
Very Short-Term Photoplethysmography-Based Heart Rate Variability for Continuous Autoregulation Assessment


1
Institute of Computer Science and Engineering, College of Computer Science (CS), National Yang Ming Chiao Tung University (NYCU), Hsinchu 300, Taiwan
2
Department of Computer Science, College of Computer Science (CS), National Yang Ming Chiao Tung University (NYCU), Hsinchu 300, Taiwan
3
Institute of Biomedical Engineering, College of Electrical and Computer Science, National Yang Ming Chiao Tung University (NYCU), Hsinchu 300, Taiwan
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(13), 6469; https://0-doi-org.brum.beds.ac.uk/10.3390/app12136469
Submission received: 31 May 2022
/
Revised: 24 June 2022
/
Accepted: 24 June 2022
/
Published: 25 June 2022
(This article belongs to the Special Issue Advances in Biomedical Signal Processing in Health Care)
Abstract
:Featured Application
A signal processing combination of instantaneous pulse rate variability and time shift multiscale entropy for autoregulation assessment was proposed.
Abstract
Background: Heart rate variability (HRV) has been widely applied for disease diagnosis. However, the 5 min signal length for HRV analysis is needed. Method: A signal processing procedure for very short-term photoplethysmography (PPG) signal for fever detection and autoregulation assessment was proposed. The Time-Shift Multiscale Entropy Analysis (TSME) was applied to instantaneous pulse rate time series (iPR) and normalized by the cumulative distribution function (CDF) of all scales to calculate novel indices. A total of 33 subjects were recruited for the study. Fifteen participants whose body temperatures were higher than 37.9 °C were served as the fever group. Others were served as the non-fever group. The total 15 s PPG signal with 200 sampling rates was used for iPR calculation. Result: The CDF value of entropy on the scale k = 19 (CDF(E(k = 19))) of iPR had the lowest p-value calculated by the Weltch t-test between two groups (p < 0.001). The Spearman correlation r between CDF(E(k = 19)) and body temperature is −0.757, 0.287, and −0.830 in all subjects, the non-fever group and the Fever group, respectively. The area under the curve, calculated from the receiver operating characteristic of CDF(E(k = 19)) of iPR is 0.915. Conclusion: The entropy of iPR is useful for detecting fever. Moreover, a short-term PPG signal is suitable to develop real-time applications, and multiscale entropy provides different scales of information for daily healthcare.
1. Introduction
Heart rate variability (HRV) has been applied for health assessment for a long time. Many studies have shown that HRV is related not only to cardiovascular diseases but also to autonomic nervous system (ANS) activity [1,2]. To measure HRV, the beat-to-beat interval (RRi) of the electrocardiography (ECG) signal is usually calculated. In time-domain analysis, indices such as Standard deviation of normal -to-normal intervals (SDNN), Proportion of NN50 divided by the total number of NNs (pNN50) calculated from RRi are useful for the diagnosis [3]. In frequency domain analysis, each frequency band in the power spectrum of RRi has been proved related to the ANS activity [2]. Furthermore, the irregularity of RRi in abnormal heartbeats is different from healthy heartbeats [4,5,6]. Instead of using ECG for HRV calculation, photoplethysmography (PPG) signal can also be used for HRV analysis, called pulse rate variability (PRV). PPG was usually worn on the user’s finger. PPG optically measures the change in blood volume in the microvascular tissue. The pulse-to-pulse interval (PPi) is obtained for PRV analysis. Although pulse arrival time (PAT) exists between the ECG and PPG signals, previous studies still showed that PRV can be a surrogate for HRV [7,8,9].
Both RRi and PPi have low time resolution, which limits the investigation of HRV and PRV [1,10]. Information about every two heartbeats is usually ignored. Therefore, instantaneous pulse rate variability (iPRV) was proposed [11]. iPRV calculates the instantaneous frequency of the main intrinsic mode function (IMF), decomposed by empirical mode decomposition (EMD) [12]. According to Bedrosian’s theorem, the source data should be no amplitude modulation for instantaneous frequency calculation. Therefore, the instantaneous frequency is calculated using the normalized Hilbert transform (NHT) or the normalized direct quadrature (NDQ) [13]. For comparison of RRi or PPi, the inverse of instantaneous frequency, called instantaneous pulse rate (iPR), is usually applied for further analysis. Time-domain and frequency-domain analyses of iPRV have been studied [11,14,15]. These studies showed that iPRV had a similar result to conventional indices compared with HRV or PRV in time- and frequency-domain analysis. Moreover, because of the higher time resolution of time series iPR, more detailed information on the variability of heartbeats can be indicated. However, the non-linear dynamical analysis of iPRV is not performed yet.
For nonlinear dynamical analysis, entropy is common for complexity measurement of time series. Shannon, who proposed Shannon entropy, was the first person who applied the concept of entropy to information theory [16]. However, Shannon entropy is only related to the probability of the appearance of the element, and it cannot measure the complexity of randomness. In the field of biomedical signal analysis, sample entropy (SampEn) is the most popular one for nonlinear dynamical analysis [17]. SampEn is based on conditional entropy, which compares the difference of short patterns in the signal. For HRV analysis, RRi was applied SampEn for complexity measurement. Many studies show that the RRi in patients with cardiovascular disease were different from the RRi in healthy people [5,6,18]. In addition, the different time scales of the signal are also concerned for more detailed information indication [5,6]. In this study, the multiscale entropy method called Time-Shift Multiscale Entropy analysis (TSME) [19] was applied in the iPR to indicate the difference between the person with fever and the person without fever. Body temperature and heart activity are usually regulated by ANS and peripheral response [20]. Fever is one of the early signs of infection and needs to be systematically monitored in the intensive care unit (ICU) [21]. Furthermore, fever is also a common sign of many infectious diseases and non-infectious diseases, and it is also an indicator of disease progression in many hospitalized patients. Body temperature measurement using traditional thermometers is reliable and low cost. However, it requires caregivers to perform the measurement and it will be time-consuming to measure frequently. Therefore, it is hard for clinicians to continuously monitor patients’ body temperature and get notified if a patient has a fever in time using the traditional technique. PPG had been widely used in the hospital setting to measure oxygen saturation and estimate blood pressure. Obtaining temperature information from the PPG can assist the clinicians to have a better understanding of the patients’ condition. In addition, PPG devices have been installed on several models of smart wearing devices on the market nowadays. Being able to monitor fever using PPG in an out-of-hospital setting may allow healthy people to get aware of their illness earlier, such as COVID-19 or heat stroke during exercise, and have a chance to seek medical assistance in time.
The structure of the paper is organized as follows: Section 2 describes the experiment, subject information, and algorithms of each signal processing and analysis method. Section 3 gives the result of TSME on iPR and PPi. The discussion of the results and further comparison are described in Section 4. Finally, Section 5 gives a conclusion.
2. Materials and Methods
2.1. Subjects and Experiment
This experiment was approved by the Research Ethics Committee for the Protection of Human Subjects of the National Chiao Tung University (NCTU-REC-103-061; date of approval: 2 June 2015). Informed consent was obtained from all subjects and their parents before the experiment. The experiment was carried out at the Yo Yo Clinic, Kaohsiung, Taiwan. A total of 33 people aged 7 to 18 years were recruited for this study. The subject’s core body temperature was measured by the doctor. 15 subjects whose body temperature was higher than 37.9 °C and who were fever diagnosed by the doctor served as the fever group, others served as the non-fever group. Subjects were asked to do supine position quietly for ten minutes. At the same time, the PPG signal was collected with 200 sampling rates by using the PPG device (Nonin 8500, Nonin Medical Inc., Plymouth, MN, USA). The previous study showed that iPRV can be performed using short-term PPG [22], a total of 15 s stable signal in the middle of the total PPG signal was used in this study. It can also decrease the computation time cost of the advanced EMD method and the SampEn algorithm.
2.2. PRV Procedure
The PRV procedure is similar to HRV but uses the PPG signal instead of the ECG signal. The first step of PRV is to find the pulse peak of the PPG signal. Then calculate the time difference between a pulse peak and the next one. The PPi can be obtained after calculating the interval between each two pulse peaks. However, in this study, only 15 s PPG was applied. The time scale of PPi was not enough for further analysis. Therefore, the PPi was interpolated into 200 sampling rates, which was the same as the PPG signal to be PPi series for further analysis.
2.3. iPRV Procedure
The iPRV applied the main decomposition method EMD of the Hilbert-Huang Transform (HHT) to calculate the instantaneous pulse rate of PPG [11]. IMF was decomposed by EMD from PPG. The IMF should satisfy two conditions: (1) the number of local minimum and local maximum must be equal to the number of zero-crossings or differ at most by one, and (2) the value of average envelop must be approximately equal to zero at any point. However, the mode mixing problem, which means that different frequency band components are decomposed into the same IMF, exists in IMFs if the signal is by EMD. Therefore, the complete ensemble EMD (CEEMD) was proposed to solve the problem [23]. Before introducing CEEMD, EMD should be described first. The first step of EMD is to calculate the upper envelope and the lower envelope by using extremum points of the raw signal. Next, compute the average envelope using the upper envelope and lower envelope. Third, subtract the average envelope from the raw signal as the output signal. Finally, check if the output signal is IMF or not. If not, let the output signal be a raw signal to redo the above steps. If the output signal is IMF, output the IMF, and using the raw signal subtract the IMF to redo the above steps until the residual is mono-component. For CEEMD, the raw signal is added and subtracted by the same white noise before performing EMD. Therefore, there are two types of raw signal: raw signal with adding white noise and raw signal with subtracting white noise. Decompose these two raw signals into IMFs. To decrease the influence of white noise, repeat the above steps with different white noise many times (50 times in this study). Finally, average all corresponding output IMFs to ensemble IMFs. According to Nuttall’s theorem, before computing the instantaneous frequency by the Hilbert transform or direct quadrature method, the oscillation of the source data should be a sinusoidal signal. That is why we decomposed PPG by EMD into IMFs. Additionally, according to Bedrosian’s theorem, the source data should be without amplitude modulation for instantaneous frequency calculation by Hilbert transform or the direct quadrature method. Therefore, in this study, the NDQ was applied to calculate the instantaneous frequency [13]. After the modulation of the amplitude was removed, the source data can be considered as a cosine function. Therefore, we can use the direct quadrature method to calculate the instantaneous phase using the arctangent. The instantaneous frequency is obtained from the derivative of the instantaneous phase. For comparison with the RRi or PPi series, the inverse of instantaneous frequency called the instantaneous pulse rate series (iPR) was computed for further processing.
2.4. Time-Shift Multiscale Entropy (TSME)
The TSME applied the main idea of Higuchi’s fractal dimension (HFD) to compute the different time scales of the source data [19,24]. Let X be the source data.
The HFD reconstructs the source data into different time scales as follows:
where N is data length, is kth time scale segment. is the βth point of source data. The TSME of the kth time scale is calculated:
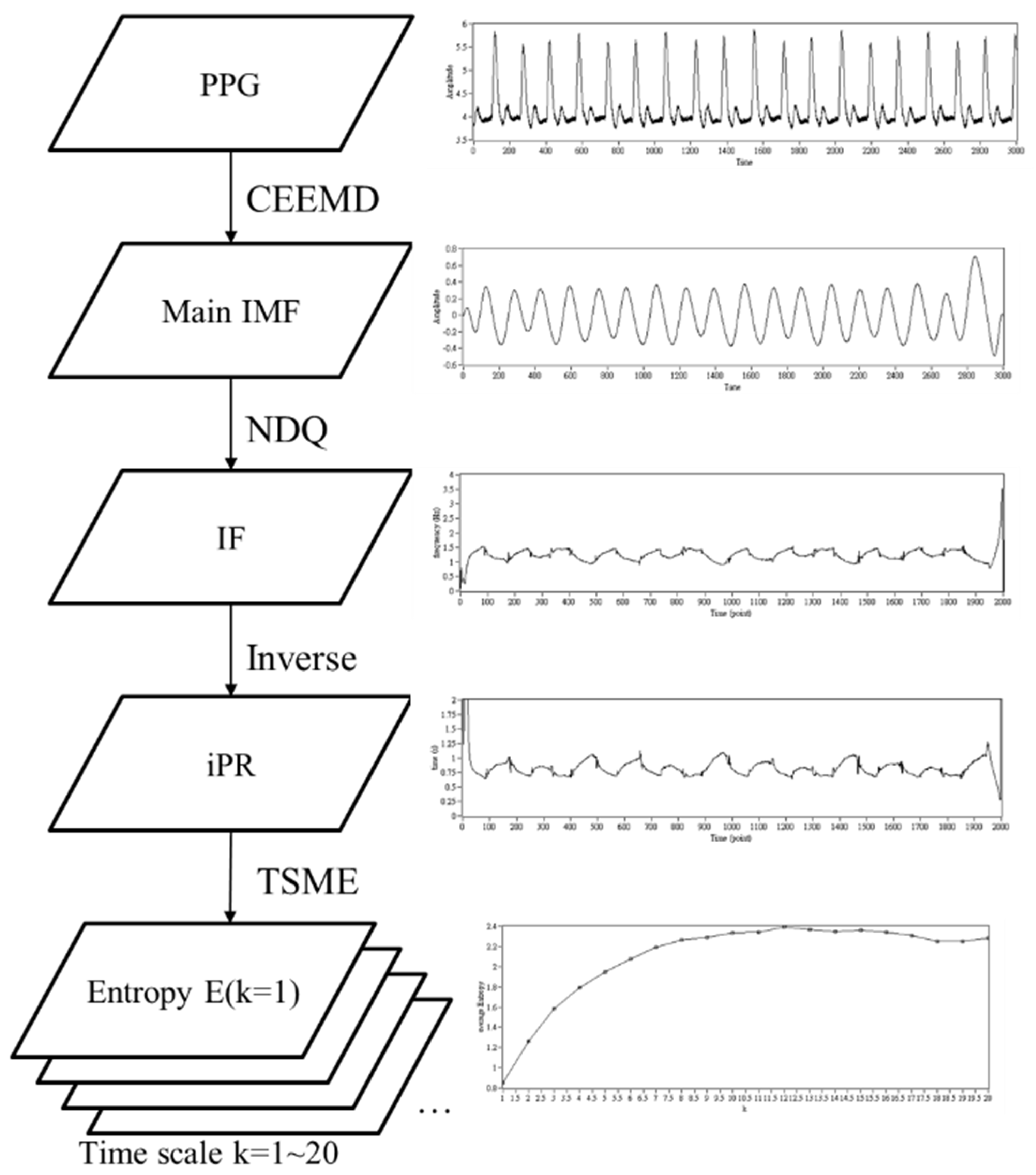
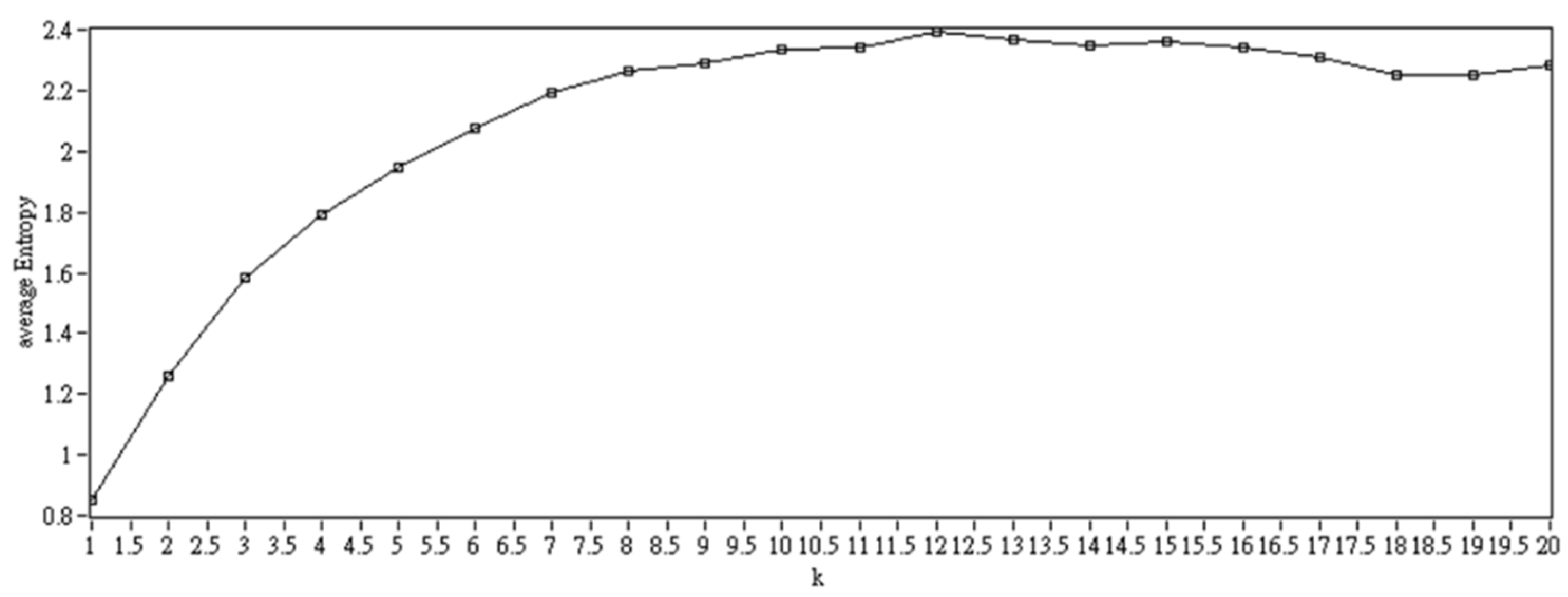
In this study, the TSME were m = 2, r = 0.15* standard deviation of the iPR or PPi series, k = 1 to k = 20. The E(k = i) denotes the ith TSME value. Figure 1 showed the demonstration of signal processing. Figure 2 showed the example of the distribution of E(k = 1~20) of a subject. Further indices according to the distribution were calculated. The TSME of all k scales could be normalized by cumulative distribution function (CDF). The CDF value of TSME in scale i is denoted as (CDF(E(k = i))).
2.5. Other Indices Calculation
In addition to the above entropy indices, the other entropy-related indices and conventional iPRV and PRV indices were calculated. Mean(E(k = 1~20)) and std(E(k = 1~20)) calculated the average value and standard deviation of E(k = 1~20). Max(E(k = 1~20)) and Min(E(k = 1~20)) was the maximum value and the minimum value of E(k = 1~20). Area(E(k = 1~20)) calculated the distribution area of distribution of E(k = 1~20).
The conventional time domain indices were the mean and standard deviation of time series (iPR or PPi). For the frequency domain analysis, the frequency bands of low frequency (LF), high frequency (HF), and very high frequency (VHF) were 0.04 Hz to 0.15 Hz, 0.15 Hz to 0.4 Hz, and 0.4 Hz to 0.9 Hz, respectively. The normalized power of each band was calculated as follows.
where TP is the total power. However, VHFs were not used in conventional PRV analysis. Only the iPRV analysis used VHF. Therefore, the TP can be calculated including VHF or not. Thus, we use superscript a to present the normalized power calculated excluding VHF and superscript b to present the normalized power calculated including VHF.
3. Results
The basic characteristic of the subjects is shown in Table 1.
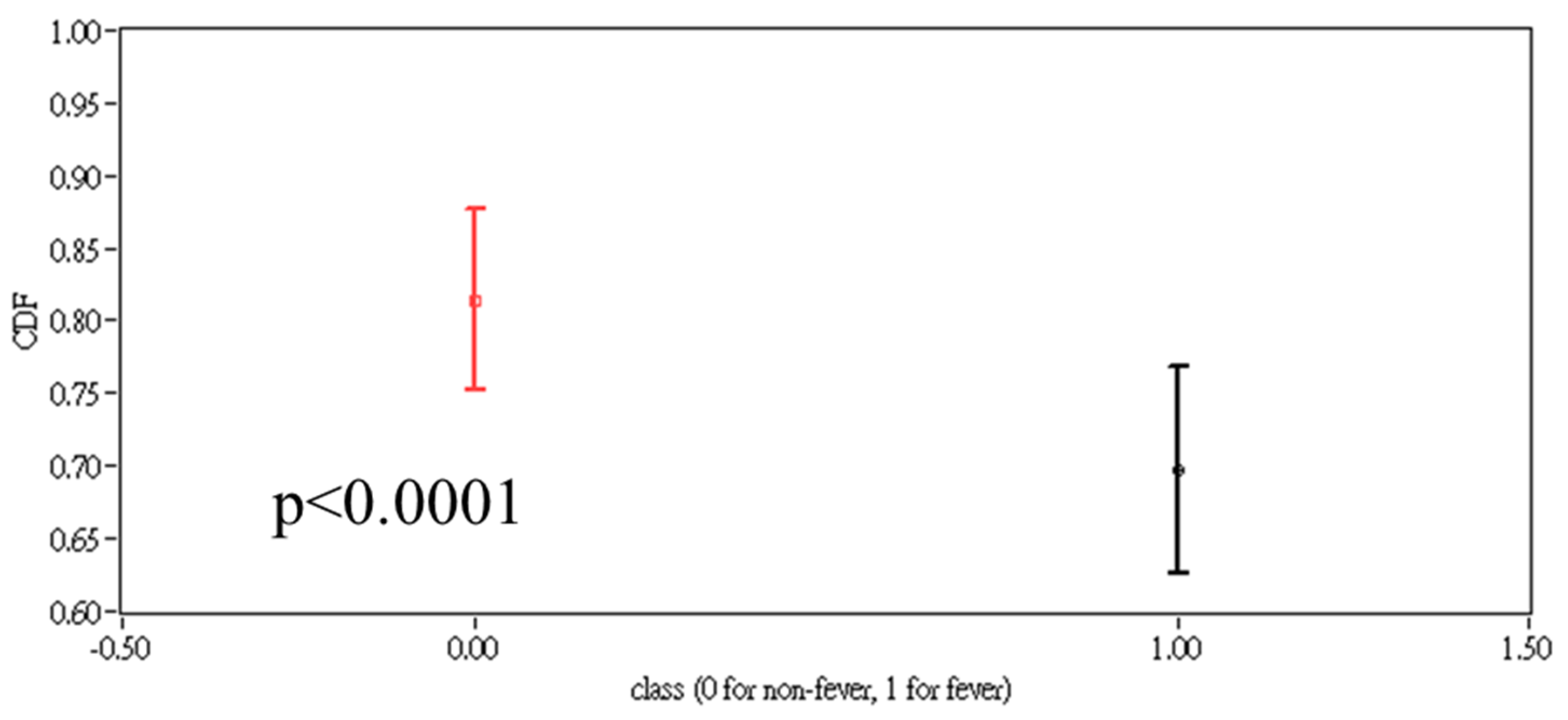
The result related to iPR is shown in Figure 3. TSME on the scale k = 19 CDF(E(k = 19)) had the lowest p-value calculated using the Weltch t-test between two groups (p < 0.001).
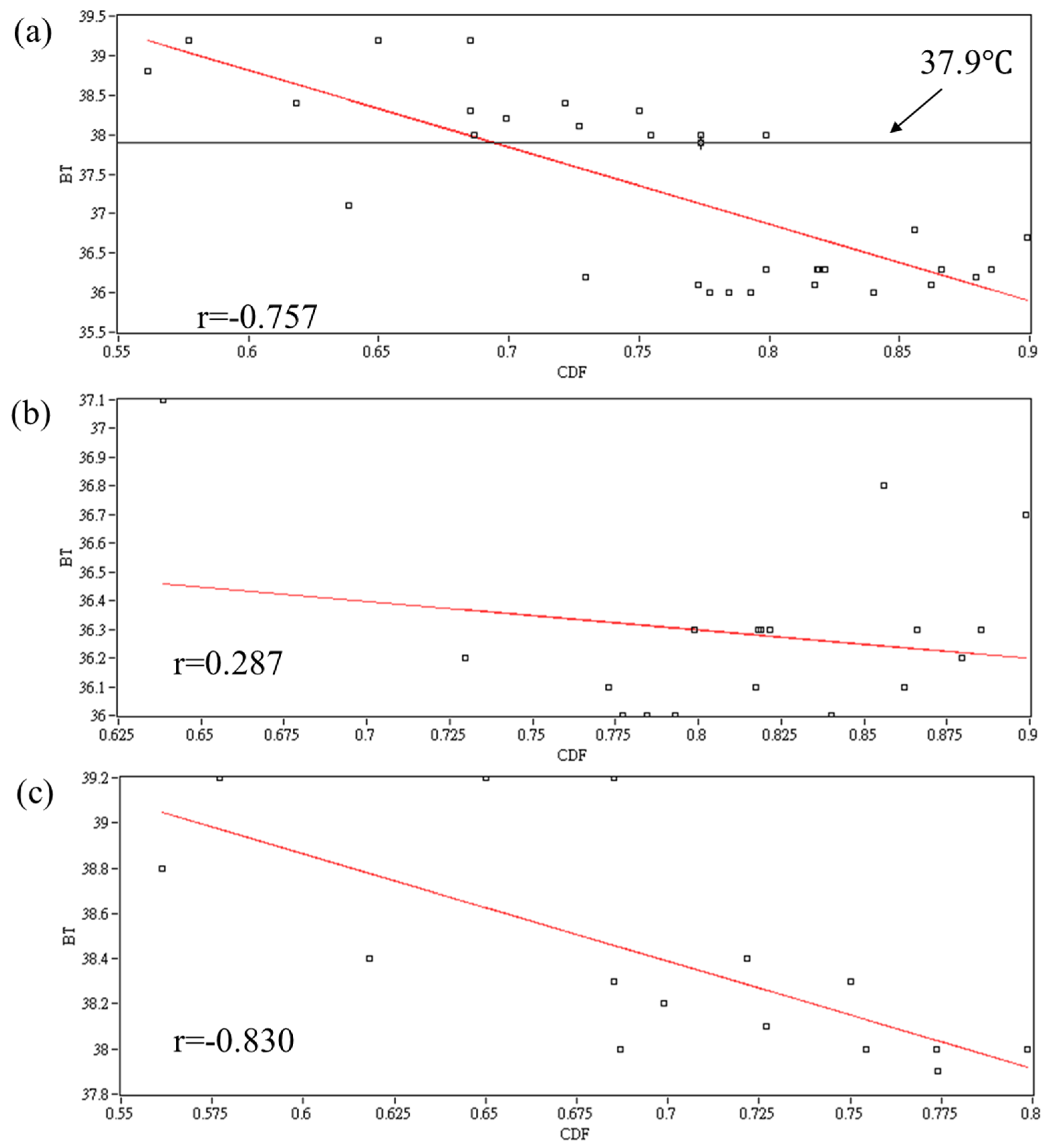
The Spearman correlation r between CDF(E(k = 19)) and body temperature is shown in Figure 4. The r values are −0.757, 0.287, and −0.830 in all subjects, the non-fever group and the fever group, respectively.
The AUC, calculated from the ROC, of each entropy variables are shown in Table 2 The AUC of CDF(E(k = 19)) had the highest value of 0.915, the sensitivity is 0.933, and the specificity is 0.833. Figure 5 showed the AUC distribution of E(k) and CDF(E(k)) calculated by using iPR.
For comparison with conventional PRV time series, Table 3 showed the AUC of the above variables calculated by using the PPi series. The AUC of all variables related to the entropy value of the PPi series was lower than the CDF(E(k = 19)) of the iPR.
4. Discussion
4.1. Body Temperature and iPRV
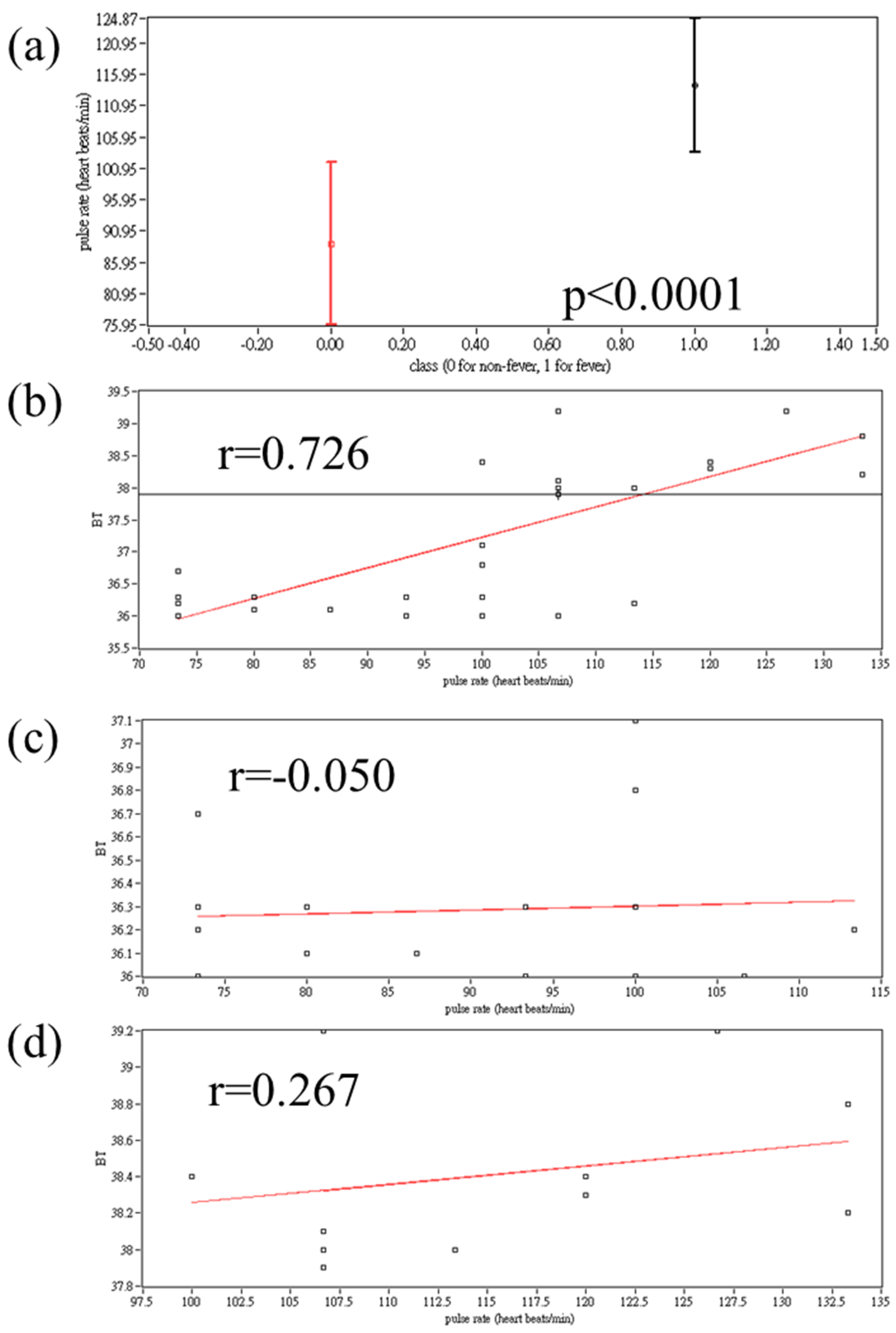
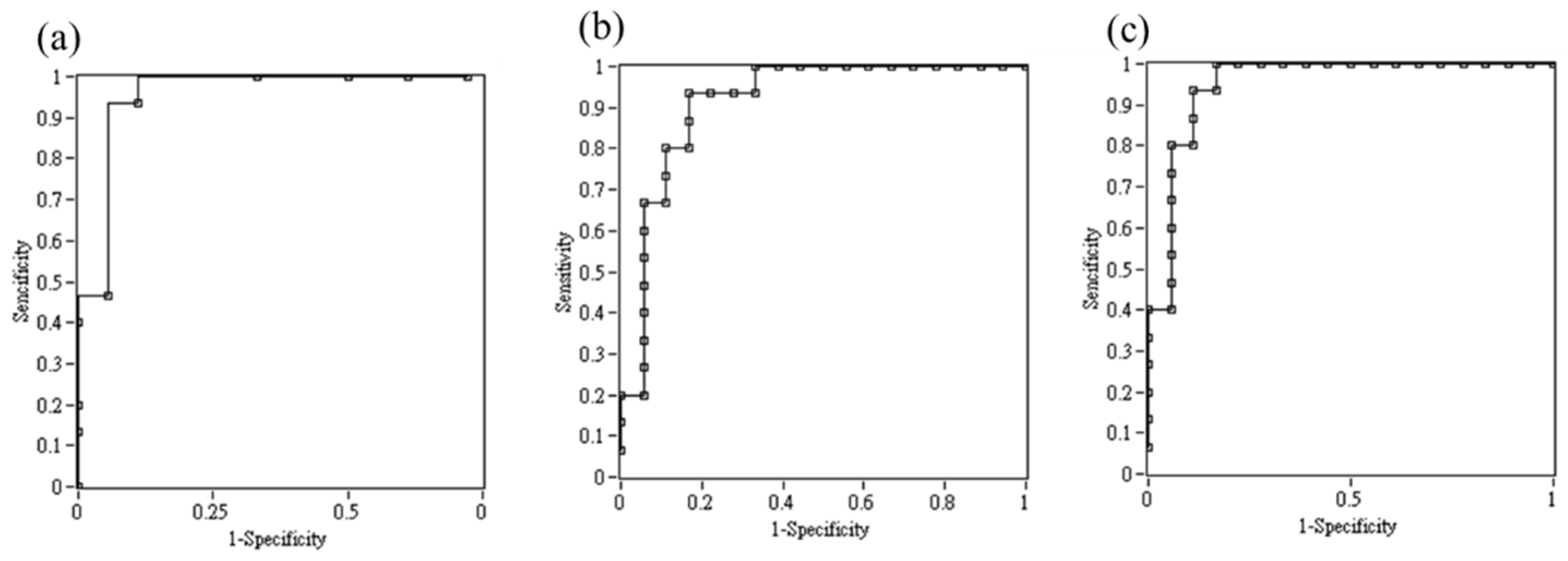
Since humans are warm-blooded animals, we need to maintain our body temperature in a fixed range. However, while our bodies are infected by germs, to increase the power of immune body temperature, the corresponding organs should be regulated by ANS [20,25]. Increase heart rate by the sympathetic nervous system (SNS) and vasoconstriction, for example. Some studies showed the relationship between thermoregulation and HRV [26,27]. Their result showed that the very low frequency band power (VLF) had a corresponding change, while the core body temperature or the environment temperature changed. However, they did not discuss the situation of fever. Moreover, to indicate a meaningful VLF, the signal length should be longer [1]. Our previous studies still showed that conventional nLF and nHF in patients with fever were different from those without fever [28]. Furthermore, we also examined whether the conventional frequency band indices in iPRV are similar to the indices in conventional HRV in our previous work in the time and frequency domain [14,15]. nLF and nHF calculated by iPRV actually showed the difference in ANS activity between patients with fever and people without fever. For non-linear dynamic analysis, the higher resolution time series can present much detail about the complexity of the time series. The CDF(E(k = 19)) of the iPR series also had a higher AUC than the CDF(E(k)) of PPi, whatever k. Therefore, the following term CDF(E(k = 19)) is denoted as the one of iPR series. Table 4 and Table 5 show the AUC calculated by time- and frequency domains of iPRV and PRV. Only pulse rate and mean (PPi) had a higher AUC than CDF(E(k = 19)). In addition to Mean(PPi), Mean(iPR) also had a high AUC, but it is because they are directly correlated with pulse rate. Although pulse rate differences are found between patients with fever and non-fever (p < 0.001), only pulse rate to find patients with fever is not enough. Influencing pulse rate is so easy. For example, the pulse rate of someone after exercise also possibly had a high pulse rate which is similar to the pulse rate of patients with fever. The pulse rate distribution is shown in Figure 6a. The pulse rate in the fever group is significantly higher than in the non-Fever group. The difference between pulse rate and CDF(E(k = 19)) is that CDF(E(k = 19)) had a high correlation compared to body temperature in the ever group, but the correlation was low between pulse rate and body temperature in the fever group (Figure 4c and Figure 6d). For patients suffering from fever, autoregulation of not only their ANS but also peripheral response. The CDF(E(k = 19)) may correspond to this reflection of autoregulation or the severity of the disease. CDF(E(k = 19)) had a higher absolute correlation |r| compared to pulse rate in each group and total subjects (Total: 0.757 vs. 0.726; Non-fever group: 0.287 vs. 0.05; Fever group: 0.830 vs. 0.267). It showed that CDF (E (k = 19)) is not directly affected by pulse rate. Body temperature, ANS activity, or peripheral response may be the possible factors that affect the CDF(E(k = 19)), especially in the Fever group. Applying logistic regression using pulse rate and CDF(E(k = 19)) can increase AUC. Using these two indices to detect patients with fever may be more reliable (Table 6 and Figure 7).
4.2. Apply Short-Term PPG for CEEMD and Entropy Analysis
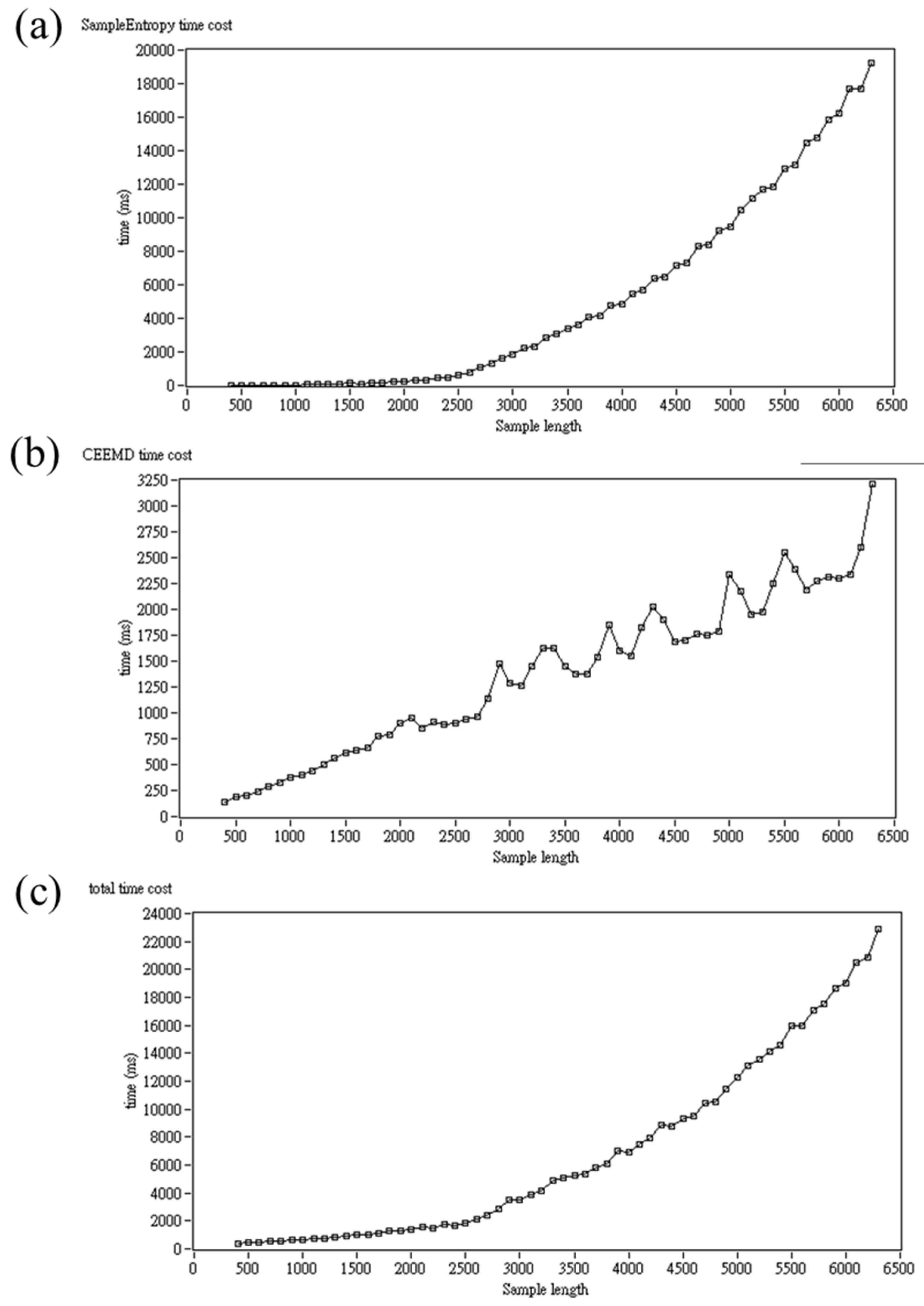
Figure 8 showed the time cost of SampEn, CEEMD, and the total time cost. The total time cost is dominated mainly by SampEn. When the sample length is larger than 3000 points, the total time cost is around 2 to 4 s. In addition, five minutes of heartbeats is needed for conventional HRV analysis [1]. These limitations restrict the development of real-time HRV application. Therefore, in this study, only 15 s were recorded for signal processing. However, the output of CEEMD had a boundary effect problem, the first 2.5 s signal and the last 2.5 s signal were eliminated. Total 10 s signal used for iPRV and TSME analysis. The time cost is only about 2 s. Because iPRV breaks the time resolution problem in HRV, the resolution of short-term time series is still enough for time and frequency-domain analysis [11,22]. For non-linear dynamic analysis, the SampEn is sensitive to sample length [17]. Some research suggests that the sample length N should be larger than 200 points for more consistent findings [29]. However, the effect of multiscale entropy analysis still needs further examination. In addition, the basic algorithm of SampEn, the cost of time is O(n2), was applied in this study [17]. Some algorithms can reduce the time cost of SampEn calculation [30]. Moreover, the parameter settings of SampEn and TSME are important. In this work, we follow the same setting as Pham, who proposed the TSME [19]. However, it is unknown whether it is the best setting for this study. In future studies, the testing of a different combination of parameter settings is necessary. Research proposed the quadratic sample entropy (QSE) method to dynamically vary the parameter r to reduce the influence of the parameter [31]. Applying the QSE may be a solution for further study.
4.3. Fever Detection and Application
To measure body temperature, the most common and easy way is using a thermometer. However, it is hard to measure body temperature continuously with a thermometer. Another way to measure body temperature is to use a thermographic camera. The thermography camera is usually used for measuring the body temperature measurement at the same time. However, the price of a thermographic camera is not cheap. Therefore, in this study, we proposed a new method for detecting fever by using a very short-term PPG signal. Although our method cannot measure body temperature directly, detecting fever is more important. Especially in the ICU, it is necessary to monitor patients who have a fever. Fever is also a common sign of many infectious diseases and non-infectious diseases. Using a thermometer to measure body temperature is a cost of manpower and cannot be measured continuously. Using a thermographic camera is too expensive. However, PPG has been widely used in ICU for pulse oximetry and breathing measurement. Moreover, measuring PPG through the camera of a mobile is also available. In addition, iPRV can also provide not only ANS but also peripheral circulation information using short-term PPG [11,14,22,28]. For homecare or other application, PPG is a cheap and non-invasive measurement, and can be applied to many situations. For example, PPG can be integrated with the watch or the camera of a cell phone can measure the PPG signal as well. Furthermore, the non-contact PPG is also developing [32,33,34,35]. The PPG has the potential to be the health monitor in many situations.
4.4. Limitations
Some limitations remain in this study. The first is a small population of subjects. The second is that only 7 to 18 years are recruited for this study. Although the response to autoregulation in 7 to 18 years is stronger, whether the age influence the result of this study is unknown. Therefore, to recruiting more subjects and researching the influence of age is further work. The third is we only recruited the fever as a high body temperature group. Fever is not the only way to increase body temperature. For example, someone after exercise also may have a high body temperature. The difference between the fever group and the after-exercise group depends on whether the set point changes or not. In other words, if a person without fever has a high body temperature, the hypothalamus and ANS will tend to decrease body temperature. For example, a decrease in heart rate or vasodilation. Current research has examined the difference between the fever group and the low body temperature group. However, it is currently unknown whether research can distinguish the reasons for high body temperature is unknown. Recruiting other groups with high body temperature due to other reasons to compare the difference among each other is also important for further research.
Additionally, the PRV result is only for reference in this study. Actually, for conventional PRV or HRV analysis, the 5 min signal is suggested [1]. Nevertheless, for comparison with iPRV, this study only applied a 15 s PPG signal for PRV analysis which may lead to the result being meaningless or not stable enough. However, the result of the iPR series or iPRV would not be influenced by this limitation.
5. Conclusions
In this study, we propose a new signal processing method for continuous fever detection by using a very short-term PPG signal. The result showed that the multiscale entropy of the iPR series is useful for fever detection. Moreover, the variables calculated by iPRV and TSME had the potential to be an indicator of autoregulation. The short-term PPG signal is suitable to develop real-time application and multiscale entropy provide different scales of information for daily healthcare.
Author Contributions
Conceptualization, P.-H.H.; methodology, P.-H.H.; validation, P.-H.H. and T.-C.H.; formal analysis, P.-H.H.; investigation, P.-H.H.; data curation, P.-H.H.; writing—original draft preparation, P.-H.H.; writing—review and editing, P.-H.H. and T.-C.H.; visualization, P.-H.H.; supervision, T.-C.H.; funding acquisition, T.-C.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was fully supported by Taiwan Ministry of Science and Technology under grant number MOST-105-2221-E-009-159, MOST 105-2634-E-009-003, and MOST109-2221-E-009-117-MY3, and in part by “Aim for the Top University Plan” of National Chiao Tung University and Ministry of Education, Taiwan, R.O.C.
Institutional Review Board Statement
This experiment was approved by the Research Ethics Committee for Human Subject Protection of the National Chiao Tung University (NCTU-REC-103-061; date of approval: 2 June 2015).
Informed Consent Statement
Written informed consent has been obtained from the participate(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Acknowledgments
We would like to thanks Chin-Yi Huang who is the pediatrician of Yo-Yo Pediatric Clinic, Kaohsiung, Taiwan, to help us recruit the subjects. We also would like to thanks Menu-Ru Li help us revise some sentences with his clinical experiences.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ANS | Autonomic nervous system |
| AUC | Area under curve |
| CDF | Cumulative distribution function |
| CEEMD | Complete ensemble EMD |
| ECG | Electrocardiography |
| EMD | Empirical mode decomposition |
| HF | High frequency power |
| HFD | Higuchi’s fractal dimension |
| HHT | Hilbert-Huang transform |
| HRV | Heart rate variability |
| ICU | Intensive care unit |
| IMF | Intrinsic mode function |
| iPR | Instantaneous pulse rate |
| iPRV | Instantaneous pulse rate variability |
| LF | Low frequency power |
| NDQ | Normalized direct quadrature |
| NHT | Normalized Hilbert transform |
| NNs | Normal-to-normal intervals |
| NN50 | Number of pairs of NNs larger than 50 ms |
| PAT | Pulse arrival time |
| pNN50 | Proportion of NN50 divided by total number of NNs |
| PPG | Photoplethysmography |
| PPi | Pulse-to-pulse interval |
| PRV | Pulse rate variability |
| QSE | Quadratic sample entropy |
| ROC | Receiver operating characteristic |
| RRi | Beat-to-beat interval |
| SampEn | Sample entropy |
| SDNN | Standard deviation of NN |
| SNS | Sympathetic nervous system |
| TP | Total power |
| TSME | Time-Shift Multiscale Entropy |
| VHF | Very high frequency power |
| VLF | Very low frequency power |
References
- Electrophysiology, Task Force of the European Society of Cardiology the North American Society of Pacing. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Berger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Farrell, T.G.; Bashir, Y.; Cripps, T.; Malik, M.; Poloniecki, J.; Bennett, E.; Ward, D.E.; Camm, A. Risk stratification for arrhythmic events in postinfarction patients based on heart rate variability, ambulatory electrocardiographic variables and the signal-averaged electrocardiogram. J. Am. Coll. Cardiol. 1997, 18, 687–697. [Google Scholar] [CrossRef] [Green Version]
- Javorka, M.; Zila, I.; Balhárek, T. Heart rate recovery after exercise: Relations to heart rate variability and complexity. Braz. J. Med. Biol. Res. 2002, 35, 991–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kageyama, T.; Kabuto, M.; Kaneko, T.; Nishikido, N. Accuracy of Pulse Rate Variability Paramete Obtained from Finger Plethysmogram: A Comparison with Heart Rate Variability Parameters Obtained from ECG. J. Occup. Health 1997, 39, 154–155. [Google Scholar] [CrossRef]
- Gil, E.; Orini, M.; Bailón, R.; Vergara, J.M.; Mainardi, L.; Laguna, P. Photoplethysmography pulse rate variability as a surrogate measurement of heart rate variability during non-stationary conditions. Physiol. Meas. 2010, 31, 1271–1290. [Google Scholar] [CrossRef]
- Kumar, C.K.; Manaswini, M.; Maruthy, K.; Kumar, A.S.; Kumar, K.M. Association of Heart rate variability measured by RR interval from ECG and pulse to pulse interval from Photoplethysmography. Clin. Epidemiol. Glob. Health 2021, 10, 100698. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 2007, 34, 623–648. [Google Scholar] [CrossRef]
- Chang, C.-C.; Hsiao, T.-C.; Hsu, H.-Y. Frequency range extension of spectral analysis of pulse rate variability based on Hilbert–Huang transform. Med. Biol. Eng. Comput. 2014, 52, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.C.; Tung, C.C.; Liu, H.H. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proc. R. Soc. London Ser. A-Math. Phys. Eng. Sci. 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Huang, N.E.; Wu, Z.; Long, S.R.; Arnold, K.C.; Chen, X.; Blank, K. On instantaneous frequency. Adv. Adapt. Data Anal. 2009, 1, 177–229. [Google Scholar] [CrossRef]
- Huang, P.-H.; Chang, C.-C.; Hsiao, T.-C. An ultra-band study of pulse rate variability for homecare by using instantaneous pulse rate variability. In Proceedings of the Ninth International Conference on eHealth, Telemedicine, and Social Medicine, Nice, France, 19 March– 23 March 2017; pp. 76–79. [Google Scholar]
- Lin, P.-C.; Huang, P.-H.; Chang, C.-C.; Hsu, H.-Y.; Hsiao, T.-C. A novel index of photoplethysmography by using instantaneous pulse rate variability during non-stationary condition. In Proceedings of the 2015 IEEE International Conference on Consumer Electronics, Taipei, China, 6 June 2015; pp. 100–101. [Google Scholar]
- Shannon, C.E. Prediction and entropy of printed English. Bell Syst. Tech. J. 1951, 30, 50–64. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol-Heart Circul. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.F.; Lin, P.Y.; Chao, H.H.; Hsu, L.; Chi, S. Average Entropy: Measurement of disorder for cardiac RR interval signals. Physica A 2019, 529, 121533. [Google Scholar] [CrossRef]
- Pham, T.D. Time-shift multiscale entropy analysis of physiological signals. Entropy 2017, 19, 257. [Google Scholar] [CrossRef]
- Nakamura, K. Central circuitries for body temperature regulation and fever. Am J Physiol-Reg I 2011, 301, R1207–R1228. [Google Scholar] [CrossRef] [Green Version]
- Achaiah, N.C.; Ajith Kumar, A.K. Fever in the Intensive Care Patient. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK570583/ (accessed on 23 June 2022).
- Lin, P.-C.; Chang, C.-C.; Hsiao, T.-C.; Hsu, H.-Y. A short-term assessment of cardiac output by using instantaneous pulse rate variability. In Proceedings of the Eighth International Conference on eHealth, Telemedicine, and Social Medicine, Venice, Italy, 24–28 April 2016; pp. 110–115. [Google Scholar]
- Yeh, J.R.; Shieh, J.S.; Huang, N.E. Complementary ensemble empirical mode decomposition: A novel noise enhanced data analysis method. Adv. Adapt. Data Anal. 2010, 2, 135–156. [Google Scholar] [CrossRef]
- Higuchi, T. Approach to an irregular time series on the basis of the fractal theory. Physica D 1988, 31, 277–283. [Google Scholar] [CrossRef]
- Bergström, R.M. Physiology of the autonomic nervous system. Acta Anaesth. Scand. 1964, 8, 17–20. [Google Scholar] [CrossRef]
- Sollers, J.J.; Sanford TNabors-Oberg, A.R.; Anderson, C.A.; Thayer, J.F. Examining changes in HRV in response to varying ambient temperature. IEEE Eng. Med. Biol. Mag. 2002, 21, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, L.A.; Frank, S.M.; Sessler, D.I.; Cheng, C.; Matsukawa, T.; Vannier, C.A. Thermoregulation and heart rate variability. Clin. Sci. 1996, 90, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, P.-H.; Chang, C.-C.; Huang, C.-Y.; Hsiao, T.-C. Can very high frequency instantaneous pulse rate variability serve as an obvious indicator of peripheral circulation? J. Commun. Comput. 2017, 14, 65–72. [Google Scholar]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The appropriate use of approximate entropy and sample entropy with short data sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Manis, G.; Aktaruzzaman, M.; Sassi, R. Low computational cost for sample entropy. Entropy 2018, 20, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirugeda-Roldán, E.M.; Cuesta-Frau, D.; Miró-Martínez Oltra-Crespo, P.S.; Vigil-Medina, L.; Varela-Entrecanales, M. A new algorithm for quadratic sample entropy optimization for very short biomedical signals: Application to blood pressure records. Comput. Methods Programs Biomed. 2014, 114, 231–239. [Google Scholar] [CrossRef]
- Moreno, J.; Ramos-Castro, J.; Movellan, J.; Parrado, E.; Rodas, G.; Capdevila, L. Facial video-based photoplethysmography to detect HRV at rest. Int. J. Sports Med. 2015, 36, 474–480. [Google Scholar] [CrossRef]
- Sun, Y.; Thakor, N. Photoplethysmography revisited: From contact to noncontact, from point to imaging. IEEE Trans. Biomed. Eng. 2015, 63, 463–477. [Google Scholar] [CrossRef] [Green Version]
- McDuff, D.J.; Blackford, E.B.; Estepp, J.R. The impact of video compression on remote cardiac pulse measurement using imaging photoplethysmography. In Proceedings of the 2017 12th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2017), Washington, DC, USA, 30 May–3 June 2017; pp. 63–70. [Google Scholar]
- Shoushan, M.M.; Reyes, B.A.; Rodriguez, A.R.M.; Chong, J.W. Contactless monitoring of heart rate variability during respiratory maneuvers. IEEE Sens. J. 2022. [Google Scholar] [CrossRef]
Figure 1.
Demonstration of signal processing.

Figure 2.
Example of different time scale E(k = 1~20) of iPR.

Figure 3.
Distribution of CDF(E(k = 19)) of iPR of 2 groups (0 for the non-Fever group; 1 for Fever group) and the value of p.
Figure 3.
Distribution of CDF(E(k = 19)) of iPR of 2 groups (0 for the non-Fever group; 1 for Fever group) and the value of p.

Figure 4.
Linear fitting and Spearman r value between body temperature and CDF(E(k = 19)) of iPR in (a) total subjects; (b) non-fever group; (c) Fever group.
Figure 4.
Linear fitting and Spearman r value between body temperature and CDF(E(k = 19)) of iPR in (a) total subjects; (b) non-fever group; (c) Fever group.

Figure 5.
Distribution of AUC of E(k) of iPR (left), and CDF(E(k)) of iPR (right).

Figure 6.
(a) Distribution of pulse rate of 2 groups; (b–d) Linear fitting and Spearman r value between body temperature and pulse rate in (b) total subjects; (c) Non-fever group; (d) Fever group.
Figure 6.
(a) Distribution of pulse rate of 2 groups; (b–d) Linear fitting and Spearman r value between body temperature and pulse rate in (b) total subjects; (c) Non-fever group; (d) Fever group.

Figure 7.
ROC curve of (a) pulse rate; (b) CDF(E(19)) of iPR; (c) logistic model of pulse rate and CDF(E(19)) of iPR.
Figure 7.
ROC curve of (a) pulse rate; (b) CDF(E(19)) of iPR; (c) logistic model of pulse rate and CDF(E(19)) of iPR.

Figure 8.
Computing time cost of (a) SampEn; (b) CEEMD; (c) total time cost.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Basic information of subjects.
| Non-Fever Group | Fever Group | Total | |
|---|---|---|---|
| # of subjects | 18 | 15 | 33 |
| # of boy | 11 | 10 | 21 |
| age | 10.78 ± 3.15 | 10.4 ± 2.38 | 10.60 ± 2.79 |
| Body temperature (°C) | 36.28 ± 0.30 * | 38.4 ± 0.47 | 37.25 ± 1.14 |
* p < 0.05 compared to the Fever group.
Table 2.
The AUC of variables related to the entropy value of iPR.
| Variable | AUC | Sensitivity | Specificity |
|---|---|---|---|
| Mean(E(k = 1~20)) | 0.659 | 0.667 | 0.722 |
| std(E(k = 1~20)) | 0.681 | 0.733 | 0.611 |
| Max(E(k = 1~20)) | 0.567 | 0.467 | 0.778 |
| Min(E(k = 1~20)) | 0.657 | 0.667 | 0.778 |
| Area(E(k = 1~20)) | 0.663 | 0.667 | 0.722 |
| E(k = 4) | 0.685 | 0.733 | 0.778 |
| CDF(E(k = 19)) | 0.915 | 0.933 | 0.833 |
Table 3.
The AUC of the variables related to the entropy value of PPi.
| Variable | AUC | Sensitivity | Specificity |
|---|---|---|---|
| Mean(E(k = 1~20)) | 0.678 | 0.600 | 0.722 |
| std(E(k = 1~20)) | 0.689 | 0.800 | 0.667 |
| Max(E(k = 1~20)) | 0.678 | 0.800 | 0.611 |
| Min(E(k = 1~20)) | 0.678 | 0.800 | 0.556 |
| Area(E(k = 1~20)) | 0.678 | 0.600 | 0.722 |
| E(k = 4) | 0.689 | 0.800 | 0.611 |
| CDF(E(k = 19)) | 0.745 | 0.733 | 0.722 |
Table 4.
The AUC of time and frequency domain indices of iPRV.
| Variable | AUC | Sensitivity | Specificity |
|---|---|---|---|
| Mean(iPR) | 0.914 | 0.867 | 0.889 |
| std(iPR) | 0.730 | 0.733 | 0.722 |
| LF | 0.7 | 0.667 | 0.722 |
| HF | 0.826 | 0.733 | 0.889 |
| VHF | 0.763 | 0.733 | 0.778 |
| LF/HF | 0.620 | 0.667 | 0.722 |
| nLF a | 0.620 | 0.667 | 0.722 |
| nHF a | 0.620 | 0.667 | 0.722 |
| nLF b | 0.630 | 0.533 | 0.944 |
| nHF b | 0.672 | 0.8 | 0.556 |
| nVHF b | 0.507 | 0.733 | 0.444 |
| Pulse rate | 0.944 | 0.933 | 0.889 |
a calculated total power including VHF; b calculated total power excluding VHF.
Table 5.
The AUC of time and frequency domain indices of PRV.
| Variable | AUC | Sensitivity | Specificity |
|---|---|---|---|
| Mean(PPi) | 0.944 | 1 | 0.889 |
| std(PPi) | 0.792 | 0.8 | 0.833 |
| LF | 0.733 | 0.8 | 0.667 |
| HF | 0.837 | 0.867 | 0.889 |
| LF/HF | 0.702 | 0.733 | 0.722 |
| nLF | 0.702 | 0.733 | 0.722 |
| nHF | 0.702 | 0.733 | 0.722 |
Table 6.
Logistic model of pulse rate and CDF(E(19)).
| Logistic Model | AUC | Sensitivity | Specificity |
|---|---|---|---|
| −1.28 + 0.02 Pulse rate-1.57CDF(E(k = 19)) | 0.952 | 0.933 | 0.889 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Huang, P.-H.; Hsiao, T.-C. Very Short-Term Photoplethysmography-Based Heart Rate Variability for Continuous Autoregulation Assessment. Appl. Sci. 2022, 12, 6469. https://0-doi-org.brum.beds.ac.uk/10.3390/app12136469
AMA Style
Huang P-H, Hsiao T-C. Very Short-Term Photoplethysmography-Based Heart Rate Variability for Continuous Autoregulation Assessment. Applied Sciences. 2022; 12(13):6469. https://0-doi-org.brum.beds.ac.uk/10.3390/app12136469
Chicago/Turabian StyleHuang, Po-Hsun, and Tzu-Chien Hsiao. 2022. "Very Short-Term Photoplethysmography-Based Heart Rate Variability for Continuous Autoregulation Assessment" Applied Sciences 12, no. 13: 6469. https://0-doi-org.brum.beds.ac.uk/10.3390/app12136469
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.