1. Introduction
Erosion is a disc-shaped or U-shaped lesion with poorly defined margins and adjacent smooth enamel [
1]. It consists of a loss of mineralized tissue due to chemical processes that cannot be attributed to bacterial activity [
2]. Erosion can have both exogenous and endogenous causes: exogenous causes include frequent consumption of acidic foods or drinks (citrus fruits, alcohol) and acidic medications such as acetylsalicylic acid or vitamin C; endogenous causes include eating disorders such as pathological conditions including anorexia or bulimia and/or gastroesophageal reflux [
3]. Patients exposed to acid reflux from an exogenous cause present erosive teeth lesions on the vestibular surfaces (both upper and lower). For patients suffering from acid reflux due to endogenous causes, it has been shown that the lingual surfaces are the most affected [
4]. Most patients suffering from erosion due to endogenous causes are affected by gastroesophageal reflux disease (GERD) [
5], which is a very common pathological condition amongst the world’s population. Prevalence is high throughout the western world: it is estimated that 25–40% of American adults experience reflux symptoms at least once a month, while approximately 7–10% suffer from it daily [
6]. The prevalence is steadily increasing, mainly due to the increasing prevalence of obesity.
In short, GERD is a gastrointestinal motility disorder that results from reflux of stomach contents into the esophagus or oral cavity, causing symptoms or complications. Acid that is returned to the oral cavity can cause erosion of dental enamel [
7]. Dental enamel is composed of 96% inorganic material and the remaining 4% organic material and water [
8]. The inorganic part is mainly composed of hydroxyapatite, which is a crystalline structure made up of calcium (Ca) and phosphate (P). Enamel does not have the intrinsic ability to repair itself when it is affected by specific dental pathologies, such as caries, abrasions or fractures, because it contains no living cells [
9]. Therefore, when enamel is exposed to the acidic environment of oral cavity, the only possibility of repairing it is through the application of alloplastic materials, such as toothpastes. They are valuable vehicles through which enamel can be protected and potentially improved in its ability to resist an acid reflux. In the context of dental erosion, fluoride toothpastes have been shown to offer some amount of protection, but erosive lesions develop despite their widespread use: Presence of fluoride in solution during dissolution of hydroxyapatite during an acid attack will make the solution highly supersaturated with fluorhydroxyapatite. Fluoride will adsorb to the surface of the partially demineralized crystals and attract calcium ions. Since carbonate- free or low-carbonate apatite is less soluble, these phases will form preferentially instead of the original mineral, under the action of the dissolved minerals. This coating will be less soluble due to the exclusion of carbonate and incorporation of fluoride, rendering the enamel more resistant to future acidic challenges [
10]. Therefore, research is focusing on different chemical compounds to make dental hard tissues more resistant to erosive demineralization. At present, polyvalent metal cations, phosphates or biopolymer additives have shown encouraging results [
11].
The aim of this study is to investigate the effectiveness of two different toothpastes, containing fluoride and non-fluoride, in preventing erosion due to gastroesophageal reflux disease. The first null hypothesis is that no difference in term of teeth remineralization is present between the two toothpaste. The second null hypothesis is that no difference in terms of teeth protection against an acid attack is present between the two studied toothpastes.
2. Materials and Methods
2.1. Sample Preparation
Six tooth elements from bovine jaws, with no caries and/or fractures, were selected for the study. After extraction, residual soft tissue remaining on the surface was removed. Subsequently, the elements were washed with a soft-bristled hand brush and immersed in a 5% sodium hypochlorite solution for 1 h. Subsequently, all samples were kept in a 0.9% NaCl solution containing 0.1% thymol to maintain hydration [
12]. Depending on the procedure performed, teeth were divided into groups A, B, C, D, E and F (
Table 1).
All teeth were cut at the cementoenamel junction using a high-speed diamond bur and water irrigation. The palatal and lingual surfaces were smoothed using dental polishers for 1 min under irrigation.
2.2. Demineralization and Remineralization
To simulate an acid attack, teeth were immersed in a 15% HCl hydrochloric acid solution for 2 min, then they were rinsed with flowing water for 30 s and dried, then immersed again in physiological solution [
13]. Two different toothpastes, having the same compounds with the exception of fluoride, were used for the remineralization process, one containing 1450 ppm of fluoride and the second without fluoride. In this article, the toothpaste containing fluoride is denoted “toothpaste A”, while the one without fluoride is “toothpaste B”. Teeth in groups C and D were brushed for 2 min per day for 14 days with the fluoride-containing toothpaste. Brushing was done with an Oral-B Genius 10,000N (P&G, USA)
® electric toothbrush with a soft brush head, attached to a vice to keep it in the correct position so the same movement was always performed.
Teeth in groups E and F were brushed in the same way as above but the toothpaste used did not contain fluoride. At the end of the treatment, teeth D and F were again immersed in the 15% hydrochloric acid HCl solution for a period of 2 min. After this step, they were rinsed under flowing water, dried, and finally re-immersed in saline solution.
2.3. Scanning Electron Microscope (SEM)
Morphological characteristics of samples were studied using the scanning electron microscope SEM, (Leica microsystems srl, Milan, Italy). To be observed correctly, samples must be conductive, so a metallic layer should be placed on top of them. In detail, samples in this study were coated with a gold layer of approximately 20 nm. The microscope used for the experimental activity was a Cambridge Stereoscan 440 (Leica microsystems srl, Milan, Italy), equipped with a Philips PV9800 EDS (Leica microsystems srl, Milan, Italy) microanalysis available at the Industrial Engineering Department of the University of Padua. Images were taken using the secondary electron detector.
2.4. Profilometer
Surface topography of teeth was analyzed using a Sensofar Plu Neox optical profilometer (Barcellona, Spain). Scans with lateral dimensions of 1.3 × 0.6 mm2 were acquired using a 20x confocal objective. Following acquisition, topographies were subjected to shape removal by subtraction of a plane. Three scans were performed in different areas for each tooth and three surface profiles were extracted for each topography, from which the roughness was calculated according to ISO 4288. Two filters, λs and λc, equal to 2.5 μm and 0.025 mm, respectively, were applied for the roughness calculation.
2.5. Measurements
A profilometer was used to obtain the measurement of tooth roughness.
This was done to measure the roughness along the tooth as well as to assess the effectiveness of the two toothpastes in demineralizing the tooth after acid attack. Statistical analysis was divided into two parts: the first one to test the effect on tooth roughness of each toothpaste, through a paired-sample test, and the second one to compare the effects of the two different toothpastes.
3. Results
3.1. Profilometer Measurements
Nine measurements were taken in each sample, but in different locations (
Table 2).
3.2. Descriptive Analysis
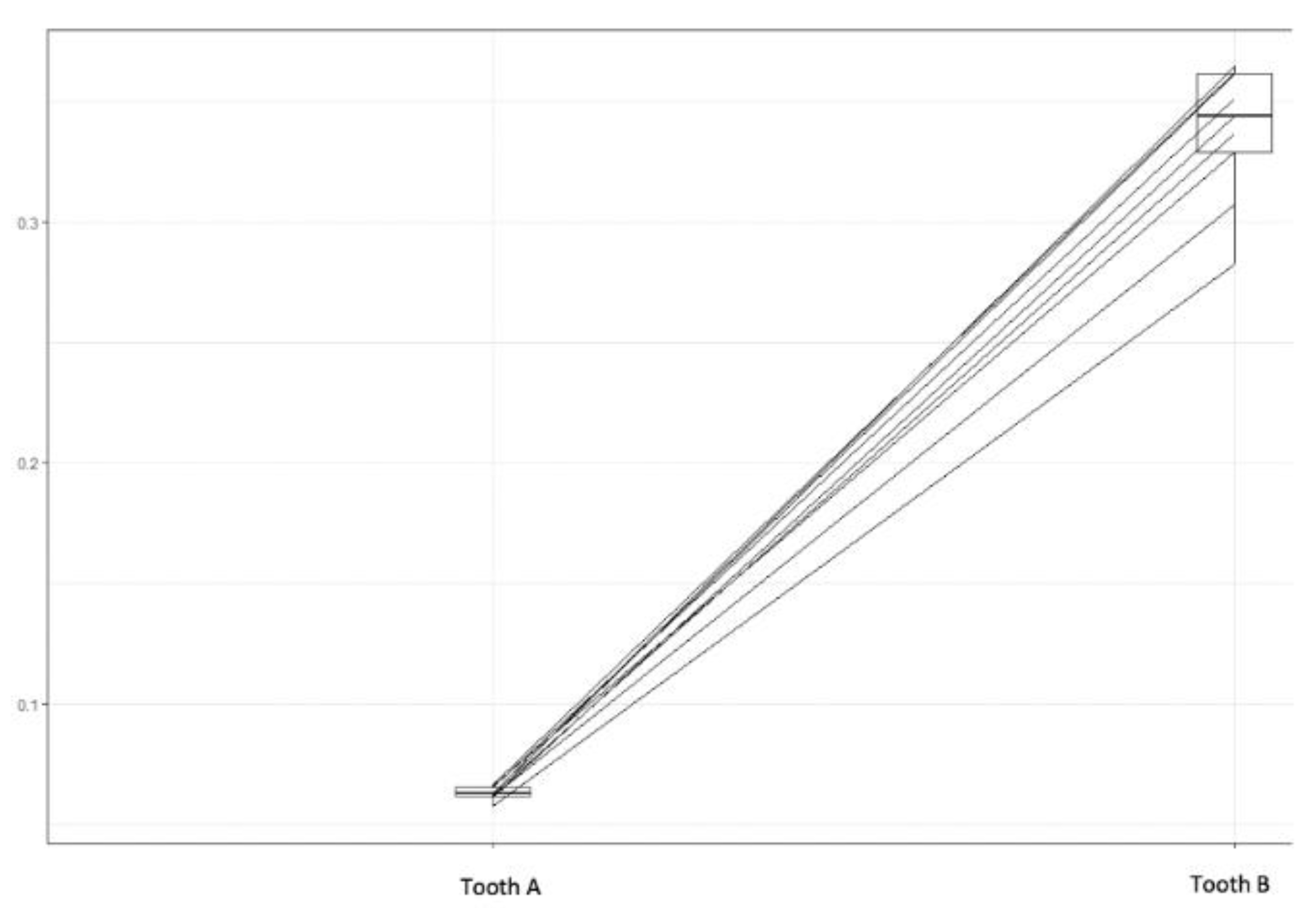
First, a descriptive analysis of the tooth roughness before (initial tooth roughness) and after acid attack without considering any toothpaste, “Tooth A” and “Tooth B”, respectively, was carried out. In
Figure 1, the comparative graph of the values of the initial stage (Tooth A) and after the application of acid attack (Tooth B) is shown and it can be clearly seen that the roughness increased significantly in all observed points.
To complete this first analysis, some descriptive measures of position and dispersion were calculated and are listed in
Table 3.
Originally the tooth had an average roughness of 0.0628 µm; after the acid attack this average increased to 0.3374 µm. It is also observed that after the acid attack, the coefficient of variation (CV) increased among the teeth, i.e., the variability of roughness in the tooth also increased significantly.
3.3. Toothpaste A
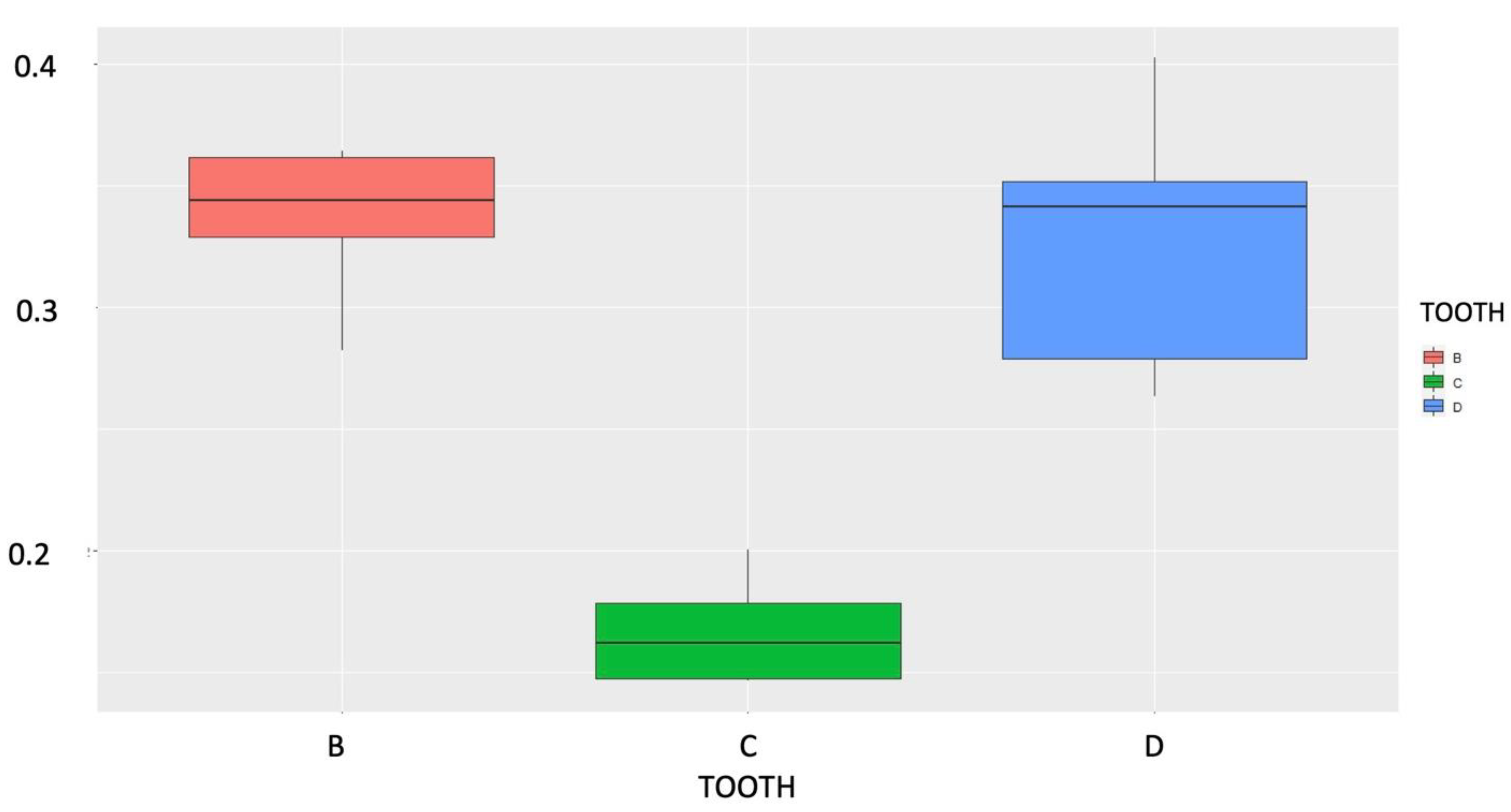
A descriptive analysis was carried out considering the effect of toothpaste A on the roughness of the tooth, analyzed after the initial acid attack (Tooth B). Then, in
Figure 2, the behavior of the performance in each situation is shown, using a Box-plot diagram. At first it was observed that there was a decrease in roughness after the acid attack and the use of toothpaste A, called “tooth C”, but after a new acid attack, called “tooth D”, the roughness returned close to the initial values. It was also observed that the “tooth D” condition (colored blue in
Figure 2) had lower roughness values than the “tooth B” condition and the greater roughness variability between these three situations.
3.4. Toothpaste B
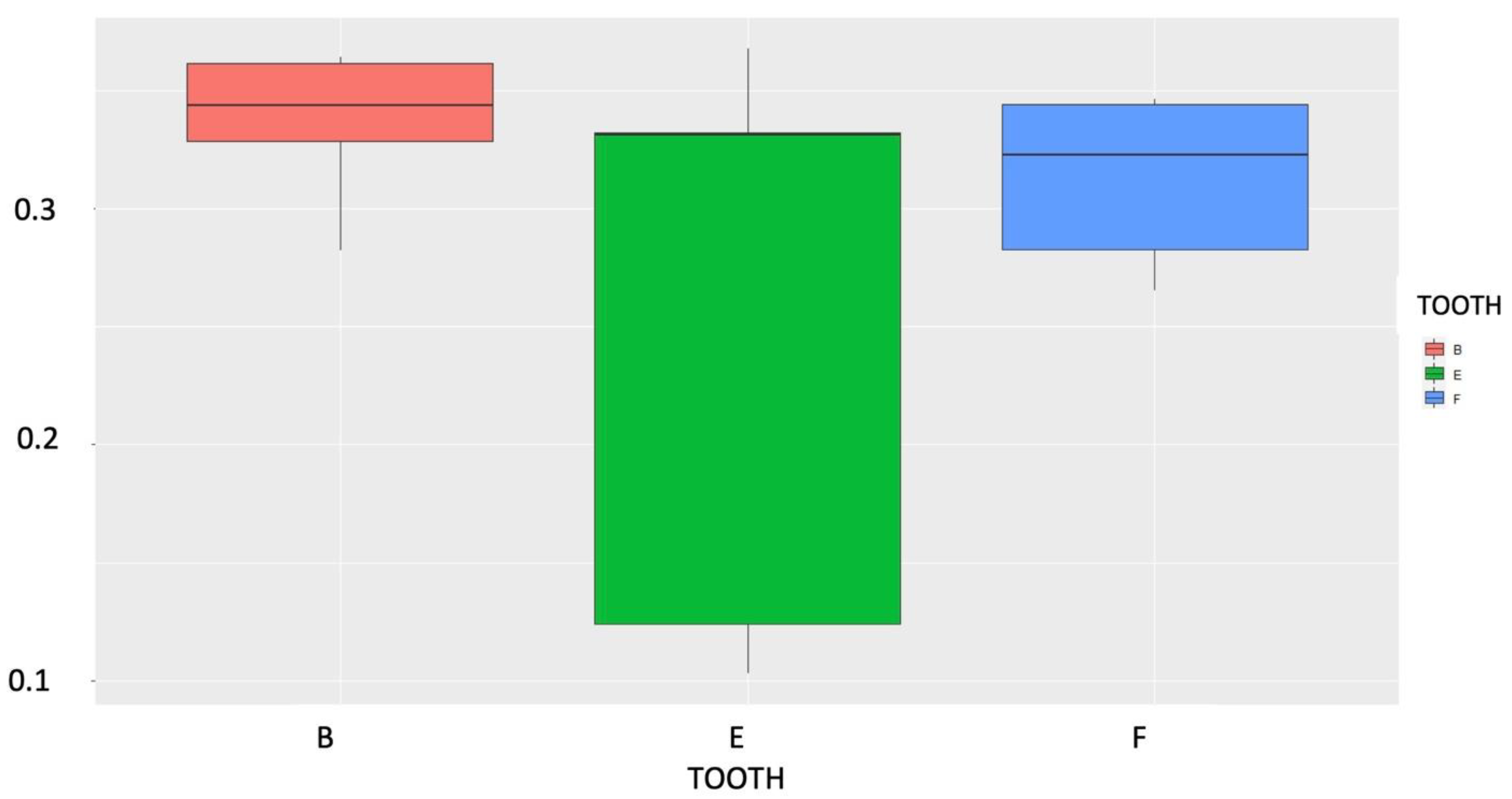
In
Figure 3 it can be observed that there was a certain decrease in roughness after the acid attack and the use of toothpaste type B (tooth E), but this decrease is not as noticeable as it occurred with the use of toothpaste A. After a new acid attack (tooth F) the roughness returned to very close to the initial values (same behavior as with toothpaste A).
3.5. Statistical Analysis: Paired Test
To perform the analyses, the Mann–Whitney test was conducted for paired data as the different conditions are applied to the same test body.
When considering a significance level of 0.05 (α = 5%), there was, on average, a statistically significant decrease in tooth roughness after the application of toothpaste A (i.e., we compared tooth B and C). It was also observed that after a new acid attack on the tooth after the use of toothpaste A, there was a significant increase in roughness. Finally, we found that, on average, there was no significant difference between teeth B and D, i.e., toothpaste A did not act in a protective manner in reducing roughness. Moreover, toothpaste B was not able to decrease roughness, on average, and did not act as a protective factor.
3.6. Statistical Analysis: Non-Paired Test
At first, a statistical analysis was carried out to analyze whether there was a statistical difference between tooth C and E regarding average roughness. A Student’s t-test was applied, after verifying that variables follow a normal distribution (p-value > 0.05, Kolmogorov–Smirnov test = 0.13).
The result of the t-test considering different variances and their respective p-value was smaller than the 5% significance level (α = 0.05), meaning that the average roughness found in tooth C is significantly lower than in tooth E, thus the first null hypothesis was rejected.
Next, it was checked whether there was a difference in the average roughness found in teeth after a new acid attack (tooth D vs tooth F).
The p-value is greater (4.17) than the 5% significance level (α = 0.05) and therefore the second null hypothesis that the averages of teeth D and F are equal is not rejected: it is concluded that there is no significant difference between the average roughness after acid attack following the use of toothpaste A and B. There is no statistical evidence, therefore, that there was greater or lower protection of toothpaste A or B after acid attack.
4. Discussion
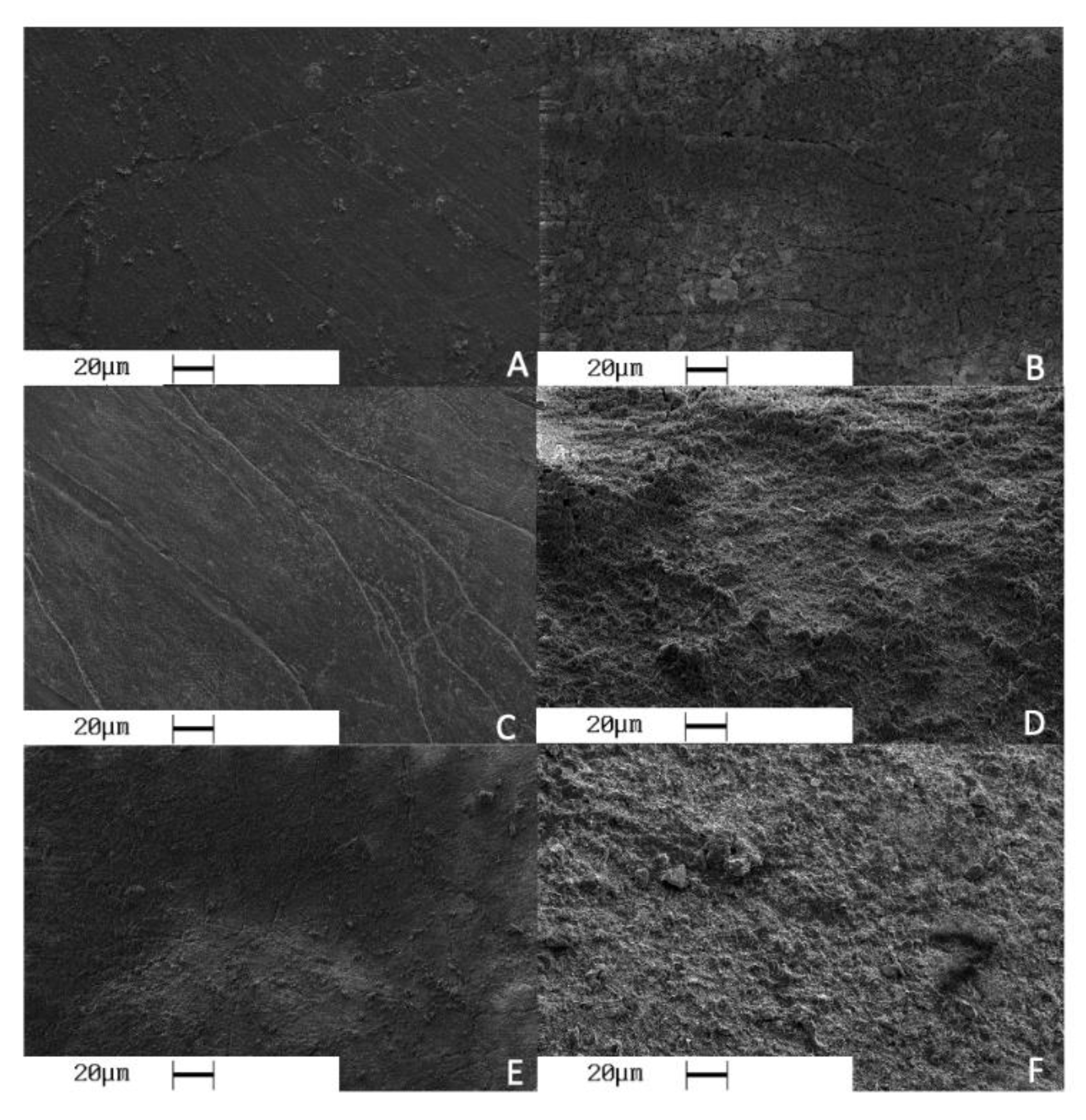
In the present study, a scanning electron microscope (SEM) and profilometer were used to test the level of protection that toothpastes can offer in the presence of erosion due to gastroesophageal reflux disease (GERD). SEM images show significant differences between intact enamel surfaces and those subjected to acid attacks (
Figure 4A,B).
SEM results are not sufficient to demonstrate the actual change to the enamel surfaces caused by the acid attack; a profilometer was also used for this reason. Data obtained from the roughness analysis show that acid attack causes a dissolution of hydroxyapatite crystals. This is because intrinsic erosion is caused by gastric juices reaching the oral cavity [
2].
Tooth A recorded an average roughness of 0.0628 μm, a value which increases exponentially in tooth B, subjected to the first acid attack. Roughness reached by tooth B has an average value of 0.3374 μm. It is now known that eating disorders, such as bulimia and gastroesophageal reflux, cause an increase in tooth roughness and appearance of erosive lesions [
14]. Frequent episodes of vomiting or regurgitation cause erosion at the level of the enamel, which is due to pH levels in the stomach reaching 1 or lower. Evidence associating GERD and dental erosion comes from two main areas: patients presenting with reflux symptoms who are then found to have dental erosion and patients presenting with erosion who are then diagnosed with GERD. One of the first studies about association between dental erosion and GERD was carried out by Jarvinen et al. [
5]. They diagnosed GERD using endoscopy to assess esophagitis in 20 patients. Dental erosion was diagnosed in four of these patients, concluding that patients diagnosed with GERD had an increased risk of developing dental erosion. Meurman [
15] conducted a similar study with a larger sample size (117 patients reporting symptoms of GERD). Dental erosion was reported to involve 24% of tooth surfaces. Authors concluded that severe reflux disease of long-lasting duration was more likely to cause dental erosion than milder forms.
Concerning the effect of toothpastes in the enamel remineralization process, it can be observed through SEM images that enamel surfaces of teeth C and E show the typical aprismatic appearance of an intact surface undergoing remineralization. (
Figure 4C,E). The merely iconographic investigation of the SEM was also confirmed by the statistical analysis of the profilometer. Numerical data confirm that roughness in elements C and E has strongly decreased, with an average value of 0.1696 μm for the first element and 0.260 μm for the second. In this first part of the analysis of the results, it can be stated that these values confirm that the toothpaste used played an important role in repairing the damage that the 15% HCl caused to sample surfaces. Literature agrees that toothpastes play a fundamental role in erosion prevention. Lussi and Jaeggi [
16] suggested that topical application of fluoridated but acidic products causes an initial dissolution of minerals contained in the enamel, thus increasing the local pH, but at the same time they are able to carry the creation of fluoro-hydroxyapatite, more resistant to bacterial attack. In addition, the buffering capacity of saliva and organic film led to a further protective effect. It seems that highly concentrated applications of mildly acidic fluoride are able to decrease the development of erosions in enamel and increase resistance to mechanical abrasion. In his study, Lippert [
17] agrees with the effectiveness of toothpastes in preventing erosive lesions and considers them to be an essential tool.
Comparing the roughness values obtained from the two toothpastes, it can be concluded that there is a statistically significant difference between the mean roughness when using toothpaste A and B after acid attacks. The average roughness found in tooth C is lower than in tooth E. Many studies in the literature confirm the results obtained, while others have reported conflicting results. Lombardini et al. [
12] found that the use of fluoridated toothpastes is effective in regenerating a homogeneous, very compact, thick and uniform surface layer. Indeed, prismatic structure of hydroxyapatite was not observed after the application of fluoridated dentifrices. In the same study, he concluded that a non-fluoridated toothpaste does not offer a sufficient degree of remineralization to protect and repair enamel damaged by acid attack. In the 1970s, Graubart [
18] showed that the use of a 2% sodium fluoride solution provides a protective action against enamel erosion. In vitro, less tooth wear was produced in the presence of fluoride toothpaste than in the presence of fluoride-free toothpaste with an equal formulation. In more recent years, several studies using different fluoride formulations, e.g., sodium fluoride, acidified phosphate fluoride, stannous fluoride, amine fluoride or titanium tetrafluoride have shown a greater protective effect in vitro [
19].
In contrast to the present study, Larsen and Nyvad [
20] and Larsen and Richards [
21] found that fluoride cannot reduce dental erosion. In principle, fluoride has a protective effect at a pH higher than the one indicated by the fluorapatite saturation curve at given concentrations of Ca and PO4. According to this study, fluoride at concentrations found in toothpastes are unlikely to have much beneficial effect on erosion, because the amount of acid produced by gastric juices is excessively high. However, it is possible that, if other erosive factors are not excessive, fluoride in solution may provide some protective effect.
Results obtained from the present study indicate that there is no statistical difference in protection from a second acid attack; that is, neither toothpaste A nor B offers a sufficient degree of remineralization in the event of a second acid attack. Indeed, from the SEM images provided, it can be seen (
Figure 4D,F) that the enamel surface is significantly eroded after a second acid attack. This is confirmed by numerical statistics, which show a considerable increase in roughness of 0.329 μm for tooth D and 0.313 μm for tooth F. Fluoride contained in toothpastes (1450 ppm) was not sufficient to prevent a second acid attack. It is reasonable to assume that higher fluoride concentrations could have prevented a second erosive lesion more effectively. This supposition is also confirmed by literature. Sorvari et al. [
22] have shown that treatment with fluoride varnish (2.26%) for 24 h and high concentration fluoride rinses (1.2%) for 48 h applied before acid challenge offer in vitro protection against erosion. This protection is presumed to be due to the precipitation of calcium fluoride-like particles that adhere to tooth surfaces and generate fluorapatite. Thus, a gentle application of fluoride (without destruction of the acquired protective film) before an erosive attack would be more beneficial. Formation of the CaF2-like layer on the tooth surface would act as a “barrier” against acid attack. This layer provides some additional minerals to dissolve during an acid attack before underlying enamel is attacked.
Different conclusions are drawn by Ganss [
10], that states that the use of fluoride is essential in the prevention of carious disease, as it offers a very high degree of protection, but not in the case of erosive lesions, that would form despite the use of fluoridated toothpastes. The study proposes, in addition to inorganic components, the use of organic substances within the toothpastes. It is assumed that polymers such as mucin or carboxymethylcellulose can form protective layers on the tooth surface. Some of these are frequent ingredients in toothpastes, e.g., hydroxyethylcellulose compounds, carboxymethylcellulose, alginate, xanthan gum, or polyethylene glycol. These studies are still in early stages, but the authors believe they may lead to a breakthrough in the prevention of erosive lesions.
A limitation of this study was that being in-vitro, some of the in-vivo variables could not be deepened, for instance human saliva remineralization effect. Moreover, further studies with a larger sample size may confirm the findings of this study.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}