
Comparison of Efficacy between Three-Dimensional Printing and Manual-Bending Implants for Inferomedial Orbital Fracture: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
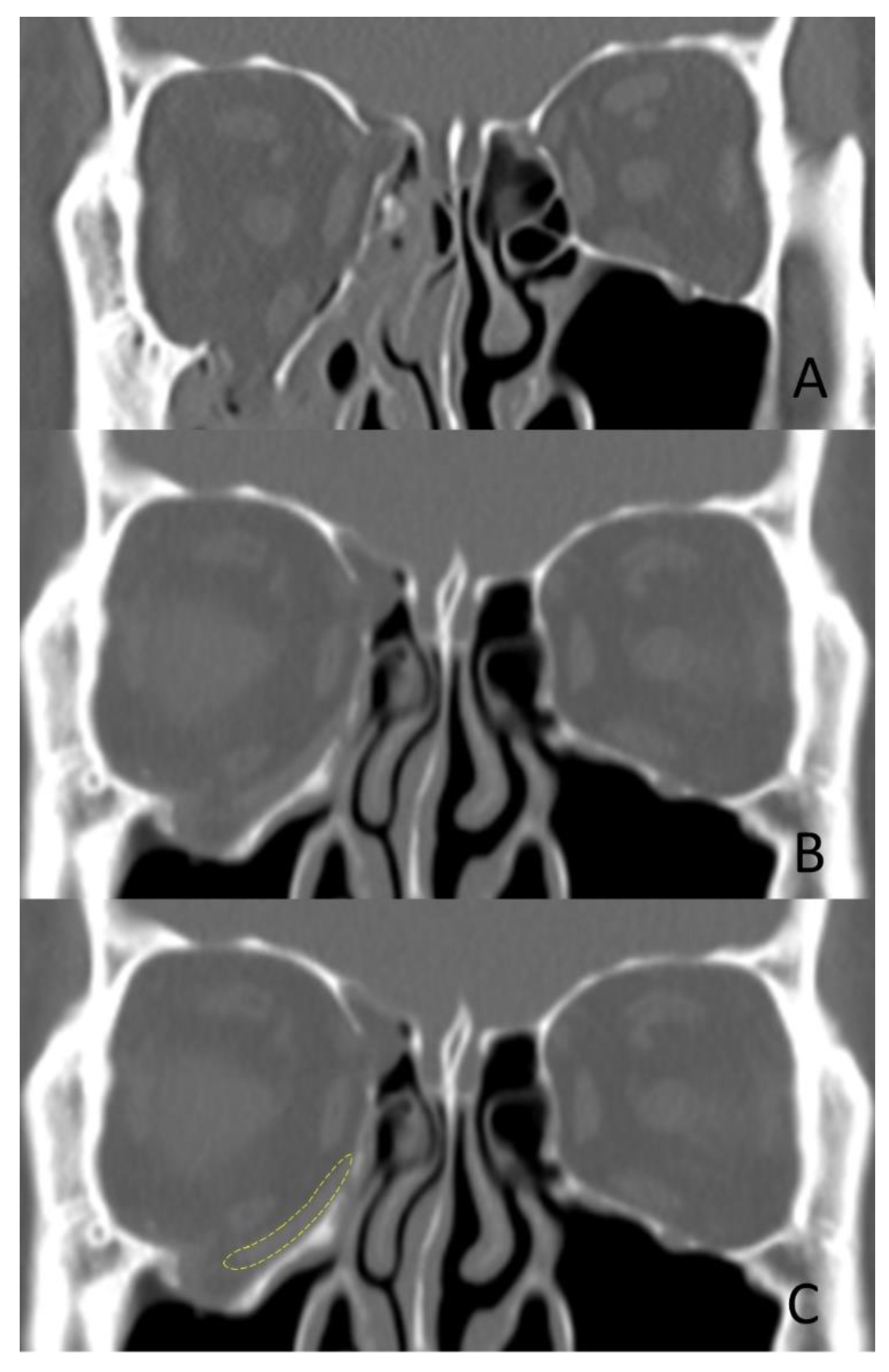
- Diagnosis of unilateral inferomedial orbital fracture with preoperative radiological evaluation including 3D CT
- Surgery within two weeks after injury
- Postoperative evaluation including clinical outcomes and radiological examination including 3D CT within three months postoperative.
- Single fracture of the medial wall or floor of the orbit
- No preoperative or postoperative 3D CT scans
- No postoperative evaluation within three months postoperative
- Surrounding combined fracture requiring open reduction and internal fixation such as fracture of the zygomaticomaxillary complex or frontal bone.
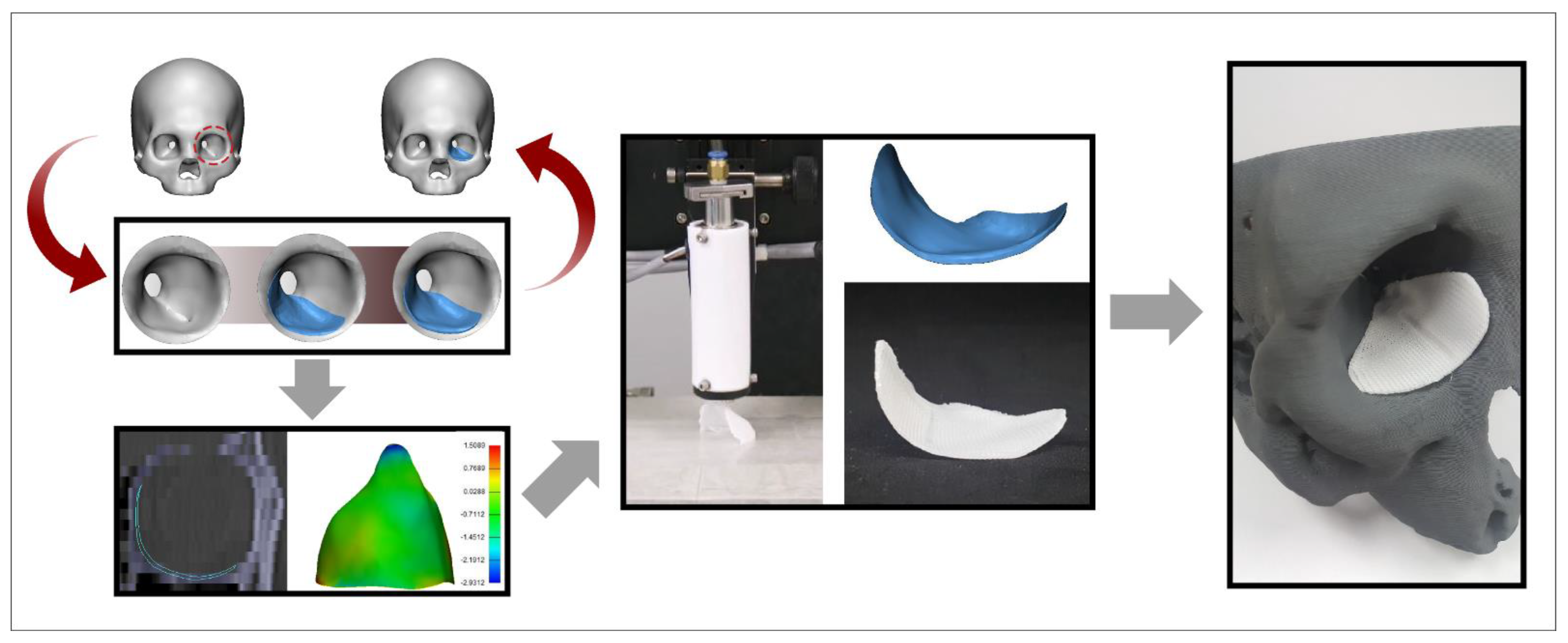
2.1. Fabrication of 3D-Printed Orbital Implant
2.2. Clinical Application
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hammer, B.; Prein, J. Correction of post-traumatic orbital deformities: Operative techniques and review of 26 patients. J. Cranio-Maxillofac. Surg. 1995, 23, 81–90. [Google Scholar] [CrossRef]
- Oh, T.S.; Jeong, W.S.; Chang, T.J.; Koh, K.S.; Choi, J.W. Customized orbital wall reconstruction using three-dimensionally printed rapid prototype model in patients with orbital wall fracture. J. Craniofac. Surg. 2016, 27, 2020–2024. [Google Scholar] [CrossRef]
- Kim, Y.C.; Jeong, W.S.; Park, T.K.; Choi, J.W.; Koh, K.S.; Oh, T.S. The accuracy of patient specific implant prebented with 3D-printed rapid prototype model for orbital wall reconstruction. J. Cranio-Maxillofac. Surg. 2017, 45, 28–36. [Google Scholar] [CrossRef]
- Goldberg, R.A.; Shorr, N.; Cohen, M.S. The medical orbital strut in the prevention of postdecompression dystopia in dysthyroid ophthalmopathy. Ophthalmic Plast. Reconstr. Surg. 1992, 8, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Jordan, D.R.; Anderson, R.L. Orbital decompression. Ophthalmic Plast. Reconstr. Surg. 2000, 16, 167–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stathopoulos, P.; Ameerally, P. Reconstructing a traumatic empty orbit: Principles, difficulties of treatment, and literature review. journal of oral and maxillofacial surgery. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2018, 76, 1952-e1. [Google Scholar] [CrossRef]
- Wright, E.D.; Davidson, J.; Codere, F.; Desrosiers, M. Endoscopic orbital decompression with preservation of an inferomedial bony strut: Minimization of postoperative diplopia. J. Otolaryngol. 1999, 28, 252–256. [Google Scholar] [PubMed]
- Shin, J.W.; Lim, J.S.; Yoo, G.; Byeon, J.H. An analysis of pure blowout fractures and associated ocular symptoms. J. Craniofac. Surg. 2013, 24, 703–707. [Google Scholar] [CrossRef]
- Hur, S.W.; Kim, S.E.; Chung, K.J.; Lee, J.H.; Kim, T.G.; Kim, Y.H. Combined orbital fractures: Surgical strategy of sequential repair. Arch. Plast. Surg. 2015, 42, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Su, G.W.; Harris, G.J. Combined inferior and medial surgical approaches and overlapping thin implants for orbital floor and medial wall fractures. Ophthalmic. Plast. Reconstr. Surg. 2006, 22, 420–423. [Google Scholar] [CrossRef]
- Cordewener, F.W.; Bos, R.R.; Rozema, F.R.; Houtman, W.A. Poly(L-lactide) implants for repair of human orbital floor defects: Clinical and magnetic resonance imaging evaluation of long-term results. J. Oral Maxillofac. Surg. 1996, 54, 9–13. [Google Scholar] [CrossRef]
- Dietz, A.; Ziegler, C.M.; Dacho, A.; Althof, F.; Conradt, C.; Kolling, G.; von Boehmer, H.; Steffen, H. Effectiveness of a new perforated 0.15 mm poly-p-dioxanon-foil versus titanium-dynamic mesh in reconstruction of the orbital floor. J. Maxillofac. Surg. 2001, 29, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.J.; Teng, L.; Jin, X.L.; Ji, Y.; Lu, J.J.; Zhang, B. Porous polyethylene implants in orbital blow-out fractures and enophthalmos reconstruction. J. Craniofac. Surg. 2009, 20, 918–920. [Google Scholar] [PubMed]
- Ono, I.; Gunji, H.; Suda, K.; Kaneko, F.; Yago, K. Orbital reconstruction with hydroxyapatite ceramic implants. Scand. J. Plast. Reconstr. Surg. Hand Surg. 1994, 28, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, S.; Yavuzer, R.; Kandal, S.; Demir, Y.H.; Ozmen, S.; Latifoglu, O.; Atabay, K. Reconstruction of traumatic orbital floor fractures with resorbable mesh plate. J. Craniofac. Surg. 2007, 18, 598–605. [Google Scholar] [CrossRef]
- Stoor, P.; Suomalainen, A.; Lindqvist, C.; Mesimaki, K.; Danielsson, D.; Westermark, A.; Kontio, R.K. Rapid prototyped patient specific implants for reconstruction of orbital wall defects. J. Cranio-Maxillofac. Surg. 2014, 42, 1644–1649. [Google Scholar] [CrossRef]
- Kozakiewicz, M. Computer-aided orbital wall defects treatment by individual design ultrahigh molecular weight polyethylene implants. J. Cranio-Maxillofaci. Surg. 2014, 42, 283–289. [Google Scholar] [CrossRef]
- Lieger, O.; Richards, R.; Liu, M.; Lloyd, T. Computer-assisted design and manufacture of implants in the late reconstruction of extensive orbital fractures. Arch. Facial Plast. Surg. 2010, 12, 186–191. [Google Scholar] [CrossRef]
- Metzger, M.C.; Schön, R.; Weyer, N.; Rafii, A.; Gellrich, N.C.; Schmelzeisen, R.; Strong, B.E. Anatomical 3-dimensional pre-bent titanium implant for orbital floor fractures. Ophthalmology 2006, 113, 1863–1868. [Google Scholar] [CrossRef]
- Cha, J.H.; Moon, M.H.; Lee, Y.H.; Koh, I.C.; Kim, K.N.; Kim, C.G.; Kim, H. Correlation between the 2-dimensional extent of orbital defects and the 3-dimensional volume of herniated orbital content in patients with isolated orbital wall fractures. Arch. Plast. Surg. 2017, 44, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Hassfeld, S.; Muhling, J. Computer assisted oral and maxillofacial surgery—A review and an assessment of technology. International J. Oral Maxillofac. Surg. 2001, 30, 2–13. [Google Scholar] [CrossRef]
- Vignesh, U.; Mehrotra, D.; Anand, V.; Howlader, D. Three dimensional reconstruction of late post traumatic orbital wall defects by customized implants using CAD-CAM, 3D stereolithographic models: A case report. J. Oral Biol. Craniofacial Res. 2017, 7, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Gander, T.; Essig, H.; Metzler, P.; Lindhorst, D.; Dubois, L.; Rücker, M.; Schumann, P. Patient Specific Implants (PSI) in reconstruction of orbital floor and wall fractures. J. Cranio-Maxillofac. Surg. 2015, 43, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vehmeijer, M.; van Eijnatten, M.; Liberton, N.; Wolff, J. A novel method of orbital floor reconstruction using virtual planning, 3-dimensional printing, and autologous bone. J. Oral Maxillofac. Surg. 2016, 74, 1608–1612. [Google Scholar] [CrossRef] [PubMed]
- Kronig, S.A.J.; Van Der Mooren, R.J.G.; Strabbing, E.M.; Stam, L.H.M.; Tan, J.A.S.L.; De Jongh, E.; van der Wal, K.G.H.; Paridaens, D.; Koudstaal, M.J. Pure orbital blowout fractures reconstructed with autogenous bone grafts: Functional and aesthetic outcomes. International J. Oral Maxillofac. Surg. 2016, 45, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, I.G.; Lee, J.S.; Oh, D.Y.; Jun, Y.J.; Rhie, J.W.; Shim, J.H.; Moon, S.H. Restoration of the inferomedial orbital strut using a standardized three-dimensional printing implant. J. Anat. 2020, 236, 923–930. [Google Scholar] [CrossRef]
- Teo, L.; Teoh, S.H.; Liu, Y.; Lim, L.; Tan, B.; Schantz, J.T.; Seah, L.L. A novel bioresorbable implant for repair of orbital floor fractures. Orbit 2015, 34, 192–200. [Google Scholar] [CrossRef]
- Parsons, G.S.; Mathog, R.H. Orbital wall and volume relationships. Arch. Otolaryngol. Head Neck Surg. 1988, 114, 743–747. [Google Scholar] [CrossRef]
- Jin, H.R.; Shin, S.O.; Choo, M.J.; Choi, Y.S. Relationship between the extent of fracture and the degree of enophthalmos in isolated blowout fractures of the medial orbital wall. J. Oral Maxillofac. Surg. 2000, 58, 617–620. [Google Scholar] [CrossRef]
- Ploder, O.; Klug, C.; Voracek, M.; Burggasser, G.; Czerny, C. Evaluation of computer-based area and volume measurement from coronal computed tomography scans in isolated blowout fractures of the orbital floor. J. Oral Maxillofac. Surg. 2002, 60, 1267–1272. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, Y.; He, Y.; An, J.; Zwahlen, R.A. Correlation between volume of herniated orbital contents and the amount of enophthalmos in orbital floor and wall fractures. J. Oral Maxillofac. Surg. 2012, 70, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Lee, J.H.; Cho, Y.-S. Analysis of degradation rate for dimensionless surface area of well-interconnected PCL scaffold via in-vitro accelerated degradation experiment. Tissue Eng. Regen. Med. 2014, 11, 446–452. [Google Scholar] [CrossRef]
- Wellisz, T. Clinical experience with the Medpor porous polyethylene implant. Aesthetic Plast. Surg. 1993, 17, 339–344. [Google Scholar] [CrossRef]
- Baek, W.I.; Kim, H.K.; Kim, W.S.; Bae, T.H. Comparison of absorbable mesh plate versus titanium-dynamic mesh plate in reconstruction of blow-out fracture: An analysis of long-term outcomes. Arch. Plast. Surg. 2014, 41, 355–361. [Google Scholar] [CrossRef]
- Hwang, K.; Kim, D.H. Comparison of the supporting strength of a poly-L-lactic acid sheet and porous polyethylene (Medpor) for the reconstruction of orbital floor fractures. J Craniofac. Surg. 2010, 21, 847–853. [Google Scholar] [CrossRef]
- Strong, E.B. Orbital fractures: Pathophysiology and implant materials for orbital reconstruction. Facial Plast. Surg. 2014, 30, 509–517. [Google Scholar] [CrossRef]
- Jansen, J.; Dubois, L.; Schreurs, R.; Gooris, P.J.; Maal, T.J.; Beenen, L.F.; Becking, A.G. Should virtual mirroring be used in the preoperative planning of an orbital reconstruction? J. Oral Maxillofac. Surg. 2018, 76, 380–387. [Google Scholar] [CrossRef]
- Karkkainen, M.; Wilkman, T.; Mesimaki, K.; Snall, J. Primary reconstruction of orbital fractures using patient-specific titanium milled implants: The Helsinki protocol. Br. J. Oral Maxillofac. Surg. 2018, 56, 791–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | p Value | |
|---|---|---|---|
| Age, year | 34.1 ± 16.5 | 34.6 ± 17.3 | 0.926 |
| Sex | 0.433 | ||
| Male | 13/16 (81.3%) | 10/16 (62.5%) | |
| Female | 3/16 (18.8%) | 6/16 (37.5%) | |
| Lesion side | 0.716 | ||
| Rt. | 5/16 (31.3%) | 7/16 (43.8%) | |
| Lt. | 11/16 (68.8%) | 9/16 (56.3%) | |
| Cause | 0.399 | ||
| Fall down | 5/16 (31.3%) | 2/16 (12.5%) | |
| Assault | 9/16 (56.3%) | 9/16 (56.3%) | |
| Accidental bump | 2/16 (12.5%) | 4/16 (25.0%) | |
| Traffic accident | 0/16 (0.0%) | 1/16 (6.3%) | |
| Operation delay, day | 7.6 ± 3.1 | 7.9 ± 2.9 | 0.773 |
| Interval of CT, day | 69.6 ± 49.0 | 69.5 ± 48.9 | 0.994 |
| OPD F/U, month | 5.1 ± 3.3 | 5.4 ± 5.5 | 0.881 |
| Pre-operative symptoms | >0.999 | ||
| Diplopia | 2/16 (12.5%) | 2/16 (12.5%) | |
| Discomfort | 3/16 (18.8%) | 2/16 (12.5%) | |
| Exophthalmos | 0/16 (0%) | 0/16 (0%) | |
| Post-operative symptoms | >0.999 | ||
| Diplopia | 1/16 (6.3%) | 1/16 (6.3%) | |
| Discomfort | 0/16 (0%) | 0/16 (0%) | |
| Exophthalmos | 0/16 (0%) | 0/16 (0%) |
| Volume (cm3) | Group A | Group B | p-Value |
|---|---|---|---|
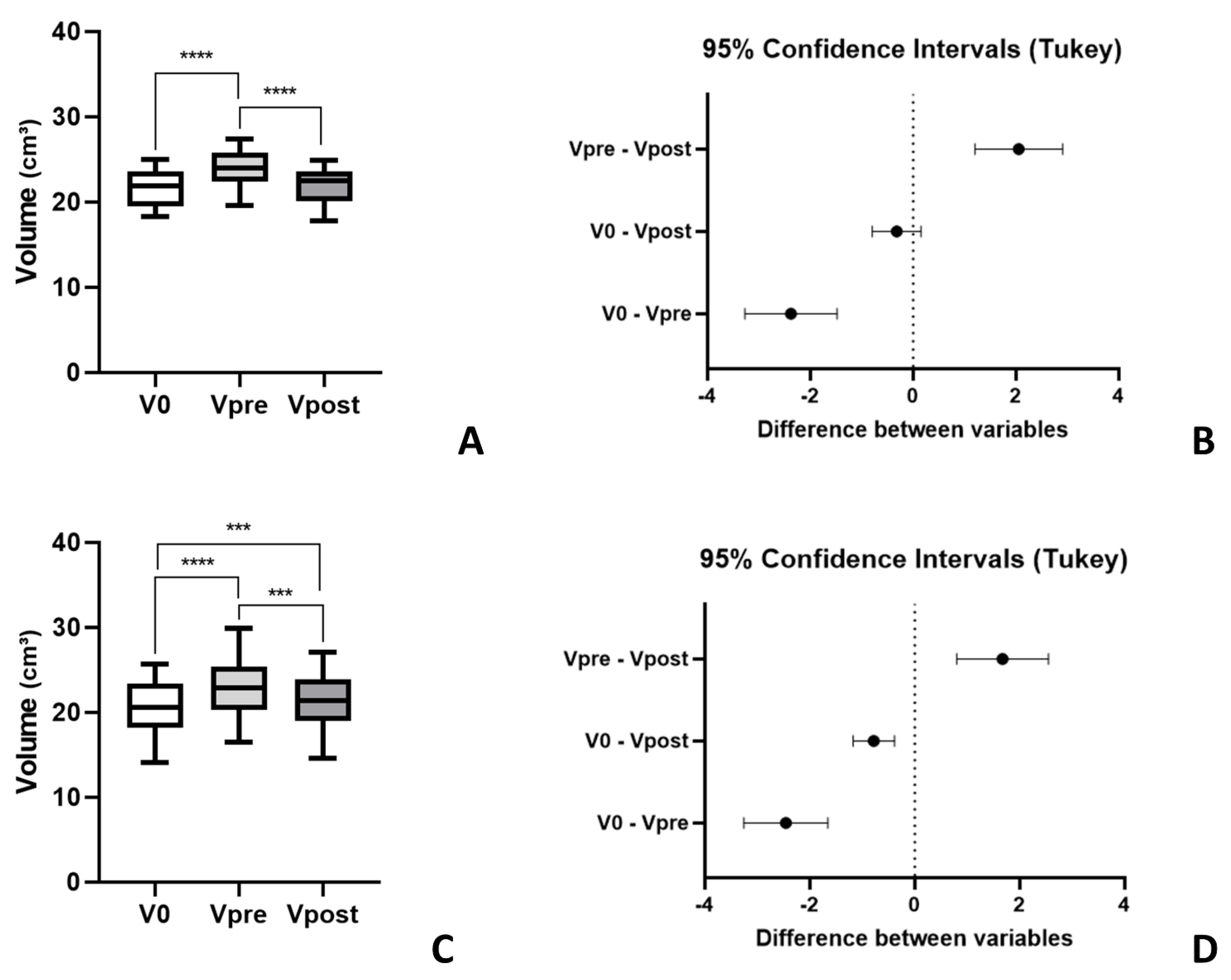
| V0 | 21.6 ± 2.2 | 20.6 ± 3.1 | 0.336 |
| Vpre | 23.9 ± 2.1 | 23.1 ± 3.6 | 0.420 |
| Vpost | 21.9 ± 2.1 | 21.4 ± 3.2 | 0.628 |
| Comparisons | p-Value |
|---|---|
| Group A | |
| V0 vs. Vpre | <0.0001 **** |
| V0 vs. Vpost | 0.2219 |
| Vpre vs. Vpost | <0.0001 **** |
| Group B | |
| V0 vs. Vpre | <0.0001 **** |
| V0 vs. Vpost | 0.0003 *** |
| Vpre vs. Vpost | 0.0004 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Lee, C.R.; Oh, D.Y.; Jun, Y.-J.; Moon, S.-H. Comparison of Efficacy between Three-Dimensional Printing and Manual-Bending Implants for Inferomedial Orbital Fracture: A Retrospective Study. Appl. Sci. 2021, 11, 7971. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177971
Kim JH, Lee CR, Oh DY, Jun Y-J, Moon S-H. Comparison of Efficacy between Three-Dimensional Printing and Manual-Bending Implants for Inferomedial Orbital Fracture: A Retrospective Study. Applied Sciences. 2021; 11(17):7971. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177971
Chicago/Turabian StyleKim, Jun Hyeok, Chae Rim Lee, Deuk Young Oh, Young-Joon Jun, and Suk-Ho Moon. 2021. "Comparison of Efficacy between Three-Dimensional Printing and Manual-Bending Implants for Inferomedial Orbital Fracture: A Retrospective Study" Applied Sciences 11, no. 17: 7971. https://0-doi-org.brum.beds.ac.uk/10.3390/app11177971