
Is Diffusion Tensor Imaging-Guided Radiotherapy the New State-of-the-Art? A Review of the Current Literature and Technical Insights

 , ,
, ,
Abstract
:1. Introduction
1.1. Intracranial Radiotherapy
1.2. Diffusion Tensor Imaging
2. Review Aims and Objectives
3. Review Results
3.1. Virtual Dissection of Eloquent WM Tracts
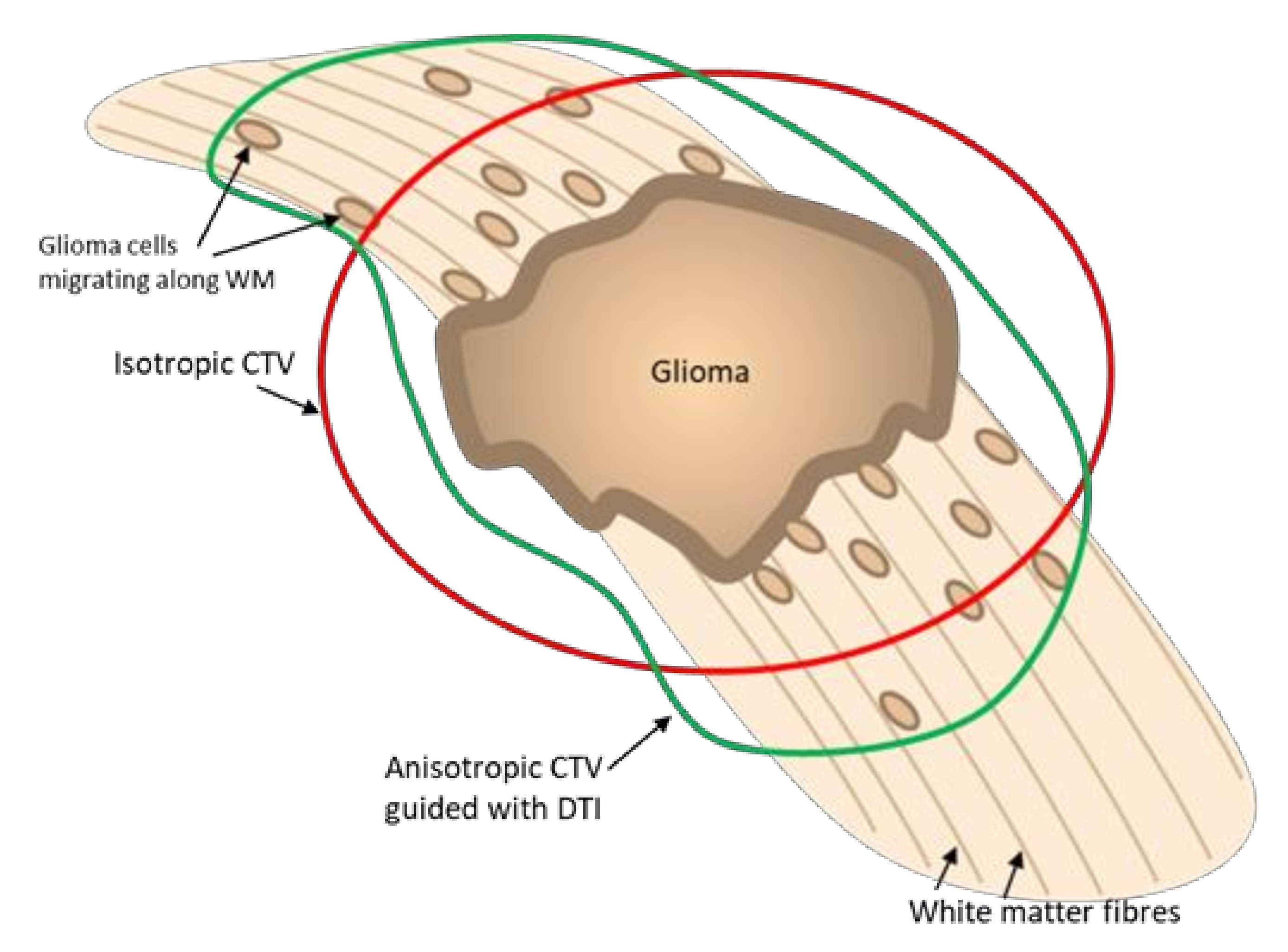
3.2. DTI Modelled Tumoral Invasion
3.3. Applications in Gliomas
3.4. Applications in Brain Metastases
3.5. Application in Benign Conditions
3.6. Future Considerations
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Halasz, L.M.; Rockhill, J.K. Stereotactic radiosurgery and stereotactic radiotherapy for brain metastases. Surg. Neurol. Int. 2013, 4, S185. [Google Scholar] [CrossRef] [PubMed]
- Niyazi, M.; Brada, M.; Chalmers, A.J.; Combs, S.E.; Erridge, S.C.; Fiorentino, A.; Grosu, A.L.; Lagerwaard, F.J.; Minniti, G.; Mirimanoff, R.O.; et al. ESTRO-ACROP guideline “target delineation of glioblastomas”. Radiother. Oncol. 2016, 118, 35–42. [Google Scholar] [CrossRef]
- Taylor, A.; Powell, M.E.B. Intensity-modulated radiotherapy—What is it? Cancer Imaging 2004, 4, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamalui-Hunter, M.; Yaddanapudi, S.; Zhao, T.; Mutic, S.; Low, D.A.; Drzymala, R.E. Patient-specific independent 3D GammaPlan quality assurance for Gamma Knife Perfexion radiosurgery. J. Appl. Clin. Med. Phys. 2013, 14, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Burnet, N.G.; Thomas, S.J.; Burton, K.E.; Jefferies, S.J. Defining the tumour and target volumes for radiotherapy. Cancer Imaging 2004, 4, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, C.L.; Gyato, K.; Awadalla, A.W.; Lustig, R.; Tochner, Z.A. A Critical Review of the Clinical Effects of Therapeutic Irradiation Damage to the Brain: The Roots of Controversy. Neuropsychol. Rev. 2004, 14, 65–86. [Google Scholar] [CrossRef]
- Dhermain, F.; Barani, I.J. Complications from radiotherapy. Handb. Clin. Neurol. 2016, 134, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.H.; Zhu, T.; Nazem-Zadeh, M.; Tao, Y.; Buchtel, H.A.; Tsien, C.I.; Lawrence, T.S.; Cao, Y. Diffusion tensor imaging predicts cognitive function change following partial brain radiotherapy for low-grade and benign tumors. Radiother. Oncol. 2016, 120, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Altabella, L.; Broggi, S.; Mangili, P.; Conte, G.M.; Pieri, V.; Iadanza, A.; del Vecchio, A.; Anzalone, N.; di Muzio, N.; Calandrino, R.; et al. Integration of Diffusion Magnetic Resonance Tractography into tomotherapy radiation treatment planning for high-grade gliomas. Phys. Med. 2018, 55, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Price, S.J.; Gillard, J.H. Imaging biomarkers of brain tumour margin and tumour invasion. Br. J. Radiol. 2011, 84, S159. [Google Scholar] [CrossRef] [Green Version]
- Trip, A.K.; Jensen, M.B.; Kallehauge, J.F.; Lukacova, S. Individualizing the radiotherapy target volume for glioblastoma using DTI-MRI: A phase 0 study on coverage of recurrences. Acta Oncol. 2019, 58, 1532–1535. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Westin, C.-F. An introduction to diffusion tensor image analysis. Neurosurg. Clin. N. Am. 2011, 22, 185. [Google Scholar] [CrossRef] [Green Version]
- Peña, A.; Green, H.A.L.; Carpenter, T.A.; Price, S.J.; Pickard, J.D.; Gillard, J.H. Enhanced visualization and quantification of magnetic resonance diffusion tensor imaging using the p:q tensor decomposition. Br. J. Radiol. 2014, 79, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Razek, A.A.K.A.; El-Serougy, L.; Abdelsalam, M.; Gaballa, G.; Talaat, M. Differentiation of residual/recurrent gliomas from postradiation necrosis with arterial spin labeling and diffusion tensor magnetic resonance imaging-derived metrics. Neuroradiology 2018, 60, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Rahmat, R.; Brochu, F.; Li, C.; Sinha, R.; Price, S.J.; Jena, R. Semi-automated construction of patient individualised clinical target volumes for radiotherapy treatment of glioblastoma utilising diffusion tensor decomposition maps. Br. J. Radiol. 2020, 93, 93. [Google Scholar] [CrossRef] [PubMed]
- Thong, P.M.; Duc, N.M. The Role of Apparent Diffusion Coefficient in the Differentiation between Cerebellar Medulloblastoma and Brainstem Glioma. Neurol. Int. 2020, 12, 34–40. [Google Scholar] [CrossRef]
- Duc, N.M. The role of diffusion tensor imaging metrics in the discrimination between cerebellar medulloblastoma and brainstem glioma. Pediatr. Blood Cancer 2020, 67, e28468. [Google Scholar] [CrossRef]
- Essayed, W.I.; Zhang, F.; Unadkat, P.; Cosgrove, G.R.; Golby, A.J.; O’Donnell, L.J. White matter tractography for neurosurgical planning: A topography-based review of the current state of the art. NeuroImage Clin. 2017, 15, 659–672. [Google Scholar] [CrossRef]
- Yahya, N.; Manan, H.A. Utilisation of Diffusion Tensor Imaging in Intracranial Radiotherapy and Radiosurgery Planning for White Matter Dose Optimization: A Systematic Review. World Neurosurg. 2019, 130, e188–e198. [Google Scholar] [CrossRef]
- Gavin, C.G.; Sabin, H.I. Stereotactic diffusion tensor imaging tractography for Gamma Knife radiosurgery. J. Neurosurg. 2016, 125, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, K.; Matsumoto, M.; Kase, M.; Nagano, O.; Aoyagi, K.; Kageyama, T. Quantification of the radiation dose to the pyramidal tract using tractography in treatment planning for stereotactic radiosurgery. Radiol. Phys. Technol. 2017, 10, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koga, T.; Shin, M.; Maruyama, K.; Kamada, K.; Ota, T.; Itoh, D.; Kunii, N.; Ino, K.; Aoki, S.; Masutani, Y.; et al. Integration of Corticospinal Tractography Reduces Motor Complications After Radiosurgery. Int. J. Radiat. Oncol. 2012, 83, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Qu, B.; Wang, J.; Ju, Z.; Zhang, Z.; Cui, Z.; Jack, Y.; Ling, Z.; Yu, X.; Pan, L. Integration of Functional MRI and White Matter Tractography in CyberKnife Radiosurgery. Technol. Cancer Res. Treat. 2017, 16, 850–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berberat, J.; McNamara, J.; Remonda, L.; Bodis, S.; Rogers, S. Diffusion tensor imaging for target volume definition in glioblastoma multiforme. Strahlenther. Onkol. 2014, 190, 939–943. [Google Scholar] [CrossRef]
- Hathout, L.; Patel, V.; Wen, P. A 3-dimensional DTI MRI-based model of GBM growth and response to radiation therapy. Int. J. Oncol. 2016, 49, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- Jordan, K.; Morin, O.; Wahl, M.; Amirbekian, B.; Chapman, C.; Owen, J.; Mukherjee, P.; Braunstein, S.; Henry, R. An Open-Source Tool for Anisotropic Radiation Therapy Planning in Neuro-oncology Using DW-MRI Tractography. Front. Oncol. 2019, 9, 810. [Google Scholar] [CrossRef] [PubMed]
- Metz, M.-C.; Molina-Romero, M.; Lipkova, J.; Gempt, J.; Liesche-Starnecker, F.; Eichinger, P.; Grundl, L.; Menze, B.; Combs, S.E.; Zimmer, C.; et al. Predicting Glioblastoma Recurrence from Preoperative MR Scans Using Fractional-Anisotropy Maps with Free-Water Suppression. Cancers 2020, 12, 728. [Google Scholar] [CrossRef] [Green Version]
- Peeken, J.C.; Molina-Romero, M.; Diehl, C.; Menze, B.H.; Straube, C.; Meyer, B.; Zimmer, C.; Wiestler, B.; Combs, S.E. Deep learning derived tumor infiltration maps for personalized target definition in Glioblastoma radiotherapy. Radiother. Oncol. 2019, 138, 166–172. [Google Scholar] [CrossRef]
- Igaki, H.; Sakumi, A.; Mukasa, A.; Saito, K.; Kunimatsu, A.; Masutani, Y.; Hanakita, S.; Ino, K.; Haga, A.; Nakagawa, K.; et al. Corticospinal tract-sparing intensity-modulated radiotherapy treatment planning. Rep. Pr. Oncol. Radiother. 2014, 19, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Conti, A.; Pontoriero, A.; Ricciardi, G.K.; Granata, F.; Vinci, S.; Angileri, F.F.; Pergolizzi, S.; Alafaci, C.; Rizzo, V.; Quartarone, A.; et al. Integration of functional neuroimaging in CyberKnife radiosurgery: Feasibility and dosimetric results. Neurosurg. Focus 2013, 34, E5. [Google Scholar] [CrossRef] [Green Version]
- Koga, T.; Maruyama, K.; Kamada, K.; Ota, T.; Shin, M.; Itoh, D.; Kunii, N.; Ino, K.; Terahara, A.; Aoki, S.; et al. Outcomes of Diffusion Tensor Tractography–Integrated Stereotactic Radiosurgery. Int. J. Radiat. Oncol. 2012, 82, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Mair, D.B.; Ames, H.M.; Li, R. Mechanisms of invasion and motility of high-grade gliomas in the brain. Mol. Biol. Cell 2018, 29, 2509–2515. [Google Scholar] [CrossRef]
- Engwer, C.; Hillen, T.; Knappitsch, M.; Surulescu, C. Glioma follow white matter tracts: A multiscale DTI-based model. J. Math. Biol. 2014, 71, 551–582. [Google Scholar] [CrossRef]
- Lu, S.; Ahn, D.; Johnson, G.; Law, M.; Zagzag, D.; Grossman, R.I. Diffusion-Tensor MR Imaging of Intracranial Neoplasia and Associated Peritumoral Edema: Introduction of the Tumor Infiltration Index. Radiology 2004, 232, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Randall, J.W.; Elhalawani, H.; Al Feghali, K.A.; Elliott, A.M.; Anderson, B.M.; Lacerda, L.; Tran, B.L.; Mohamed, A.S.; Brock, K.K.; et al. Detection of Glioblastoma Subclinical Recurrence Using Serial Diffusion Tensor Imaging. Cancers 2020, 12, 568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlisa, G.; Rados, M.; Pavlisa, G.; Pavic, L.; Potocki, K.; Mayer, D. The differences of water diffusion between brain tissue infiltrated by tumor and peritumoral vasogenic edema. Clin. Imaging 2009, 33, 96–101. [Google Scholar] [CrossRef]
- Eichler, A.F.; Chung, E.; Kodack, D.P.; Loeffler, J.S.; Fukumura, D.; Jain, R.K. The biology of brain metastases—Translation to new therapies. Nat. Rev. Clin. Oncol. 2011, 8, 344. [Google Scholar] [CrossRef] [Green Version]
- Predicting Sites of Tumour Progression in the Invasive Margin of Glioblastomas (PRaM-GBM Study)—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03294434 (accessed on 6 October 2021).
- Zakaria, H.; Haider, S.; Lee, I. Automated Whole Brain Tractography Affects Preoperative Surgical Decision Making. Cureus 2017, 9, e1656. [Google Scholar] [CrossRef] [Green Version]
- Perez, J.; Mazo, C.; Trujillo, M.; Herrera, A. MRI and CT Fusion in Stereotactic Electroencephalography: A Literature Review. Appl. Sci. 2021, 11, 5524. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Type of Study | Number of Subjects | Summary | Main Outcomes |
|---|---|---|---|---|
| Virtual dissection of Eloquent WM Tracts | ||||
| Altabella et al., 2018 [9] | Theoretical planning study | 19 (all with HGG) | Tractography used to dissect multiple eloquent tracts bilaterally (CST, SLF, IFOF, UNF). Tracts included as OAR during inverse planning with TomoTherapy. | Significant reduction in maximum and mean radiation dose to the tracts, particularly to contralateral tracts. |
| Gavin and Sabin 2016 [20] | Clinical feasibility study | 20 (5 VS, 5 AVM, 9 CM, 1 Menig) | DTI tractography performed using ‘StealthViz’ used on user selected tracts which were included as OAR into GammaPlan prior to GKRS on a series of cases. | Methodologies outlined and shown to be clinically feasible. |
| Kawasaki et al., 2017 [21] | Theoretical planning study | 23 (20 CM, 3 AVM) | Tractography used to include pyramidal tract as OAR in GKRS planning and plans with and without tractography compared. | Maximum radiation dose to the pyramidal tracts significantly reduced when tractography used in planning. |
| Koga et al., 2012 [22] | Retrospective cohort study | 52 (all with AVM, 24 tractography, 28 control) | Integration of tractography into radiotherapy planning for AVM at a single centre with 28 control cases being prior and 24 test cases after this. Patients followed up for a minimum of 3 years. | Significantly less motor complication in patients with tractography integration. No significant difference in treatment success. |
| Sun et al., 2017 [23] | Theoretical planning study | 16 (6 AVM, 8 CM, 2 Menig) | Integration of fMRI to with tractography to model the corticospinal tracts and ‘sensory pathway’. | Significant reduction of the maximum radiation dose to the included cortical areas and tracts. |
| DTI modelled tumoural invasion | ||||
| Berberat et al., 2014 [24] | Theoretical planning study | 13 (all with glioblastoma) | Use of DTI p and q maps and tractography to define the CTV. Comparison to CTV defined by oedema on T2w MRI or isotropic expansion of the GTV. | The DTI-defined CTV was significantly smaller than the T2w MRI-defined CTV and still included sites of tumour recurrence. |
| Hathout et al., 2016 [25] | Theoretical modelling study | NA | DTI-based 3D mathematical model of glioblastoma growth. | Produces model using DTI to model tumour infiltration shown to predict glioma growth in example cases. |
| Jordan et al., 2019 [26] | Theoretical modelling study | NA | Study that develops open-source DTI based fibre-tracking software that produces anisotropic CTV to better capture likely areas of tumour infiltration. | The software is shown to qualitatively capture areas of recurrence well in a few example cases. |
| Metz et al., 2020 [27] | Retrospective observational study | 35 (all with glioblastoma) | Use of deep learning to correct FA maps for free water and used to predict areas of glioma recurrence on follow-up imaging. | Area under the curve for recurrence prediction of 0.77 using FA and 0.9 using free water-corrected FA values. |
| Peeken et al., 2019 [28] | Theoretical planning study | 33 (all with glioblastoma) | Use of deep-learning-based free water-corrected FA maps to define the GTV and compared to traditionally defined GTV. | Free water corrected FA map-based GTV were significantly smaller than traditionally defined GTV but still include the recurrence area of all but one of the 14 subjects with recurrence. |
| Rahmat et al., 2020 [15] | Theoretical planning study | 50 (all with glioblastoma) | Semi-automated DTI-defined tumour volume. GTV manually defined using q map, which was automatically expanded using an expansion model on the p map to model tumour infiltration. Comparison made to manual segmentation of p and q maps. | Mean Dice coefficient of 74% between manual and semi-automated method over all 50 patients. |
| Applications in Gliomas | ||||
| Altabella et al., 2018 [9] | Theoretical planning study | 19 (all with HGG) | Tractography used to dissect multiple eloquent tracts bilaterally (CST, SLF, IFOF, UNF). Tracts included as OAR during inverse planning with TomoTherapy. Treatment plans with and without tractography were compared. | Significant reduction in maximum and mean radiation dose to the tracts, particularly to contralateral tracts. |
| Igaki et al., 2014 [29] | Clinical feasibility study | NA | Integration of tractography into radiotherapy planning in glioblastoma by including the corticospinal tracts as OAR in planning. | Integration of tractography shown to be feasible and reduce radiation does in two cases. |
| Metz et al., 2020 [27] | Retrospective observational study | 35 (all with glioblastoma) | Use of deep learning to correct FA maps for free water and used to predict areas of glioma recurrence on follow up imaging. | Area under the curve for recurrence prediction of 0.77 using FA and 0.9 using free water-corrected FA values. |
| Yahya and Manan 2019 [19] | Systematic review | NA | Systematic review of literature on DTI in intracranial radiotherapy. | Finds only three articles evaluating DTI in radiotherapy that includes gliomas, none of which were case control trials or used prospective integration. |
| Applications in Brain Metastases | ||||
| Conti et al., 2013 [30] | Theoretical planning study | 25 (10 AVM, 3 CM, 12 ‘brain tumours’ | fMRI and tractography of eloquent structures in close proximity to the lesions. Comparison of radiotherapy plans with and without integration. | Found an average reduction in radiation dose by 17% to eloquent regions when fMRI and tractography integrated. |
| Gavin and Sabin 2016 [20] | Clinical feasibility study | 20 (5 VS, 5 AVM, 9 CM, 1 Menig) | DTI tractography used to guide GKRS. | Applied to nine cases of cerebral metastasis successfully; however, there was no comparison to a control group. |
| Kawasaki et al., 2017 [21] | Theoretical planning study | 23 (20 CM, 3 AVM) | Tractography used to include pyramidal tract as OAR in GKRS planning and plans with and without tractography were compared. | Twenty out of 23 subjects had CM. The maximum radiation dose to the pyramidal tracts significantly reduced when tractography was used in planning. |
| Sun et al., 2017 [23] | Theoretical planning study | 16 (6 AVM, 8 CM, 2 Menig) | Integration of fMRI to select tractography seed point to model the corticospinal tracts and ‘sensory pathway’. Functional regions and tracts included as OAR during planning for CyberKnife radiosurgery. Treatment plans with and without integration were compared. | Significant reduction of the maximum radiation dose to the included cortical areas and tracts. |
| Yahya and Manan 2019 [19] | Systematic review | NA | Systematic review of literature on DTI in intracranial radiotherapy. | Finds five articles evaluating DTI in radiotherapy that includes CM, one of which uses prospective integration. |
| Applications in Benign Conditions | ||||
| Gavin and Sabin 2016 [20] | Clinical feasibility study | 20 (5 VS, 5 AVM, 9 CM, 1 Menig) | DTI tractography used to guide GKRS. | Applied to five cases of vestibular schwannoma, five cases of AVM, and one case of meningioma successfully; however, there was no comparison to a control group. |
| Kawasaki et al., 2017 [21] | Theoretical planning study | 23 (20 CM, 3 AVM) | Tractography used to include pyramidal tract as OAR in GKRS planning and plans with and without tractography were compared. | Three out of 23 subjects had AVM. The maximum radiation dose to the pyramidal tracts significantly reduced when tractography was used in planning. However, the plan not used for treatment. |
| Koga et al., 2012 [22] | Retrospective cohort study | 52 (all with AVM, 24 tractography, 28 control) | Integration of tractography into radiotherapy planning for AVM at a single centre in 2004 with 28 control cases being prior to this and 24 test cases after this. Patients followed up for minimum of 3 years. | Significantly less motor complication in patients with tractography integration. No significant difference in treatment success. |
| Koga et al., 2012 [31] | Prospective integration | 155 (all with AVM, 71 of which had tractography) | Routine integration of tractography in radiotherapy of AVMs at a single centre. Selected tracts user selected if suspected to be close to the pathology. | Tractography used in 71 out of 155 radiotherapy cases during the study period with 60% of cases using tractography finding the critical tracts within 5 mm of the lesion. |
| Sun et al., 2017 [23] | Theoretical planning study | 16 (6 AVM, 8 CM, 2 Menig) | Integration of fMRI to select tractography seed point to model the corticospinal tracts and ‘sensory pathway’. Functional regions and tracts included as OAR during planning for CyberKnife radiosurgery. Treatment plans with and without integration were compared. | Significant reduction of the maximum radiation dose to the included cortical areas and tracts. |
| Yahya and Manan 2019 [19] | Systematic review | NA | Systematic review of literature on DTI in intracranial radiotherapy. | Finds 13 articles evaluating DTI in radiotherapy that include AVM, many of which use prospective integration. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colman, J.; Mancini, L.; Manolopoulos, S.; Gupta, M.; Kosmin, M.; Bisdas, S. Is Diffusion Tensor Imaging-Guided Radiotherapy the New State-of-the-Art? A Review of the Current Literature and Technical Insights. Appl. Sci. 2022, 12, 816. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020816
Colman J, Mancini L, Manolopoulos S, Gupta M, Kosmin M, Bisdas S. Is Diffusion Tensor Imaging-Guided Radiotherapy the New State-of-the-Art? A Review of the Current Literature and Technical Insights. Applied Sciences. 2022; 12(2):816. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020816
Chicago/Turabian StyleColman, Jordan, Laura Mancini, Spyros Manolopoulos, Meetakshi Gupta, Michael Kosmin, and Sotirios Bisdas. 2022. "Is Diffusion Tensor Imaging-Guided Radiotherapy the New State-of-the-Art? A Review of the Current Literature and Technical Insights" Applied Sciences 12, no. 2: 816. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020816