
Theoretical Evaluation of Microwave Ablation Applied on Muscle, Fat and Bone: A Numerical Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Matierials
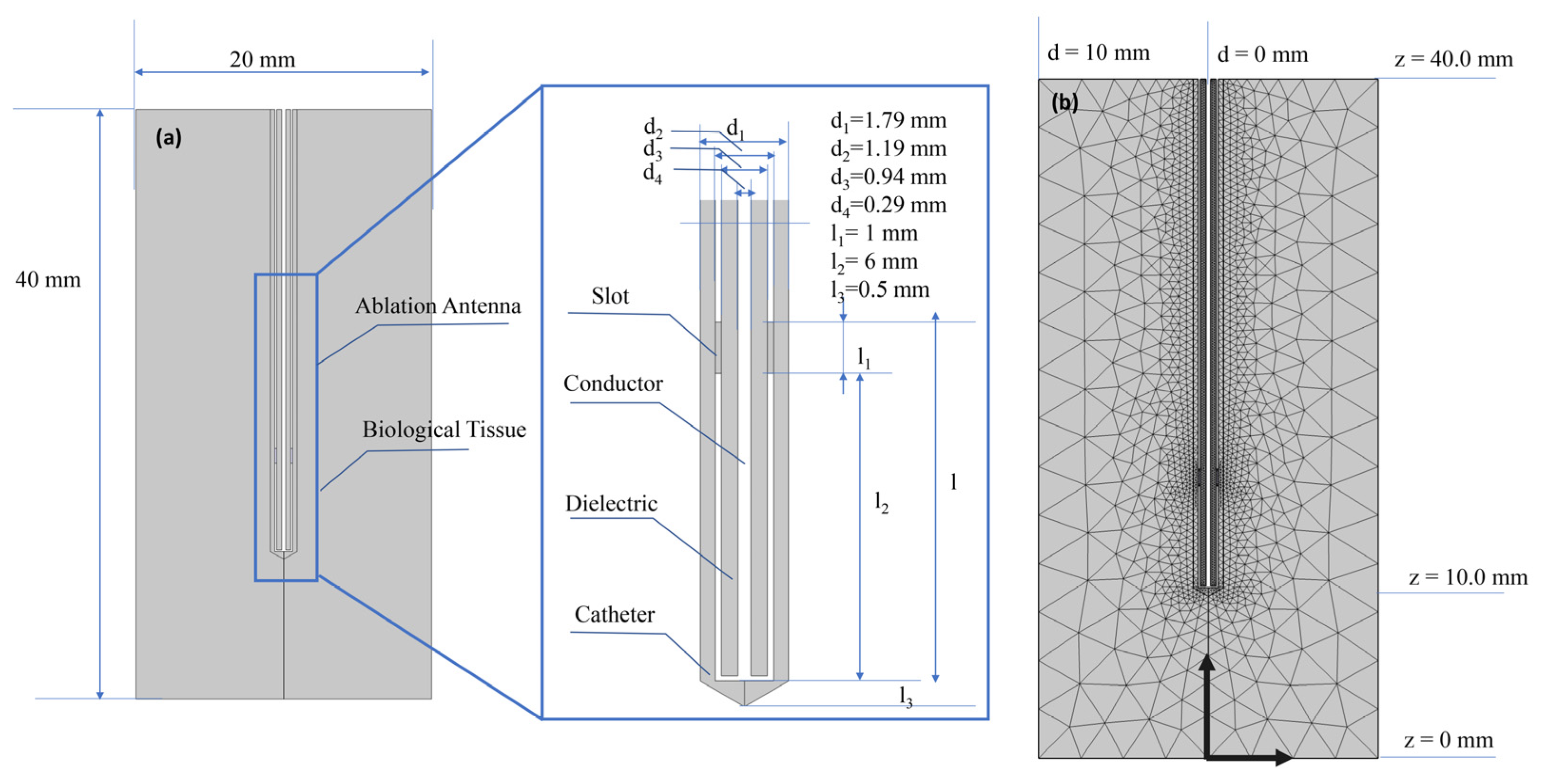
2.2. Numerical Study
2.3. Mathematical Modelling
- It considers the entire tissue to contain a uniform blood perfusion rate and can not reflect local characteristics;
- The fact remains that it is challenging to confirm blood perfusion rate of tissue;
- Numerical simulation of large vessels is affected by blood perfusion rate, so tissue temperature has apparent deviations.
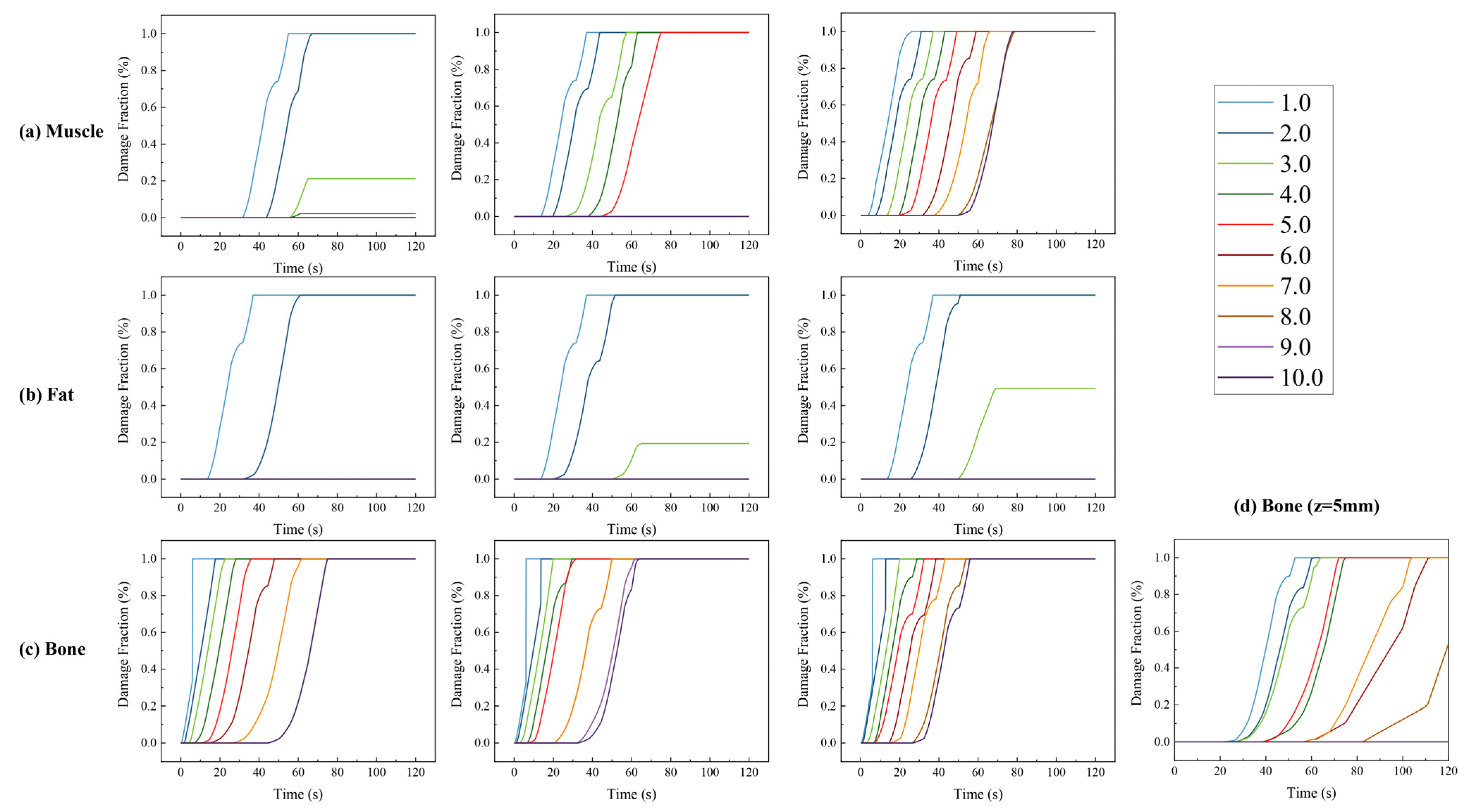
2.4. Heat Damage
- Once tissue temperature exceeds the specific damage temperature , the tissue will be damaged;
- When tissue reaches temperature and damage time exceeds , or tissue temperature exceeds the necrosis temperature , tissue is necrotic.
3. Results
4. Discussion
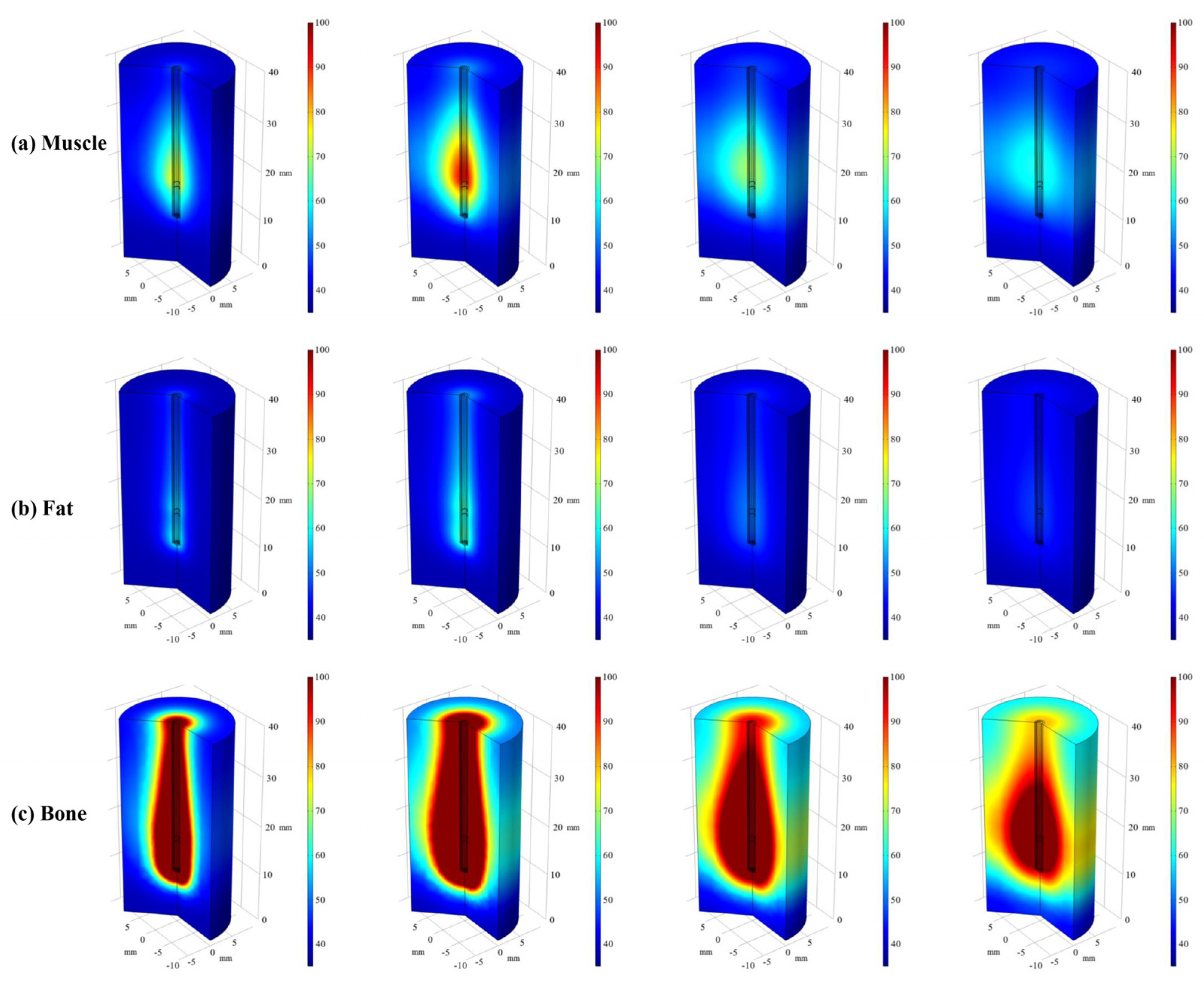
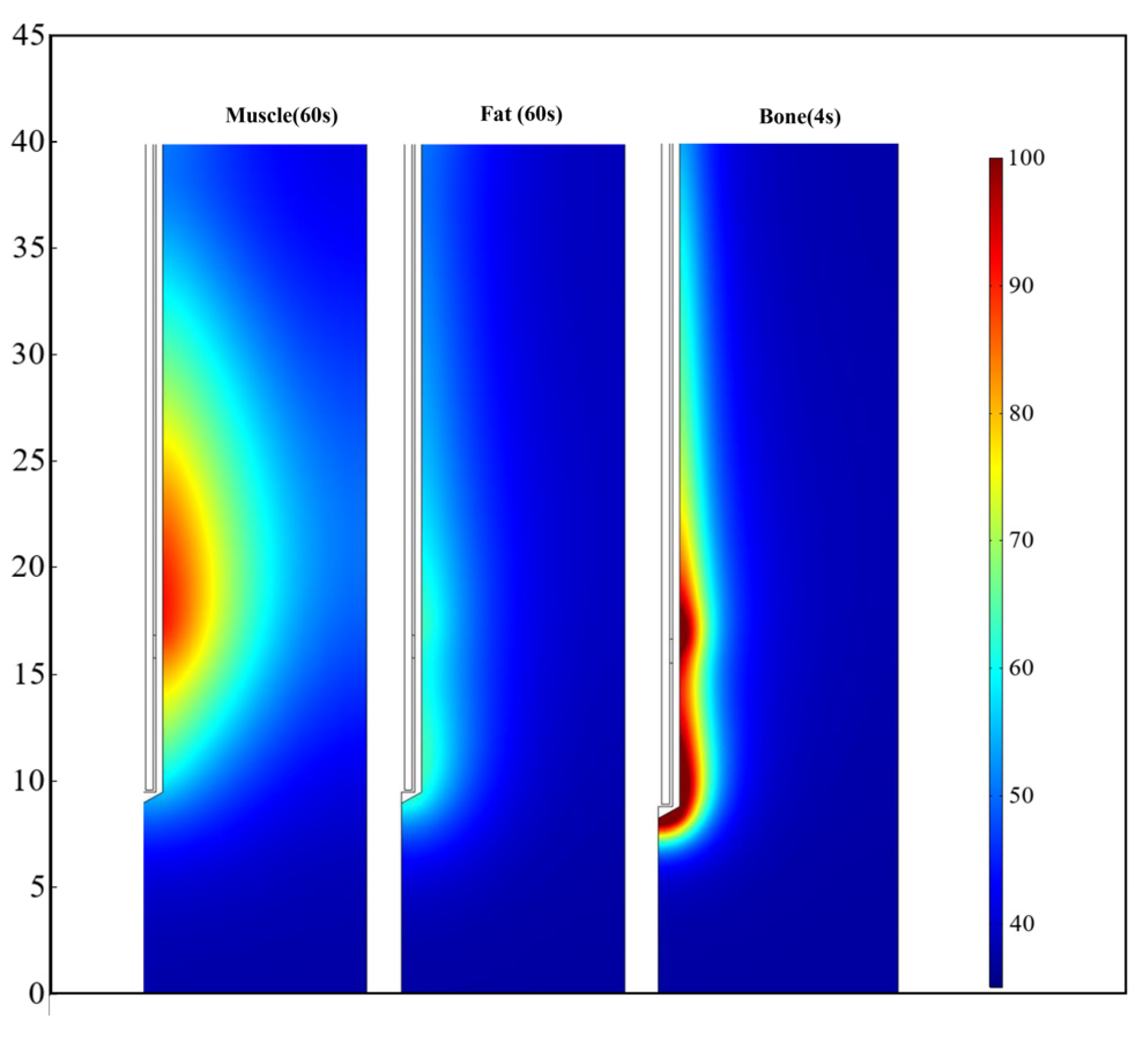
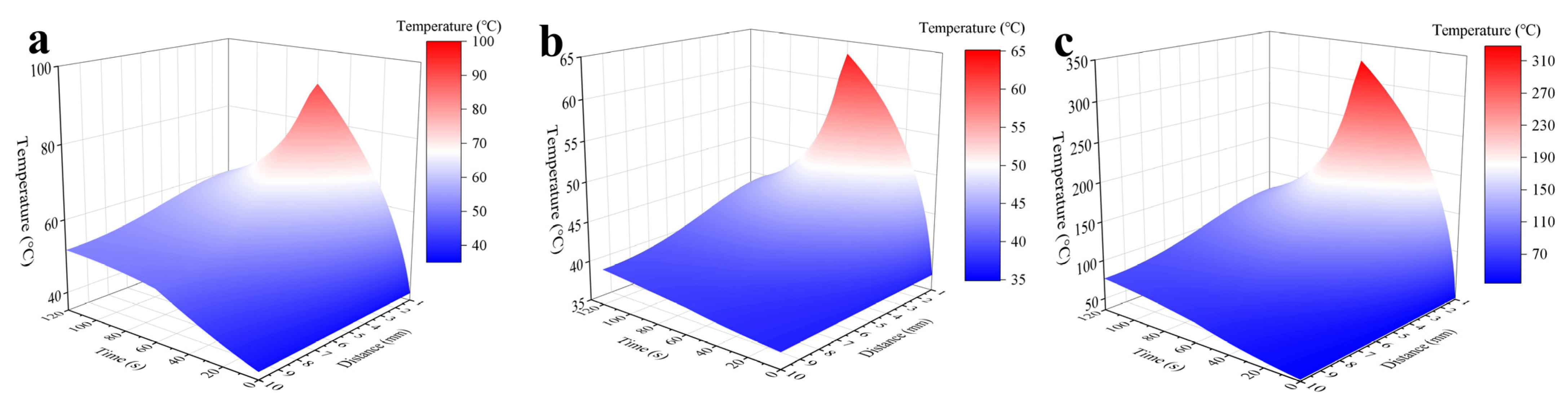
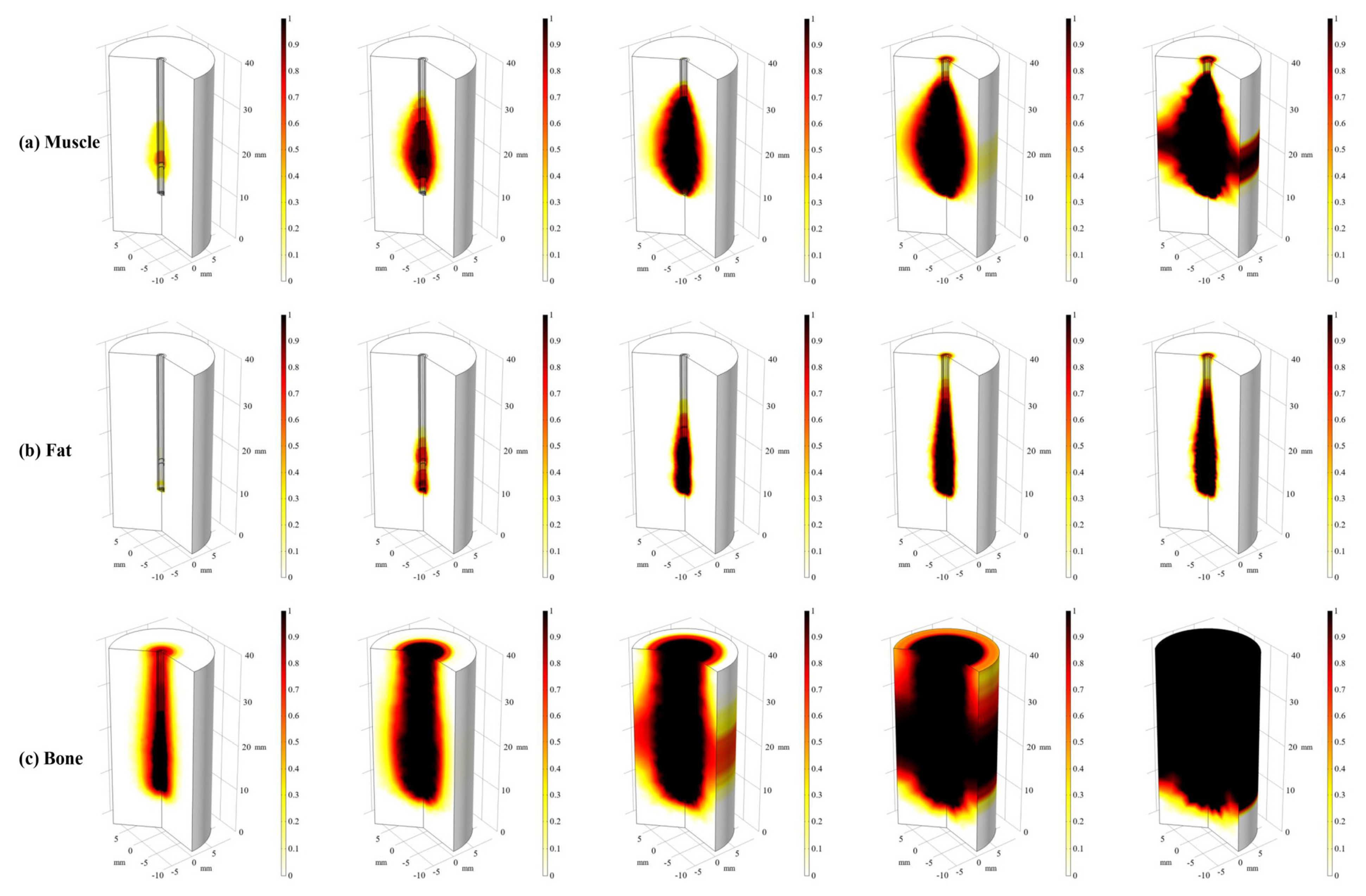
4.1. Visualization of Heat Transfer
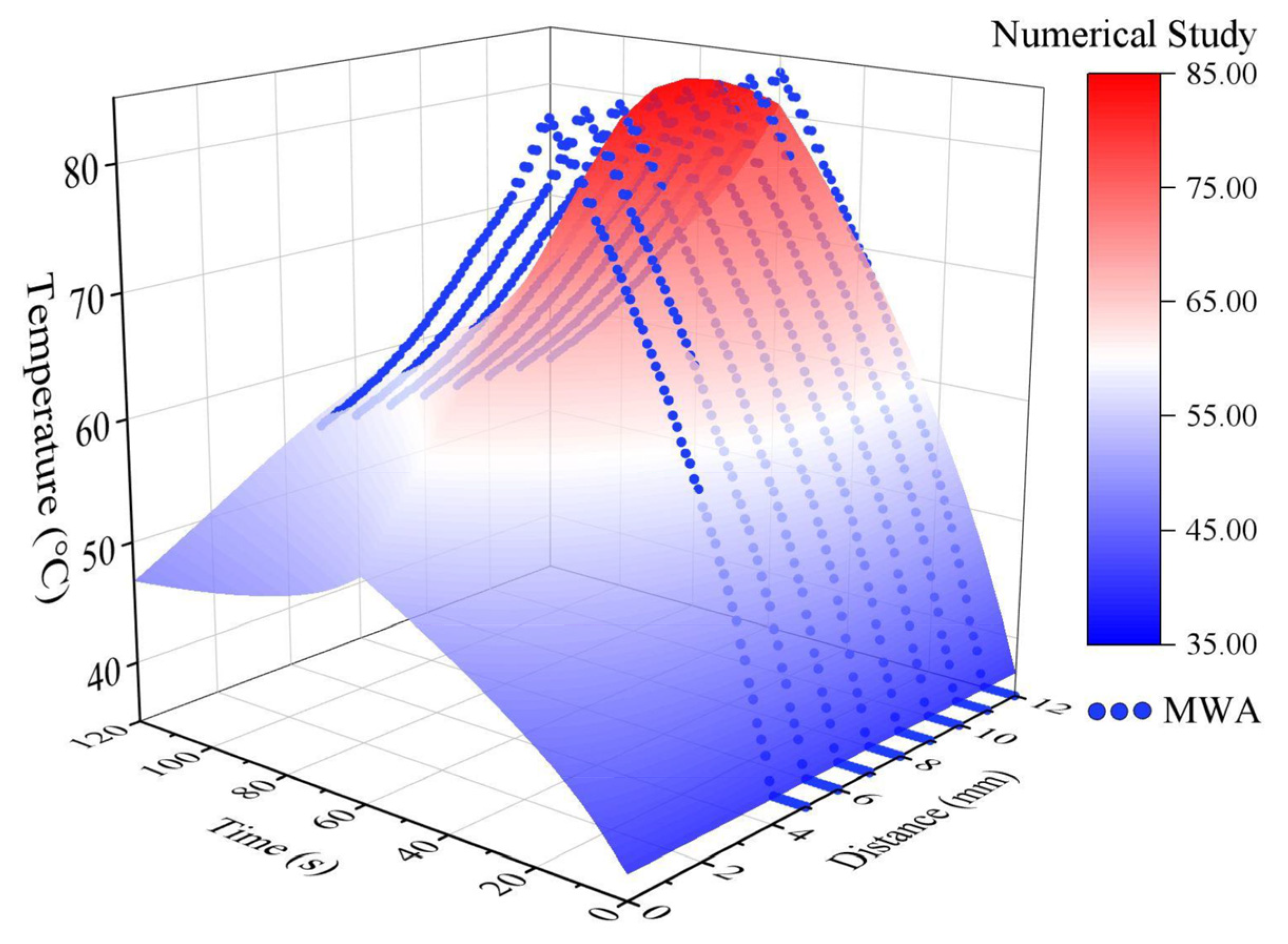
4.2. Quantitative Analysis of Heat Transfer
4.3. Damage Volume Comparison
4.4. Potential Extension and Outlook
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Philip, A.; Gupta, S.; Ahrar, K.; Tam, A.L. A Spectrum of Nerve Injury after Thermal Ablation: A Report of Four Cases and Review of the Literature. Cardiovasc. Interv. Radiol. 2013, 36, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.K. Therapeutic Heating Applications of Radio Frequency Energy. In Biological and Medical Aspects of Electromagnetic Fields, 3rd ed.; Barnes, F.S., Greenebaum, B., Eds.; CRC Press: Boca Raton, FL, USA, 2018; pp. 414–425. [Google Scholar]
- Lopresto, V.; Pinto, R.; Farina, L.; Cavagnaro, M. Treatment planning in microwave thermal ablation: Clinical gaps and recent research advances. Int. J. Hyperth. 2017, 33, 83–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vroomen, L.G.P.H.; Petre, E.N.; Cornelis, F.H.; Solomon, S.B.; Srimathveeravalli, G. Irreversible electroporation and thermal ablation of tumors in the liver, lung, kidney and bone: What are the differences? Diagn. Interv. Imaging 2017, 98, 609–617. [Google Scholar] [CrossRef]
- De Fouw, M.; Oosting, R.M.; Eijkel, B.I.M.; van Altena, P.F.J.; Peters, A.A.W.; Dankelman, J.; Beltman, J.J. Comparison of the tissue interaction between thermal ablation and cryotherapy as treatment for cervical precancerous lesions in an ex-vivo model. Health Technol. 2020, 10, 1275–1281. [Google Scholar] [CrossRef]
- Monfardini, L.; Varano, G.M.; Foà, R.; Della Vigna, P.; Bonomo, G.; Orsi, F. Local Recurrence of Renal Cancer After Surgery: Prime Time for Percutaneous Thermal Ablation? Cardiovasc. Interv. Radiol. 2015, 38, 1542–1547. [Google Scholar] [CrossRef]
- Mauri, G.; Sconfienza, L.M. Is operators’ experience more important than the ablation technique in image-guided thermal ablations? Int. J. Hyperth. 2017, 33, 955–956. [Google Scholar] [CrossRef] [Green Version]
- Hakime, A.; Yevich, S.; Tselikas, L.; Deschamps, F.; Petrover, D.; De Baere, T. Percutaneous Thermal Ablation with Ultrasound Guidance. Fusion Imaging Guidance to Improve Conspicuity of Liver Metastasis. Cardiovasc. Interv. Radiol. 2017, 40, 721–727. [Google Scholar] [CrossRef]
- Abbass, M.A.; Killin, J.K.; Mahalingam, N.; Hooi, F.M.; Barthe, P.G.; Mast, T.D. Real-Time Spatiotemporal Control of High-Intensity Focused Ultrasound Thermal Ablation Using Echo Decorrelation Imaging in ex Vivo Bovine Liver. Ultrasound Med. Biol. 2018, 44, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Chinnaratha, M.A.; Sathananthan, D.; Pateria, P.; Tse, E.; MacQuillan, G.; Mosel, L.; Pathi, R.; Madigan, D.; Wigg, A.J. High local recurrence of early-stage hepatocellular carcinoma after percutaneous thermal ablation in routine clinical practice. Eur. J. Gastroenterol. Hepatol. 2015, 27, 349–354. [Google Scholar] [CrossRef]
- Feng, B.; Liang, P. Local thermal ablation of renal cell carcinoma. Eur. J. Radiol. 2012, 81, 437–440. [Google Scholar] [CrossRef]
- Lopresto, V.; Argentieri, A.; Pinto, R.; Cavagnaro, M. Temperature dependence of thermal properties of ex vivo liver tissue up to ablative temperatures. Phys. Med. Cine Biol. 2019, 64, 105016. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.N.; Jeong, S.; Choi, H.J.; Cho, J.H.; Cheon, Y.K.; Park, S.W.; Kim, Y.S.; Lee, D.H.; Moon, J.H. The safety of newly developed automatic temperature-controlled endobiliary radiofrequency ablation system for malignant biliary strictures: A prospective multicenter study. J. Gastroenterol. Hepatol. 2019, 34, 1454–1459. [Google Scholar] [CrossRef]
- De Vita, E.; Zaltieri, M.; De Tommasi, F.; Massaroni, C.; Faiella, E.; Zobel, B.B.; Iadicicco, A.; Schena, E.; Grasso, R.F.; Campopiano, S. Multipoint Temperature Monitoring of Microwave Thermal Ablation in Bones through Fiber Bragg Grating Sensor Arrays. Sensors 2020, 20, 3200. [Google Scholar] [CrossRef] [PubMed]
- Kadado, A.J.; Akar, J.G.; Hummel, J.R. Luminal esophageal temperature monitoring to reduce esophageal thermal injury during catheter ablation for atrial fibrillation: A review. Trends Cardiovasc. Med. 2019, 29, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.H.; Zou, H.Y.; Qiu, L.; Zhang, X.X. Size effect on the thermal conductivity of octadecanoic acid: A molecular dynamics study. Comput. Mater. Sci. 2019, 158, 14–19. [Google Scholar] [CrossRef]
- Zou, H.Y.; Feng, Y.H.; Qiu, L.; Zhang, X.X. Effect of the loading amount and arrangement of iodine chains on the interfacial thermal transport of carbon nanotubes: A molecular dynamics study. RSC Adv. 2020, 10, 44196–44204. [Google Scholar] [CrossRef]
- Singh, S.; Repaka, R. Effect of different breast density compositions on thermal damage of breast tumor during radiofrequency ablation. Appl. Therm. Eng. 2017, 125, 443–451. [Google Scholar] [CrossRef]
- Wu, X.; Liu, B.L.; Xu, B.K. Theoretical evaluation of high frequency microwave ablation applied in cancer therapy. Appl. Therm. Eng. 2016, 107, 501–507. [Google Scholar] [CrossRef]
- Wang, T.; Zhao, G.; Qiu, B.S. Theoretical evaluation of the treatment effectiveness of a novel coaxial multi-slot antenna for conformal microwave ablation of tumors. Int. J. Heat Mass Transf. 2015, 90, 81–91. [Google Scholar] [CrossRef]
- Pop, M.; Davidson, S.R.H.; Gertner, M.; Jewett, M.A.S.; Sherar, M.D.; Kolios, M.C. A Theoretical Model for RF Ablation of Kidney Tissue and Its Experimental Validation. In Proceedings of the Biomedical Simulation, Berlin/Heidelberg, Germany, 23–24 January 2010; pp. 119–129. [Google Scholar]
- Weinbaum, S.; Jiji, L.M. A new simplified bioheat equation for the effect of blood flow on local average tissue temperature. J. Biomech. Eng. 1985, 107, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Klinger, H.G. Heat transfer in perfused biological tissue—I: General theory. Bull. Math. Biol. 1974, 36, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Khaled, A.R.A.; Vafai, K. The role of porous media in modeling flow and heat transfer in biological tissues. Int. J. Heat Mass Transf. 2003, 46, 4989–5003. [Google Scholar] [CrossRef]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef] [PubMed]
- Wulff, W. The Energy Conservation Equation for Living Tissue. IEEE Transa. Biomed. Eng. 1974, BME-21, 494–495. [Google Scholar] [CrossRef]
- Solovchuk, M.A.; Thiriet, M.; Sheu, T.W.H. Computational study of acoustic streaming and heating during acoustic hemostasis. Appl. Therm. Eng. 2017, 124, 1112–1122. [Google Scholar] [CrossRef]
- Askarizadeh, H.; Ahmadikia, H. Analytical study on the transient heating of a two-dimensional skin tissue using parabolic and hyperbolic bioheat transfer equations. Appl. Math. Model. 2015, 39, 3704–3720. [Google Scholar] [CrossRef]
- Huang, H.-W.; Lin, W.-L.; Moros, E.G. A robust power deposition scheme for tumors with large counter-current blood vessels during hyperthermia treatment. Appl. Therm. Eng. 2015, 89, 897–907. [Google Scholar] [CrossRef]
- Abd Wahab, A.; Salim, M.I.M.; Ahamat, M.A.; Abd Manaf, N.; Yunus, J.; Lai, K.W. Thermal distribution analysis of three-dimensional tumor-embedded breast models with different breast density compositions. Med. Biol. Eng. Comput. 2016, 54, 1363–1373. [Google Scholar] [CrossRef]
- Mayrovitz, H.N.; Grammenos, A.; Corbitt, K.; Bartos, S. Age-related changes in male forearm skin-to-fat tissue dielectric constant at 300 MHz. Clin. Physiol. Funct. Imaging 2017, 37, 198–204. [Google Scholar] [CrossRef]
- Brace, C.L. Radiofrequency and microwave ablation of the liver, lung, kidney, and bone: What are the differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.; Namgung, B.; Woo, D.G.; Choi, J.S.; Kim, H.S.; Tack, G.R. Effect of Input Waveform Pattern and Large Blood Vessel Existence on Destruction of Liver Tumor Using Radiofrequency Ablation: Finite Element Analysis. J. Biomech. Eng. 2010, 132, 061003. [Google Scholar] [CrossRef]
- Yarmolenko, P.S.; Moon, E.J.; Landon, C.; Manzoor, A.; Hochman, D.W.; Viglianti, B.L.; Dewhirst, M.W. Thresholds for thermal damage to normal tissues: An update. Int. J. Hyperth. 2011, 27, 320–343. [Google Scholar] [CrossRef]
- Douplik, A.; Saiko, G.; Schelkanova, I.; Tuchin, V.V. 3—The response of tissue to laser light. In Lasers for Medical Applications; Jelínková, H., Ed.; Woodhead Publishing: Cambridge, UK, 2013; pp. 47–109. [Google Scholar]
- Nagarajan, V.K.; Ward, J.M.; Yu, B. Association of Liver Tissue Optical Properties and Thermal Damage. Lasers Surg. Med. 2020, 52, 779–787. [Google Scholar] [CrossRef]
- Sarkar, D.; Haji-Sheikh, A.; Jain, A. Temperature distribution in multi-layer skin tissue in presence of a tumor. Int. J. Heat Mass Transf. 2015, 91, 602–610. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Unit | Muscle | Fat | Bone |
|---|---|---|---|---|
| Conductivity | S/m | 0.439 | 0.0254 | 0.394 |
| Dielectric constant | 60.0 | 12.0 | 11.4 | |
| Thermal conductivity | W/mK | 0.49 | 0.21 | 0.32 |
| Constant pressure heat capacity | J/kgK | 3421 | 2348 | 1313 |
| Density | kg/m3 | 1090 | 911 | 1908 |
| Metabolic thermogenesis | W/m3 | 700 | 400 | 0 |
| Blood perfusion rate | 1/s | 0.0008 | 0.0002 | 0.000833 |
| Reference | [18,30] | [18,31] | [32] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.; Yu, M.-A.; Qiu, L.; Chen, H.-Y.; Zhao, Z.-L.; Wu, J.; Peng, L.-L.; Wang, Z.-L.; Xiao, R.-X. Theoretical Evaluation of Microwave Ablation Applied on Muscle, Fat and Bone: A Numerical Study. Appl. Sci. 2021, 11, 8271. https://0-doi-org.brum.beds.ac.uk/10.3390/app11178271
Chen C, Yu M-A, Qiu L, Chen H-Y, Zhao Z-L, Wu J, Peng L-L, Wang Z-L, Xiao R-X. Theoretical Evaluation of Microwave Ablation Applied on Muscle, Fat and Bone: A Numerical Study. Applied Sciences. 2021; 11(17):8271. https://0-doi-org.brum.beds.ac.uk/10.3390/app11178271
Chicago/Turabian StyleChen, Cheng, Ming-An Yu, Lin Qiu, Hong-Yu Chen, Zhen-Long Zhao, Jie Wu, Li-Li Peng, Zhi-Liang Wang, and Ruo-Xiu Xiao. 2021. "Theoretical Evaluation of Microwave Ablation Applied on Muscle, Fat and Bone: A Numerical Study" Applied Sciences 11, no. 17: 8271. https://0-doi-org.brum.beds.ac.uk/10.3390/app11178271