
TNF-α, IL-1β, MMP-8 Crevicular Profile in Patients with Chronic Kidney Disease and Periodontitis


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Clinical Examination
2.4. Assessment of TNF-α, IL-1β, MMP-8 in the Crevicular Fluid
2.5. Statistical Analysis
3. Results
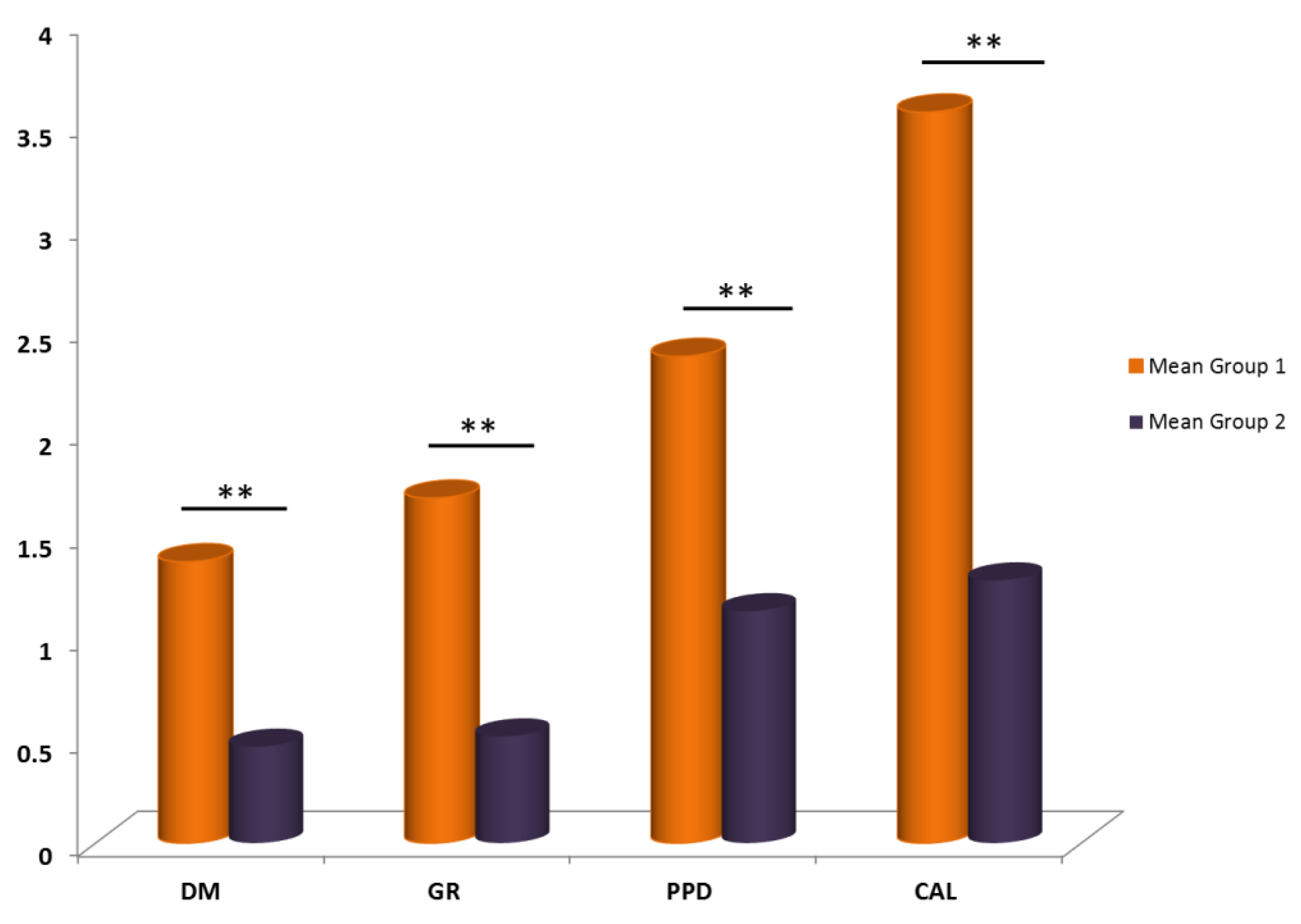
3.1. Periodontal Profile in the Study Groups
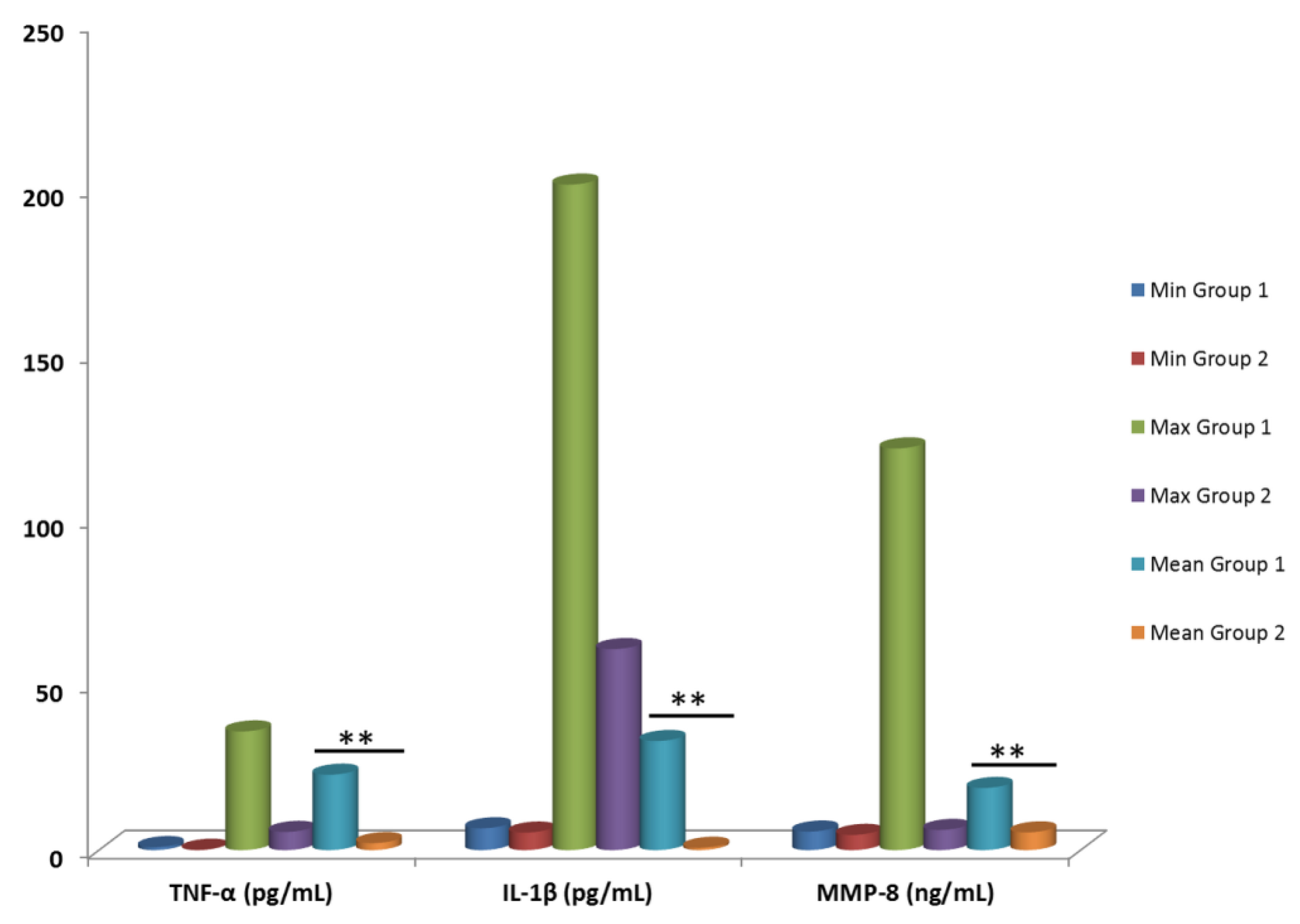
3.2. Local Oral Expression of TNF-α, IL-1β and MMP-8 Inflammatory Biomarkers in Gingival Fluid
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraser, S.D.; Blakeman, T. Chronic kidney disease: Identification and management in primary care. Pragmatic Obs. Res. 2016, 7, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, J.-C.; Zhang, L.-X. Prevalence and Disease Burden of Chronic Kidney Disease. Adv. Exp. Med. Biol. 2019, 1165, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Bello, A.K.; Alrukhaimi, M.; Ashuntantang, G.E.; Basnet, S.; Rotter, R.C.; Douthat, W.G.; Kazancıoğlu, R.T.; Köttgen, A.; Nangaku, M.; Powe, N.R.; et al. Complications of chronic kidney disease: Current state, knowledge gaps, and strategy for action. Kidney Int. Suppl. 2017, 7, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, J.; Herrlinger, S.; Pruy, A.; Metzger, T.; Wanner, C. Inflammation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int. 1999, 55, 648–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feghali, C.A.; Wright, T.M. Cytokines in acute and chronic inflammation. Front. Biosci. 1997, 2, 12–26. [Google Scholar]
- Sharma, P.; Fenton, A.; Dias, I.H.K.; Heaton, B.; Brown, C.L.R.; Sidhu, A.; Rahman, M.; Griffiths, H.R.; Cockwell, P.; Ferro, C.J.; et al. Oxidative stress links periodontal inflammation and renal function. J. Clin. Periodontol. 2021, 48, 357–367. [Google Scholar] [CrossRef]
- Anding, K.; Gross, P.; Rost, J.M.; Allgaier, D.; Jacobs, E. The influence of uraemia and haemodialysis on neutrophil phagocytosis and antimicrobial killing. Nephrol. Dial. Transplant. 2003, 18, 2067–2073. [Google Scholar] [CrossRef] [Green Version]
- Nassar, G.M. Preventing and Treating Inflammation: Role of Dialysis Access Management. Semin. Dial. 2012, 26, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Kantarci, A.; Hasturk, H.; Dyke, T.E. Host-mediated resolution of inflammation in periodontal diseases. Periodontol. 2000 2006, 40, 144–163. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Proença, L.; Bellini, D.H.; Chambrone, L.; Alcoforado, G.; Mendes, J.J. The impact of nonsurgical periodontal treatment on oral health-related quality of life: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 585–596. [Google Scholar] [CrossRef]
- Popova, C.; Dosseva-Panova, V.; Kisselova, A.; Panov, V.E. Subgingival microbiota in severe chronic periodon-titis. J. IMAB-Annu. Proc. Sci. Pap. 2014, 20, 554–557. [Google Scholar] [CrossRef] [Green Version]
- Garlet, G. Destructive and Protective Roles of Cytokines in Periodontitis: A Re-appraisal from Host Defense and Tissue Destruction Viewpoints. J. Dent. Res. 2010, 89, 1349–1363. [Google Scholar] [CrossRef]
- Miyata, Y.; Obata, Y.; Mochizuki, Y.; Kitamura, M.; Mitsunari, K.; Matsuo, T.; Ohba, K.; Mukae, H.; Nishino, T.; Yoshimura, A.; et al. Periodontal Disease in Patients Receiving Dialysis. Int. J. Mol. Sci. 2019, 20, 3805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapellas, K.; Singh, A.; Bertotti, M.; Nascimento, G.G.; Jamieson, L.M.; on behalf of the Perio-CKD collaboration. Periodontal and chronic kidney disease association: A systematic review and meta-analysis. Nephrology 2019, 24, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Deschamps-Lenhardt, S.; Martin-Cabezas, R.; Hannedouche, T.; Huck, O. Association between periodontitis and chronic kidney disease: Systematic review and meta-analysis. Oral Dis. 2018, 25, 385–402. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Narváez, R.V.; Valenzuela-Narváez, D.R.; Valenzuela-Narváez, D.; Córdova-Noel, M.E.; Mejía-Ruiz, C.L.; Salcedo-Rodríguez, M.N.; Gonzales-Aedo, O. Periodontal disease as a predictor of chronic kidney disease (CKD) stage in older adults. J. Int. Med. Res. 2021, 49, 3000605211033266. [Google Scholar] [CrossRef]
- Chambrone, L.; Foz, A.M.; Guglielmetti, M.R.; Pannuti, C.M.; Artese, H.; Feres, M.; Romito, G.A. Periodontitis and chronic kidney disease: A systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J. Clin. Periodontol. 2013, 40, 443–456. [Google Scholar] [CrossRef]
- Lertpimonchai, A.; Rattanasiri, S.; Tamsailom, S.; Champaiboon, C.; Ingsathit, A.; Kitiyakara, C.; Limpianunchai, A.; Attia, J.; Sritara, P.; Thakkinstian, A. Periodontitis as the risk factor of chronic kidney disease: Mediation analysis. J. Clin. Periodontol. 2019, 46, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Artese, H.; De Sousa, C.O.; Luiz, R.; Sansone, C.; Torres, M.C.M.D.B. Effect of non-surgical periodontal treatment on chronic kidney disease patients. Braz. Oral Res. 2010, 24, 449–454. [Google Scholar] [CrossRef]
- Borawski, J.; Wilczynska-Borawska, M.; Stokowska, W.; Mysliwiec, M.; Geelen, J.M.; van der Velden, T.J.A.M.; Loo, D.M.W.M.T.; Boerman, O.C.; Heuvel, L.P.W.J.V.D.; Monnens, L.A.H. The periodontal status of pre-dialysis chronic kidney disease and maintenance dialysis patients. Nephrol. Dial. Transplant. 2006, 22, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Cengiz, M.; Sümer, P.; Cengiz, S.; Yavuz, U. The effect of the duration of the dialysis in hemodialysis patients on dental and periodontal findings. Oral Dis. 2009, 15, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.A.; Taylor, G.W.; West, B.T.; McCarthy, E.T. Bidirectional relationship between chronic kidney and periodontal disease: A study using structural equation modeling. Kidney Int. 2011, 79, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vathesatogkit, P.; Woodward, M.; Tanomsup, S.; Ratanachaiwong, W.; Vanavanan, S.; Yamwong, S.; Sritara, P. Cohort Profile: The electricity generating authority of Thailand study. Int. J. Epidemiol. 2012, 41, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kshirsagar, A.V.; Moss, K.L.; Elter, J.R.; Beck, J.D.; Offenbacher, S.; Falk, R.J. Periodontal disease is associated with renal insufficiency in the Atherosclerosis Risk in Communities (ARIC) study. Am. J. Kidney Dis. 2005, 45, 650–657. [Google Scholar] [CrossRef]
- Ismail, G.; Dumitriu, H.T.; Dumitriu, A.S.; Ismail, F.B. Periodontal Disease: A Covert Source of Inflammation in Chronic Kidney Disease Patients. Int. J. Nephrol. 2013, 2013, 515796. [Google Scholar] [CrossRef]
- Liu, K.; Liu, Q.; Chen, W.; Liang, M.; Luo, W.; Wu, X.; Ruan, Y.; Wang, J.; Xu, R.; Zhan, X.; et al. Prevalence and Risk Factors of CKD in Chinese Patients with Periodontal Disease. PLoS ONE 2013, 8, e70767. [Google Scholar] [CrossRef] [Green Version]
- Ruospo, M.; Palmer, S.C.; Craig, J.; Gentile, G.; Johnson, D.W.; Ford, P.; Tonelli, M.; Petruzzi, M.; De Benedittis, M.; Strippoli, G.F. Prevalence and severity of oral disease in adults with chronic kidney disease: A systematic review of observational studies. Nephrol. Dial. Transplant. 2013, 29, 364–375. [Google Scholar] [CrossRef]
- Grubbs, V.; Vittinghoff, E.; Taylor, G.; Kritz-Silverstein, D.; Powe, N.; Bibbins-Domingo, K.; Ishani, A.; Cummings, S.R.; Osteoporotic Fractures in Men (MrOS) Study Research Group. The association of periodontal disease with kidney function decline: A longitudinal retrospective analysis of the MrOS dental study. Nephrol. Dial. Transplant. 2016, 31, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Nylund, K.M.; Meurman, J.H.; Heikkinen, A.M.; Honkanen, E.; Vesterinen, M.; Furuholm, J.O.; Tervahartiala, T.; Sorsa, T.; Ruokonen, H.M. Periodontal inflammatory burden and salivary matrix metalloproteinase-8 concentration among patients with chronic kidney sisease at the predialysis stage. J. Periodontol. 2015, 86, 1212–1220. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions-Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- Shulman, J.D.; Cappelli, D.P. Epidemiology of Dental Caries. In Prevention in Clinical Oral Health Care; Capelli, D.P., Mobley, C.C., Eds.; Mosby: Maryland Heights, MO, USA, 2008; pp. 2–13. [Google Scholar]
- Fisher, M.A.; Borgnakke, W.; Taylor, G.W. Periodontal disease as a risk marker in coronary heart disease and chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2010, 19, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, M.; Mochizuki, Y.; Miyata, Y.; Obata, Y.; Mitsunari, K.; Matsuo, T.; Ohba, K.; Mukae, H.; Yoshimura, A.; Nishino, T.; et al. Pathological Characteristics of Periodontal Disease in Patients with Chronic Kidney Disease and Kidney Transplantation. Int. J. Mol. Sci. 2019, 20, 3413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricardo, A.C.; Goh, V.; Chen, J.; Cedillo-Couvert, E.; Kapella, M.; Prasad, B.; Parvathaneni, S.; Knutson, K.; Lash, J.P. Association of Sleep Duration, Symptoms, and Disorders with Mortality in Adults with Chronic Kidney Disease. Kidney Int. Rep. 2017, 2, 866–873. [Google Scholar] [CrossRef] [Green Version]
- Locksley, R.M.; Killeen, N.; Lenardo, M.J. The TNF and TNF Receptor Superfamilies: Integrating Mammalian Biology. Cell 2001, 104, 487–501. [Google Scholar] [CrossRef] [Green Version]
- Bennett, J.M.; Reeves, G.; Billman, G.E.; Sturmberg, J.P. Inflammation-nature’s way to efficiently respond to all types of challenges: Implications for understanding and managing "the epidemic" of chronic diseases. Front. Med. (Lausanne) 2018, 5, 316. [Google Scholar] [CrossRef] [Green Version]
- Varfolomeev, E.; Vucic, D. Intracellular regulation of TNF activity in health and disease. Cytokine 2018, 101, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Dostert, C.; Grusdat, M.; Letellier, E.; Brenner, D. The TNF Family of Ligands and Receptors: Communication Modules in the Immune System and Beyond. Physiol. Rev. 2019, 99, 115–160. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef] [Green Version]
- Dinarello, C.A. Overview of the IL-1 family in innate inflammation and acquired immunity. Immunol. Rev. 2018, 281, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Laronha, H.; Caldeira, J. Structure and Function of Human Matrix Metalloproteinases. Cells 2020, 9, 1076. [Google Scholar] [CrossRef] [PubMed]
- Egido, J.; Gómez-Chiarri, M.; Ortíz, A.; Bustos, C.; Alonso, J.; Gómez-Guerrero, C.; Gómez-Garre, D.; López-Armada, M.J.; Plaza, J.; Gonzalez, E. Role of tumor necrosis factor-alpha in the pathogenesis of glomerular diseases. Kidney Int. Suppl. 1993, 39, S59–S64. [Google Scholar] [PubMed]
- Nilsson, L.; Szymanowski, A.; Swahn, E.; Jonasson, L. Soluble TNF Receptors Are Associated with Infarct Size and Ventricular Dysfunction in ST-Elevation Myocardial Infarction. PLoS ONE 2013, 8, e55477. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Hennekens, C.H.; Buring, J.E.; Rifai, N. C-Reactive Protein and Other Markers of Inflammation in the Prediction of Cardiovascular Disease in Women. N. Engl. J. Med. 2000, 342, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.P.; Pais, P.; Moulder, J.E. Chronic Kidney Disease After Hematopoietic Stem Cell Transplantation. Semin. Nephrol. 2010, 30, 627–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niedzielska, I.; Chudek, J.; Kowol, I.; Slabiak-Blaz, N.; Kolonko, A.; Kuczera, P.; Wiecek, A. The odontogenic-related microinflammation in patients with chronic kidney disease. Ren. Fail. 2014, 36, 883–888. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.; Vallance, P.; Deanfield, J. Treatment of Periodontitis and Endothelial Function. N. Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, F.; Wu, B.; Qu, Q.; Gao, J.; Yan, W.; Huang, X.; Ma, D.; Yue, J.; Chen, T.; Liu, F.; et al. The clinical response and systemic effects of non-surgical periodontal therapy in end-stage renal disease patients: A 6-month randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Ikezawa, I.; Tai, H.; Shimada, Y.; Komatsu, Y.; Galicia, J.C.; Yoshie, H. Imbalance between soluble tumour necrosis factor receptors type 1 and 2 in chronic periodontitis. J. Clin. Periodontol. 2005, 32, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Teles, R.; Sakellari, D.; Teles, F.; Konstantinidis, A.; Kent, R.; Socransky, S.; Haffajee, A. Relationships Among Gingival Crevicular Fluid Biomarkers, Clinical Parameters of Periodontal Disease, and the Subgingival Microbiota. J. Periodontol. 2010, 81, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Gokul, K.; Faizuddin, M.; Pradeep, A.R. Estimation of the level of tumor necrosis factor- α in gingival crevicular fluid and serum in periodontal health & disease: A biochemical study. Indian J. Dent. Res. 2012, 23, 348–352. [Google Scholar] [PubMed]
- Reis, C.; Da Costa, A.V.; Guimarães, J.T.; Tuna, D.; Braga, A.C.; Pacheco, J.J.; Arosa, F.A.; Salazar, F.; Cardoso, E.M. Clinical improvement following therapy for periodontitis: Association with a decrease in IL-1 and IL-6. Exp. Ther. Med. 2014, 8, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.B. Dysregulated Phosphate Metabolism, Periodontal Disease, and Cancer: Possible Global Health Implications. Dent. J. 2019, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Dağ, A.; Fırat, E.T.; Kadiroğlu, A.K.; Kale, E.; Yılmaz, M.E. Significance of elevated gingival crevicular fluid tumor necrosis factor-α and interleukin-8 levels in chronic hemodialysis patients with periodontal disease. J. Periodontal Res. 2010, 45, 445–450. [Google Scholar] [CrossRef]
- Kimmel, P.L.; Phillips, T.M.; Simmens, S.J.; Peterson, R.A.; Weihs, K.L.; Alleyne, S.; Cruz, I.; Yanovski, J.; Veis, J.H. Immunologic function and survival in hemodialysis patients. Kidney Int. 1998, 54, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balakrishnan, V.S.; Guo, D.; Rao, M.; Jaber, B.L.; Tighiouart, H.; Freeman, R.L.; Huang, C.; King, A.J.; Pereira, B.J.; the HEMO Study Group. Cytokine gene polymorphisms in hemodialysis patients: Association with comorbidity, functionality, and serum albumin. Kidney Int. 2004, 65, 1449–1460. [Google Scholar] [CrossRef] [Green Version]
- Biasucci, L.M.; Liuzzo, G.; Fantuzzi, G.; Caligiuri, G.; Rebuzzi, A.G.; Ginnetti, F.; Dinarello, C.A.; Maseri, A. Increasing Levels of Interleukin (IL)-1Ra and IL-6 During the First 2 Days of Hospitalization in Unstable Angina Are Associated with Increased Risk of In-Hospital Coronary Events. Circulation 1999, 99, 2079–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangarao, S.; Govindarajan, K.; Muthukumar, S. Relationship between interleukin 1α levels in the gingival crevicular fluid in health and in inflammatory periodontal disease and periodontal inflamed surface area: A correlative study. J. Indian Soc. Periodontol. 2015, 19, 618–623. [Google Scholar] [CrossRef]
- Chaudhari, A.U.; Byakod, G.N.; Waghmare, P.F.; Karhadkar, V.M. Correlation of Levels of Interleukin-1β in Gingival Crevicular Fluid to the Clinical Parameters of Chronic Periodontitis. J. Contemp. Dent. Pr. 2011, 12, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Becerik, S.; Öztürk, V.; Özgen; Atmaca, H.; Atilla, G.; Emingil, G. Gingival Crevicular Fluid and Plasma Acute-Phase Cytokine Levels in Different Periodontal Diseases. J. Periodontol. 2012, 83, 1304–1313. [Google Scholar] [CrossRef] [PubMed]
- Ertugrul, A.S.; Sahin, H.; Dikilitas, A.; Alpaslan, N.; Bozoglan, A. Comparison of CCL28, interleukin-8, interleukin-1β and tumor necrosis factor-alpha in subjects with gingivitis, chronic periodontitis and generalized aggressive periodontitis. J. Periodontal Res. 2013, 48, 44–51. [Google Scholar] [CrossRef]
- Fujita, Y.; Ito, H.; Sekino, S.; Numabe, Y. Correlations between pentraxin 3 or cytokine levels in gingival crevicular fluid and clinical parameters of chronic periodontitis. Odontology 2011, 100, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.P.; Faveri, M.; Gursky, L.C.; Mestnik, M.J.; Feres, M.; Haffajee, A.D.; Socransky, S.S.; Teles, R.P. Effects of periodontal therapy on GCF cytokines in generalized aggressive periodontitis subjects. J. Clin. Periodontol. 2011, 39, 295–302. [Google Scholar] [CrossRef]
- Ülker, A.E.; Tulunoglu, O.; Özmeriç, N.; Can, M.; Demirtaş, S. The Evaluation of Cystatin C, IL-1β, and TNF-α Levels in Total Saliva and Gingival Crevicular Fluid From 11- to 16-Year-Old Children. J. Periodontol. 2008, 79, 854–860. [Google Scholar] [CrossRef]
- Ma, X.; Wang, Y.; Wu, H.; Li, F.; Feng, X.; Xie, Y.; Xie, D.; Wang, W.; Lo, E.C.M.; Lu, H. Periodontal health related–inflammatory and metabolic profiles of patients with end-stage renal disease: Potential strategy for predictive, preventive, and personalized medicine. EPMA J. 2021, 12, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Hasty, K.A.; Pourmotabbed, T.F.; Goldberg, G.I.; Thompson, J.P.; Spinella, D.G.; Stevens, R.M.; Mainardi, C.L. Human neutrophil collagenase. A distinct gene product with homology to other matrix metalloproteinases. J. Biol. Chem. 1990, 265, 11421–11424. [Google Scholar] [CrossRef]
- Balbín, M.; Fueyo-Silva, A.; Knauper, V.; Pendas, A.M.; López, J.M.; Jiménez, M.G.; Murphy, G.; López-Otín, C. Collagenase 2 (MMP-8) Expression in Murine Tissue-remodeling Processes. Analysis of its potential role in postpartum involution of the uterus. J. Biol. Chem. 1998, 273, 23959–23968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herman, M.P.; Sukhova, G.K.; Libby, P.; Gerdes, N.; Tang, N.; Horton, D.B.; Kilbride, M.; Breitbart, R.E.; Chun, M.; Schönbeck, U. Expression of neutrophil collagenase (matrix metalloproteinase-8) in human atheroma: A novel collagenolytic pathway suggested by transcriptional profiling. Circulation 2001, 104, 1899–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirilä, E.; Sharabi, A.; Salo, T.; Quaranta, V.; Tu, H.; Heljasvaara, R.; Koshikawa, N.; Sorsa, T.; Maisi, P. Matrix metalloproteinases process the laminin-5 gamma 2-chain and regulate epithelial cell migration. Biochem. Biophys. Res. Commun. 2003, 303, 1012–1017. [Google Scholar] [CrossRef]
- Basu, R.K.; Donaworth, E.; Siroky, B.; Devarajan, P.; Wong, H.R. Loss of matrix metalloproteinase-8 is associated with worsened recovery after ischemic kidney injury. Ren. Fail. 2015, 37, 469–475. [Google Scholar] [CrossRef] [Green Version]
- van der Zijl, N.J.; Hanemaaijer, R.; Tushuizen, M.E.; Schindhelm, R.K.; Boerop, J.; Rustemeijer, C.; Bilo, H.J.; Verheijen, J.H.; Diamant, M. Urinary matrix metalloproteinase-8 and -9 activities in type 2 diabetic subjects: A marker of incipient diabetic nephropathy? Clin. Biochem. 2010, 43, 635–639. [Google Scholar] [CrossRef]
- Golub, L.M.; Lee, H.M.; Stoner, J.A.; Sorsa, T.; Reinhardt, R.A.; Wolff, M.S.; Ryan, M.E.; Nummikoski, P.V.; Payne, J.B. Subantimicrobial-Dose Doxycycline Modulates Gingival Crevicular Fluid Biomarkers of Periodontitis in Postmenopausal Osteopenic Women. J. Periodontol. 2008, 79, 1409–1418. [Google Scholar] [CrossRef] [Green Version]
- Nizam, N.; Gümüş, P.; Pitkänen, J.; Tervahartiala, T.; Sorsa, T.; Buduneli, N. Serum and Salivary Matrix Metalloproteinases, Neutrophil Elastase, Myeloperoxidase in Patients with Chronic or Aggressive Periodontitis. Inflammation 2014, 37, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Miralda, I.; Uriarte, S.M. Periodontal Pathogens’ strategies disarm neutrophils to promote dysregulated inflammation. Mol. Oral Microbiol. 2021, 36, 103–120. [Google Scholar] [CrossRef] [PubMed]
- Mäntylä, P.; Stenman, M.; Kinane, D.F.; Tikanoja, S.; Luoto, H.; Salo, T.; Sorsa, T. Gingival crevicular fluid collagenase-2 (MMP-8) test stick for chair-side monitoring of periodontitis. J. Periodontal Res. 2003, 38, 436–439. [Google Scholar] [CrossRef]
- Konopka, Ł.; Pietrzak, A.; Brzezińska-Błaszczyk, E. Effect of scaling and root planing on interleukin-1β, interleukin-8 and MMP-8 levels in gingival crevicular fluid from chronic periodontitis patients. J. Periodontal Res. 2012, 47, 681–688. [Google Scholar] [CrossRef]
- Rai, B.; Kaur, J.; Jain, R.; Anand, S.C. Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. Saudi Dent. J. 2010, 22, 129–131. [Google Scholar] [CrossRef] [Green Version]
- Leppilahti, J.M.; Hernández-Ríos, P.A.; Gamonal, J.A.; Tervahartiala, T.; Brignardello-Petersen, R.; Mäntylä, P.; Sorsa, T.; Hernández, M. Matrix metalloproteinases and myeloperoxidase in gingival crevicular fluid provide site-specific diagnostic value for chronic periodontitis. J. Clin. Periodontol. 2013, 41, 348–356. [Google Scholar] [CrossRef]
- Yakob, M.; Kari, K.; Tervahartiala, T.; Sorsa, T.; Söder, P.O.; Meurman, J.H.; Söder, B. Associations of periodontal microorganisms with salivary proteins and MMP-8 in gingival crevicular fluid. J. Clin. Periodontol. 2011, 39, 256–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yakob, M.; Meurman, J.H.; Sorsa, T.; Söder, B. Treponema denticola associates with increased levels of MMP-8 and MMP-9 in gingival crevicular fluid. Oral Dis. 2013, 19, 694–701. [Google Scholar] [CrossRef]
- Machowska, A.; Carrero, J.J.; Lindholm, B.; Stenvinkel, P. Therapeutics targeting persistent inflammation in chronic kidney disease. Transl. Res. 2016, 167, 204–213. [Google Scholar] [CrossRef]
- Atarashi, K.; Suda, W.; Luo, C.; Kawaguchi, T.; Motoo, I.; Narushima, S.; Kiguchi, Y.; Yasuma, K.; Watanabe, E.; Tanoue, T.; et al. Ectopic colonization of oral bacteria in the intestine drives T H 1 cell induction and inflammation. Science 2017, 358, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Tomofuji, T.; Ekuni, D.; Yamanaka, R.; Kusano, H.; Azuma, T.; Sanbe, T.; Tamaki, N.; Yamamoto, T.; Watanabe, T.; Miyauchi, M.; et al. Chronic Administration of Lipopolysaccharide and Proteases Induces Periodontal Inflammation and Hepatic Steatosis in Rats. J. Periodontol. 2007, 78, 1999–2006. [Google Scholar] [CrossRef]
- Nakajima, M.; Arimatsu, K.; Kato, T.; Matsuda, Y.; Minagawa, T.; Takahashi, N.; Ohno, H.; Yamazaki, K. Oral Administration of P. gingivalis Induces Dysbiosis of Gut Microbiota and Impaired Barrier Function Leading to Dissemination of Enterobacteria to the Liver. PLoS ONE 2015, 10, e0134234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.W.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olteanu, M.; Surlin, P.; Oprea, B.; Rauten, A.M.; Popescu, R.M.; Niţu, M.; Camen, G.C.; Caraivan, O. Gingival inflammatory infiltrate analysis in patients with chronic periodontitis and diabetes mellitus. Romanian J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2011, 52, 1311–1317. [Google Scholar]
- Kc, S.; Wang, X.Z.; Gallagher, J.E. Diagnostic sensitivity and specificity of host-derived salivary biomarkers in periodontal disease amongst adults: Systematic review. J. Clin. Periodontol. 2019, 47, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Șurlin, P.; Camen, A.; Stratul, S.I.; Roman, A.; Gheorghe, D.-N.; Herăscu, E.; Osiac, E.; Rogoveanu, I. Optical coherence tomography assessment of gingival epithelium inflammatory status in periodontal—Systemic affected patients. Ann. Anat.-Anat. Anz. 2018, 219, 51–56. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Group 1 (n = 59) | Group 2 (n = 20) |
|---|---|---|
| Age (mean ± SD) | 58.56 ± 14.00 | 35.25 ± 9.28 |
| Gender (#, %) | ||
| Female | 28 (47.40) | 16 (80.00) |
| Male | 31 (52.60) | 4 (20.00) |
| Environment (#, %) | ||
| Urban | 12 (30.40) | 19 (95.00) |
| Rural | 47 (79.60) | 1 (5.00) |
| DM (mean) | 1.37 | 0.47 |
| Bleeding on probing (#, %) | 49 (83.05) | 15 (75.00) |
| Gingival edema (#, %) | 31 (52.54) | 6 (30.00) |
| GR (mean, mm) | 1.68 | 0.52 |
| PPD (mean, mm) | 2.37 | 1.13 |
| CAL (mean, mm) | 3.56 | 1.28 |
| Periodontitis stage (#, %) | ||
| Mild stage | 3 (5.08) | 7 (35.00) |
| Moderate stage | 10 (16.94) | 5 (25.00) |
| Severe stage | 46 (77.96) | 8 (40.00) |
| Periodontitis Staging | DM (Mean Value) | GR (Mean Value, mm) | PPD (Mean Value, mm) | CAL (Mean Value, mm) |
|---|---|---|---|---|
| Stage 1 (mild) n = 3 | 1.51 | 0.98 | 1.21 | 0.20 |
| Stage 2 (moderate) n = 10 | 1.06 | 1.45 | 2.08 | 1.33 |
| Stage 3–4 (severe) n = 46 | 1.38 | 1.80 | 2.68 | 4.65 |
| Periodontitis Staging | DM (Mean Value) | GR (Mean Value, mm) | PPD (Mean Value, mm) | CAL (Mean Value, mm) |
|---|---|---|---|---|
| Stage 1 (mild) n = 7 | 0.54 | 0.82 | 1.32 | 0.61 |
| Stage 2 (moderate) n = 5 | 0.40 | 0.34 | 1.28 | 1.09 |
| Stage 3–4 (severe) n = 8 | 0.44 | 0.38 | 0.93 | 1.78 |
| Values | TNF-α (pg/mL) | IL-1β (pg/mL) | MMP-8 (ng/mL) | |||
|---|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 1 | Group 2 | Group 1 | Group 2 | |
| Minimum | 0.90 | 0.10 | 6.60 | 5.30 | 5.60 | 4.60 |
| Mean | 22.80 | 2.10 | 33.00 | 0.71 | 18.80 | 5.35 |
| Maximum | 35.90 | 5.50 | 201.30 | 60.80 | 121.50 | 6.10 |
| Periodontitis Staging | TNF-α (pg/mL) | IL-1β (pg/mL) | MMP-8 (ng/mL) | |||
|---|---|---|---|---|---|---|
| Mean Values | ||||||
| Group 1 | Group 2 | Group 1 | Group 2 | Group 1 | Group 2 | |
| Stage 1 (mild) | 27.40 | 2.10 | 30.30 | 10.70 | 7.70 | 5.50 |
| Stage 2 (moderate) | 23.50 | 2.00 | 39.15 | 14.40 | 32.65 | 5.70 |
| Stage 3–4 (severe) | 22.55 | 2.15 | 29.40 | 9.25 | 18.35 | 5.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andronovici, A.M.; Caruntu, I.-D.; Onofriescu, M.; Hurjui, L.L.; Giusca, S.-E.; Covic, A.S.; Braescu, R.; Foia, L.-G. TNF-α, IL-1β, MMP-8 Crevicular Profile in Patients with Chronic Kidney Disease and Periodontitis. Appl. Sci. 2022, 12, 736. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020736
Andronovici AM, Caruntu I-D, Onofriescu M, Hurjui LL, Giusca S-E, Covic AS, Braescu R, Foia L-G. TNF-α, IL-1β, MMP-8 Crevicular Profile in Patients with Chronic Kidney Disease and Periodontitis. Applied Sciences. 2022; 12(2):736. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020736
Chicago/Turabian StyleAndronovici, Alina Maria, Irina-Draga Caruntu, Mihai Onofriescu, Loredana Liliana Hurjui, Simona-Eliza Giusca, Andreea Simona Covic, Radu Braescu, and Liliana-Georgeta Foia. 2022. "TNF-α, IL-1β, MMP-8 Crevicular Profile in Patients with Chronic Kidney Disease and Periodontitis" Applied Sciences 12, no. 2: 736. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020736