
A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic


1
Technische Universität Berlin, Faculty V Mechanical Engineering and Transport Systems, Institute of Land and Sea Transport, Chair of Naturalistic Driving Observation for Energetic Optimisation and Accident Avoidance, Straße des 17. Juni 135, 10623 Berlin, Germany
2
Department of Whole Vehicle Development, Volkswagen AG, Berliner Ring 2, 38440 Wolfsburg, Germany
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(18), 8556; https://0-doi-org.brum.beds.ac.uk/10.3390/app11188556
Submission received: 30 June 2021
/
Revised: 9 September 2021
/
Accepted: 10 September 2021
/
Published: 15 September 2021
(This article belongs to the Special Issue Epidemiology and Public Health in Applied Sciences)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:The COVID-19 pandemic affected many areas of public life and industry. This also applies to research particularly that relies on scientific studies with test persons. In order to minimize the risk of infection, several aspects of experiment design including the setting might require alteration. An extensive review of the latest research involving the COVID-19 pandemic as a blueprint for dealing with other health situations has been conducted in order to develop a step-by-step approach to plan a study with regard to infection protection. As a result, a generic six-step concept was developed that is applicable for scientific studies in both stationary rooms and vehicles while being adaptable to the respective circumstances. The infection protection measures determined through research were implemented in the individual sub-steps from study planning to execution. They allow a step-by-step approach to prevent infections in scientific studies with different settings during a pandemic and in situations where increased hygiene measures are required.
1. Introduction
Due to the coronavirus disease 19 (COVID-19) pandemic, all areas of daily life are reduced in order protect against infection [1]. This also affects companies and scientific institutions that carry out scientific studies, which include test persons. They either cannot take place or must strictly comply with infection protection measures. Until the cumbersome infection protection measures are unnecessary, scientific research will be negatively impacted by the postponement of a large number of studies. In order to allow such work to continue, a holistic concept considering pandemic characteristics and indicators with various extensive hygiene measures, can enable subject studies to continue without increasing the risk of infection. From planning to conduction, each phase of a study requires specific measures. They must be compiled into a generic step-by-step approach, so that it is applicable to different study settings.
2. Related Works
Previous concepts for conducting subject studies during a pandemic are usually very short, undetailed and only outline some aspects that are necessary for the safe conduct of the studies. A concept of the TU Dresden [2] formulates only rough conditions of participation, hygiene and distance rules. Furthermore, it only mentions the disinfection and ventilation measures.
Aerosols and droplet cores, in contrast to droplets, follow the movement of indoor air. Their movement in enclosed spaces is also dependent on heat sources, ventilation and the movement of persons and objects in the room [3]. Aerosols and droplet cores are able to fully distribute in a room [4], so that infections can occur despite social distancing [5]. The concentration of aerosols and droplet cores in the air depends on a number of factors: the number of people present, their activities and total time in the room as well as the room’s size and ventilation. [6].A study by Kriegel [4] demonstrates that the concentration of infectious particles increases the longer an infected person is in an unventilated room. The number of infectious particles increases significantly more in a smaller room than in a larger room. At the same time, the number of indented particles loaded by viruses increases exponentially. Through ventilation, the concentration of infectious particles can be significantly reduced. Here the air change rate, i.e., the time period in which the room air is exchanged for fresh air [7], plays a role. Even a rate of 2.8 air changes per hour leads to a significantly lower number of infectious particles in the room and decreases further with a higher air change rate. The number of indented particles loaded with viruses also decreases significantly through an increased rate of air change and avoids the exponential growth found in an unventilated room.
Studies in vehicles require special measures. A study by Makoto [8] for simulations of droplet and aerosol spread in a room shows that conversations between two people sitting in close proximity increase the risk of infection. The study also shows that they can’t pick up drops directly from the air if they do not face each other while speaking. Another study by Makoto [9] simulates the distribution of aerosols and droplet cores in the air of an unventilated vehicle. It established that aerosols and droplet cores are distributed almost homogeneously in the entire interior air of the vehicle very quickly. Due to the low interior volume of vehicles, the concentration of aerosols and droplet cores increases faster than indoors, which can lead to an aerogenic infection even after a short exposure.
Due to the geometric properties of the interior of a vehicle, it is usually not possible to maintain a recommended distance of at least 1.5 m between the driver and the passenger [10]. Based on trigonometric calculations, this distance can only be achieved in a diagonal seating arrangement if there are no more than two persons in the vehicle [11]. To prevent viral infections in vehicles, it is recommended to attach partitions that can fully prevent both direct contact and droplet infections while limiting aerogenic infections [12]. Such protective walls can be installed, either as a barrier between the front and rear part of the vehicle, or between the driver and the passenger. A study by Makoto [9] shows the distribution of aerosols and droplet cores in a vehicle three seconds after the driver coughs with a slightly open window on the driver’s side and built-in partition wall. It is clear from this that a partition successfully avoids a homogeneous distribution of the particles, as they remain mostly in the front area of the vehicle. Most aerosols and droplet cores that enter the rear of the vehicle flow with the air below the protective wall. A slightly open window can also allow many particles to escape from the vehicle.
Similar to as in stationary venues, ventilation of the vehicle interior can prevent aerogenic infections [9]. Due to the much lower volume, however, significantly higher air exchange rates can be achieved in vehicles. Depending on the type of ventilation, the volume of the interior, the number of occupants in the vehicle and the speed of the vehicle, the air in the interior of the vehicle can be replaced for fresh air more than 300 times per hour. Three fresh air supply strategies can be used: the fresh machine supply, the opening of the windows or the combination of both methods [13]. In a study by Mathai et al. [13] it is shown, that opening the windows has a positive effect on the air exchange rate which can be further improved by increasing vehicle speed. The more windows are opened, the higher the infection protection. The mechanical supply of fresh air also has a positive effect on the air change rate as shown in a study by Fruin et al. [14]. At a higher setting of the ventilation system, the air exchange rate increases. This principle also applies to stationary vehicles. A study by Knibbs et al. [15] confirms this as the risk of infection decreases with the ventilation system switched on while driving at an increased speed.
In the following section, the results of the literature research are presented for the different phases of a study. Subsequently, the individual concept phases are examined critically in the discussion section while conclusions and potential future work are presented in closing.
3. Results
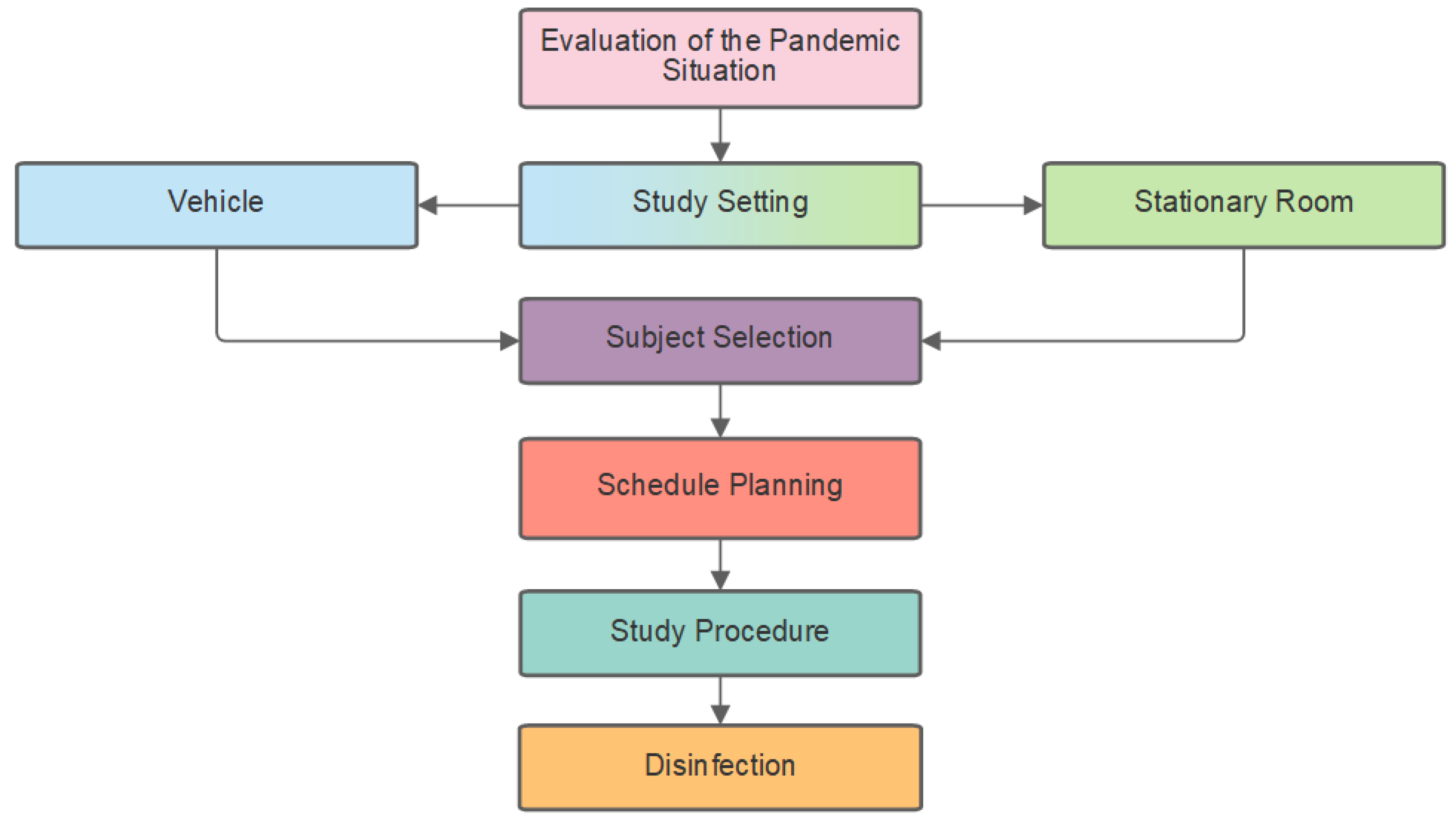
A comprehensive analysis of pandemic research lead to the development of a concept (Figure 1) for conducting subject studies while preventing infections as during the COVID-19 pandemic. Both research on virology and infection prevention before and after the start of the pandemic were considered in order to develop a six-step concept applicable to studies in vehicles and stationary facilities.
The concept includes the relevant steps for planning and conducting a subject study using the example of the COVID-19 pandemic. However, this concept can also be used for other pandemics or situations where comprehensive hygiene measures are required. For the concept we focused on subject studies conducted in stationary rooms and vehicles.
3.1. Evaluation of the Pandemic Situation
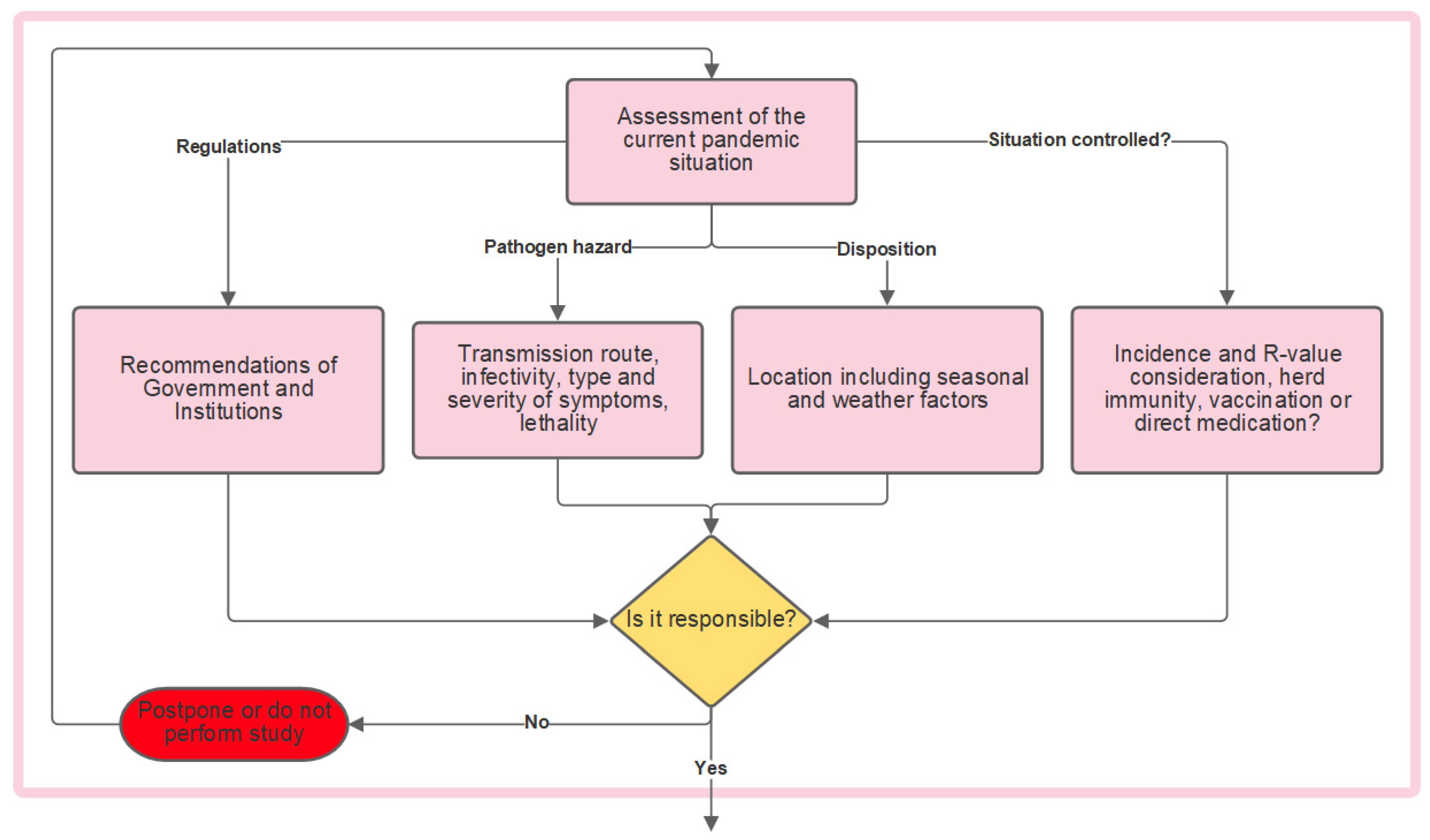
Before a study can be conducted during a pandemic, the current situation including various aspects of the pathogen must first be evaluated in order to decide whether such a study is justifiable (Figure 2).
For this purpose, it is advisable to first consider the recommendations of the responsible authorities and institutions. It is possible that after this step, a postponement of the study is the only responsible course of action. Absent that determination or if only minor measures are officially recommended, an independent qualitative risk evaluation should be conducted.
3.1.1. Pathogen Hazard
When assessing the pandemic situation independently, the pathogen should be considered first. If the pathogen is transmitted via vectors, water or food, the studies should be feasible without any problems, since no infections can be caused by the study. If the pathogen is transmitted via direct or indirect human-to-human contact, infections may occur during the study. Therefore, other factors must be considered. For instance, if a very high viral load is required for infection, meaning an infection is only possible at all after a long exposure time, the study can be adjusted so that the study time is less than the exposure time required for infection. If the pathogen is moderately to highly infectious, the likely course of illness must be considered. If severe health consequences are expected, or if the lethality rate is particularly high, it may not be responsible to conduct the study. In cases where the pathogen is only dangerous for certain types of people, then the risk group can and must be excluded. For the COVID-19 pandemic these would be people aged 50 and over [16] and persons with pre-existing conditions that affect the heart, respiratory system, liver or kidney [17].
3.1.2. Disposition
Dispositions that are particularly conducive to infection must be avoided as some epidemics may be seasonal [18]. Pathogen-specific disposition conditions should be analyzed in order to be able to avoid them accordingly.
3.1.3. Situation Controlled?
Statistical indicators can be used to assess the current and future pandemic situation. The main indicators include incidence, prevalence, lethality, mortality rate and the number of reproductions [19,20].
How and to what extent a disease is treatable should also be considered. If suitable and effective antiviral therapies are available, then conducting studies with test persons can be justifiable, since serious consequences of the disease can be avoided in spite of possible infections. If many people have already been vaccinated against the pathogen or if within the population there is a natural immunity, conduct studies in person can be considered more responsible than at other times during a pandemic.
3.2. Infection Protection Measures—Stationary Test Rooms
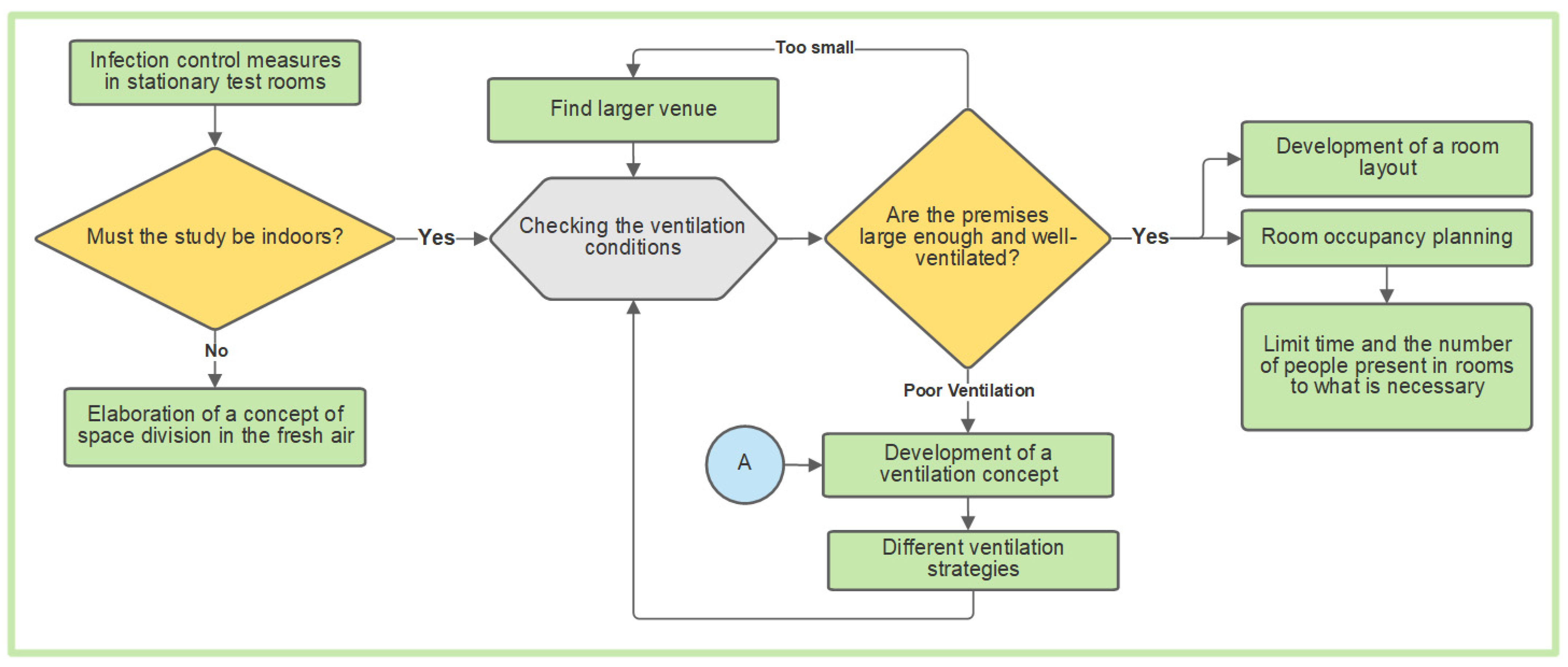
In order to use a stationary indoor facility, appropriate infection protection measures have to be implemented in advance (Figure 3). These include the required hygiene measures and a preliminary examination of the test person. Only after this exam should the subjects enter the actual trial. Respiratory masks [21], Filtering Face Piece 2 (FFP2) or better [5], have to be worn at all times. This ventilation concept applies also to vehicles (Section 3.3).
3.2.1. Stationary Test Rooms—Ventilation Conditions
When planning in-person studies, it must first be clarified whether it must be held indoors. If so, it is imperative to check the ventilation conditions in the rooms. It must be confirmed that six air changes per hour can be achieved in all rooms that are to be used [22] and that the relative humidity between 40% and 60% can be maintained [23]. Additionally, the level of carbon dioxide in the rooms must be monitored. The amount of time until 1000 ppm limit is reached should be tested in advance [3]. The latter test can aid in a room size evaluation [24]. If the critical carbon dioxide concentration is reached too quickly, this may indicate that the rooms are too small. If the required humidity and air exchange rate cannot be maintained, a ventilation concept must be worked out for the rooms. If windows are present, this should take into account shock ventilation. Care must be taken to ensure that the rooms do not cool down, since the temperature difference between the room and the environment will lead to room air escaping through the windows [3]. In order to monitor the air quality as well as the number of aerosols and droplet cores in a room, devices can also be used to measure the carbon dioxide concentration in the room air. For rooms with windows but without a ventilation system, timely regular intervals of ventilation can be calculated in advance [25].
To achieve the required air exchange rates, the use of mechanical ventilation systems is recommended. For this purpose, central ventilation systems can be installed in the rooms. However, the effectiveness of such ventilation systems comes at a high financial cost. If mechanical ventilation systems are used, it must be noted that vertical air movements should be avoided and that displacement ventilation systems are therefore particularly suitable for ventilating stationary rooms [22].
Displacement ventilation is recommended. With this method spring vents are installed near the ground, so that the usually colder fresh air accumulates at the bottom of a room. Aerosols and droplet cores also rise with the convection flow and are sucked out, making aerogenic infections less likely [3].
3.2.2. Stationary Test Rooms—Room Occupancy Planning
If the room size and ventilation is satisfactory, planning occupancy and layout must serve to maintain safe distances of at least 1.5 m [24,26] and avoid crowding in the room. The goal of planning the room layout should be to minimize the number of people in the room while factoring in the time present. This can be carried out in advance through scheduling [27].
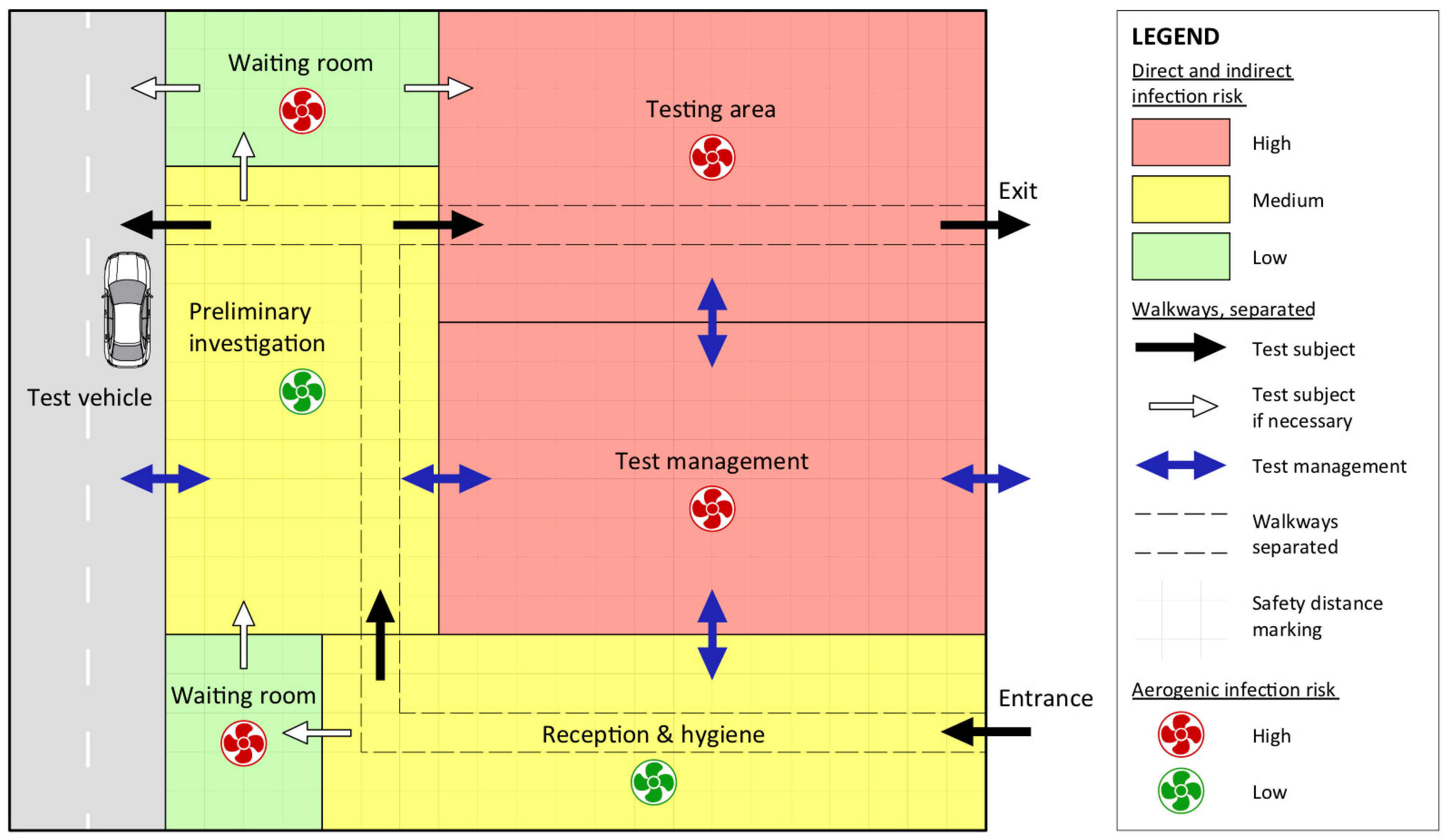
The first step of planning the room layout is a hygienic cleaning and a preliminary examination. Waiting areas for test subjects as well as break areas for the test administration are required. If the actual study takes place in a simulator, the experimental room must be separate. The walking paths and directions of the test subjects must be clearly marked. In order to limit encounters, the testing rooms should have separate entrances and exits. Similarly, the walking paths to and from the rooms should be separated. This ensures that safe distances are maintained even in narrow corridors. An ideal room layout is shown in Figure 4. It includes a room for reception with hygienic measures, a room for the preliminary examination, as well as a break room for the administration and a test room.
The walking routes of the subjects are shown with black and white arrows, while the walking routes of the test administration are marked with blue arrows. Since the investigators have to enter each room, their entry and exit is not restricted. The subjects, however, can only move from entrance to exit in the direction shown. In addition, Figure 4 shows the relative risk of infection by the color of the room. The waiting rooms have a low risk (green) of direct or indirect contact or droplet infection, since only one volunteer can be in the waiting room at a given time. Rooms colored yellow have a medium risk of infection, as two people are present in these rooms at the same time. Red rooms, such as the experimental room and the management’s common area, have a high risk of infection, since at least two people are present in these rooms for a longer time. In the rooms marked in yellow and red, it is therefore particularly important to pay attention to the basic infection protection measures (e.g., safe distance, respiratory mask, hygiene).
Additionally, a green or red rotor symbol represents the risk of aerogenic infection. A green rotor symbol, as seen in the reception or hygiene rooms, denotes a low risk of infection due to aerosol exposure. These rooms as well as the pre-examination room, are only used for short time periods. In all other rooms, a high risk of aerogenic infections is symbolized by the red rotor, as several people may be present in these rooms for longer periods of time. While waiting rooms are occupied by only one person at a time, they are assumed to be small with a typically longer duration. In these rooms, the air conditions must be closely monitored.
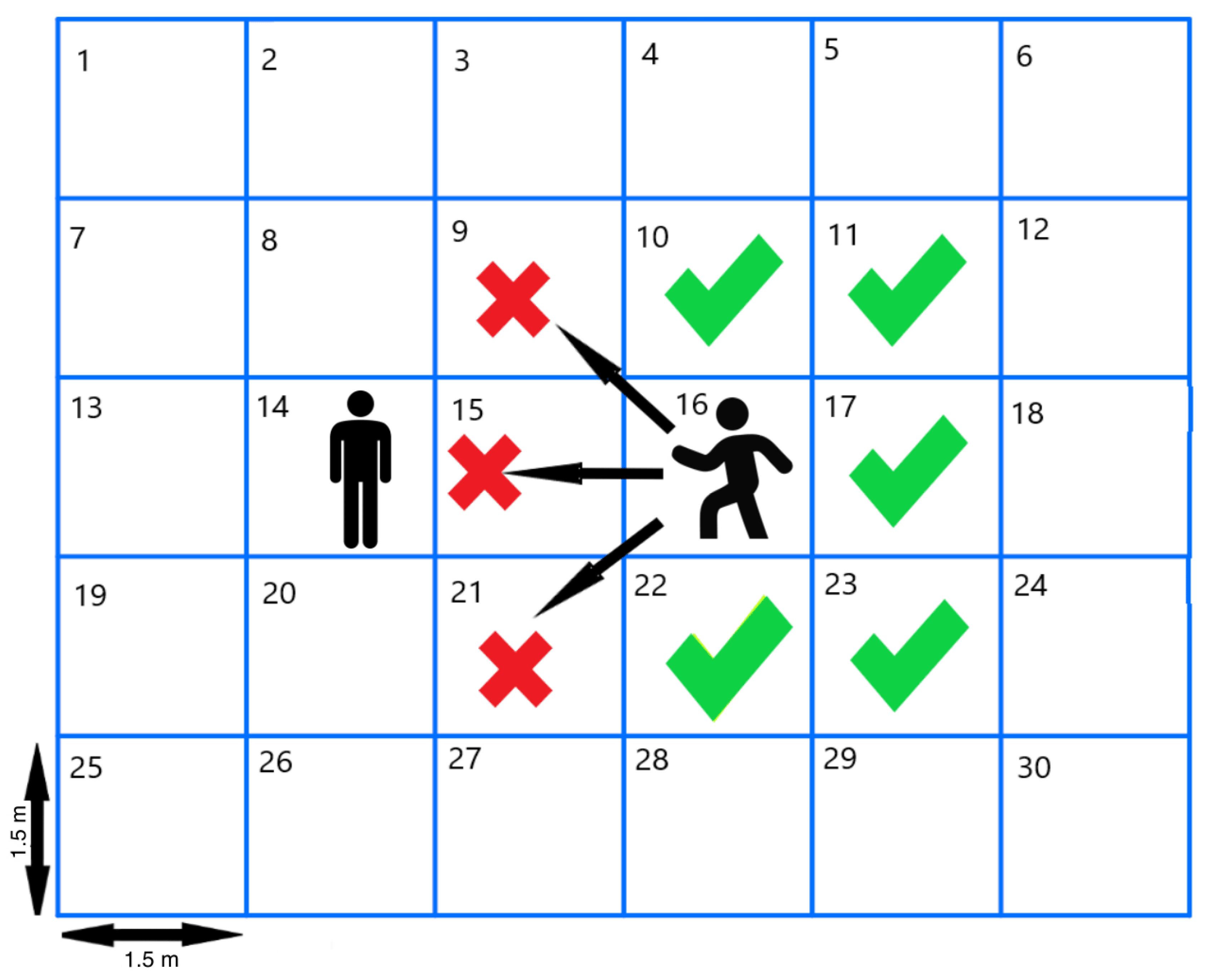
In order to maintain safe distances in stationary rooms, markings can be placed on the floor, which are at least 1.5 m apart. If the entire floor of the room is divided into a grid, the people in a room can easily maintain the required distance. No more than one person stands in a square measuring 1.5 m × 1.5 m, and the adjacent square is kept empty to maintain a distance between the two individuals. This is illustrated in Figure 5, where two people occupy a room divided into 30 sections.
One person stands in section 14, the other in 16. Since section 15 is located between them, it can be seen at first glance that the necessary safe distance is maintained. When one person is stationary, then no one else may enter the sections 21, 25 or 9. However, if someone moves into these squares, the other person must move back. In order for the person on the right to enter Section 15, the person on the left would have to have moved to 13 beforehand.
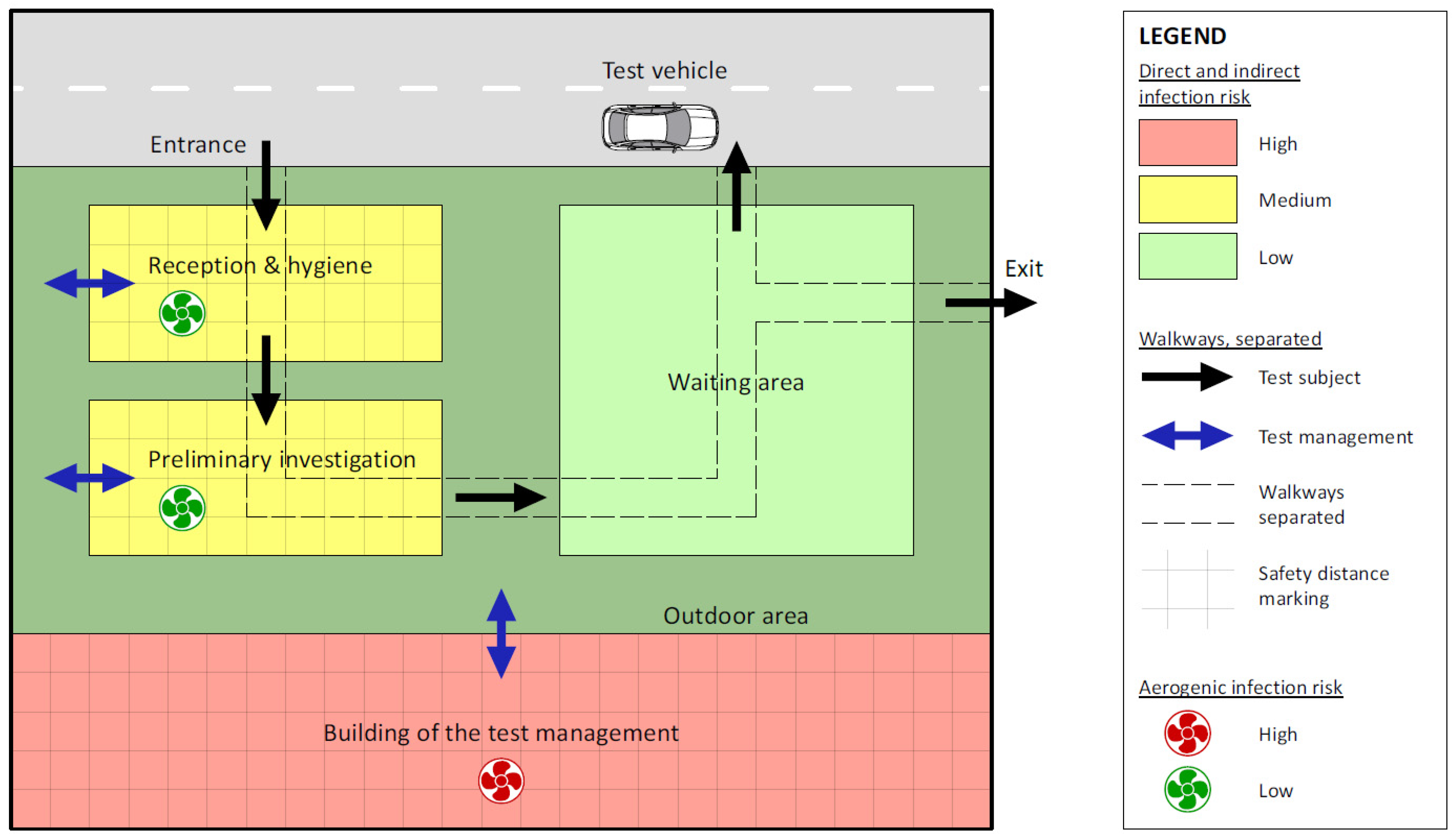
If not absolutely necessary to enter the test rooms, hygienic measures and the preliminary examination should take place outdoors. This eliminates the possibility of aerogenic infections passing between the test administration and the test subjects. In order to conduct these first activities outdoors, an area allocation concept including the use of triage or fixed tents needs to be developed. The walking routes of the subjects as well as the individual stations must be clearly marked and distinguishable, so that they always remain in designated areas. Furthermore, clearly marked entrances and exits must be provided. Such a concept is shown in Figure 6.
Just as in Figure 4, the infection risks are also estimated. In the tents for reception, hygiene and preliminary examinations, a medium risk of infection via direct and indirect contact as well as droplets is to be expected, since two persons must interact in these rooms despite all infection protection measures. In the waiting area, there is a low risk of infection because no other person is present at the same time as the test person. Aerogenic infections can also be ruled out in the waiting area, since all aerosols emitted by the subjects escape directly into the environment. In the triage tents aerogenic infections cannot be completely excluded, but such kind of infections are not to be expected here, as they can be well prevented with air purification devices. In addition, large amounts of fresh air can enter the triage tents from outside due to wind, if the tent structure allows air exchange or one side of the tent is raised for a short time. A high risk of infection is expected within the building of the test management, since at least two people of the staff could be present in these rooms for a longer time.
3.3. Infection Protection Measures—Vehicle
In order to carry out a test subject study in a vehicle, special aspects must be taken into account, which are shown in Figure 7. In particular, the vehicle as a comparatively small room and ventilation conditions play a decisive role in comparison to stationary test rooms. It is necessary that both occupants wear a respirator mask during the entire test. The respirators worn should be at least FFP2 standard, so that both self-protection and protection from others are ensured. If it is not possible for the person driving to wear a respirator due to the study conditions, special care must be taken to ensure that as little as possible is spoken during the test in order to minimize the number of aerosols and droplets emitted and that the mentioned partition wall is installed.
3.3.1. Vehicle Occupancy
In order to determine the requirement for infection control measures in the study vehicle, it must first be clarified whether a person conducting the test must be present in the vehicle in addition to the test subjects. If the test subjects can be monitored by cameras or if only the acquisition of sensory data is important, which can also be evaluated after the execution of the individual driving tests and therefore, no supervisor must be present in the vehicle during the test and no infection control measures are required during the execution of the actual test. To prevent indirect contact infections and aerogenic infections afterwards between the test subjects, disinfection is required and the vehicle must be aired out.
If a supervisor must be present in the vehicle during the test drive, then a number of infection control measures are required. First of all, the safety distance to the driver-subject must be maintained. Therefore, the supervisor should sit in the right rear seat. Only one subject is allowed in the car at a time, otherwise the safe distances will be inadequate. Furthermore, a transparent partition must be installed between the supervisor and the subject. Depending on the study setting, this would either separate the front and the rear seats or the driver and passenger seats.
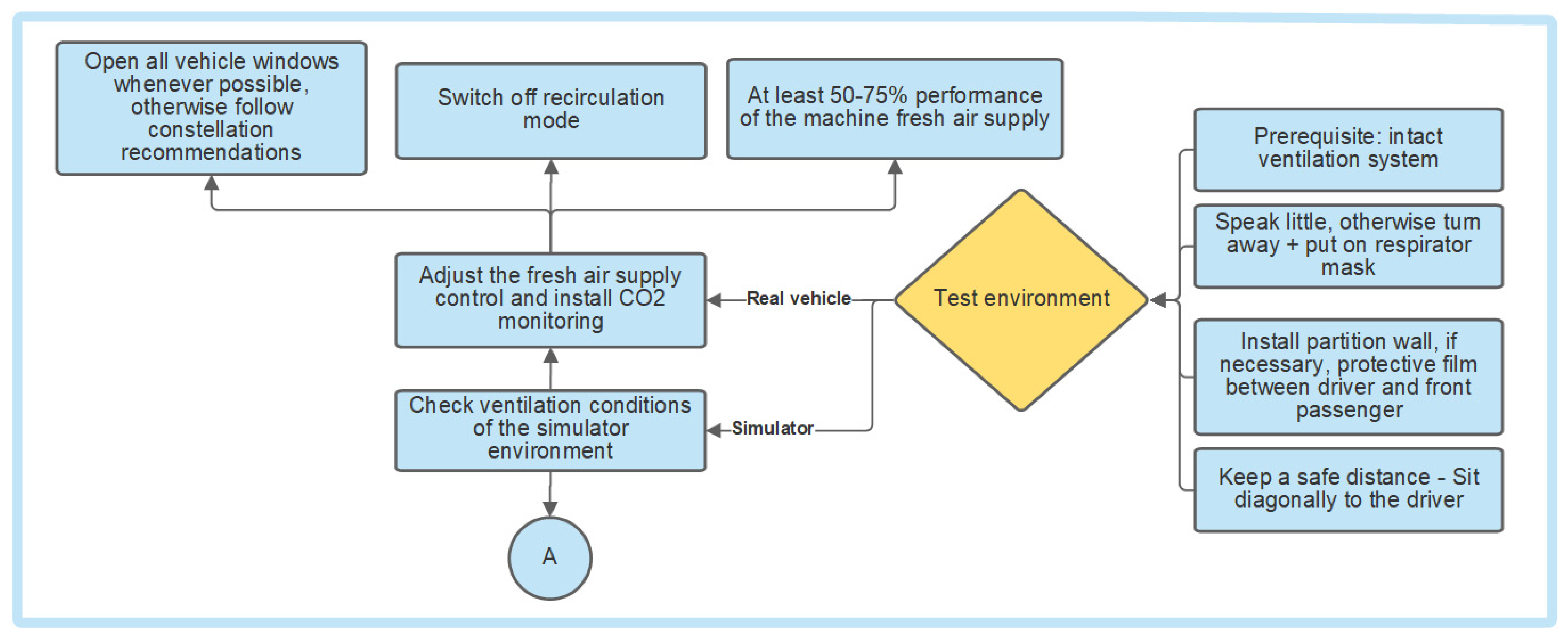
3.3.2. Ventilation in a Vehicle
The test vehicle requires a working ventilation system. Here a distinction must be made between tests in real vehicles and simulators. While unlimited fresh air is available in real vehicle studies, the simulator will depend on the ventilation conditions in the room where it is located. If the study is carried out in a real vehicle, the fresh air supply must be set correctly before the start of the test. The recirculation mode of the ventilation system cannot be used. If possible, at least 50% of the maximum output of the vehicle’s mechanical fresh air supply should be used, so that at least 60 air changes per hour take place. While in motion, all vehicle windows are to be open whenever possible in order to maximize air exchange rates in the vehicle. Opening the windows is particularly recommended at speeds above 10 m/s. A carbon dioxide monitor should also be installed in the vehicle. If this rises above 1000 ppm during the test, it is imperative to increase the output of the mechanical fresh air supply or to open more windows.
If the study is carried out with the help of a simulator, a ventilation concept according to the example for stationary rooms should be employed. If a ventilation system is present in the simulator, 50–75% of the maximum output is necessary just as in the real vehicle. This serves to protect against aerogenic infections in the simulator. With the help of additional ventilation in the simulator, potentially contaminated air is released into the air, where it is removed or cleaned. Additionally, air must move between the simulator and the room. Otherwise, no fresh air will enter the simulator, causing the risk of infection to increase rapidly over time. Even though this is only of concern if more than one person is in the simulator.
3.4. Subject Selection
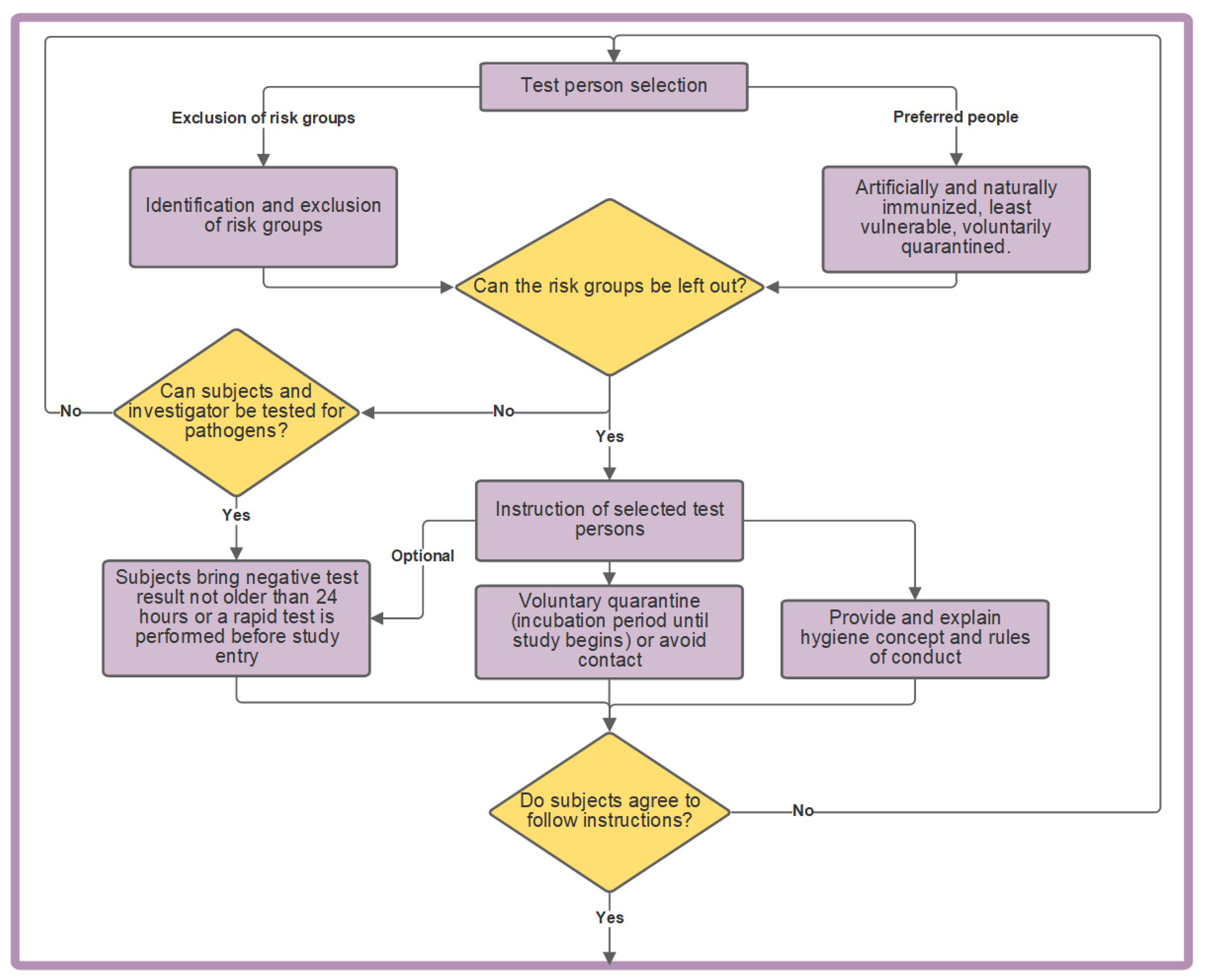
Most importantly, at-risk individuals are not invited to the study (Figure 8). The risk group classification should be used. For the COVID-19 pandemic, elderly and previously ill people would be excluded from the study. Furthermore, people working in health care or who have direct contact with patients or risk groups for other reasons, should also be excluded from the study, as they are at an increased risk of being infected or infecting people in the risk groups. People who live in or have recently traveled to a high-risk region should also be excluded. Preference therefore should be given to individuals expected to have a less severe course of disease following infection with the pathogen. Immunized individuals, with proof in the form of a certificate or antibody testing should also be targeted for the study. Those individuals who are willing to quarantine voluntarily in advance of the study and for the maximum incubation period of the pathogen, may also be given priority for invitation to the study.
Furthermore, it must be decided whether the study can be conducted without the individuals who need to be excluded, as this may make it impossible to have a representative cross-section of a population. If all persons on site can show a negative test result, infections most likely can be excluded. As for the Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV-2) [28], either a Polymerase Chain Reaction (PCR) laboratory test or a PCR rapid test administered at the study site would have to be performed prior to starting the study. A PCR laboratory test is preferred, as PCR rapid tests or self-tests are less accurate [29]. With a positive or unclear result, the tested person is not allowed to participate in the study.
Members of risk groups can participate in the study if and only if every person involved in the study can be tested for the pathogen. If it is not possible to test all persons involved for the pathogen, then the risk group members cannot participate. Therefore, the study must be postponed. If members of risk groups are excluded from participation, then testing for subjects and investigators can be optional. Nevertheless, it is recommended to test all subjects for the pathogen, since this benefits the study overall as infections can almost be eliminated.
3.5. Conducting the Study
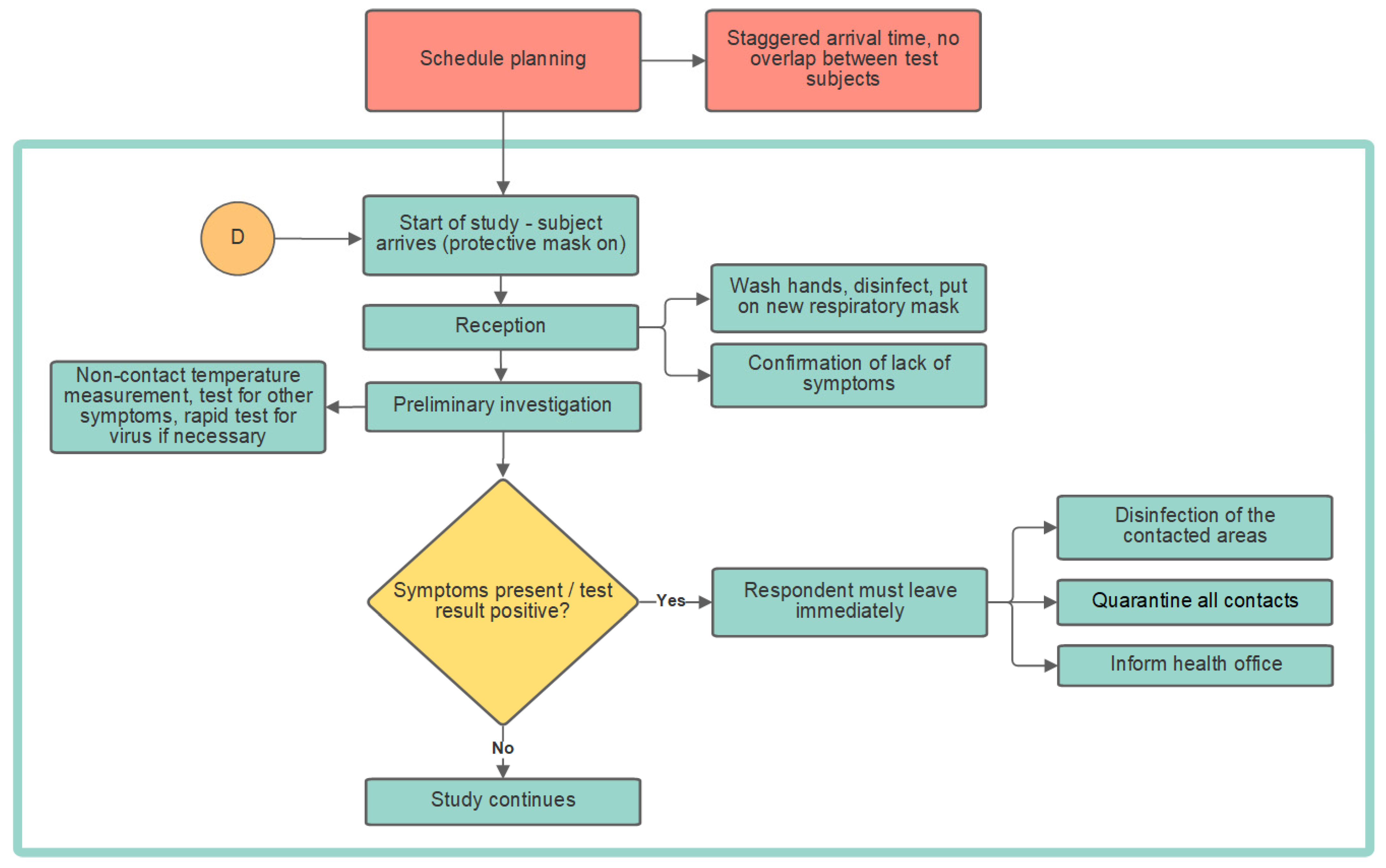
The following chapter consists of the schedule and study procedure (Figure 9). The scheduling takes place before the actual start of the study and ensures an organized test process. The conduction of the study is divided into the subjects of reception, preliminary examination and the actual study. Reception and preliminary examination are necessary in order not to allow infected subjects to enter the study and to implement and communicate initial hygiene measures.
3.5.1. Planning of Test Times
The planning of the individual test times must be carried out in advance (Figure 9). The goal should be that only one test subject arrives at a given time. Therefore, the duration of the test subject’s visit (from reception to discharge) should be determined through a dry run. On the basis of this time, individual subjects can then be assigned appointments for arrival, with which subject overlap is avoided. In effect, the arrival of a subject is always scheduled after the previous participant has left the premises.
3.5.2. Reception
The test subjects must first sign a declaration that they are symptom-free. This is intended to prevent someone with pathogen-specific symptoms from participating in the study, but at a minimum, it serves as a legal safeguard for the trial management. Subsequently, the subject will be given a new mask that meets at least the FFP2 standard. The subject must wear the mask to ensure the best possible protection for themselves and others during the study. Test subjects should be forbidden from using their own masks, as these may not meet the required standard or may have been worn for too long. It is important that the mask becomes put on only after the subject has washed and disinfected their hands. For this purpose, the subject must be instructed on the correct hand washing and disinfection procedures. The test administration must ensure a sufficient safe distance from the subject at all times.
3.5.3. Preliminary Investigation
The preliminary examination involves being checked for infection-specific symptoms. During the COVID-19 pandemic, for example, the body temperature of the volunteers should be measured, as fever is a common symptom of COVID-19 [16]. This is best carried out in a non-contact manner using infrared thermometers. COVID-19 affects the sense of smell, a loss of which can be ascertained through a smell test.
If the participant is symptom-free, a rapid test (if applicable) for the virus is carried out at this point. Until the test result is available, the patient must go to the waiting area. If the test result is positive or if the test person exhibits symptoms specific to the infection, the health department must be informed immediately of the possible infection. In addition, all persons who have had contact with this subject must be quarantined. The reception, hygiene station, waiting areas and the pre-examination room must all be completely disinfected afterwards. If the test result is negative and no infection-specific symptoms are present, the actual study can begin.
3.5.4. During the Experiment
After a successful preliminary examination, the subjects move on to the vehicle or room for the study. If this requires the subjects to wear equipment, such as eye tracking glasses, the investigator must explain to the subjects how to put on the equipment themselves, since the administration cannot do this for them while maintaining a safe distance. The test persons must first enter the vehicle or the simulator with the mask on. If the study must be accomplished maskless, it should only be removed immediately before the start of the test. Furthermore, the ventilation settings should not be adjustable so that suboptimal conditions are avoided. When the vehicle is safely parked and the test complete, the subject must immediately put the mask back on. The same applies for studies in a simulator. Both the equipment and the vehicle must be disinfected afterwards so that the next person can use them safely.
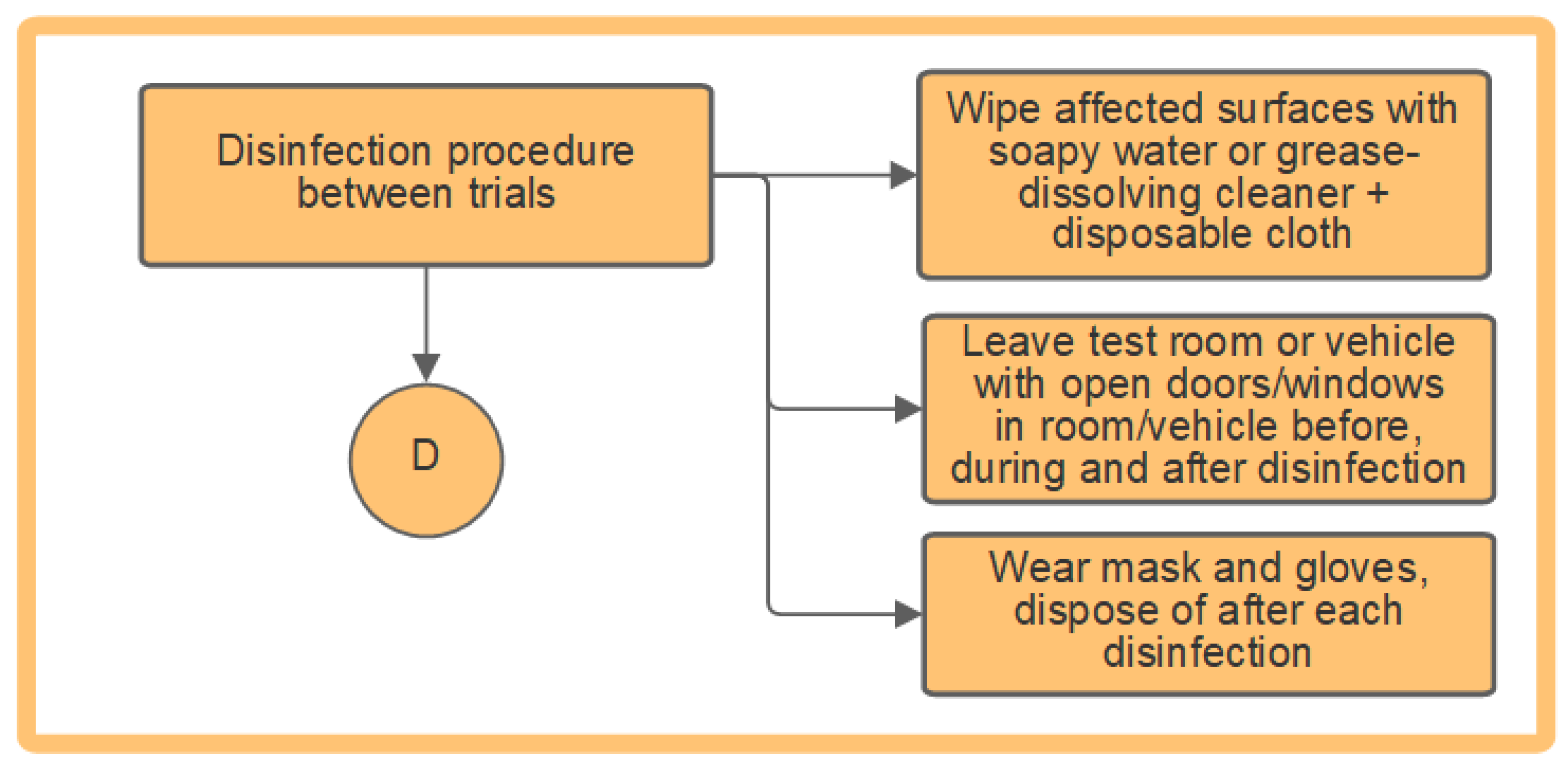
3.6. Disinfection
When disinfecting the stationary room or the study vehicle (Figure 10), all affected surfaces must be treated with a disposable wipe soaked in degreasing cleaner or soapy water. The wipe must not be reused. Before starting the disinfection, the room or vehicle should be ventilated for 10 min by opening all doors and windows. The person performing the disinfection must wear a mask and disposable gloves during the entire disinfection process. The gloves must be disposed of after the disinfection process.
The entire procedure must be performed after each trial in order to reduce the risk of infection for the subsequent subject.
4. Discussion
If studies are conducted indoors, the room-specific conditions must be observed. The concept shows how to reduce the risk of infection, but it must be adapted to the available space. In particular, ventilation conditions are crucial as infection can occur despite social distancing indoors [5]. Fans and suction systems that move air laterally should not be used, as this can actually increase the risk of infection via aerosols and droplet cores [22]. The amount of time an individual is in the room should be kept at a minimum [4]. This is of particular importance in smaller rooms.
If the available space is dissimilar from the concept, the risk of infection in the study-specific case can be reduced through the division of the testing areas. Markings help maintain a 1.5 m distance between individuals. This is only relevant, however if the paths between stations cross and the room planning in Figure 4 is impossible. During the study, occupancy of the test site should be kept to a minimum to further reduce the infection risk.
Studies conducted in vehicles are a more challenging case as they offer a smaller space where a diagonal seating arrangement must be employed for a maximum of two individuals to be spaced safely more than 1.5 m apart. The use of a partition further reduces the risk of infection. In most cases, the dividers are not airtight and therefore, only prevent droplet infections and not aerogenic infections because the air and virus-containing particles can flow around the protective walls [3]. Partitions do significantly slow down the distribution of aerosols and droplet cores in the vehicle [9].
The air exchange rates similarly play an important role in smaller spaces such as a vehicle. Opening the car windows as the weather allows should complement the operation of the ventilation as an infection protection measure. The use of the air circulation on the other hand is not recommended, since it would block out fresh air and aerosols and droplet cores are not removed leaving occupants at heightened risk of infection [30].
When selecting subjects, those who are vulnerable and part of at-risk groups should be avoided. If absolutely necessary, these individuals can participate provided their risk of infection can be reduced through comprehensive testing including a rapid test at the study start. It should be noted that a less representative statistical distribution of the total population risks the quality of the study outcome even when populations are excluded for reasons of safety.
Studies occurring during a pandemic, require unnecessary encounters to be avoided. Arrival times for subjects, for instance should be staggered and reception and pre-examination areas must be prepared. The participating subjects must be informed about hygienic measures. Throughout the study, adherence to the respiratory mask, social distancing and hygiene mandates are required. Preliminary examinations shall test subjects for symptoms, the virus or even potentially antibodies in order to prevent infected people from participating. Since rapid tests in particular are only a snapshot and can be less accurate than PCR tests, caution is required. That’s why a positive rapid test needs to be confirmed by a PCR laboratory test [31]. The offsetting of participant arrivals also creates clarity made possible by good organization. These positive characteristics are also worthwhile for studies not occurring in the midst of a pandemic.
After each trial, disinfection is required to protect the next subject from a possible infection. Disinfecting wipes are used to prevent indirect contact infections, and ventilation prevents aerogenic infections. When disinfecting, gloves and respiratory masks must be worn. The use of trained cleaning personnel for this task should be discussed. This should not be mandatory, as the disinfection process is relatively easy and straight forward. Furthermore, there are different types of disinfection. For vehicles, wiping disinfection with soapy water is suitable, as it can reach vehicle contours. Other disinfection strategies such as physical or thermal ones are available, but they are more complicated to employ. Frequent chemical disinfection can damage vehicle surfaces, which can result in a loss of value. This is particularly important when working with rented vehicles. It is, however, more important that hygienic conditions are maintained. Even outside of pandemics, viral and bacterial infections are always possible and therefore should be avoided through hygienic measures.
5. Conclusions and Future Works
The research review and the resulting concept show that subject studies during a pandemic are feasible, depending on the transmission path of the pathogen. As a result, a generic concept has been developed through the example of the COVID-19 pandemic, but the individual sections can also be applied to other situations such as a flu epidemic, where infection protection measures are appropriate. Situational adjustments to the concept may be required. It can serve as a template for the development of other infection protection concepts specifically for the implementation of scientific studies with test persons. However, no infection protection measure provides 100% safety, so there is always a residual infection risk.
In addition to this qualitative concept, a quantitative tool would further aid in a robust risk assessment of conducting studies during pandemics. For instance, a numerical maximum threshold could determine when a study must be cancelled or postponed. This value could be calculated through weighting different factors of infection transmission and indicators of pandemic development. The goal would be to help the test administration confidently decide whether a study can be safely and responsibly conducted under certain difficult circumstances. Breaking down costs associated with this concept would move beyond an epidemiological point of view to incorporate an optimal economic implementation. This information would allow for exact resource planning, thereby reducing financial risks. Simulations could also be carried out in order to collect data on the effectiveness of the concept in advance, which would identify weak points of the concept at an early stage.
Author Contributions
Conceptualization, A.S. and T.K.; methodology, A.S., T.K. and S.M.; software, A.S. and T.K.; validation, A.S., T.K. and S.M.; formal analysis, A.S. and T.K.; investigation, A.S.; resources, A.S.; writing—original draft preparation, T.K. and A.S.; writing—review and editing, T.K., A.S. and S.M.; visualization, A.S. and T.K.; supervision, T.K.; funding acquisition, T.K. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge support by the German Research Foundation and the Open Access Publication Fund of TU Berlin.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank William E. Zirkle for language editing. The concept shown here is the result of a recent bachelor’s thesis by A.S., which contains the long version of this paper.
Conflicts of Interest
The authors declare no conflict of interest. The results, opinions and conclusions expressed in this paper are not necessarily those of Volkswagen Aktiengesellschaft.
References
- Robert Koch Institut (RKI). Coronavirus SARS-CoV-2: Informationen zur Ausweisung internationaler Risikogebiete Durch das Auswärtige Amt, BMG und BMI. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikogebiete_neu.html (accessed on 12 March 2021).
- Technische Universität Dresden. Hygienekonzept für Fahrsimulator-Studie. Available online: https://tu-dresden.de/bu/verkehr/iad/kft/ressourcen/dateien/newsdokumente/202103/EMISA_Hygienekonzept_Coronavirus-Fragebogen.pdf?lang=de (accessed on 23 August 2021).
- Technische Universität Berlin. FAQ zu Aersolen in Bezug auf SARS-CoV-2: Dauerlüften, Luftfilter—Wie Umgehen mit Den Aerosolen in Innenräumen? Available online: https://www.tu.berlin/forschen/themenportal-forschen/2020/august/faq-zu-aersolen-in-bezug-auf-sars-cov-2/ (accessed on 12 March 2021).
- Kriegel, M. Anzahl der mit SARS-CoV-2 beladenen Partikel in der Raumluft und Deren Eingeatmete Menge, sowie die Bewertung des Infektionsrisikos, sich Darüber mit COVID-19 Anzustecken. 2020. Available online: https://depositonce.tu-berlin.de/bitstream/11303/11767.3/9/Virenbeladene_Partikel_im_Raum_v3.pdf (accessed on 12 March 2021).
- Schulze-Röbbecke, R.; Reska, M.; Lemmen, S. Welche Schutzmaske schützt vor COVID-19?: Was ist evidenzbasiert? Krankenhaushygiene up2date 2020, 15, 123–132. [Google Scholar]
- Kriegel, M.; Hartmann, A. COVID-19 Ansteckung über Aerosolpartikel: Vergleichende Bewertung von Innenräumen Hinsichtlich des Situationsbedingten R-Wertes. 2021. Available online: https://depositonce.tu-berlin.de/bitstream/11303/12578/5/kriegel_hartmann_2021.pdf (accessed on 25 April 2021).
- Paschotta, R. Luftwechselrate. Available online: https://www.energie-lexikon.info/luftwechselrate.html#:%7E:text=Die%20Luftwechselrate%20eines%20Raums%20oder,%2Fh%20%3D%20h%E2%88%921 (accessed on 12 March 2021).
- Makoto, T. Prediction and Countermeasures for Infection by Virus Contaminated Droplet in Indoor Environment. Available online: https://www.covid19-ai.jp/en-us/presentation/2020_rq1_droplet_infection_simulation/articles/article003/ (accessed on 12 March 2021).
- Makoto, T. Prediction and Countermeasures for Infection by Virus Contaminated Droplet in Indoor Environment. Available online: https://www.covid19-ai.jp/en-us/presentation/2020_rq1_droplet_infection_simulation/articles/article004/ (accessed on 12 March 2021).
- Pischinger, S.; Seiffert, U. Vieweg Handbuch Kraftfahrzeugtechnik; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; ISBN 978-3-658-09527-7. [Google Scholar]
- Sinanovic, A. Durchführung von Probandenstudien während der COVID-19 Pandemie. Bachelorarbeit; Technische Universität Berlin: Berlin, Germany, 2021. [Google Scholar]
- BG-Verkehr. Taxi. Available online: https://www.bg-verkehr.de/coronavirus/tipps-fuer-unternehmen-und-ihre-beschaeftigten/taxi (accessed on 11 March 2021).
- Mathai, V.; Das, A.; Bailey, J.A.; Breuer, K. Airflows inside passenger cars and implications for airborne disease transmission. Sci. Adv. 2021, 7, eabe0166. [Google Scholar] [CrossRef] [PubMed]
- Fruin, S.A.; Hudda, N.; Sioutas, C.; Delfino, R.J. Predictive model for vehicle air exchange rates based on a large, representative sample. Environ. Sci. Technol. 2011, 45, 3569–3575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knibbs, L.D.; Morawska, L.; Bell, S.C. The risk of airborne influenza transmission in passenger cars. Epidemiol. Infect. 2012, 140, 474–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert Koch Institut (RKI). Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=A26AFC1E37AB7F14D92A29479166C41F.internet121?nn=2386228 (accessed on 12 March 2021).
- Robert Koch Institut (RKI). Coronavirus SARS-CoV-2: Informationen und Hilfestellungen für Personen mit einem höheren Risiko für einen schweren COVID-19-Krankheitsverlauf. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikogruppen.html (accessed on 12 March 2021).
- Robert Koch Institut (RKI). Warum Treten Grippewellen Immer im Winter auf? Available online: https://www.rki.de/SharedDocs/FAQ/Influenza/FAQ02.html (accessed on 27 April 2021).
- Suttorp, N. (Ed.) Infektionskrankheiten: Verstehen, Erkennen, Behandeln; Thieme: Stuttgart, Germany; New York, NY, USA, 2004; ISBN 9783131877116. [Google Scholar]
- Robert Koch Institut (RKI). Navigation: Virus und Epidemiologie. Available online: https://www.rki.de/SharedDocs/FAQ/NCOV2019/FAQ_Liste_Epidemiologie.html (accessed on 12 March 2021).
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Im Alltag Maske Tragen. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/im-alltag-maske-tragen.html (accessed on 11 March 2021).
- Kähler, C.; Hain, R. Musizieren während der Pandemie -was rät die Wissenschaft?: Über Infektionsrisiken beim Chorsingen und Musizieren mit Blasinstrumenten. Available online: https://www.unibw.de/lrt7/musizieren_waehrend_der_pandemie.pdf (accessed on 12 March 2021).
- Ahlawat, A.; Wiedensohler, A.; Mishra, S.K. An Overview on the Role of Relative Humidity in Airborne Transmission of SARS-CoV-2 in Indoor Environments. Aerosol. Air Qual. Res. 2020, 20, 1856–1861. [Google Scholar] [CrossRef]
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Abstand Halten. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/abstand-halten.html#:%7E:text=Achten%20Sie%20im%20%C3%B6ffentlichen%20Raum,Sie%20auf%20H%C3%A4ndesch%C3%BCtteln%20oder%20Umarmungen (accessed on 11 March 2021).
- Bundeszentrale für Gesundheitliche Aufklärung (BZgA). Regelmäßig Lüften. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona/regelmaessig-lueften.html (accessed on 11 March 2021).
- Xie, X.; Li, Y.; Chwang, A.T.Y.; Ho, P.L.; Seto, W.H. How far droplets can move in indoor environments--revisiting the Wells evaporation-falling curve. Indoor Air 2007, 17, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege (BGW). Medizinische Gesichtsmaske—Mund-Nasen-Schutz (MNS). Available online: https://www.bgw-online.de/DE/Arbeitssicherheit-Gesundheitsschutz/Hygiene_und_Infektionsschutz/Masken/Maske-02_Mund-Nasen-Schutz.html (accessed on 11 March 2021).
- Deutschland. Die Timeline zum Coronavirus in Deutschland: Hier findet ihr die Wichtigsten Entwicklungen zu COVID-19 in Deutschland im Überblick. Available online: https://www.deutschland.de/de/die-timeline-coronavirus-germany-deutschland (accessed on 11 March 2021).
- Heinrich, C.; Collin, C. Corona-Nachweis: Die Testverfahren im Überblick. Available online: https://www.apotheken-umschau.de/krankheiten-symptome/infektionskrankheiten/coronavirus/corona-nachweis-die-testverfahren-im-ueberblick-724147.html#PCR-Schnelltest (accessed on 12 March 2021).
- Ott, W.; Klepeis, N.; Switzer, P. Air change rates of motor vehicles and in-vehicle pollutant concentrations from secondhand smoke. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Seifried, J.; Böttcher, S.; von Kleist, M.; Jenny, M.A.; Antão, E.; Oh, D.Y.; Jung-Sendzik, T.; Broich, K.; Denkinger, C.; Bartenschlager, T.; et al. Antigentests als ergänzendes Instrument in der Pandemiebekämpfung. Epidemiol. Bull. 2021, 17, 3–14. [Google Scholar] [CrossRef]
Figure 1.
Holistic concept for infection prevention in studies conducted in stationary rooms and vehicles.
Figure 1.
Holistic concept for infection prevention in studies conducted in stationary rooms and vehicles.

Figure 2.
Evaluation of the pandemic situation.

Figure 3.
Infection control measures in stationary test rooms.

Figure 4.
Indoor floor plan example for conducting a study in a room or vehicle.

Figure 5.
Markings on the floor to maintain a safe distance; the red cross indicates areas that should be avoided and the green check indicates possible areas to walk.
Figure 5.
Markings on the floor to maintain a safe distance; the red cross indicates areas that should be avoided and the green check indicates possible areas to walk.

Figure 6.
Outdoor area plan for conducting a study using a vehicle.

Figure 7.
Infection control measures in vehicles and simulators.

Figure 8.
Subject selection.

Figure 9.
Planning of the schedule and study procedure.

Figure 10.
Disinfection of the experimental environment.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kantusch, T.; Sinanovic, A.; Marker, S. A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic. Appl. Sci. 2021, 11, 8556. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188556
AMA Style
Kantusch T, Sinanovic A, Marker S. A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic. Applied Sciences. 2021; 11(18):8556. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188556
Chicago/Turabian StyleKantusch, Timmy, Advan Sinanovic, and Stefanie Marker. 2021. "A Concept for Conducting Scientific Studies in Vehicles and Stationary Test Rooms during the COVID-19 Pandemic" Applied Sciences 11, no. 18: 8556. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188556
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.