
A Simple Approach for Counting CD4+ T Cells Based on a Combination of Magnetic Activated Cell Sorting and Automated Cell Counting Methods

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Isolation of Peripheral Blood Mononuclear Cells (PBMC) from Whole Blood by Sucrose Gradient Centrifugation
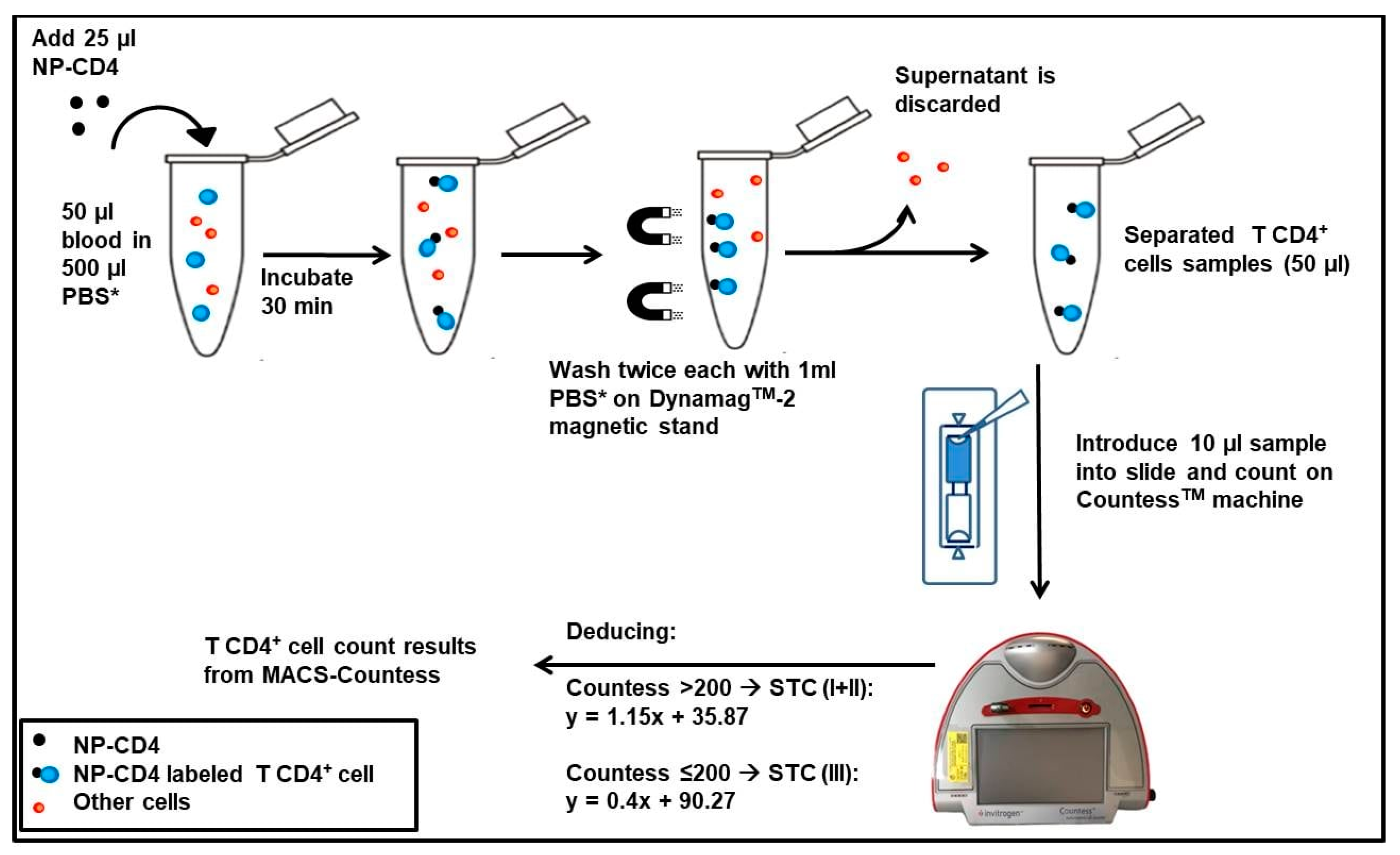
2.3. Isolation of CD4+ T Cells from PBMCs and Whole Blood Using Anti-CD4 Antibodies Conjugated with Magnetic Nanoparticles
2.4. Fluorescence-Activated Cell Sorting (FACS) and Flow Cytometry Analysis of Cell Population before and after Cell Separation
2.5. Immunofluorescence Labeling of Cell Population before and after Cell Separation
2.6. Cell Enumeration on CountessTM Automated Cell Counter
2.7. Statistical Analysis
3. Results
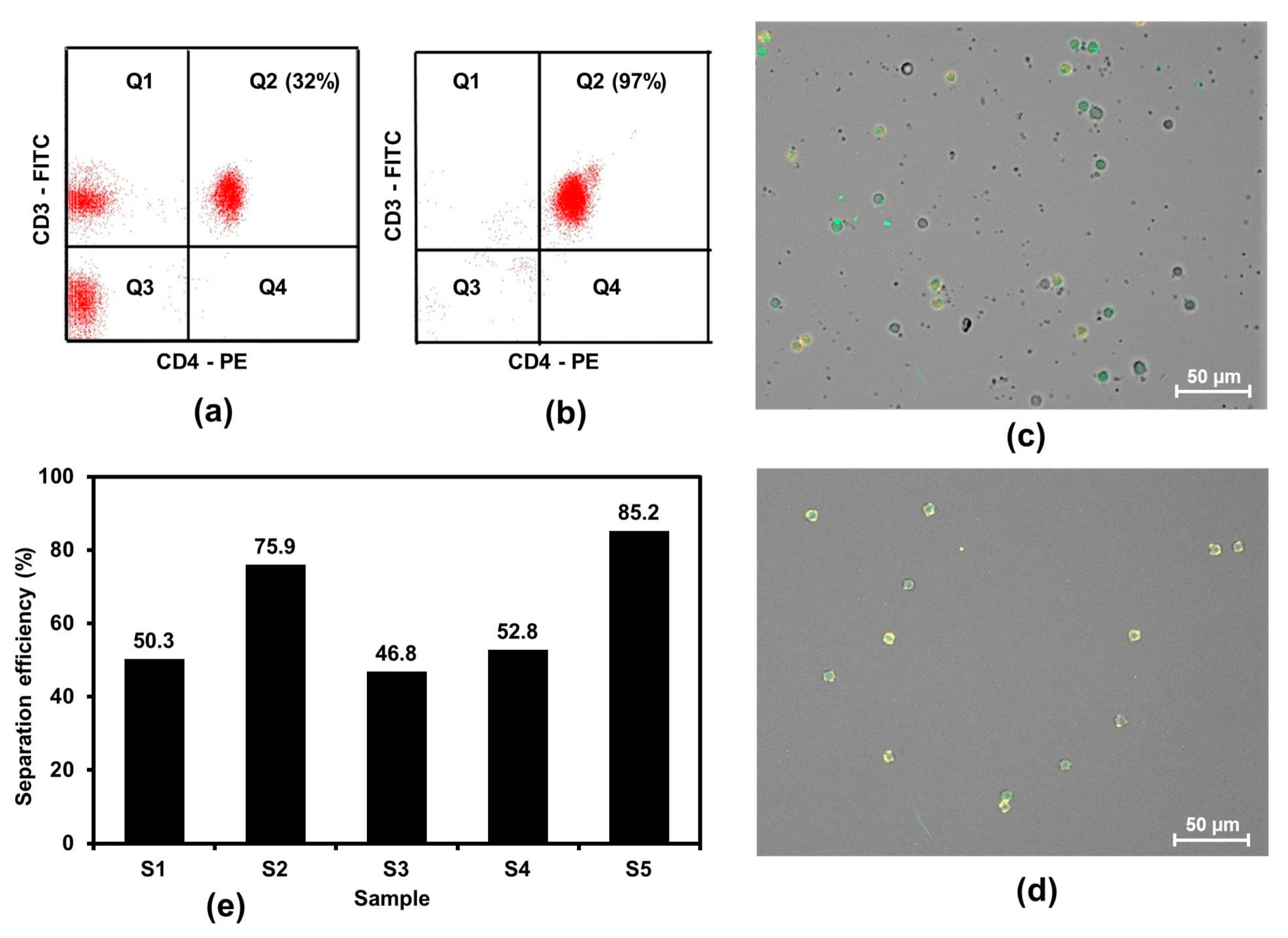
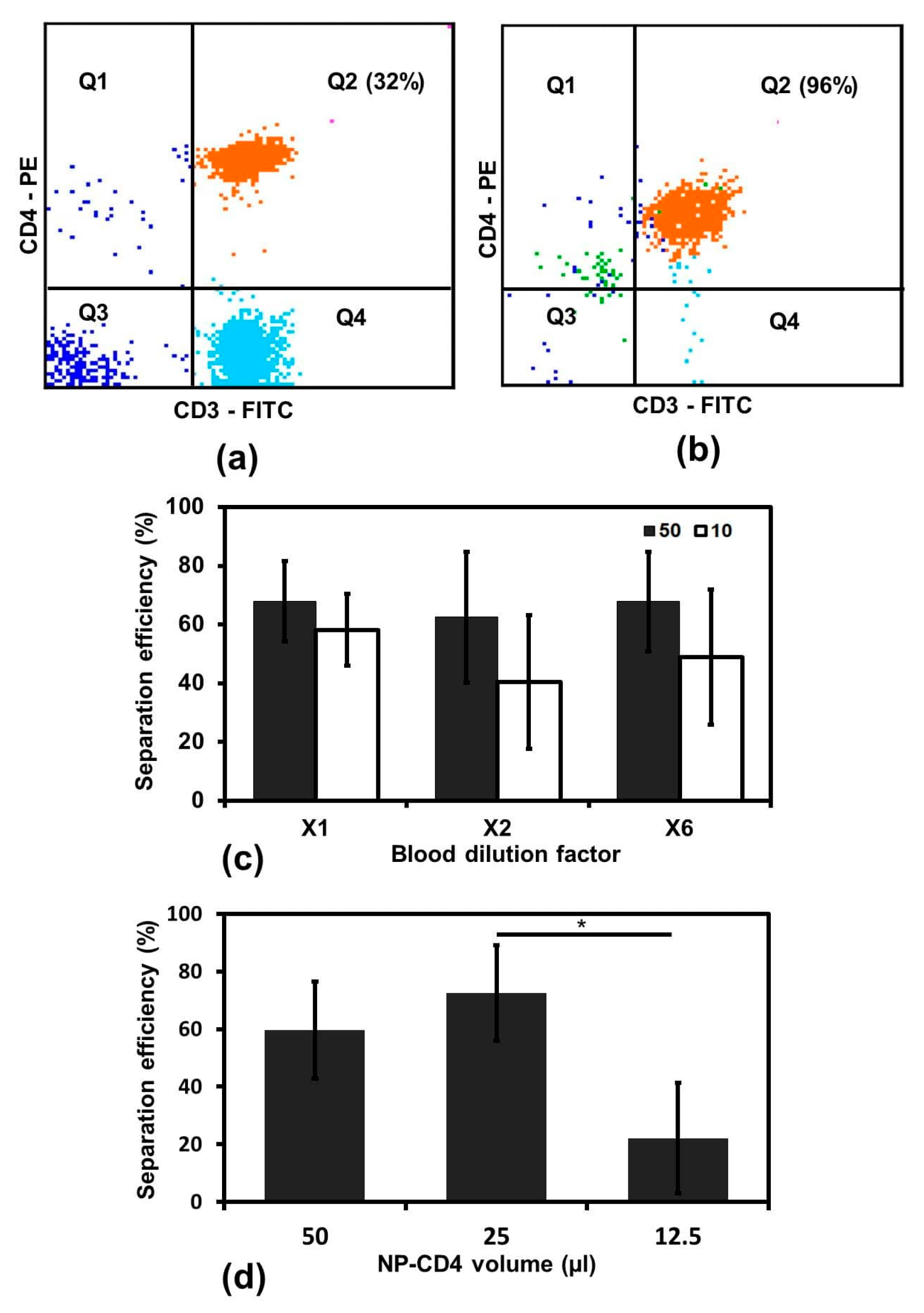
3.1. Separation of CD4+ T Cells from PBMCs Using NP-CD4
3.2. Optimizing Variation for CD4+ T Cell MACS Separation
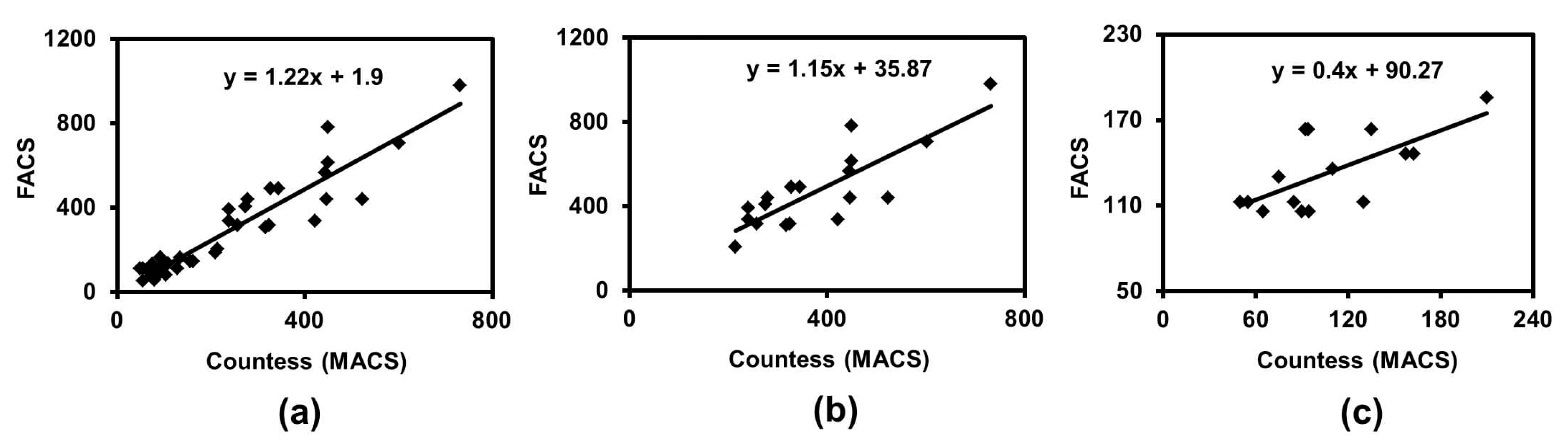
3.3. Comparison between MACS-Countess to FACS Methods
3.3.1. Generating STCs between Countess (MACS) and FACS
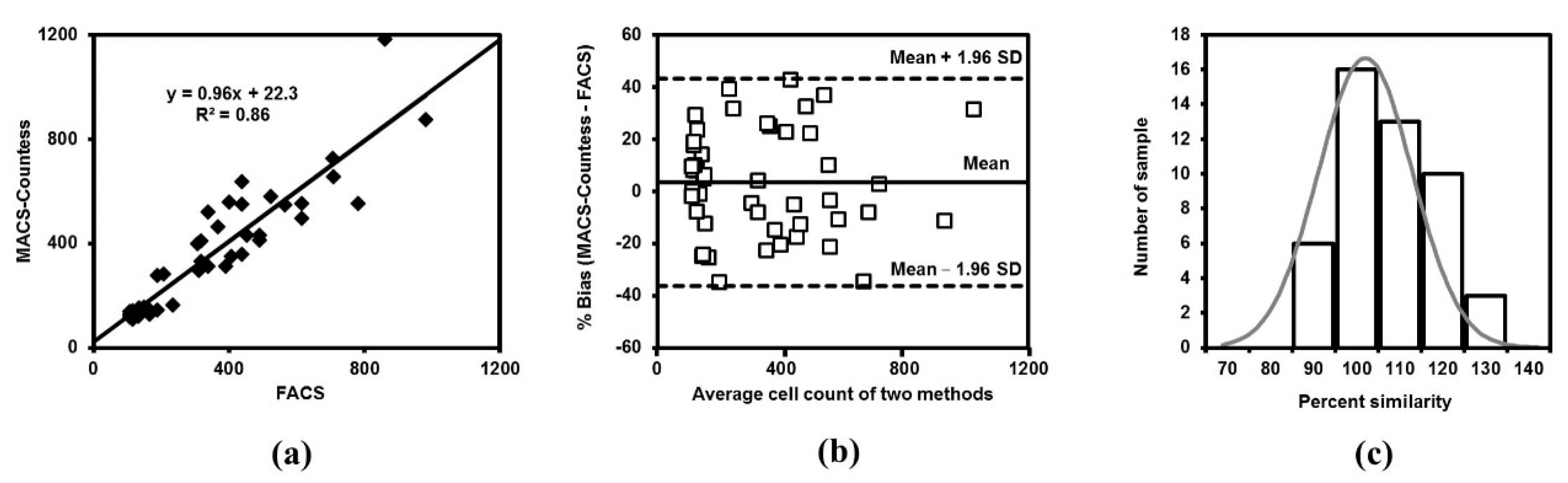
3.3.2. MACS-Countess Compared with FACS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klatzmann, D.; Barre-Sinoussi, F.; Nugeyre, M.T.; Danquet, C.; Vilmer, E.; Griscelli, C.; Brun-Veziret, F.; Rouzioux, C.; Gluckman, J.C.; Chermann, J.-C.; et al. Selective tropism of lymphadenopathy associated virus (LAV) for helper-inducer T lymphocytes. Science 1984, 225, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Haase, A.T. Population biology of HIV-1 infection: Viral and CD4+ T cell demographics and dynamics in lymphatic tissues. Annu. Rev. Immunol. 1999, 17, 625–656. [Google Scholar] [CrossRef] [PubMed]
- Song, A.; Liu, X.; Huang, X.; Meyers, K.; Oh, D.-Y.; Hou, J.; Xia, W.; Su, B.; Wang, N.; Lu, X.; et al. From CD4-based initiation to treating all HIV-infected adults immediately: An evidence-based meta-analysis. Front. Immunol. 2018, 9, 212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.Q.; Yao, Y.M.; Huang, Z.Y.; Cao, J.T.; Zhu, C.W.; Yu, K.H.; Pan, J.; Hu, B.J. Low CD4 T cell count predicts radiological progression in severe and critically ill COVID-19 patients: A case control study. J. Thorac. Dis. 2021, 13, 4723–4730. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Casado, J.L.; Härter, G.; Vizcarra, P.; Moreno, A.; Cattaneo, D.; Meraviglia, P.; Spinner, C.D.; Schabaz, F.; Grunwald, S.; et al. Immune deficiency is a risk factor for severe COVID-19 in people living with HIV. HIV Med. 2021, 22, 372–378. [Google Scholar] [CrossRef]
- Chu, H.; Zhou, J.; Wong, B.H.-Y.; Li, C.; Chan, J.F.-W.; Cheng, Z.-S.; Yang, D.; Wang, D.; Lee, A.C.-Y.; Li, C.; et al. Middle East respiratory syndrome coronavirus efficiently infects human primary T lymphocytes and activates the extrinsic and intrinsic apoptosis pathways. J. Infect. Dis. 2016, 213, 904–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and functional exhaustion of T cells in patients with coronavirus disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef]
- De Biasi, S.; Meschiari, M.; Gibellini, L.; Bellinazzi, C.; Borella, R.; Fidanza, L.; Gozzi, L.; Iannone, A.; Tartaro, D.L.; Mattioli, M.; et al. Marked T cell activation, senescence, exhaustion and skewing towards TH17 in patients with COVID-19 pneumonia. Nat. Commun. 2020, 11, 3434. [Google Scholar] [CrossRef]
- De Wit, E.; Van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef]
- Filion, L.G.; Izaguirre, C.A.; Garber, G.E.; Huebsh, L.; Aye, M.T. Detection of surface and cytoplasmic CD4 on blood monocytes from normal and HIV-1 infected individuals. J. Immunol. Methods 1990, 135, 59–69. [Google Scholar] [CrossRef]
- Schnizlein-Bick, C.T.; Spritzler, J.; Wilkening, C.L.; Nicholson, J.K.A.; O’Gorman, M.R.G. Evaluation of TruCount absolute-count tubes for determining CD4 and CD8 cell numbers in human immunodeficiency virus-positive adults. Clin. Diagn. Lab. Immunol. 2000, 7, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Glynn, M.T.; Kinahan, D.J.; Ducrée, J. CD4 counting technologies for HIV therapy monitoring in resource-poor settings–state-of-the-art and emerging microtechnologies. Lab Chip 2013, 13, 2731–2748. [Google Scholar] [CrossRef]
- Thakar, M.; Mahajan, B.; Shaikh, N.; Bagwan, S.; Sane, S.; Kabra, S.; Rewari, B.; Shaukat, M.; Singh, N.; Trevor, P.; et al. Utility of the point of care CD4 analyzer, PIMA, to enumerate CD4 counts in the field settings in India. AIDS Res. Ther. 2012, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Sukapirom, K.; Onlamoon, N.; Thepthai, C.; Polsrila, K.; Tassaneetrithep, B.; Pattanapanyasat, K. Performance evaluation of the Alere PIMA CD4 test for monitoring HIV-infected individuals in resource-constrained settings. JAIDS J. Acquir. Immune Defic. Syndr. 2011, 58, 141–147. [Google Scholar] [CrossRef]
- Pham, M.D.; Agius, P.A.; Romero, L.; McGlynn, P.; Anderson, D.; Crowe, S.M.; Luchters, S. Acceptability and feasibility of point-of-care CD4 testing on HIV continuum of care in low and middle income countries: A systematic review. BMC Health Serv. Res. 2016, 16, 343. [Google Scholar] [CrossRef] [Green Version]
- Larson, B.; Schnippel, K.; Ndibongo, B.; Long, L.; Fox, M.P.; Rosen, S. How to estimate the cost of point-of-care CD4 testing in program settings: An example using the Alere PimaTM analyzer in South Africa. PLoS ONE 2012, 7, e35444. [Google Scholar]
- Kang, J.H.; Krause, S.; Tobin, H.; Mammoto, A.; Kanapathipillai, M.; Ingber, D.E. A combined micromagnetic-microfluidic device for rapid capture and culture of rare circulating tumor cells. Lab Chip 2012, 12, 2175–2181. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Aguilar, Z.P.; Yang, L.; Kuang, M.; Duan, H.; Xiong, Y.; Wei, H.; Wang, A. Antibody conjugated magnetic iron oxide nanoparticles for cancer cell separation in fresh whole blood. Biomaterials 2011, 32, 9758–9765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshino, T.; Hirabe, H.; Takahashi, M.; Kuhara, M.; Takeyama, H.; Matsunaga, T. Magnetic cell separation using nano-sized bacterial magnetic particles with reconstructed magnetosome membrane. Biotechnol. Bioeng. 2008, 101, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Mikš-Krajnik, M.; Yang, Y.; Xu, W.; Yuk, H.-G. Real-time PCR method combined with immunomagnetic separation for detecting healthy and heat-injured Salmonella Typhimurium on raw duck wings. Int. J. Food Microbiol. 2014, 186, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Carinelli, S.; Xufre, C.; Alegret, S.; Marti, M.; Pividori, M.I. CD4 quantification based on magneto ELISA for AIDS diagnosis in low resource settings. Talanta 2016, 160, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Zeb, Q.; Wang, C.; Shafiq, S.; Liu, L. An overview of single-cell isolation techniques. In Single-Cell Omics; Academic Press: Cambridge, MA, USA, 2019; pp. 101–135. [Google Scholar]
- Pollock, M.A.; Jefferson, S.G.; Kane, J.W.; Lomax, K.; MacKinnon, G.; Winnard, C.B. Method comparison—A different approach. Ann. Clin. Biochem. 1992, 29, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Scott, L.E.; Galpin, J.S.; Glencross, D.K. Multiple method comparison: Statistical model using percentage similarity. Cytom. Part B Clin. Cytom. J. Int. Soc. Anal. Cytol. 2003, 54, 46–53. [Google Scholar] [CrossRef]
- Stevens, W.; Gelman, R.; Glencross, D.K.; Scott, L.E.; Crowe, S.M.; Spira, T. Evaluating new CD4 enumeration technologies for resource-constrained countries. Nat. Rev. Microbiol. 2008, 6, S29–S38. [Google Scholar] [CrossRef]
- Peeling, R.W.; Sollis, K.A.; Glover, S.; Crowe, S.M.; Landay, A.L.; Cheng, B.; Barnett, D.; Denny, T.N.; Spira, T.J.; Stevens, W.S.; et al. CD4 enumeration technologies: A systematic review of test performance for determining eligibility for antiretroviral therapy. PLoS ONE 2015, 10, e0115019. [Google Scholar] [CrossRef] [Green Version]
- Kleiveland, C.R. Peripheral blood mononuclear cells. In The Impact of Food Bioactives on Health: In Vitro and Ex Vivo Models; Springer: Cham, Switzerland, 2015; pp. 161–167. [Google Scholar]
- Mwau, M.; Adungo, F.; Kadima, S.; Njagi, E.; Kirwaye, C.; Abubakr, N.S.; Okubi, L.A.; Waihenya, M.; Lusike, J.; Hungu, J. Evaluation of PIMATM® point of care technology for CD4 T cell enumeration in Kenya. PLoS ONE 2013, 8, e67612. [Google Scholar]
- Makadzange, A.T.; Bogezi, C.; Boyd, K.; Gumbo, A.; Mukura, D.; Matubu, A.; Ndhlovu, C.E. Evaluation of the FACSPresto, a new point of care device for the enumeration of CD4% and absolute CD4+ T cell counts in HIV infection. PLoS ONE 2016, 11, e0157546. [Google Scholar]
- Pinto, I.C.; Sabidó, M.; Pereira, A.B.; Mello, M.B.; de Melo Xavier Shimizu, A.; Protti, B.L.; Benzaken, A.S. Field evaluation of a point-of-care CD4 analyzer for monitoring HIV patients in the interior of the Amazon region, Brazil. PLoS ONE 2015, 10, e0121400. [Google Scholar] [CrossRef]
- Elharti, E.; Abbadi, H.; Bensghir, R.; El Filali, K.M.; Elmrabet, H.; Oumzil, H. Assessment of two POC technologies for CD4 count in Morocco. AIDS Res. Ther. 2020, 17, 31. [Google Scholar] [CrossRef]
- Schneider, T.; Karl, S.; Moore, L.R.; Chalmers, J.J.; Williams, P.S.; Zborowski, M. Sequential CD34 cell fractionation by magnetophoresis in a magnetic dipole flow sorter. Analyst 2010, 135, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratt, E.D.; Huang, C.; Hawkins, B.G.; Gleghorn, J.P.; Kirby, B.J. Rare cell capture in microfluidic devices. Chem. Eng. Sci. 2011, 66, 1508–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Banada, P.P.; Chatni, M.R.; Lim, K.S.; Bhunia, A.K.; Ladisch, M.; Bashir, R. A multifunctional micro-fluidic system for dielectrophoretic concentration coupled with immuno-capture of low numbers of Listeria monocytogenes. Lab Chip 2006, 6, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.E.; Benson, C.; Holmes, K.K.; Brooks, J.T.; Pau, A.; Masur, H.; Centers for Disease Control and Prevention (CDC); National Institutes of Health; HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recomm. Rep. 2009. Available online: https://pubmed.ncbi.nlm.nih.gov/19357635/ (accessed on 17 October 2021).
- He, R.; Lu, Z.; Zhang, L.; Fan, T.; Xiong, R.; Shen, X.; Feng, H.; Meng, H.; Lin, W.; Jiang, W.; et al. The clinical course and its correlated immune status in COVID-19 pneumonia. J. Clin. Virol. 2020, 127, 104361. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Jiang, D.; Gao, L.; Zhou, J.; Xiao, J.; Cheng, X.; He, B.; Chen, Y.; Lei, P.; Tan, X.; et al. Clinical characteristics and predictive value of lower CD4+ T cell level in patients with moderate and severe COVID-19: A multicenter retrospective study. BMC Infect. Dis. 2021, 21, 57. [Google Scholar] [CrossRef]
- Lutwama, F.; Serwadda, R.; Mayanja-Kizza, H.; Shihab, H.M.; Ronald, A.; Kamya, M.R.; Thomas, D.; Johnson, E.; Quinn, T.C.; Moore, R.D.; et al. Evaluation of Dynabeads and Cytospheres compared with flow cytometry to enumerate CD4+ T cells in HIV-infected Ugandans on antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2008, 48, 297. [Google Scholar] [CrossRef] [Green Version]
- Boyle, D.S.; Hawkins, K.R.; Steele, M.S.; Singhal, M.; Cheng, X. Emerging technologies for point-of-care CD4 T-lymphocyte counting. Trends Biotechnol. 2012, 30, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, M.; Daneau, G.; Ding, T.; Sitoe, N.E.; Westerman, L.E.; Stokx, J.; Jani, I.V.; Coetzee, L.M.; Scott, L.; De Weggheleire, A.; et al. Performance of the PointCare NOW system for CD4 counting in HIV patients based on five independent evaluations. PLoS ONE 2012, 7, e41166. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group (CD4+ T Cells/µL) | Sample Order | MACS-Countess (CD4+ T Cells/µL) | STC | Deduced Value (CD4+ T Cells/µL) | FACS (CD4+ T Cells/µL) | Bias (%) |
|---|---|---|---|---|---|---|
| I (1200–600) | 1 | 1000 | I + II | 1183.6 | 860 | 31.7 |
| 2 | 539.7 | I + II | 655.3 | 709 | −7.9 | |
| 3 | 402.3 | I + II | 497.7 | 615 | −21.1 | |
| II (600–200) | 1 | 474.9 | I + II | 581 | 524 | 10.3 |
| 2 | 343.8 | I + II | 430.5 | 452 | −4.9 | |
| 3 | 454.5 | I + II | 557.5 | 400.7 | 32.7 | |
| 4 | 372.4 | I + II | 463.3 | 368 | 22.9 | |
| 5 | 227.3 | I + II | 296.7 | 310.3 | −4.5 | |
| 6 | 182.5 | III | 163.8 | 232.8 | −34.8 | |
| III (200–100) | 1 | 135 | III | 144.6 | 186.2 | −25.1 |
| 2 | 152.3 | III | 151.6 | 131.3 | 14.3 | |
| 3 | 99.8 | III | 130.5 | 120 | 8.3 | |
| 4 | 95 | III | 128.5 | 118.5 | 8.1 | |
| 5 | 75 | III | 120.5 | 111 | 8.2 | |
| 6 | 125 | III | 140.6 | 104.7 | 29.3 |
| Method | Cut-Off | Sensitivity | Specificity | PPV | NPV | Upward Misclassification Rate | Downward Misclassification Rate |
|---|---|---|---|---|---|---|---|
| MACS-Countess | 350 cells/µL | 89.7% | 94.7% | 96.3% | 85.7% | 10.3% | 5.3% |
| 500 cells/µL | 89.7% | 88.9% | 97.2% | 66.7% | 10.3% | 11.1% | |
| PIMA [29,30,31,32] | 350 cells/µL | 89.6–100% | 85.7–86.7% | 91.2% | 92.3% | 0–10.4% | 13.3–14.3% |
| 500 cells/µL | 95.5% | 84.2% | 76.0–80.2% | 94.9–96.4% | 4.5% | 15.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vo, N.D.; Nguyen, A.T.V.; Le, H.T.; Nguyen, N.H.; Pham, H.T.T. A Simple Approach for Counting CD4+ T Cells Based on a Combination of Magnetic Activated Cell Sorting and Automated Cell Counting Methods. Appl. Sci. 2021, 11, 9786. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219786
Vo ND, Nguyen ATV, Le HT, Nguyen NH, Pham HTT. A Simple Approach for Counting CD4+ T Cells Based on a Combination of Magnetic Activated Cell Sorting and Automated Cell Counting Methods. Applied Sciences. 2021; 11(21):9786. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219786
Chicago/Turabian StyleVo, Ngoc Duc, Anh Thi Van Nguyen, Hoi Thi Le, Nam Hoang Nguyen, and Huong Thi Thu Pham. 2021. "A Simple Approach for Counting CD4+ T Cells Based on a Combination of Magnetic Activated Cell Sorting and Automated Cell Counting Methods" Applied Sciences 11, no. 21: 9786. https://0-doi-org.brum.beds.ac.uk/10.3390/app11219786