
Relationship between Carotid Artery Calcification and Periodontitis in the Saudi Population: A Retrospective Study

 ,
,
Abstract
:1. Introduction
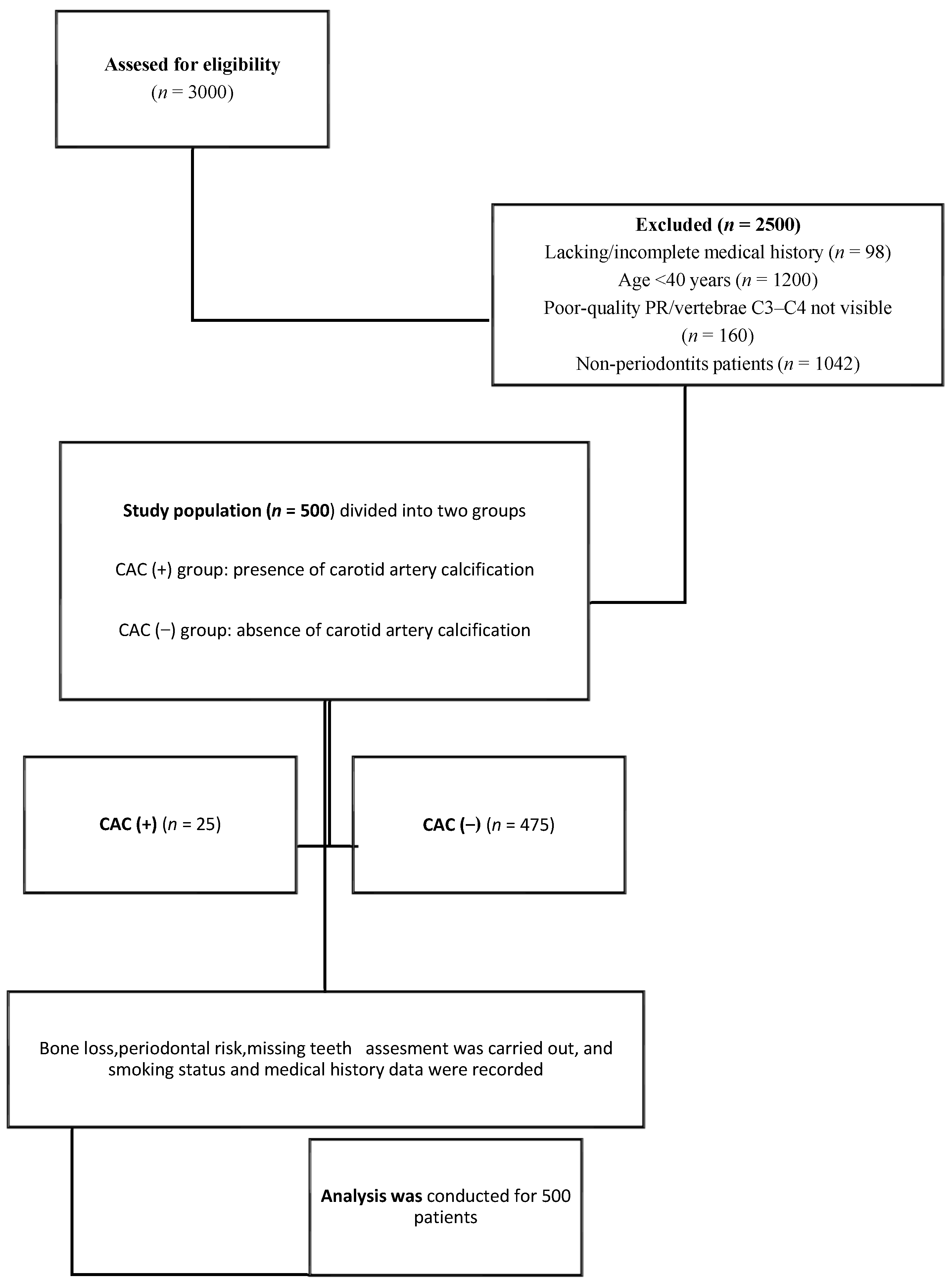
2. Material and Methods
2.1. Study Design
2.2. Assessment of Carotid Artery Calcification in Panoramic Radiographs
2.3. Data Collection
2.4. Assessment of Percentage of Alveolar Bone Loss
2.5. Number of Missing Teeth
2.6. Assessment of Periodontal Risk [46]
2.7. Statistical Analysis
3. Result
3.1. Prevalence and Distribution of Carotid Artery Calcification
3.2. Gender and Carotid Artery Calcification
3.3. Age and Carotid Artery Calcification
3.4. Smoking and Carotid Artery Calcification
3.5. Percentage of Alveolar Bone Loss and Carotid Artery Calcification
3.6. Number of Missing Teeth
3.7. Periodontal Risk
3.8. Systemic Diseases and Carotid Artery Calcification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alves, N.; Deana, N.F.; Garay, I. Detection of common carotid artery calcifications on panoramic radiographs: Prevalence and reliability. Int. J. Clin. Exp. Med. 2014, 7, 1931–1939. [Google Scholar]
- Van Gils, M.J.; Vukadinovic, D.; van Dijk, A.C.; Dippel, D.W.; Niessen, W.J.; van der Lugt, A. Carotid atherosclerotic plaque progression and change in plaque composition over time: A 5-year follow-up study using serial CT angiography. AJNR Am. J. Neuroradiol. 2012, 33, 1267–1273. [Google Scholar] [CrossRef]
- Shi, X.; Gao, J.; Lv, Q.; Cai, H.; Wang, F.; Ye, R.; Liu, X. Calcification in atherosclerotic plaque vulnerability: Friend or foe? Front. Physiol. 2020, 11, 56. [Google Scholar] [CrossRef]
- VVos, A.; Kockelkoren, R.; de Vis, J.B.; van der Schouw, Y.T.; van der Schaaf, I.C.; Velthuis, B.K.; Mali, W.P.; de Jong, P.A.; Majoie, C.B.; Roos, Y.B.; et al. Risk factors for atherosclerotic and medial arterial calcification of theintracranial internal carotid artery. Atherosclerosis 2018, 276, 44–49. [Google Scholar] [CrossRef]
- Song, P.; Fang, Z.; Wang, H.; Cai, Y.; Rahimi, K.; Zhu, Y.; Fowkes, F.G.R.; Fowkes, F.J.; Rudan, I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: A systematic review, meta-analysis, and modelling study. Lancet Glob. Health 2020, 8, 721–729. [Google Scholar] [CrossRef]
- Çetin, M.B.; Sezgin, Y.; Yilmaz, M.N.N.; Seçgin, C.K. Assessment of Carotid Artery Calcifications on Digital Panoramic Radiographs and Their Relationship with Periodontal Condition and Cardiovascular Risk Factors. Int. Dent. J. 2021, 71, 160–166. [Google Scholar] [CrossRef]
- Senosiain-Oroquieta, A.; Pardo-Lopez, B.; De Carlos-Villafranca, F.; Cobo-Plana, J. Detección de placas de ateroma mediante radiografías dentales. RCOE 2006, 11, 297–303. [Google Scholar] [CrossRef]
- Romano-Sousa, C.M.; Krejci, L.; Medeiros, F.M.M.; Graciosa-Filho, R.G.; Martins, M.F.F.; Guedes, V.N.; Fenyo-Pereira, M. Diagnostic agreement between panoramic radiographs and color doppler images of carotid atheroma. J. Appl. Oral Sci. 2009, 17, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; McPherson, R.; Abruzzo, A.; Thomas, S.E.; Gorantla, V.R. Carotid Artery Calcification: What We Know So Far. Cureus 2021, 13, e18938. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Tempel, D.; van Haperen, R.; van der Baan, A.; Grosveld, F.; Daemen, M.J.; Krams, R.; de Crom, R. Atherosclerotic lesion size and vulnerability are determined by patterns of fluid shear stress. Circulation 2006, 113, 2744–2753. [Google Scholar] [CrossRef] [PubMed]
- Top Ten Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 23 May 2023).
- World Health Organization—Noncommunicable Diseases (NCD) Country Profiles. 2018. Available online: https://www.who.int/publications/i/item/9789241514620 (accessed on 18 July 2022).
- Bos, D.; Leening, M.J.; Kavousi, M.; Hofman, A.; Franco, O.H.; van der Lugt, A.; Vernooij, M.W.; Ikram, M.A. Comparison of atherosclerotic calcification in major vessel beds on the risk of all-cause and cause-specific mortality: The Rotterdam study. Circ. Cardiovasc. Imaging 2015, 8, e003843. [Google Scholar] [CrossRef]
- Wyman, R.A.; Fraizer, M.C.; Keevil, J.G.; Busse, K.L.; Aeschlimann, S.E.; Korcarz, C.E. Ultrasound detected carotid plaque as a screening tool for advanced subclinical atherosclerosis. Am. Heart J. 2005, 150, 1081–1085. [Google Scholar] [CrossRef]
- Ariayi, A.S.; Berndt, D.; Lambrecht, J.T. Panoramic radiography for diagnosis of soft tissue calcifications—An aid to identify stroke prone patients? Schweiz Monatsschr Zahnmed 2009, 119, 1009–1013. (In German) [Google Scholar]
- Saxena, A.; Ng, E.Y.; Lim, S.T. Imaging modalities to diagnose carotid artery stenosis: Progress and prospect. Biomed. Eng. Online 2019, 18, 66. [Google Scholar] [CrossRef]
- Derlin, T.; Richter, U.; Bannas, P.; Begemann, P.; Buchert, R.; Mester, J.; Klutmann, S. Feasibility of 18F-sodium fluoride PET/CT for imaging of atherosclerotic plaque. J. Nucleic Med. 2010, 51, 862–865. [Google Scholar] [CrossRef]
- Derlin, T.; Wisotzki, C.; Richter, U.; Apostolova, I.; Bannas, P.; Weber, C.; Mester, J.; Klutmann, S. In vivo imaging of mineral deposition in carotid plaque using 18Fsodium fluoride PET/CT: Correlation with atherogenic risk factors. J. Nucl. Med. 2011, 52, 362–368. [Google Scholar] [CrossRef]
- Derlin, T.; Tóth, Z.; Papp, L.; Wisotzki, C.; Apostolova, I.; Habermann, C.R.; Mester, J.; Klutmann, S. Correlation of inflammation assessed by 18F-FDG PET, active mineral deposition assessed by 18F-fluoride PET, and vascular calcification in atherosclerotic plaque: A dual-tracer PET/CT study. J. Nucleic Med. 2011, 52, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, P.B.; Bolger, A.F.; Papapanou, P.N.; Osinbowale, O.; Trevisan, M.; Levison, M.E.; Taubert, K.A.; Newburger, J.W.; Gornik, H.L.; Gewitz, M.H.; et al. Periodontal disease and atherosclerotic vascular disease: Does the evidence support an independent association? A scientific statement from the American Heart Association. Circulation 2012, 125, 2520–2544. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Bartold, P.M. Periodontal health. J. Periodontol. 2018, 89, S9–S16. [Google Scholar] [PubMed]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global burden of severe periodontitis in 1990−2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Lin, X.; Zheng, P.; Chen, H. Inflammatory cytokine levels in patients with periodontitis and/or coronary heart disease. Int. J. Clin. Exp. Pathol. 2015, 8, 2214. [Google Scholar]
- DeStefano, F.; Anda, R.F.; Kahn, H.S.; Williamson, D.F.; Russell, C.M. Dental disease and risk of coronary heart disease and mortality. BMJ 1993, 306, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Bahekar, A.A.; Singh, S.; Saha, S.; Molnar, J.; Arora, R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: A meta-analysis. Am. Heart J. 2007, 154, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Velsko, I.M.; Chukkapalli, S.S.; Rivera, M.F.; Lee, J.-Y.; Chen, H.; Zheng, D.; Bhattacharyya, I.; Gangula, P.R.; Lucas, A.R.; Kesavalu, L. Active invasion of oral and aortic tissues by Porphyromonas gingivalis in mice causally links periodontitis and atherosclerosis. PLoS ONE 2014, 9, e97811. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.; Herrera, D.; Kozarov, E.; Roldan, S.; Progulske-Fox, A. Periodontal bacterial invasion and infection: Contribution to atherosclerotic pathology. J. Clin. Periodontol. 2013, 40, S30–S50. [Google Scholar] [CrossRef] [PubMed]
- AlSakr, A.; Blanchard, S.; Wong, P.; Thyvalikakath, T.; Hamada, Y. Association between intracranial carotid artery calcifications and periodontitis: A cone-beam computed tomography study. J. Periodontol. 2021, 92, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.F.; Genco, R.J.; Cohen, D.W.; Mealey, B.L. Periodontal Medicine; BC Decker: Hamilton, ON, Canada, 2000. [Google Scholar]
- Schenkein, H.A.; Loos, B.G. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J. Clin. Periodontol. 2013, 40, S51–S69. [Google Scholar] [CrossRef]
- Haraszthy, V.I.; Zambon, J.J.; Trevisan, M.; Zeid, M.; Genco, R.J. Identification of periodontal pathogens in atheromatous plaques. J. Periodontol. 2000, 71, 1554–1560. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Lande, A. Panoramic radiographic identification of carotid arterial plaques. Oral Surg. Oral Med. Oral Pathol. 1981, 52, 102–104. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Baker, J.D. Panoramic radiography: An aid in detecting patients at risk of cerebrovascular accident. J. Am. Dent. Assoc. 1994, 125, 1598–1603. [Google Scholar] [CrossRef]
- Roldán-Chicano, R.; Oñate-Sánchez, R.E.; López-Castaño, F.; Cabrerizo-Merino, M.C.; Martínez López, F. Panoramic radiograph as a method for detecting calcified atheroma plaques. Review of literature. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, E261–E266. [Google Scholar]
- Ahmad, M.; Madden, R.; Perez, L. Triticeous cartilage: Prevalence on panoramic radiographs and diagnostic criteria. Oral Surg Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 99, 225–230. [Google Scholar] [CrossRef]
- Bengtsson, V.W.; Persson, G.R.; Renvert, S. Assessment of carotid calcifications on panoramic radiographs in relation to other used methods and relationship to periodontitis and stroke: A literature review. Acta Odontol. Scand. 2014, 76, 401–412. [Google Scholar] [CrossRef]
- Khosropanah, S.H.; Shahidi, S.H.; Bronoosh, P.; Rasekhi, A. Evaluation of carotid calcification detected using panoramic radiography and carotid Doppler sonography in patients with and without coronary artery disease. Br. Dent. J. 2009, 207, 162–163. [Google Scholar] [CrossRef]
- Ravon, N.A.; Hollender, L.G.; McDonald, V.; Persson, G.R. Signs of carotid calcification from dental panoramic radiographs are in agreement with Doppler sonography results. J. Clin. Periodontol. 2003, 30, 1084–1090. [Google Scholar] [CrossRef]
- Beckstrom, B.W.; Horsley, S.H.; Scheetz, J.P.; Khan, Z.; Silveira, A.M.; Clark, S.J.; Greenwell, H.; Farman, A.G. Correlation between carotid area calcifications and periodontitis: A retrospective study of digital panoramic radiographic findings in pretreatment cancer patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 359–366. [Google Scholar] [CrossRef]
- Uthman, A.T.; Al-Saffar, A. Prevalence in digital panoramic radiographs of carotid area calcification among Iraqi individuals with stroke-related disease. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 68–73. [Google Scholar] [CrossRef]
- Alzoman, H.A.; Al-Sadhan, R.E.; Al-Lahem, Z.H.; Al-Sakaker, A.N.; Al-Fawaz, Y.F. Prevalence of carotid calcification detected on panoramic radiographs in a Saudi population from a training institute in Central Saudi Arabia. Saudi Med. J. 2012, 33, 177–181. [Google Scholar]
- Alsweed, A.; Farah, R.; Ps, S.; Farah, R. The Prevalence and Correlation of Carotid Artery Calcifications and Dental Pulp Stones in a Saudi Arabian Population. Diseases 2019, 7, 50. [Google Scholar] [CrossRef]
- Sinjab, A.Z.; Soman, C.; Sahab, L.A. Prevalence of carotid artery calcifications in Riyadh from digital panoramic radiographs and its relationship with cardiovascular disorders: A retrospective cross-sectional study. Saudi J. Oral Sci. 2021, 8, 28–32. [Google Scholar] [CrossRef]
- Bassiouny, M.A.; Grant, A.A. The accuracy of the Schei ruler: A laboratory investigation. J. Periodontol. 1975, 46, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Tonetti, M.S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev. Dent. 2003, 1, 7–16. [Google Scholar]
- Almog, D.M.; Horev, T.; Illig, K.A.; Green, R.M.; Carter, L.C. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Garo, M.; Johansson, E.; Ahlqvist, J.; Jaghagen, E.L.; Arnerlov, C.; Wester, P. Detection of calcifications in panoramic radiographs in patients with carotid stenoses ≥50%. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 385–391. [Google Scholar]
- Lee, J.S.; Kim, O.S.; Chung, H.J.; Kim, Y.J.; Kweon, S.S.; Lee, Y.H.; Shin, M.H.; Yoon, S.J. The correlation of carotid artery calcification on panoramic radiographs and determination of carotid artery atherosclerosis with ultrasonography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 739–745. [Google Scholar] [CrossRef]
- Cohen, S.N.; Friedlander, A.H.; Jolly, D.A.; Date, L. Carotid calcification on panoramic radiographs: An important marker for vascular risk. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Bayram, B.; Uckan, S.; Acikgoz, A.; Müderrisoglu, H.; Aydinalp, A. Digital panoramic radiography: A reliable method to diagnose carotid artery atheromas? Dentomaxillofac. Radiol. 2006, 35, 266–270. [Google Scholar] [CrossRef]
- Ezoddini-Ardakani, F.; Mirzaei, M.; Nayer, S.; Besharati, S.; Moeini, M. Evaluation of Positive Predictive Value for Digital Panoramic Radiography in Comparison to Ultrasound in the Diagnosis of Calcified Carotid Atheroma. Health 2014, 6, 1933–1940. [Google Scholar] [CrossRef]
- Tiller, R.; Bengel, W.; Rinke, S.; Ziebolz, D. Association between carotid area calcifications and periodontal risk: A cross sectional study of panoramic radiographic findings. BMC Cardiovasc. Disord. 2011, 11, 67. [Google Scholar] [CrossRef]
- Nasseh, I.; Aoun, G. Carotid Artery Calcification: A Digital Panoramic-Based Study. Diseases 2018, 6, 15. [Google Scholar] [CrossRef]
- Brand, H.S.; Mekenkamp, W.C.; Baart, J.A. Prevalence of carotid artery calcification on panoramic radiographs. Ned. Tijdschr. Tandheelkd. 2009, 116, 69–73. [Google Scholar]
- Kamak, G.; Yildirim, E.; Rencber, E. Evaluation of the relationship between periodontal risk and carotid artery calcifications on panoramic radiographs. Eur. J. Dent. 2015, 9, 483–489. [Google Scholar] [CrossRef]
- Tamura, T.; Inui, M.; Nakamura, S.; Nakase, M.; Okumura, K.; Tagawa, T. Clinicostatistical study of carotid calcification on panoramic radiographs. Oral Dis. 2005, 11, 314–317. [Google Scholar] [CrossRef] [PubMed]
- Ohba, T.; Takata, Y.; Ansai, T.; Morimoto, Y.; Tanaka, T.; Kito, S.; Awano, S.; Akifusa, S.; Takehara, T. Evaluation of calcified carotid artery atheromas detected by panoramic radiograph among 80-year-olds. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, A.H.; Altman, L. Carotid artery atheromas in postmenopausal women. Their prevalence on panoramic radiographs and their relationship to atherogenic risk factors. J. Am. Dent. Assoc. 2001, 132, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.M.O.; Soares, G.C.; Kurita, L.M. Prevalence of carotid artery calcifications among 2500 digital panoramic radiographs of an adult Brazilian population. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e256. [Google Scholar]
- Patil, S.R. Prevalence of carotid artery calcification in postmenopausal women and its correlation with atherogenic risk factors. J. Nat. Sci. Biol. Med. 2015, 6, S1. [Google Scholar] [CrossRef]
- Dewake, N.; Ishioka, Y.; Uchida, K.; Taguchi, A.; Higashi, Y.; Yoshida, A.; Yoshinari, N. Association between Carotid Artery Calcification and Periodontal Disease Progression in Japanese Men and Women: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 3365. [Google Scholar] [CrossRef] [PubMed]
- Azimi, S.; Sarlak, H.; Tofangchiha, M. Determining the prevalence of carotid artery calcification and associations with medical history using dental panoramic radiographs. Dent. Med. Probl. 2016, 53, 29–33. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, O.S.; Chung, H.J.; Kim, Y.J.; Kweon, S.S.; Lee, Y.H.; Shin, M.H.; Yoon, S.J. The prevalence and correlation of carotid artery calcification on panoramic radiographs and peripheral arterial disease in a population from the Republic of Korea: The Dong-gu study. Dentomaxillofac. Radiol. 2013, 42, 29725099. [Google Scholar] [CrossRef]
- Almog, D.M.; Tsimidis, K.; Moss, M.E.; Gottlieb, R.H.; Carter, L.C. Evaluation of a training program for detection of carotid artery calcifications on panoramic radiographs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 90, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Brito, A.C.; Nascimento, H.A.; Argento, R.; Beline, T.; Ambrosano, G.M.B.; Freitas, D.Q. Prevalence of suggestive images of carotid artery calcifications on panoramic radiographs and its relationship with predisposing factors. Cien. Saude Colet. 2016, 21, 2201–2208. [Google Scholar] [CrossRef]
- Ertas, E.T.; Sisman, Y. Detection of incidental carotid artery calcifications during dental examinations: Panoramic radiography as an important aid in dentistry. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, e11–e17. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.; Soroushian, S.; Ganguly, R. Coincidence of calcified carotid atheromatous plaque, osteoporosis, and periodontal bone loss in dental panoramic radiographs. Imaging Sci. Dent. 2013, 43, 235–243. [Google Scholar] [CrossRef]
- Christou, P.; Leemann, B.; Schimmel, M.; Kiliaridis, S.; Müller, F. Carotid artery calcification in ischemic stroke patients detected in standard dental panoramic radiographs—A preliminary study. Adv. Med. Sci. 2010, 55, 26–31. [Google Scholar] [CrossRef]
- Lankier, J.F. Smoking and cardiovascular disease. Am. J. Med. 1992, 93, S8–S12. [Google Scholar] [CrossRef]
- Monteiro, I.A.; Ibrahim, C.; Albuquerque, R.; Donaldson, N.; Salazar, F.; Monteiro, L. Assessment of carotid calcifications on digital panoramic radiographs: Retrospective analysis and review of the literature. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Atalay, Y.; Asutay, F.; Agacayak, K.S.; Koparal, M.; Adali, F.; Gulsun, B. Evaluation of calcified carotid atheroma on panoramic radiographs and Doppler ultrasonography in an older population. Clin. Interv. Aging 2015, 10, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Engebretson, S.P.; Lamster, I.B.; Elkind, M.S.V.; Rundek, T.; Serman, N.J.; Demmer, R.T. Radiographics measures of chronic periodontitis and carotid artery plaque. Stroke 2005, 36, 561–566. [Google Scholar] [CrossRef]
- Thanakun, S.; Pornprasertsuk-Damrongsri, S.; Izumi, Y. C-reactive protein levels and the association of carotid artery calcification with tooth loss. Oral Dis. 2017, 23, 69–77. [Google Scholar] [CrossRef]
- Andriankaja, O.M.; Genco, R.J.; Dmochowski, J.D.J.; Hovey, K.; Falkner, K.L.; Scannapieco, F.; Trevisan, M. The use of different measurements and definitions of periodontal disease in the study of the association between periodontal disease and risk of myocardial infarction. J. Periodontol. 2006, 77, 1067–1073. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Subcategory | Number of Subjects (%) |
|---|---|---|
| Periodontitis | (n = 500) | |
| Gender | Male | 276 (54.2%) |
| Female | 224 (44.8%) | |
| Age (years) | ≤60 (40–60) | 362 (72.4%) |
| ≥61 (61–90) | 138 (27.6%) | |
| Mean ± SD | 54.64 ± 9.91 | |
| Carotid artery calcification | Present | 25 (5%) |
| Absent | 475 (95%) | |
| Systemic diseases | Diabetes | 52 (10.4%) |
| Hypertension | 36 (7.2%) | |
| Both diabetes and hypertension | 29 (5.8%) | |
| Smoker | Yes | 72 (14.4%) |
| No | 428 (85.6%) | |
| Percentage of alveolar bone loss | Mean ± SD | 40.9 ± 15.49 |
| Number of missing teeth | Mean ± SD | 6.45 ± 5.64 |
| Periodontal risk | Low | 65 (13%) |
| Medium | 270 (54%) | |
| High | 165 (33%) |
| Variables | Subcategory | Number of Subjects (%) (n = 25) |
|---|---|---|
| Appearance of carotid artery calcification | Single | 20 (80%) |
| Multiple | 5 (20%) | |
| Distribution of carotid artery calcification | Bilateral | 13 (52%) |
| Unilateral | 12 (48%) Left side—7 (28%) Right side—5 (20%) |
| Variables | Subcategory | Calcification | p-Value | |
|---|---|---|---|---|
| CAC (−) (n = 475) | CAC (+) Present (n = 25) | |||
| Gender | Male | 274 (57.6%) | 2 (8%) | <0.0001 C (s) |
| Female | 201 (42.3%) | 23 (92%) | ||
| Age (years) | ≤60 | 344 (72.4%) | 18 (72%) | 0.94 C |
| ≥61 | 131 (27.5%) | 7 (28%) | ||
| Mean ± SD | 54.54 ± 9.97 | 55.58 ± 9.49 | 0.3475 MW | |
| Diabetics | Yes | 50 (10.5%) | 2 (8%) | 0.6 C |
| No | 425 (89.4%) | 23 (92) | ||
| Hypertension | Yes | 32 (6.7%) | 4 (16%) | 0.08 C |
| No | 443 (93.2%) | 21 (84%) | ||
| Combination of diabetes and hypertension | Yes | 29 (6.1%) | 0 | 0.2 C |
| No | 446 (93.9%) | 25 (100%) | ||
| Smoker | Yes | 71 (14.9%) | 1 (4%) | 0.12 C |
| No | 404 (85.0%) | 24 (96%) | ||
| Percentage of alveolar bone loss | Mean ± SD | 39.99 ± 15.47 | 41.06 ± 15.49 | 0.005 MW (s) |
| Number of missing teeth | Mean ± SD | 5.3 ± 5.6 | 6.1 ± 6.4 | 0.4 MW |
| Periodontal risk | Low | 58 (12.2%) | 7 (28%) | 0.001 C (s) |
| Medium | 259 (54.5%) | 11 (44%) | ||
| High | 158 (33.2%) | 7 (28%) | ||
| Variables | Subcategory | Age (Years) | |
|---|---|---|---|
| ≤60 (n = 362) | ≥61 (n = 138) | ||
| Gender | Male | 191 (52.76%) | 85 (61.5%) |
| Female | 171 (47.23%) | 53 (38.4%) | |
| Calcification | Present | 18 (4.97%) | 7 (5.08%) |
| Absent | 344 (95.03%) | 131 (94.92%) | |
| Systemic diseases | Diabetes | 32 (8.83%) | 20 (14.4%) |
| Hypertension | 21 (5.80%) | 15 (10.86%) | |
| Combination of hypertension and diabetes | 13 (3.59%) | 16 (11.59%) | |
| Smoker | Yes | 51 (14.08%) | 21 (15.21%) |
| No | 311 (85.91%) | 117 (84.78%) | |
| Percentage of alveolar bone loss | Mean ± SD | 39.6 ± 15.4 | 44.1 ± 15.4 |
| Number of missing teeth | Mean ± SD | 4.6 ± 5.0 | 7.2 ± 6.7 |
| Periodontal risk | Low | 43 (11.87%) | 22 (15.94%) |
| Medium | 204 (56.35%) | 66 (47.82%) | |
| High | 115 (31.76%) | 50 (36.23%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibraheem, W.I.; Bhati, A.K.; Alhomood, M.A.; Allayl, O.A.; Qsadi, A.A.; Mohammed, T.I.M.; Aljabri, Y.S. Relationship between Carotid Artery Calcification and Periodontitis in the Saudi Population: A Retrospective Study. Appl. Sci. 2023, 13, 12370. https://0-doi-org.brum.beds.ac.uk/10.3390/app132212370
Ibraheem WI, Bhati AK, Alhomood MA, Allayl OA, Qsadi AA, Mohammed TIM, Aljabri YS. Relationship between Carotid Artery Calcification and Periodontitis in the Saudi Population: A Retrospective Study. Applied Sciences. 2023; 13(22):12370. https://0-doi-org.brum.beds.ac.uk/10.3390/app132212370
Chicago/Turabian StyleIbraheem, Wael I., Ashok Kumar Bhati, Manar Ali Alhomood, Omaima Ahmed Allayl, Alzhouor Ali Qsadi, Tahani Ibrahim Mnaji Mohammed, and Yahya Sulaiman Aljabri. 2023. "Relationship between Carotid Artery Calcification and Periodontitis in the Saudi Population: A Retrospective Study" Applied Sciences 13, no. 22: 12370. https://0-doi-org.brum.beds.ac.uk/10.3390/app132212370