
Is the Course of Headache Complaints Related to the Course of Orofacial Pain and Disability in Patients Treated for Temporomandibular Pain? An Observational Study

 , , ,
, , ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Ethics and Registration
2.2. Study Population
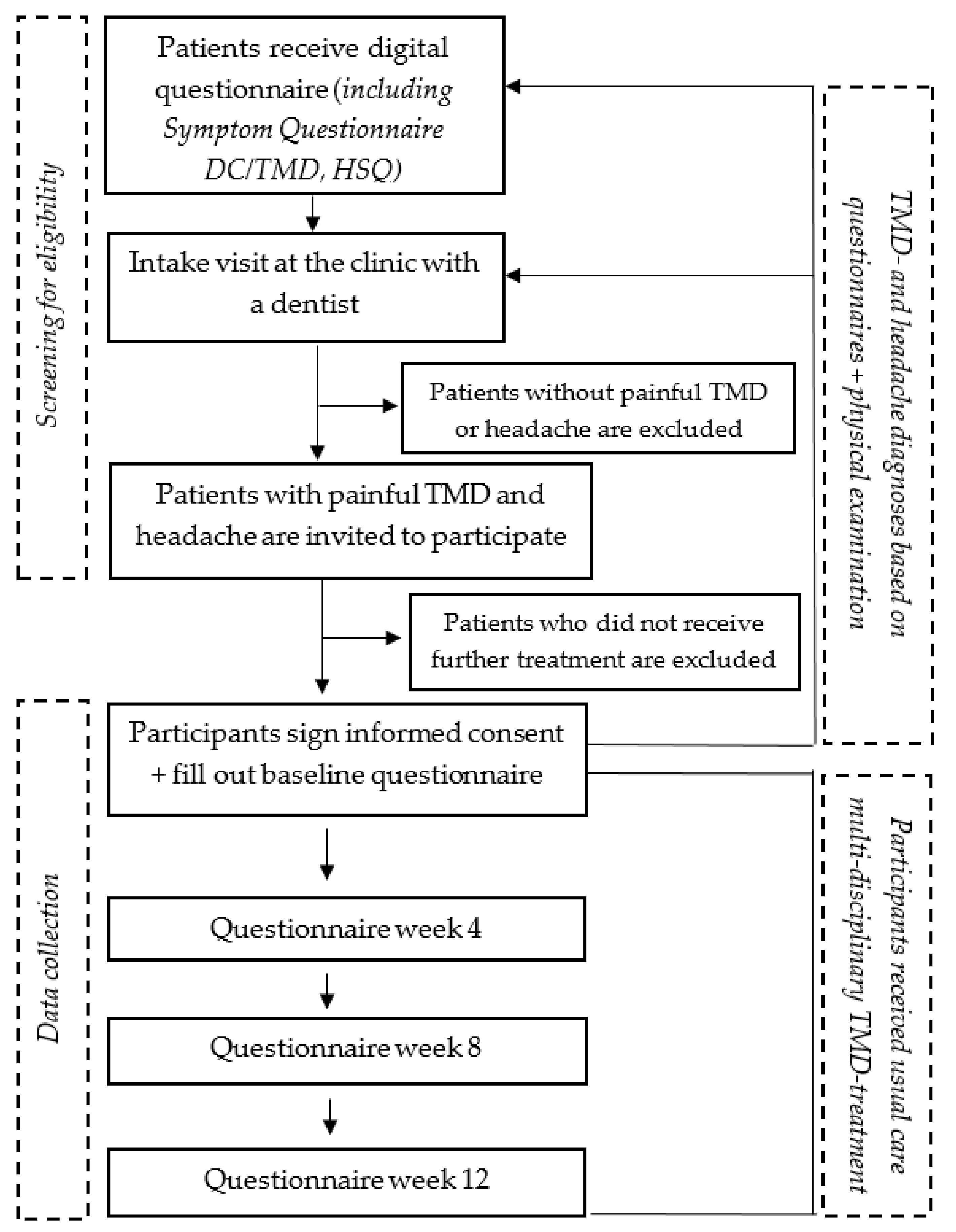
2.3. Flow of the Study
2.4. TMD-Pain
2.5. Headache
2.6. Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Study Population
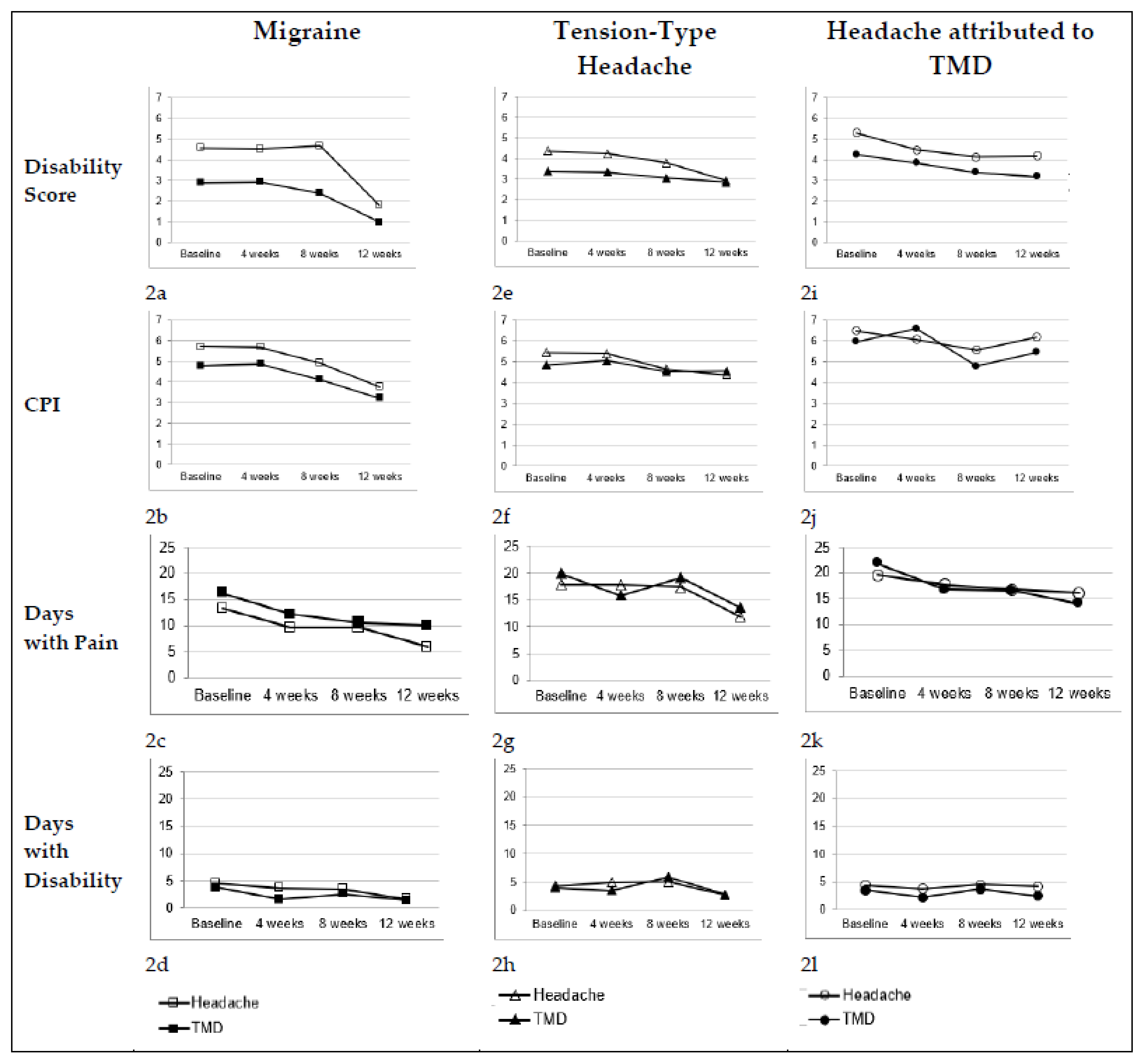
3.2. Longitudinal Course of TMD and Migraine Complaints
3.3. Longitudinal Course of TMD and Tension-Type Headache Complaints
3.4. Longitudinal Course of TMD and Headache Attributed to TMD Complaints
4. Discussion
4.1. Primary Outcome Measure: Disability Score
4.2. Secondary Outcome Measures: Pain Intensity, Days with Pain and Days with Disability
4.3. Limitations of the Study
4.4. Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- LeResche, L. Epidemiology of Temporomandibular Disorders: Implications for the Investigation of Etiologic Factors. Crit. Rev. Oral Biol. Med. 1997, 8, 291–305. [Google Scholar] [CrossRef]
- de Leeuw, R.; Klasser, G.D. American Academy of Orofacial Pain Guidelines for Assessment, Diagnosis, and Management, 6th ed.; Quintessence Publishing Co.: Berlin, Germany, 2018. [Google Scholar]
- Rollman, A.; Visscher, C.M.; Gorter, R.C.; Naeije, M. Care seeking for orofacial pain. J. Orofac. Pain 2012, 26, 206–214. [Google Scholar] [PubMed]
- Türp, J.; Kowalski, C.; O’Leary, N.; Stohler, C. Pain Maps from Facial Pain Patients Indicate a Broad Pain Geography. J. Dent. Res. 1998, 77, 1465–1472. [Google Scholar] [CrossRef]
- Visscher, C.M.; Lobbezoo, F.; De Boer, W.; Van Der Zaag, J.; Naeije, M. Prevalence of cervical spinal pain in craniomandibular pain patients. Eur. J. Oral Sci. 2001, 109, 76–80. [Google Scholar] [CrossRef]
- Van der Meer, H.A.; Speksnijder, C.M.; Engelbert, R.H.H.; Lobbezoo, F.; Nijhuis-van der Sanden, M.W.G.; Visscher, C.M. The association between headaches and temporomandibular disorders is confounded by bruxism and somatic complaints. Clin. J. Pain 2017, 33, 835–843. [Google Scholar] [CrossRef]
- Franco, A.L.; Gonçalves, D.; Castanharo, S.M.; Speciali, J.G.; Bigal, M.E.; Camparis, C.M. Migraine is the most prevalent primary headache in individuals with temporomandibular disorders. J. Orofac. Pain 2010, 24, 287–292. [Google Scholar]
- Di Paolo, C.; D’Urso, A.; Papi, P.; Di Sabato, F.; Rosella, D.; Pompa, G.; Polimeni, A. Temporomandibular Disorders and Headache: A Retrospective Analysis of 1198 Patients. Pain Res. Manag. 2017, 2017, 3203027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goncalves, D.A.G.; Camparis, C.M.; Speciali, J.G.; Franco, A.L.; Castanharo, S.M.; Bigal, M.E. Temporomandibular Disorders are differentially associated with headache diagnoses; a controlled study. Clin. J Pain. 2011, 27, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, D.A.G.; Camparis, C.M.; Speciali, J.G.; Castanharo, S.M.; Ujikawa, L.T.; Lipton, R.B.; Bigal, M.E. Treatment of Comorbid Migraine and Temporomandibular Disorders: A Factorial, Double-Blind, Randomized, Placebo-Controlled Study. J. Orofac. Pain 2013, 27, 325–335. [Google Scholar] [CrossRef]
- Garrigós Pedrón, M.; La Touche, R.; Navarro-Desentre, P.; Gracia-Naya, M.; Segura-Ortí, E. Effects of a Physical Therapy Protocol in Patients with Chronic Migraine and Temporomandibular Disorders: A Randomized, Single-Blinded, Clinical Trial. J. Oral Fac. Pain Headache 2018, 32, 137–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hara, K.; Shinozaki, T.; Okada-Ogawa, A.; Matsukawa, Y.; Dezawa, K.; Nakaya, Y.; Chen, J.-Y.; Noma, N.; Oka, S.; Iwata, K.; et al. Headache attributed to temporomandibular disorders and masticatory myofascial pain. J. Oral Sci. 2016, 58, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Su, N.; Visscher, C.M.; Van Wijk, A.J.; Lobbezoo, F.; Van Der Heijden, G.J. A Prediction Model for Types of Treatment Indicated for Patients with Temporomandibular Disorders. J. Oral Fac. Pain Headache 2019, 33, 25–38. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Fac. Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Van Der Meer, H.A.; Visscher, C.M.; Engelbert, R.H.H.; Mulleners, W.M.; Nijhuis-van der Sanden, M.W.G.; Speksnijder, C.M. Development and psychometric validation of the headache screening questionnaire—Dutch Version. Musculoskelet. Sci. Pract. 2017, 31, 52–61. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; List, T.; Anderson, G.; Jensen, R.; John, M.T.; Nixdorf, D.; Goulet, J.-P.; Kang, W.; Truelove, E.; et al. Diagnostic criteria for headache attributed to temporomandibular disorders. Cephalalgia 2012, 32, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Von Korff, M.; Ormel, J.; Keefe, F.J.; Dworkin, S.F. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Günther, T.; Schierz, O.; Hahnel, S.; Rauch, A. Field-testing a psychosocial assessment scoring form for TMD patients—Summarizing axis II instruments. BMC Oral Health 2020, 20, 267. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 21 August 2021).
- Salaffi, F.; Stancati, A.; Silvestri, C.A.; Ciapetti, A.; Grassi, W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain 2004, 8, 283–291. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Kang, J.-H. Effects on migraine, neck pain, and head and neck posture, of temporomandibular disorder treatment: Study of a retrospective cohort. Arch. Oral Biol. 2020, 114, 104718. [Google Scholar] [CrossRef]
- Conti, P.C.R.; Costa, Y.M.; Gonçalves, D.A.; Svensson, P. Headaches and myofascial temporomandibular disorders: Overlapping entities, separate managements? J. Oral Rehabil. 2016, 43, 702–715. [Google Scholar] [CrossRef]
- Tassorelli, C.; Diener, H.-C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of chronic migraine in adults. Cephalalgia 2018, 38, 815–832. [Google Scholar] [CrossRef]
- Van der Meer, H.A.; Calixtre, L.B.; Engelbert, R.H.H.; Visscher, C.M.; Nijhuis-van der Sanden, M.W.; Speksnijder, C.M. Effects of physical therapy for temporomandibular disorders on headache pain intensity: A systematic review. Musculoskelet. Sci. Pract. 2020, 50, 102277. [Google Scholar] [CrossRef]
- Moseley, G.L.; Butler, D.S. Fifteen Years of Explaining Pain: The Past, Present, and Future. J. Pain 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotze, M.; Moseley, G.L. Theoretical Considerations for Chronic Pain Rehabilitation. Phys. Ther. 2015, 95, 1316–1320. [Google Scholar] [CrossRef] [Green Version]
- Ohrbach, R.; Fillingim, R.B.; Mulkey, F.; Gonzalez, Y.; Gordon, S.; Gremillion, H.; Lim, P.-F.; Ribeiro-Dasilva, M.; Greenspan, J.D.; Knott, C.; et al. Clinical Findings and Pain Symptoms as Potential Risk Factors for Chronic TMD: Descriptive Data and Empirically Identified Domains from the OPPERA Case-Control Study. J. Pain 2011, 12, T27–T45. [Google Scholar] [CrossRef] [Green Version]
- Ligthart, L.; Gerrits, M.M.J.G.; Boomsma, D.I.; Penninx, B.W.J.H. Anxiety and Depression Are Associated With Migraine and Pain in General: An Investigation of the Interrelationships. J. Pain 2013, 14, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Seng, E.K.; Buse, D.C.; Klepper, J.E.; Ma, J.E.K.; Ma, S.J.M.; Ma, A.S.G.; Grosberg, B.M.; Pavlovic, J.M.; Robbins, M.S.; Vollbracht, S.E.; et al. Psychological Factors Associated With Chronic Migraine and Severe Migraine-Related Disability: An Observational Study in a Tertiary Headache Center. Headache J. Head Face Pain 2017, 57, 593–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, D.S.; Buse, D.C.; Lipton, R.B.; Thomas, J.G.; Rathier, L.; Roth, J.; Pavlovic, J.M.; Evans, E.W.; Wing, R.R. Clinical Pain Catastrophizing in Women With Migraine and Obesity. Headache 2015, 55, 923–933. [Google Scholar] [CrossRef] [Green Version]
- Wieckiewicz, M.; Zietek, M.; Smardz, J.; Zenczak-Wieckiewicz, D.; Grychowska, N. Mental Status as a Common Factor for Masticatory Muscle Pain: A Systematic Review. Front. Psychol. 2017, 8, 646. [Google Scholar] [CrossRef] [Green Version]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The Effect of Neuroscience Education on Pain, Disability, Anxiety, and Stress in Chronic Musculoskeletal Pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Warren, S.; Fuentes, J.; Magee, D.J. Clinical relevance vs. statistical significance: Using neck outcomes in patients with temporomandibular disorders as an example. Man. Ther. 2011, 16, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S. The importance of determining the clinical significance of research results in physical therapy clinical research. Braz. J. Phys. Ther. 2018, 22, 175–176. [Google Scholar] [CrossRef]
- Annoni, M.; Miller, F.G. Placebo Effects and the Ethics of Therapeutic Communication: A Pragmatic Perspective. Kennedy Inst. Ethic J. 2016, 26, 79–103. [Google Scholar] [CrossRef]
- Elliott, R.; Bohart, A.C.; Watson, J.C.; Murphy, D. Therapist empathy and client outcome: An updated meta-analysis. Psychotherapy 2018, 55, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. Bias in observational study designs: Prospective. BMJ 2014, 349, g7731. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall Study Population (n = 60) | TMD-Pain and Migraine (n = 22) | TMD-Pain and TTH (n = 21) | TMD-Pain and Headache Attributed to TMD (n = 17) | |
|---|---|---|---|---|
| Age; mean ± sd | 41.3 ± 14.2 | 46.9 ± 13.2 | 39.0 ± 13.8 | 36.8 ± 14.3 |
| Gender; n (%) | ||||
| Female | 50 (83.3) | 20 (90.9) | 15 (71.4) | 15 (88.2) |
| Male | 10 (16.7) | 2 (9.1) | 6 (28.6) | 2 (11.8) |
| TMD pain subtype; n (%) | ||||
| Myalgia | 37 (61.7) | 13 (59.1) | 13 (61.9) | 11 (64.7) |
| Arthralgia | 5 (8.3) | 2 (9.1) | 3 (14.3) | 0 (0.0) |
| Combined myalgia and arthralgia | 18 (30.0) | 7 (31.8) | 5 (23.8) | 6 (35.3) |
| Headache; n (%) | ||||
| (Probable) migraine | 36 (60.0) | 22 (100) | 2 (9.5) | 12 (70.6) |
| (Probable) TTH | 48 (80.0) | 12 (54.5) | 21 (100) | 15 (88.2) |
| Headache attributed to TMD | 17 (28.3) | 0 (0.0) | 0 (0.0) | 17 (100) |
| Duration of TMD pain; n (%) | ||||
| <1 year | 10 (16.7) | 6 (27.3) | 3 (14.3) | 1 (5.9) |
| 1–10 years | 26 (43.3) | 7 (31.8) | 12 (57.1) | 7 (41.2) |
| >10 years | 13 (21.7) | 3 (13.6) | 3 (14.3) | 7 (41.2) |
| Missing | 11 (18.3) | 6 (27.3) | 3 (14.3) | 2 (11.8) |
| Outcome Measure | Type of Pain Complaint | Baseline Mean ± sd | Week 4 Mean ± sd | Week 8 Mean ± sd | Week 12 Mean ± sd | Difference between Complaints F (p-Value) | Change over Time F (p-Value) | Difference between Complaints over Time F (p-Value) |
|---|---|---|---|---|---|---|---|---|
| Migraine (N = 22) | ||||||||
| Disability Score (0–10) | TMD complaints | 2.9 ± 3.1 | 2.9 ± 2.4 | 2.4 ± 2.8 | 1.0 ± 1.1 | 17.162 (0.000) | 8.707 (0.001) | 1.928 (0.159) |
| Headache complaints | 4.6 ± 3.0 | 4.4 ± 2.7 | 4.7 ± 3.4 | 1.8 ± 2.0 | ||||
| CPI (0–10) | TMD complaints | 4.8 ± 2.6 | 5.0 ± 2.6 | 4.1 ± 2.3 | 3.2 ± 2.0 | 2.740 (0.113) | 6.229 (0.004) | 0.578 (0.637) |
| Headache complaints | 5.7 ± 1.6 | 5.7 ± 1.7 | 4.9 ± 1.8 | 3.8 ± 1.7 | ||||
| Days with pain (0–30) | TMD complaints | 16.2 ± 11.1 | 11.9 ± 8.4 | 10.6 ± 8.1 | 10.0 ± 9.4 | 3.470 (0.077) | 4.378 (0.017) | 2.236 (0.117) |
| Headache complaints | 13.3 ± 8.8 | 9.3 ± 5.7 | 9.6 ± 5.3 | 5.8 ± 3.6 | ||||
| Days with Disability (0–30) | TMD complaints | 3.8 ± 6.0 | 1.6 ± 2.0 | 2.6 ± 3.6 | 1.4 ± 2.9 | 4.448 (0.047) | 1.724 (0.196) | 0.920 (0.450) |
| Headache complaints | 4.6 ± 5.8 | 3.7 ± 5.0 | 3.5 ± 4.2 | 1.6 ± 2.9 | ||||
| Tension-Type Headache (N = 21) | ||||||||
| Disability Score (0–10) | TMD complaints | 3.4 ± 2.8 | 3.2 ± 3.0 | 3.1 ± 2.6 | 2.8 ± 2.8 | 5.072 (0.036) | 2.111 (0.135) | 1.352 (0.289) |
| Headache complaints | 4.4 ± 2.9 | 4.1 ± 2.7 | 3.8 ± 2.6 | 2.9 ± 2.8 | ||||
| CPI (0–10) | TMD complaints | 4.8 ± 2.6 | 5.0 ± 2.8 | 4.5 ± 2.3 | 4.5 ± 2.0 | 0.325 (0.575) | 2.533 (0.089) | 0.634 (0.603) |
| Headache complaints | 5.4 ± 2.1 | 5.2 ± 2.1 | 4.6 ± 2.6 | 4.4 ± 2.4 | ||||
| Days with pain (0–30) | TMD complaints | 20.0 ± 10.4 | 16.8 ± 11.0 | 19.2 ± 10.2 | 13.5 ± 10.7 | 0.248 (0.624) | 6.043 (0.005) | 2.236 (0.119) |
| Headache complaints | 17.9 ± 10.5 | 18.6 ± 2.1 | 17.4 ± 10.0 | 11.9 ± 10.3 | ||||
| Days with Disability (0–30) | TMD complaints | 4.0 ± 8.2 | 3.4 ± 5.8 | 5.9 ± 8.1 | 2.8 ± 4.7 | 0.882 (0.359) | 2.758 (0.072) | 1.137 (0.361) |
| Headache complaints | 4.3 ± 8.9 | 4.9 ± 6.8 | 5.1 ± 6.6 | 2.7 ± 4.7 | ||||
| Headache attributed to TMD (N = 17) | ||||||||
| Disability Score (0–10) | TMD complaints | 4.2 ± 2.8 | 4.1 ± 2.9 | 3.4 ± 2.9 | 3.2 ± 2.3 | 2.329 (0.146) | 1.659 (0.221) | 0.274 (0.843) |
| Headache complaints | 5.3 ± 2.4 | 4.7 ± 2.6 | 4.1 ± 2.7 | 4.2 ± 2.6 | ||||
| CPI(0–10) | TMD complaints | 6.0 ± 2.5 | 6.6 ± 1.5 | 4.8 ± 2.5 | 5.5 ± 2.2 | 1.133 (0.303) | 1.975 (0.164) | 3.057 (0.063) |
| Headache complaints | 6.5 ± 2.1 | 6.2 ± 2.1 | 5.6 ± 1.9 | 6.2 ± 1.9 | ||||
| Days with pain (0–30) | TMD complaints | 21.8 ± 10.5 | 16.1 ± 9.2 | 16.6 ± 10.8 | 14.1 ± 10.9 | 0.020 (0.889) | 3.520 (0.043) | 1.598 (0.234) |
| Headache complaints | 19.6 ± 11.6 | 17.6 ± 10.1 | 16.7 ± 8.9 | 16.1 ± 10.5 | ||||
| Days with Disability (0–30) | TMD complaints | 3.5 ± 4.5 | 2.4 ± 2.8 | 3.7 ± 4.9 | 2.5 ± 5.4 | 1.900 (0.187) | 0.783 (0.523) | 0.392 (0.760) |
| Headache complaints | 4.4 ± 5.0 | 4.0 ± 5.2 | 4.5 ± 4.8 | 4.2 ± 6.1 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Meer, H.A.; Calixtre, L.B.; Speksnijder, C.M.; Engelbert, R.H.H.; Nijhuis-van der Sanden, M.W.G.; Visscher, C.M. Is the Course of Headache Complaints Related to the Course of Orofacial Pain and Disability in Patients Treated for Temporomandibular Pain? An Observational Study. Appl. Sci. 2021, 11, 7780. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177780
van der Meer HA, Calixtre LB, Speksnijder CM, Engelbert RHH, Nijhuis-van der Sanden MWG, Visscher CM. Is the Course of Headache Complaints Related to the Course of Orofacial Pain and Disability in Patients Treated for Temporomandibular Pain? An Observational Study. Applied Sciences. 2021; 11(17):7780. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177780
Chicago/Turabian Stylevan der Meer, Hedwig A., Letícia B. Calixtre, Caroline M. Speksnijder, Raoul H. H. Engelbert, Maria W. G. Nijhuis-van der Sanden, and Corine M. Visscher. 2021. "Is the Course of Headache Complaints Related to the Course of Orofacial Pain and Disability in Patients Treated for Temporomandibular Pain? An Observational Study" Applied Sciences 11, no. 17: 7780. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177780