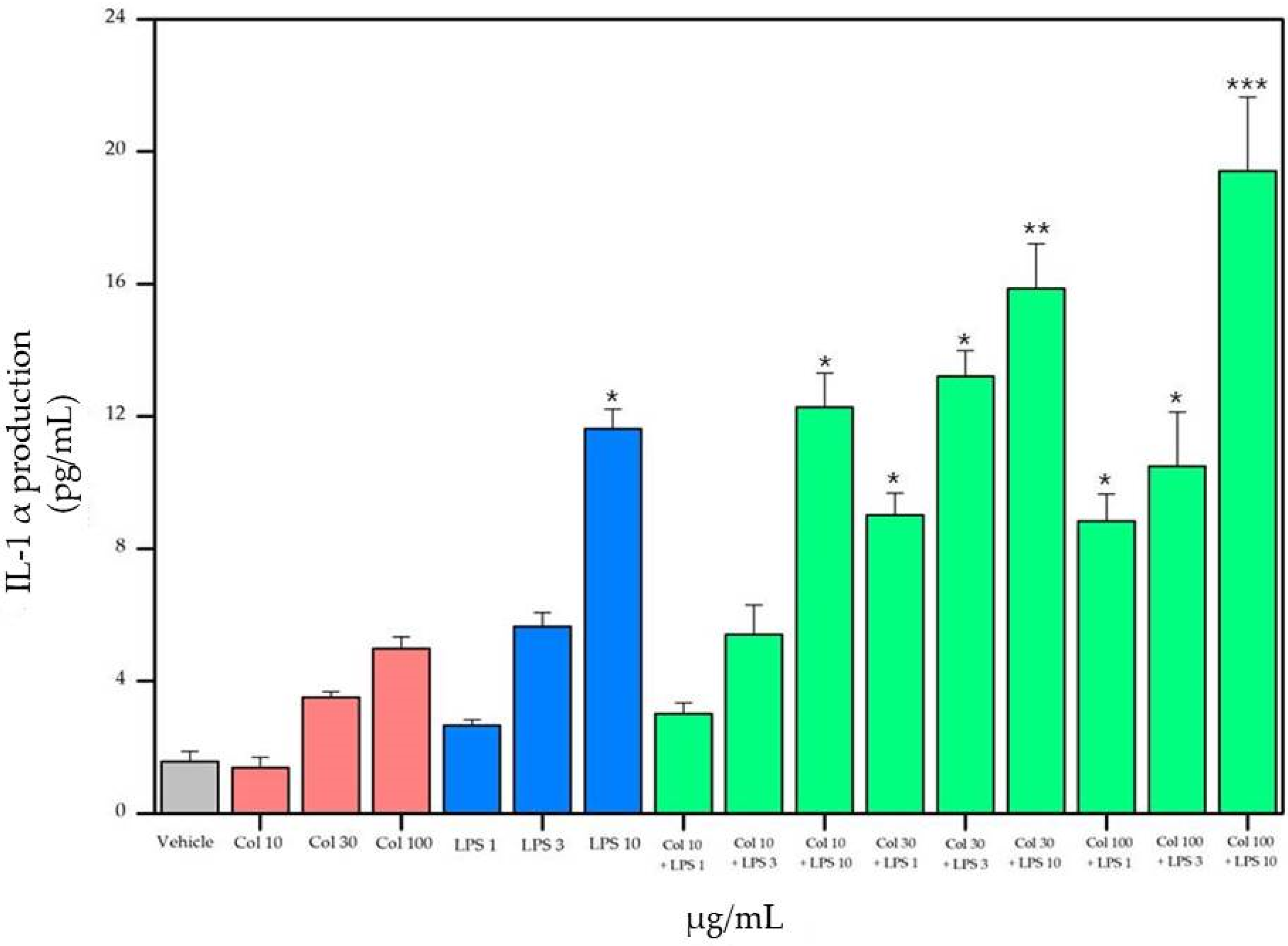
), and max–min whiskers (I). The changes were significantly different between the control and test groups, and before and after intake, with p < 0.001 (***). ), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*), p < 0.01 (**), and p < 0.001 (***).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*), p < 0.01 (**), and p < 0.001 (***).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*), p < 0.01 (**), and p < 0.001 (***).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*), p < 0.01 (**), and p < 0.001 (***). ), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*) and p < 0.01 (**).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*) and p < 0.01 (**).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*) and p < 0.01 (**).
), and max–min whiskers (I). The changes were significantly different between the control and test groups, before and after intake, with p < 0.05 (*) and p < 0.01 (**). 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protective Layer | Muco Layer | ||
|---|---|---|---|
| Components | Proportion (%) | Components | Proportion (%) |
| HPMC | 10.0 | Collagen peptide | 10.7 |
| HPC | 7.7 | HPMC | 8.8 |
| Glycerin | 0.7 | Carrageenan | 0.4 |
| Water | 29.4 | Sucrose distearate | 0.2 |
| Ethanol | 52.2 | Glycerin | 0.7 |
| - | - | Polyacrylate | 0.7 |
| - | - | Water | 62.4 |
| - | - | Ethanol | 16.1 |
| Parameters | Classification | Control Group (n = 21) | Test Group (n = 22) | ||
|---|---|---|---|---|---|
| Frequency (n) | Proportion (%) | Frequency (n) | Proportion (%) | ||
| Age | 30s | 0 | 0.00 | 1 | 4.55 |
| 40s | 10 | 47.62 | 15 | 68.18 | |
| 50s | 11 | 52.38 | 6 | 27.27 | |
| Skin type | Dry skin | 15 | 71.43 | 11 | 50.00 |
| Oily skin | 0 | 0.00 | 1 | 4.55 | |
| Normal skin | 4 | 19.05 | 3 | 13.64 | |
| Combination skin | 2 | 9.52 | 7 | 31.82 | |
| Skin irritation reaction to the environment | Yes | 0 | 0.00 | 0 | 0.00 |
| No | 21 | 100.00 | 22 | 100.00 | |
| Prickle and itch | Yes | 0 | 0.00 | 0 | 0.00 |
| No | 21 | 100.00 | 22 | 100.00 | |
| Side effects | Yes | 0 | 0.00 | 0 | 0.00 |
| No | 21 | 100.00 | 22 | 100.00 | |
| Change in skin condition during menstruation | Yes | 1 | 4.76 | 1 | 4.55 |
| No | 20 | 95.24 | 21 | 95.45 | |
| Applied sunscreen | Daily use | 8 | 38.10 | 10 | 45.45 |
| Used when going out | 13 | 61.90 | 12 | 54.55 | |
| Not used | 0 | 0.00 | 0 | 0.00 | |
| Sensory Question (1) | Control Group | Test Group | ||
|---|---|---|---|---|
| 2 w | 4 w | 2 w | 4 w | |
| The degree of skin hydration | 3.95 ± 0.74 | 4.38 ± 0.74 | 4.14 ± 0.64 * | 4.73 ± 0.83 * |
| The degree of reduction in sagging skin | 3.62 ± 0.67 * | 4.14 ± 0.91 * | 3.86 ± 0.83 * | 4.45 ± 0.91 * |
| The degree of elasticity of the skin | 3.81 ± 0.81 | 4.33 ± 0.91 | 4.18 ± 0.85 * | 4.68 ± 0.78 * |
| The degree of smoothness of the skin | 4.14 ± 0.57 | 4.43 ± 0.87 | 4.27 ± 0.70 | 4.73 ± 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.H.; Im, D.; Lee, K.-H.; Yoon, S.; Ham, Y.B. Cytokine-Related Effect of Buccal-Delivered Collagen Peptide Incorporated in Mucoadhesive Films to Improve Female Skin Conditions. Appl. Sci. 2021, 11, 7486. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167486
Kim YH, Im D, Lee K-H, Yoon S, Ham YB. Cytokine-Related Effect of Buccal-Delivered Collagen Peptide Incorporated in Mucoadhesive Films to Improve Female Skin Conditions. Applied Sciences. 2021; 11(16):7486. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167486
Chicago/Turabian StyleKim, Yeon Ho, Dahye Im, Kyung-Hee Lee, Saemi Yoon, and Yun Beom Ham. 2021. "Cytokine-Related Effect of Buccal-Delivered Collagen Peptide Incorporated in Mucoadhesive Films to Improve Female Skin Conditions" Applied Sciences 11, no. 16: 7486. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167486