
Automated Detection of Gastric Cancer by Retrospective Endoscopic Image Dataset Using U-Net R-CNN

 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Related Works
1.3. Objective
2. Methods
2.1. Outline
2.2. Image Dataset
2.3. Data Augmentation
2.4. Initial Detection
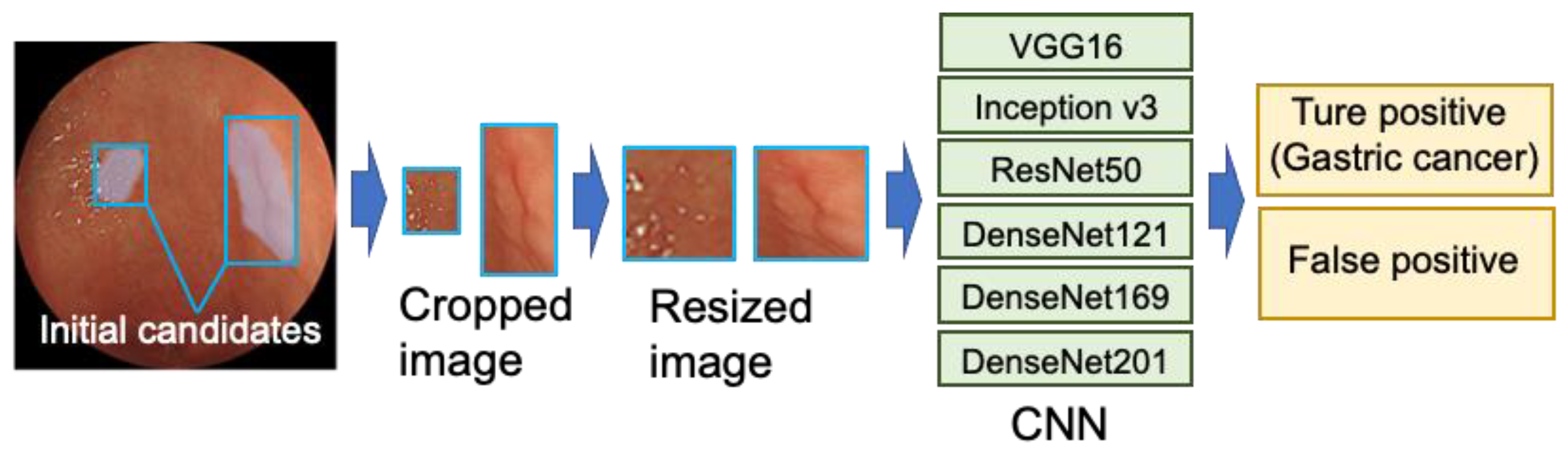
2.5. Box Classification
2.6. Evaluation Metrics
3. Results
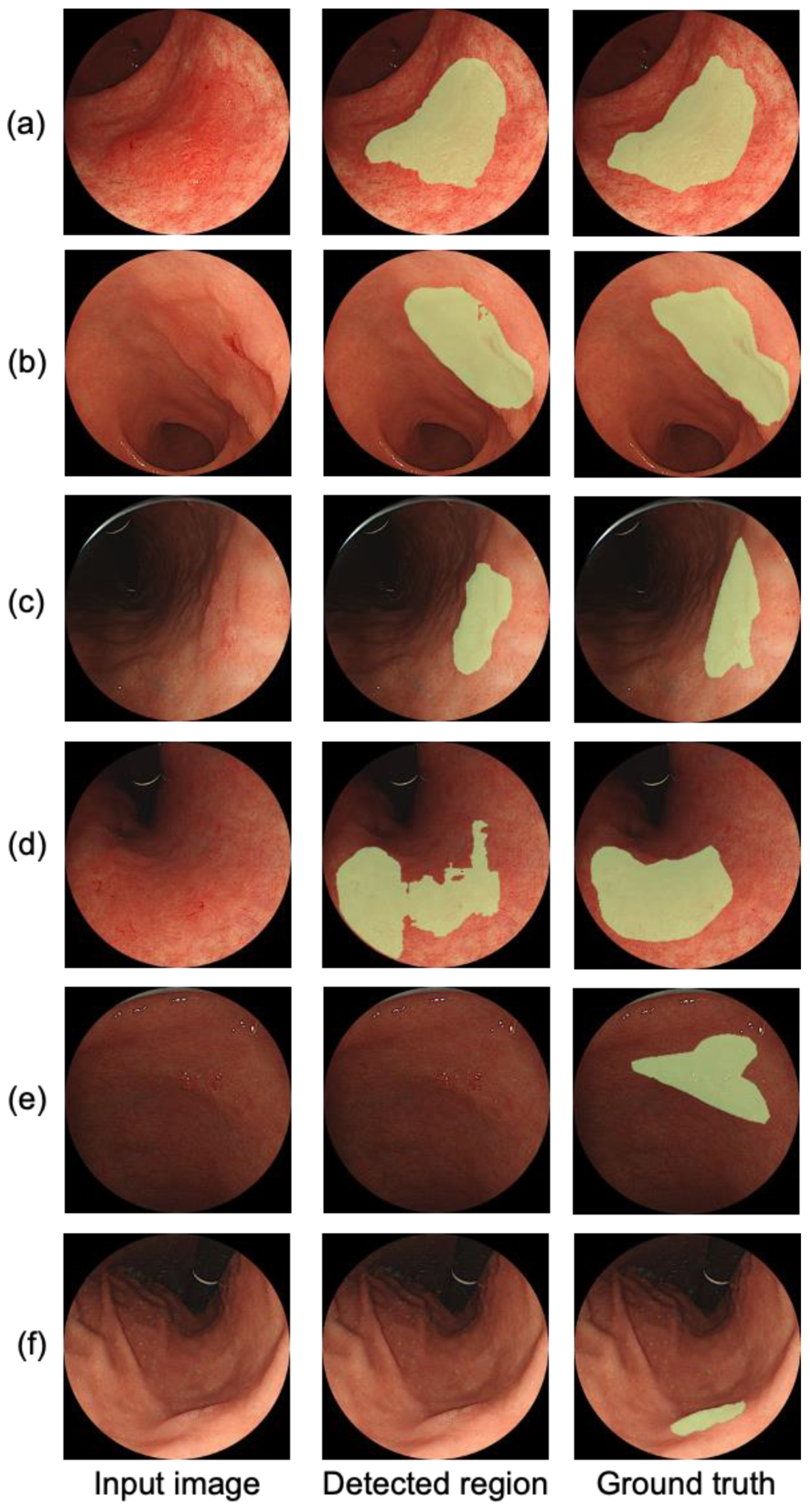
3.1. Initial Detection
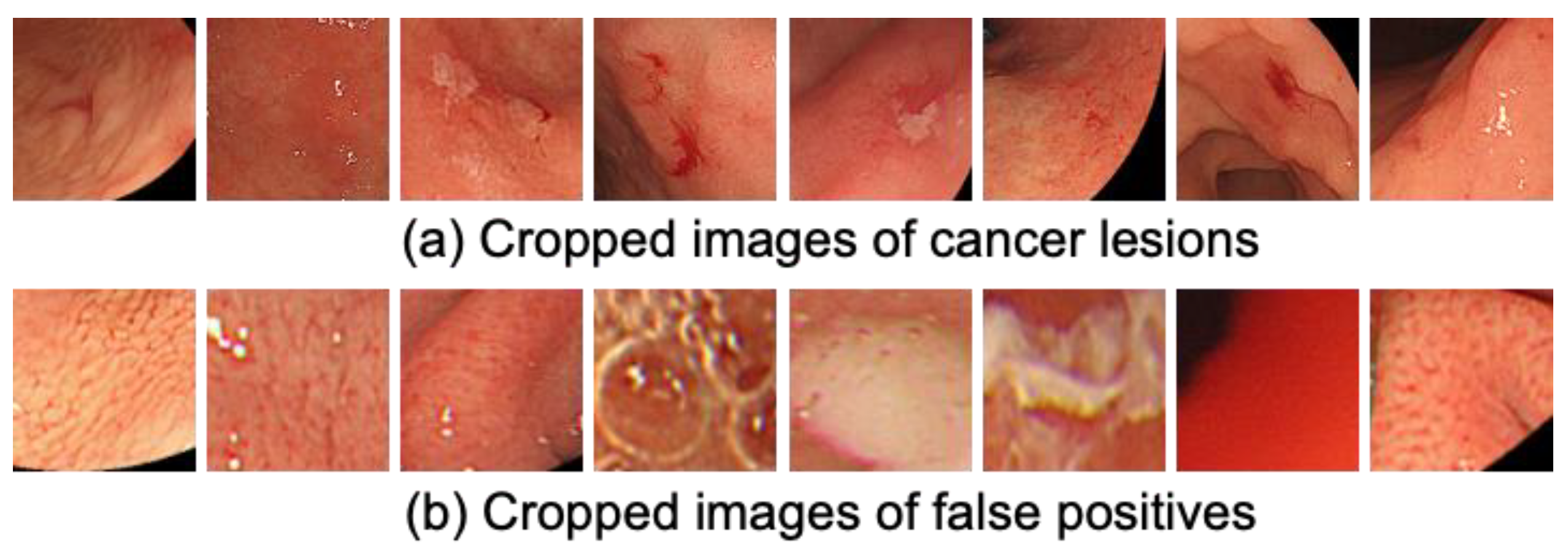
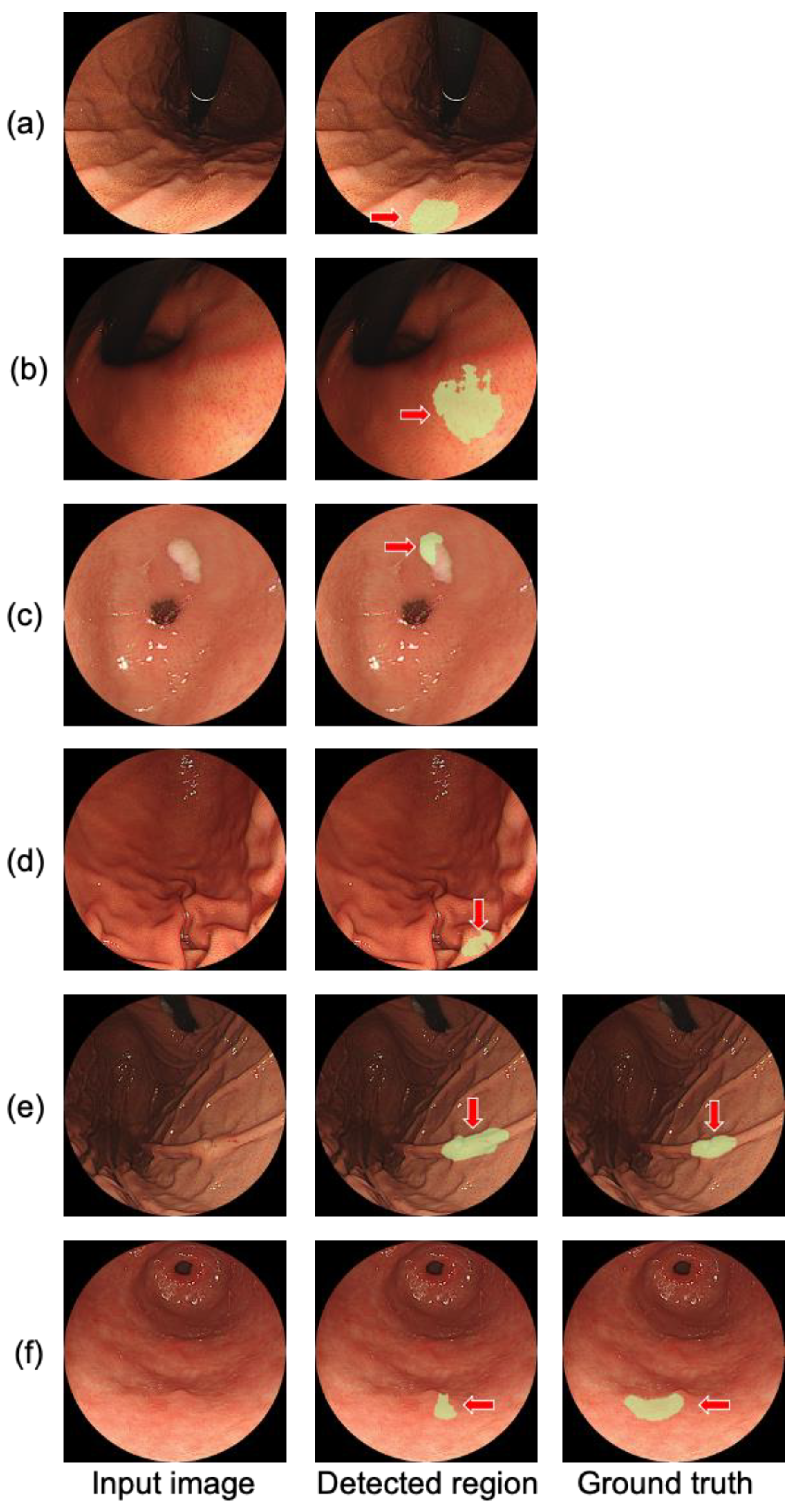
3.2. False Positive Reduction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the global burden of disease study global burden of disease cancer collaboration. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [PubMed]
- Karger Publishers [Internet]. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality, and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 31 October 2021).
- Tashiro, A.; Sano, M.; Kinameri, K.; Fujita, K.; Takeuchi, Y. Comparing mass screening techniques for gastric cancer in Japan. World J. Gastroenterol. 2006, 12, 4873–4874. [Google Scholar] [PubMed]
- Toyoizumi, H.; Kaise, M.; Arakawa, H.; Yonezawa, J.; Yoshida, Y.; Kato, M.; Yoshimura, N.; Goda, K.; Tajiri, H. Ultrathin endoscopy versus high-resolution endoscopy for diagnosing superficial gastric neoplasia. Gastrointest. Endosc. 2009, 70, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, A.; Tsukamoto, T.; Yamada, A.; Kiriyama, Y.; Imaizumi, K.; Saito, K.; Fujita, H. Deep learning approach to classification of lung cytological images: Two-step training using actual and synthesized images by progressive growing of generative adversarial networks. PLoS ONE 2020, 15, e0229951. [Google Scholar] [CrossRef] [PubMed]
- Yan, K.; Cai, J.; Zheng, Y.; Harrison, A.P.; Jin, D.; Tang, Y.B.; Tang, Y.X.; Huang, L.; Xiao, J.; Lu, L. Learning from Multiple Datasets with Heterogeneous and Partial Labels for Universal Lesion Detection in CT. arXiv 2020, arXiv:2009.02577. [Google Scholar] [CrossRef] [PubMed]
- Sahiner, B.; Pezeshk, A.; Hadjiiski, L.M.; Wang, X.; Drukker, K.; Cha, K.H.; Summers, R.M.; Giger, M.L. Deep learning in medical imaging and radiation therapy. Med. Phys. 2019, 46, e1–e36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toda, R.; Teramoto, A.; Tsujimoto, M.; Toyama, H.; Imaizumi, K.; Saito, K.; Fujita, H. Synthetic CT Image Generation of Shape-Controlled Lung Cancer using Semi-Conditional InfoGAN and Its Applicability for Type Classification. Int. J. Comput. Assist. Rad. Surg. 2021, 16, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, M.; Teramoto, A.; Dosho, M.; Tanahashi, S.; Fukushima, A.; Ota, S.; Inui, Y.; Matsukiyo, R.; Obama, Y.; Toyama, H. Automated classification of increased uptake regions in bone SPECT/CT images using three-dimensional deep convolutional neural network. Nucl. Med. Commun. 2021, 42, 877–883. [Google Scholar] [PubMed]
- Teramoto, A.; Fujita, H.; Yamamuro, O.; Tamaki, T. Automated detection of pulmonary nodules in PET/CT images: Ensemble false-positive reduction using a convolutional neural network technique. Med. Phys. 2016, 43, 2821–2827. [Google Scholar] [CrossRef] [PubMed]
- Shichijo, S.; Endo, Y.; Aoyama, K.; Takeuchi, Y.; Ozawa, T.; Takiyama, H.; Matsuo, K.; Fujishiro, M.; Ishihara, S.; Ishihara, R.; et al. Application of convolutional neural networks for evaluating Helicobacter pylori infection status on the basis of endoscopic images. Scand. J. Gastroenterol. 2019, 54, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, Y.; Shen, Z.; Zhang, X.; Sang, J.; Ding, Y.; Yang, X.; Li, J.; Chen, M.; Jin, C.; et al. Convolutional neural network for the diagnosis of early gastric cancer based on magnifying narrow band imaging. Gastric Cancer. 2020, 23, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Hu, W.; Chen, F.; Liu, J.; Yang, Y.; Wang, L.; Duan, H.; Si, J. Gastric precancerous diseases classification using CNN with a concise model. PLoS ONE 2017, 12, e0185508. [Google Scholar] [CrossRef] [PubMed]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 2018, 21, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, Y.; Takemoto, S.; Hori, K.; Nishimura, M.; Ikematsu, H.; Yano, T.; Yokota, H. Automatic detection of early gastric cancer in endoscopic images using a transferring convolutional neural network. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 4138–4141. [Google Scholar]
- Shibata, T.; Teramoto, A.; Yamada, H.; Ohmiya, N.; Saito, K.; Fujita, H. Automated Detection and Segmentation of Early Gastric Cancer from Endoscopic Images Using Mask R-CNN. Appl. Sci. 2020, 10, 3842. [Google Scholar] [CrossRef]
- Yagi, K.; Nakamura, A.; Sekine, A. Characteristic endoscopic and magnified endoscopic findings in the normal stomach without Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2002, 17, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. Lect. Notes. Comput. Sci. 2015, 9351, 234–241. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2017, arXiv:1412.6980. [Google Scholar]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Efron, B. Estimating the error rate of a prediction rule: Improvement on cross-validation. J. Am. Stat. Assoc. 1983, 78, 316–331. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Cases |
|---|---|
| Tumor position | |
| Lower third | 33 |
| Middle third | 52 |
| Upper third | 9 |
| Macroscopic classification | |
| Type 0-I | 0 |
| Type 0-IIa | 10 |
| Type 0-IIb | 0 |
| Type 0-IIc | 63 |
| Type 0-III | 0 |
| Type 0 mixed (0-IIa + IIc and IIc + III) | 21 |
| Depth of tumor invasion | |
| T1a (mucosa) | 71 |
| T1b (submucosa) | 23 |
| Histopathological classification | |
| Undifferentiated | 13 |
| Differentiated | 75 |
| Mixed | 6 |
| Classifier | Detection Sensitivity | False Positives/Image | |
|---|---|---|---|
| Lesion-Based | Image-Based | ||
| None | 0.989 | 0.942 | 0.0348 |
| VGG16 | 0.989 | 0.942 | 0.0348 |
| ResNet50 | 0.989 | 0.932 | 0.0281 |
| DenseNet121 | 0.978 | 0.916 | 0.0273 |
| DenseNet169 | 0.989 | 0.897 | 0.0108 |
| DenseNet201 | 0.989 | 0.901 | 0.0240 |
| Evaluation Using All Gastric Cancer Cases | Evaluation Using the Detected Gastric Cancer Cases | |||
|---|---|---|---|---|
| Di | Ji | Di | Ji | |
| Previous method [16] | 0.542 | 0.371 | 0.720 | 0.494 |
| Proposed method | 0.555 | 0.427 | 0.602 | 0.463 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teramoto, A.; Shibata, T.; Yamada, H.; Hirooka, Y.; Saito, K.; Fujita, H. Automated Detection of Gastric Cancer by Retrospective Endoscopic Image Dataset Using U-Net R-CNN. Appl. Sci. 2021, 11, 11275. https://0-doi-org.brum.beds.ac.uk/10.3390/app112311275
Teramoto A, Shibata T, Yamada H, Hirooka Y, Saito K, Fujita H. Automated Detection of Gastric Cancer by Retrospective Endoscopic Image Dataset Using U-Net R-CNN. Applied Sciences. 2021; 11(23):11275. https://0-doi-org.brum.beds.ac.uk/10.3390/app112311275
Chicago/Turabian StyleTeramoto, Atsushi, Tomoyuki Shibata, Hyuga Yamada, Yoshiki Hirooka, Kuniaki Saito, and Hiroshi Fujita. 2021. "Automated Detection of Gastric Cancer by Retrospective Endoscopic Image Dataset Using U-Net R-CNN" Applied Sciences 11, no. 23: 11275. https://0-doi-org.brum.beds.ac.uk/10.3390/app112311275