Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis

 ,
, 

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Quantitative Analysis
2.2. Qualitative Analysis
2.2.1. Stainless Steel Diamond Bur
2.2.2. Round Tungsten Carbide Bur
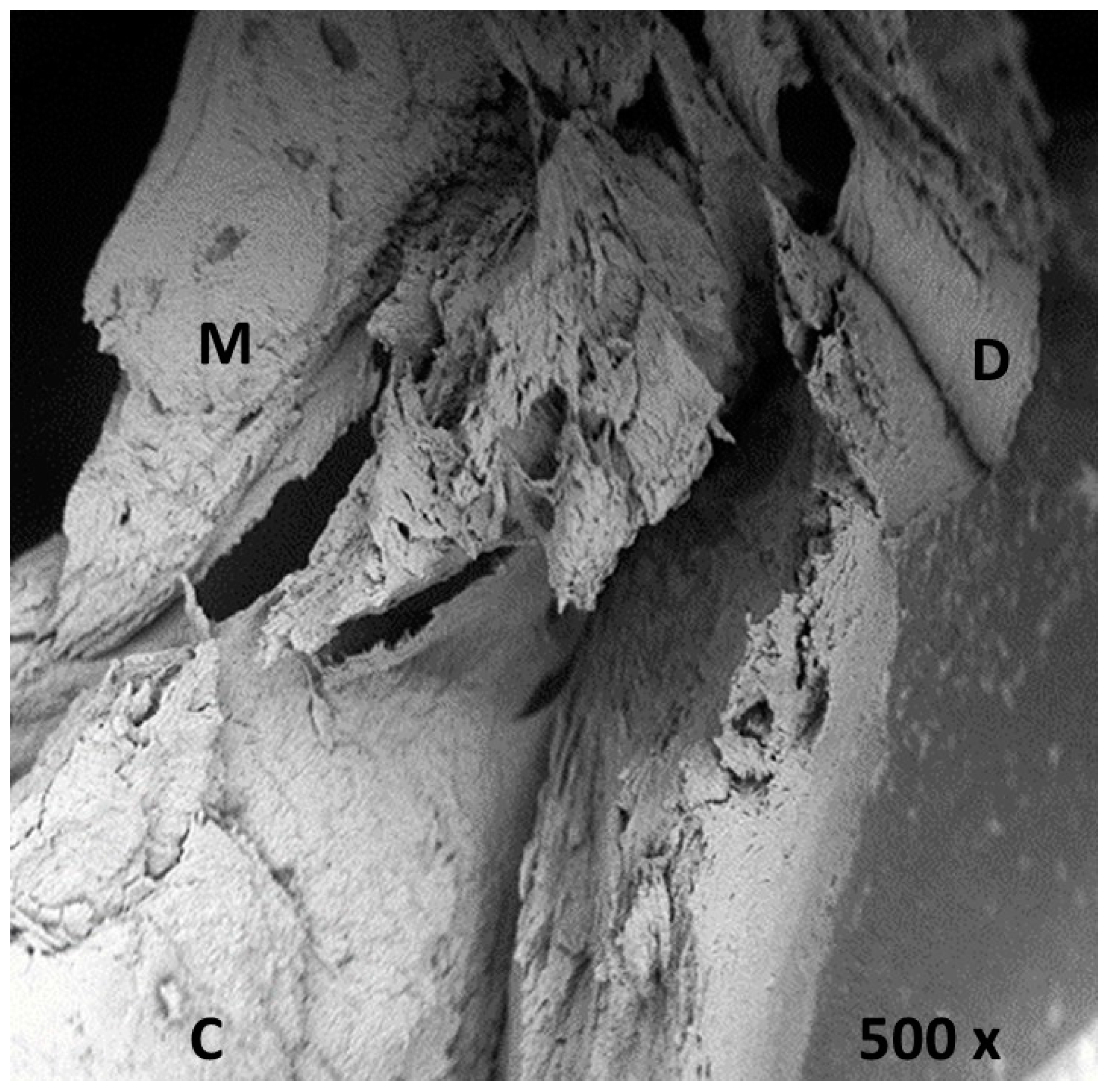
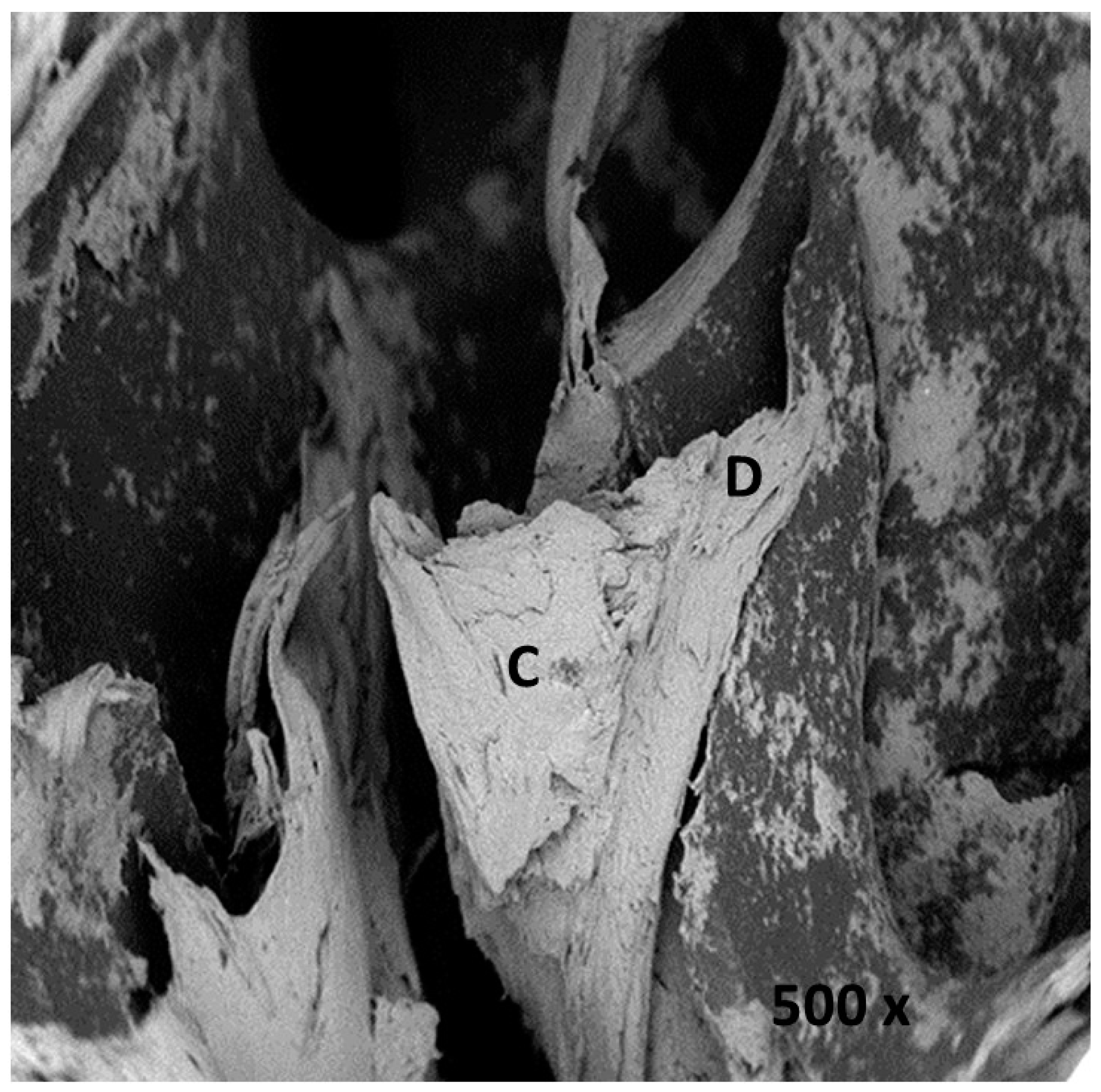
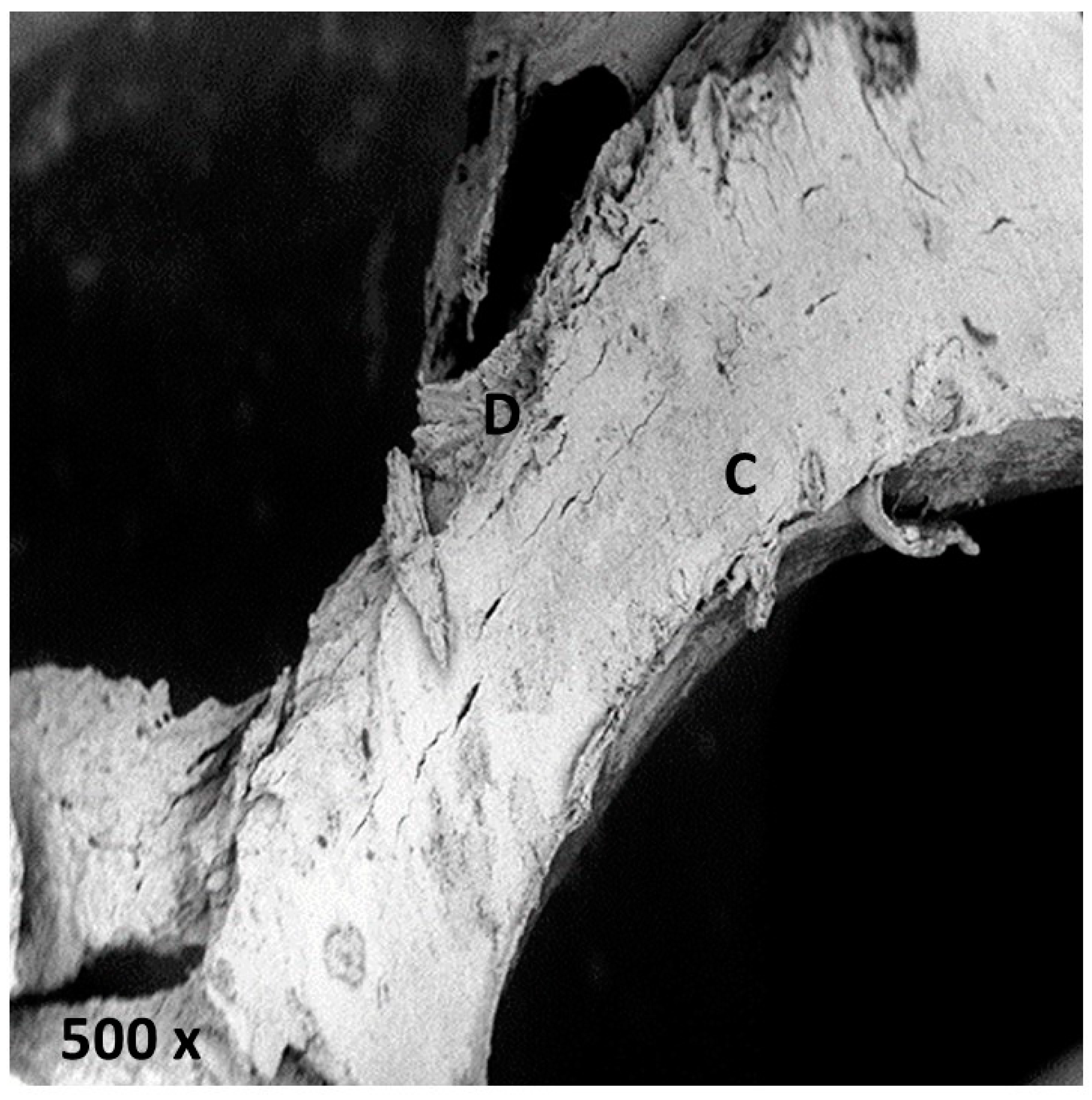
2.2.3. Stainless Steel Lindemann Type Bur
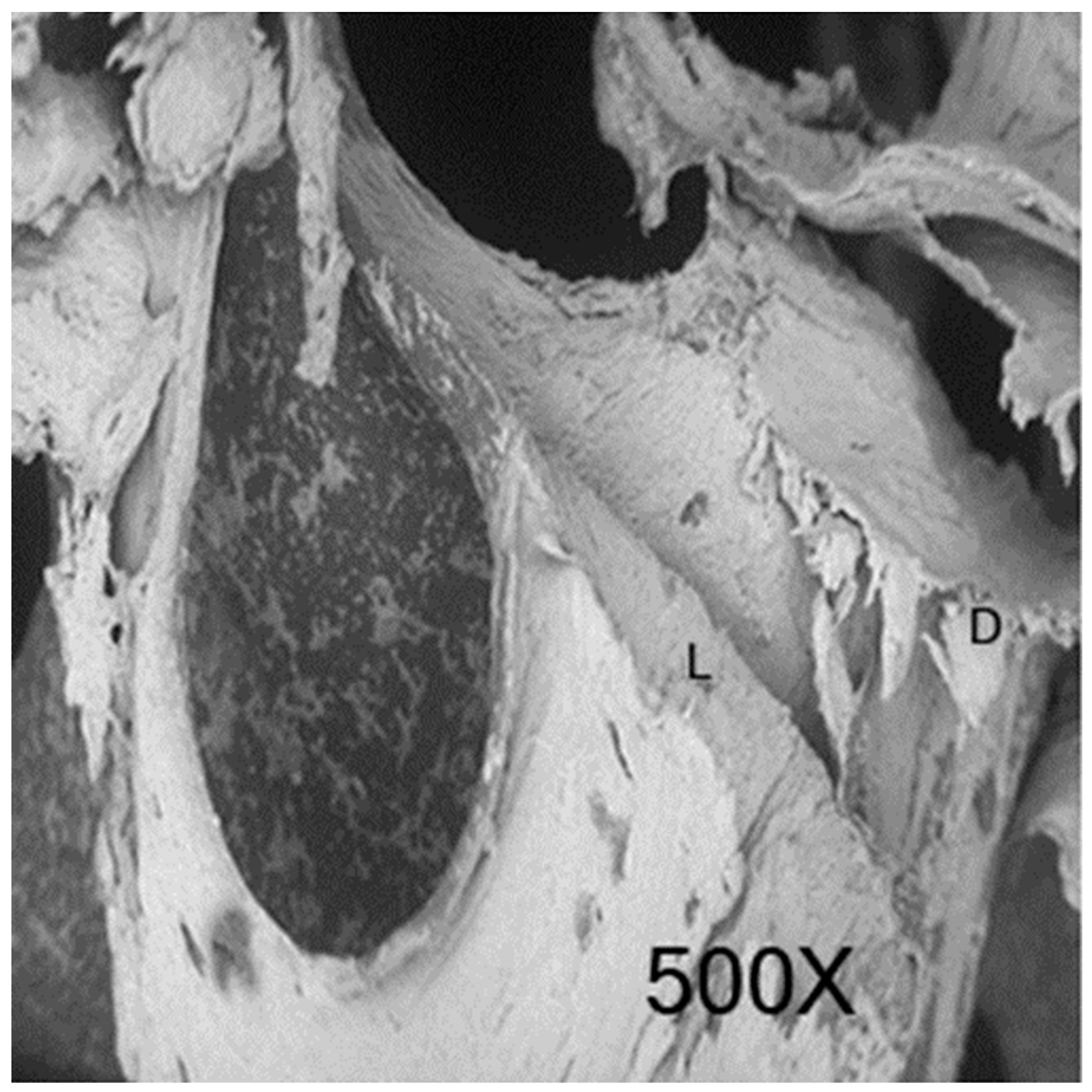
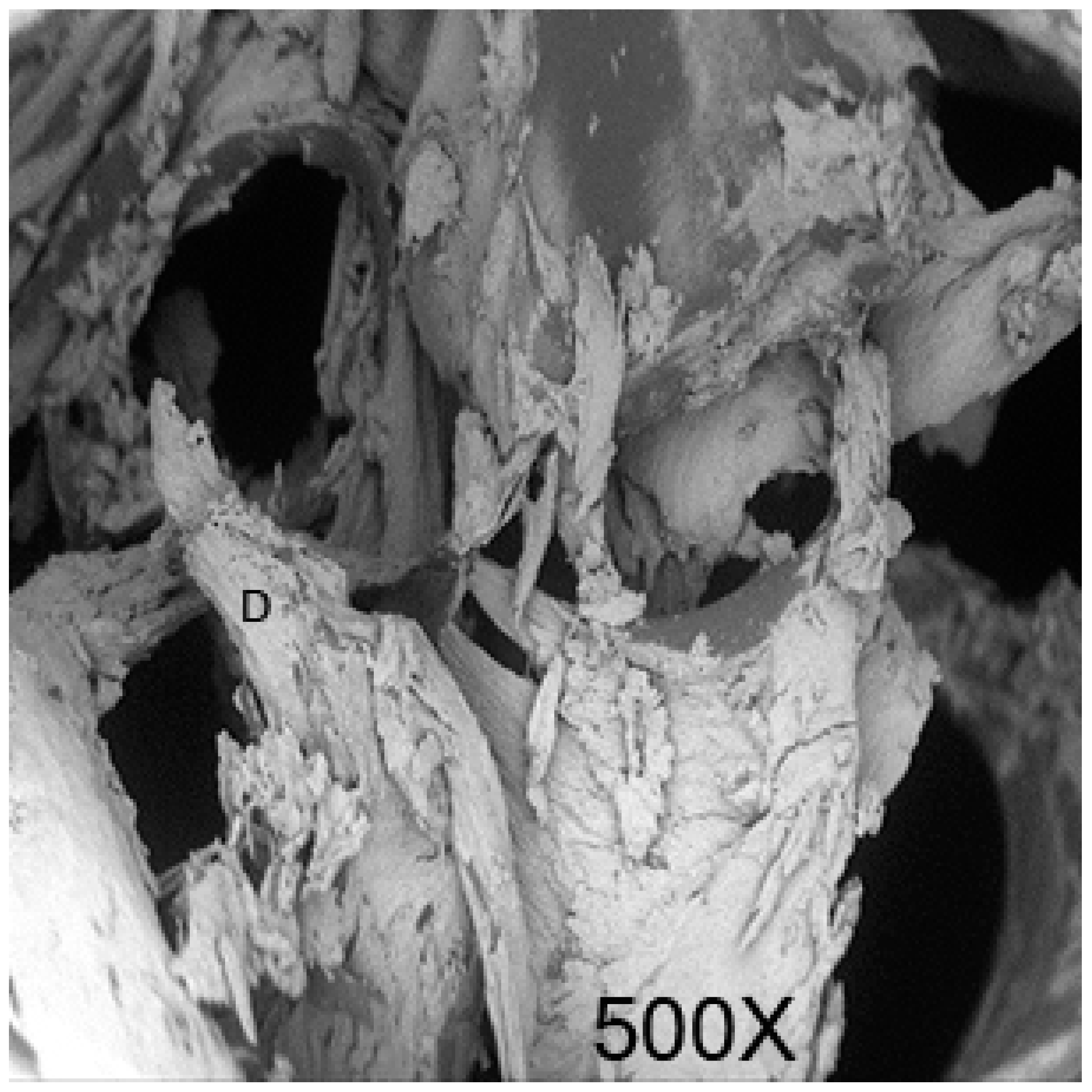
2.2.4. Piezosurgery OT12S Tip
2.2.5. Sonosurgery SFS 101
2.2.6. Control Sample
3. Discussion
4. Materials and Methods
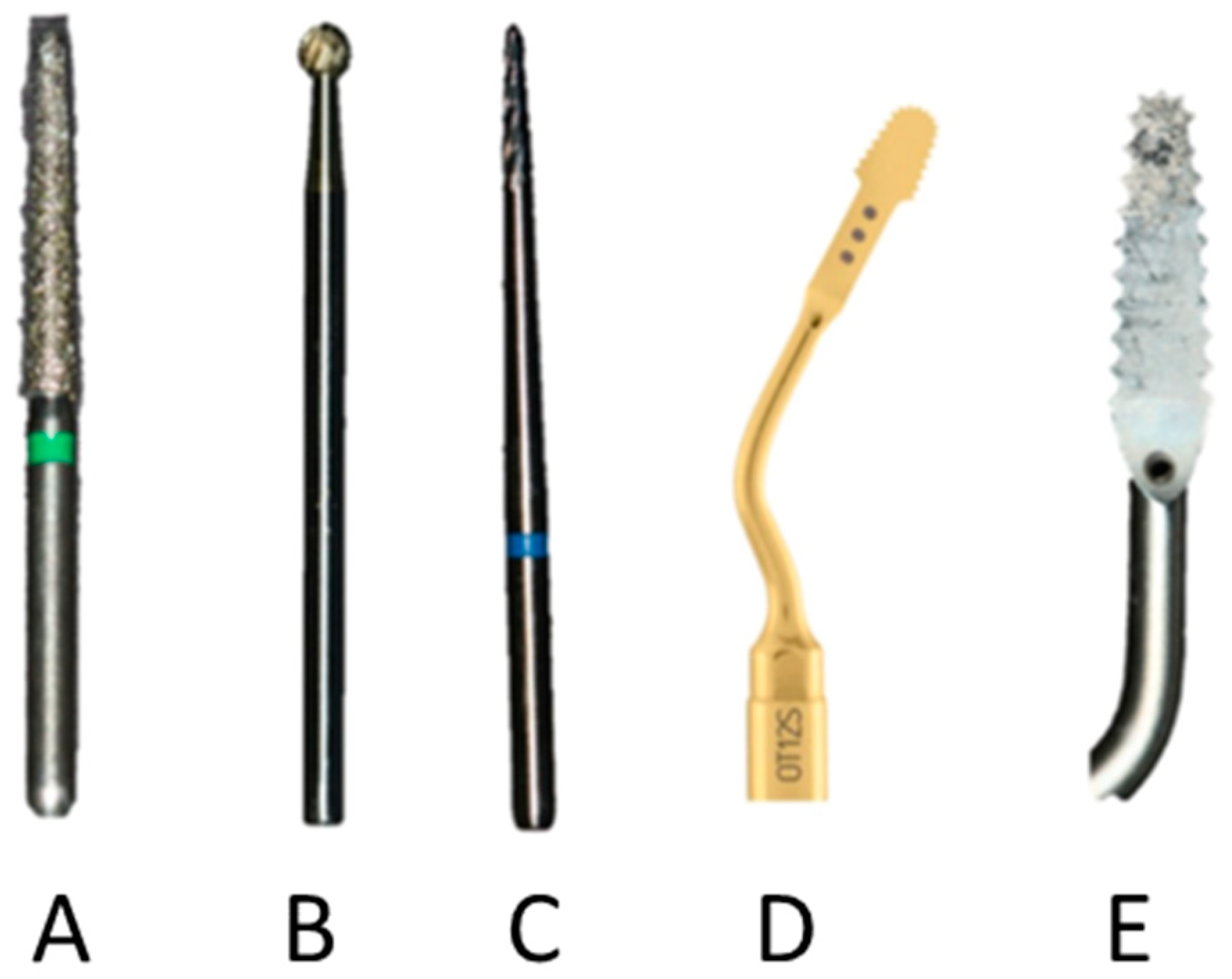
- Group A: One stainless steel diamond bur truncated conical shape (ISO diameter 016) Komet (Komet, Lemgo, Germany);
- Group B: One round tungsten carbide bur Komet (ISO diameter 018) (Komet, Lemgo, Germany);
- Group C: One stainless steel Lindemann type bur Komet (ISO diameter 016) (Komet, Lemgo, Germany)
- Group D: One Mectron OT12S tip mounted on a Piezosurgery Touch (Mectron, Vicenza, Italy);
- Group E: One Sonosurgery SFS 101 mounted on a Sonosurgery (Komet Dental, Lemgo, Germany).
- Minimal percentage variance between osteotomic track thickness and tip thickness;
- Osteotomized bone surface as smooth as possible;
- Microarchitecture integrity, limiting the presence of bone debris and avoiding thermal injuries to the bone; and
- Cutting time kept as short as possible.
- Cut precision (sharpness);
- Depth of incision (depth);
- Peripheral thermal damages (carbonization); and
- Presence of bone debris (bone fragments).
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Park, Y.; Choi, S.; Cho, K.; Lee, J. Dimensional alterations following vertical ridge augmentation using collagen membrane and three types of bone grafting materials: A retrospective observational study. Clin. Implant Dent. Relat. Res. 2017, 19, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Alayan, J.; Ivanovski, S.A. prospective controlled trial comparing xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus augmentation—Complications; patient-reported outcomes and volumetric analysis. Clin. Oral Implants Res. 2018, 29, 248–262. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.N.; Cammisa, F.P.; Sandhu, H.S.; Diwan, A.D.; Girardi, F.P.; Lane, J.M. The biology of bone grafting. J. Am. Acad. Orthop. Surg. 2005, 13, 77–86. [Google Scholar]
- Keskin, D.; Gündoǧdu, C.; Atac, A.C. Experimental comparison of bovine-derived xenograft; xenograft-autologous bone marrow and autogenous bone graft for the treatment of bony defects in the rabbit ulna. Med. Princ. Pract. 2007, 16, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Jones, E.; Mc Gonagle, D.; Giannoudis, P.V. Bone regeneration: Current concepts and future directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Felice, P.; Piana, L.; Checchi, L.; Corvino, V.; Nannmark, U.; Piattelli, M. Vertical ridge augmentation of an atrophic posterior mandible with an inlay technique and cancellous equine bone block: A case report. Int. J. Periodontics Restor. Dent. 2013, 33, 159–166. [Google Scholar] [CrossRef]
- Pistilli, R.; Signorini, L.; Pisacane, A.; Lizio, G.; Felice, P. Case of severe bone atrophy of the posterior maxilla rehabilitated with blocks of equine origin bone: Histological results. Implant Dent. 2013, 22, 8–15. [Google Scholar] [CrossRef]
- De Angelis, N.; Scivetti, M. Lateral ridge augmentation using an equine flex bone block infused with recombinant human platelet-derived growth factor BB: A clinical and histologic study. J. Periodontics Restor. Dent. 2011, 31, 383–388. [Google Scholar]
- Ludovichetti, M.; Di Stefano, D.A.; Pagnutti, S.; Vaccari, E.; Ludovichetti, F.S.; Celletti, R. Vertical ridge augmentation using a flexible heterologous cortical bone sheet: Threeyear follow-up. J. Periodontics Restor. Dent. 2011, 31, 401–407. [Google Scholar]
- Di Stefano, D.A.; Artese, L.; Iezzi, G.; Piattelli, A.; Pagnutti, S.; Piccirilli, M.; Perrotti, V. Alveolar ridge regeneration with equine spongy bone: A clinical; histological; and immunohistochemical case series. Clin. Implant Dent. Relat. Res. 2009, 11, 90–100. [Google Scholar] [CrossRef]
- Cortese, A.; Pantaleo, G.; Borri, A.; Caggiano, M.; Amato, M. Platelet-rich fibrin (PRF) in implant dentistry in combination with new bone regenerative technique in elderly patients. Int. J. Surg. Case Rep. 2016, 28, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Artese, L.; Piattelli, A.; Di Stefano, D.A.; Piccirilli, M.; Pagnutti, S.; D’Alimonte, E.; Perrotti, V. Sinus lift with autologous bone alone or in addition to equine bone: An immunohistochemical study in man. Implant Dent. 2011, 20, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Vinci, R.; Zizzari, V.L.; Zara, S.; La Scala, V.; Cataldi, A.; Gherlone, E.; Piattelli, A. Maxillary sinus augmentation procedures through equine-derived biomaterial or calvaria autologous bone: Immunohistochemical evaluation of OPG/RANKL in humans. Eur. J. Histochem. 2013, 57, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Zizzari, V.L.; Vinci, R.; Zara, S.; Di Tore, U.; Manica, M.; Cataldi, A.; Mortellaro, C.; Piattelli, A.; Gherlone, E. Equine and porcine bone substitutes in maxillary sinus augmentation: A histological and immunohistochemical analysis of VEGF expression. J. Craniofac. Surg. 2014, 25, 835–839. [Google Scholar] [CrossRef]
- Qing, L.L.; Zhao, H.; Liu, L.L. Progress on low suscepti bility mechanisms of transmissible spongiform encephalopathies. Dongwuxue Yanjiu 2014, 35, 436–445. [Google Scholar] [CrossRef]
- Zhang, J. The structural stability of wild-type horse prion protein. J. Biomol. Struct. Dyn. 2011, 29, 369–377. [Google Scholar] [CrossRef]
- Pacaccio, D.J.; Stern, S.F. Demineralized bone matrix: Basic science and clinical applications. Clin. Podiatr. Med. Surg. 2005, 22, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Chesmel, K.D.; Branger, J.; Wertheim, H.; Scarborough, N. Healing response to various forms of human demineralized bone matrix in athymic rat cranial defects. J. Oral Maxillofac. Surg. 1998, 56, 857–865. [Google Scholar] [CrossRef]
- Guizzardi, S.; Di Silvestre, M.; Scandroglio, R.; Ruggeri, A.; Savini, R. Implants of heterologous demineralized bone matrix for induction of posterior spinal fusion in rats. Spine 1992, 17, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Valente, N.A.; Mang, T.; Hatton, M.; Mikulski, L.; Andreana, S. Effects of Two Diode Lasers with and Without Photosensitization on Contaminated Implant Surfaces: An Ex Vivo Study. Photomed. Laser Surg. 2017, 35, 347–356. [Google Scholar] [CrossRef]
- Lew, D.; Marino, A.A.; Startzell, J.M.; Keller, J.C. A comparative study of osseointegration of titanium implants in corticocancellous block and corticocancellous chip grafts in canine ilium. J. Oral Maxillofac. Surg. 1994, 52, 952–958. [Google Scholar] [CrossRef]
- Schlee, M.; Rothamel, D. Ridge augmentation using customized allogenic bone blocks: Proof of concept and histological findings. Implant Dent. 2013, 22, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Thoma, D.S.; Jung, R.E.; Sanz-Martin, I.; Unger, S.; Cantalapiedra, A.; Hämmerle, C.H.F. Guided bone regeneration with particulate vs. block xenogenic bone substitutes: A pilot cone beam computed tomographic investigation. Clin. Oral Implants Res. 2017, 28, e262–e270. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, G.; Iannello, G.; Terranova, A.; Lo Giudice, R.; Pantaleo, G.; Cicciù, M. Transcrestal sinus lift procedure approaching atrophic maxillary ridge: A 60-month clinical and radiological follow-up evaluation. Int. J. Dent. 2015, 2015, 261652. [Google Scholar] [CrossRef] [PubMed]
- De Ponte, F.S.; Cutroneo, G.; Falzea, R.; Rizzo, G.; Catalfamo, L.; Favaloro, A.; Vermiglio, G.; Runci, M.; Centofanti, A.; Anastasi, G. Histochemical and morphological aspects of fresh frozen bone: A preliminary study. Eur. J. Histochem. 2016, 60, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Cortese, A.; Pantaleo, G.; Amato, M.; Claudio, P.P. Ridge expansion by flapless split crest and immediate implant placement: Evolution of the technique. J. Craniofac. Surg. 2016, 27, e123–e128. [Google Scholar] [CrossRef]
- Bruno, V.; Berti, C.; Barausse, C.; Badino, M.; Gasparro, R.; Ippolito, D.R.; Felice, P. Clinical Relevance of Bone Density Values from CT Related to Dental Implant Stability: A Retrospective Study. BioMed Res. Int. 2018, 2018, 6758245. [Google Scholar] [CrossRef]
- Schwartz-Arad, D.; Levin, L. Intraoral autogenous block onlay bone grafting for extensive reconstruction of atrophic maxillary alveolar ridges. J. Periodontol. 2005, 76, 636–641. [Google Scholar] [CrossRef]
- Strietzel, F.P.; Khongkhunthian, P.; Khattiya, R.; Patchanee, P.; Reichart, P.A. Healing pattern of bone defects covered by different membrane types—A histologic study in the porcine mandible. J. Biomed. Mater. Res. Part B Appl. Biomater. 2006, 78, 35–46. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Ferrari, D.; Wieland, M.; Schmitz, L.; Engelhardt, E.; Becker, J. Guided bone regeneration at dehiscence-type defects using biphasic hydroxyapatite + beta tricalcium phosphate (Bone Ceramic®) or a collagen-coated natural bone mineral (BioOss Collagen®): An immunohistochemical study in dogs. Int. J. Oral Maxillofac. Surg. 2007, 36, 1198–1206. [Google Scholar] [CrossRef]
- Waasdo, J.; Reynolds, M.A. Allogeneic bone onlay grafts for alveolar ridge augmentation: A systematic review. Int. J. Oral Maxillofac. Implants 2010, 25, 525–531. [Google Scholar]
- Rullo, R.; Festa, V.M.; Rullo, F.; Trosino, O.; Cerone, V.; Gasparro, R.; Laino, L.; Sammartino, G. The use of piezosurgery in genioplasty. J. Craniofac. Surg. 2016, 27, 414–415. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Marconcini, S.; Giacomelli, L.; Rispoli, L.; Calvo, J.L.; Covani, U. A randomized clinical evaluation of ultrasound bone surgery versus traditional. J. Oral Maxillofac. Surg. 2010, 68, 330–336. [Google Scholar] [CrossRef]
- Ferri, M.; Lang, N.P.; Angarita Alfonso, E.E.; Bedoya Quintero, I.D.; Burgos, E.M.; Botticelli, D. Use of sonic instruments for implant biopsy retrieval. Clin. Oral Implants Res. 2015, 26, 1237–1243. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Nigrone, V.; Longo, A.; Cicciù, M. Supernumerary and supplemental teeth: Case report. Eur. J. Paediatr. Dent. 2008, 9, 97–101. [Google Scholar] [PubMed]
- Rundle, C.H.; Wang, H.; Yu, H.; Chadwick, R.B.; Davis, E.I.; Wergedal, J.E.; Lau, K.H.; Mohan, S.; Ryaby, J.T.; Baylink, D.J. Microarray analysis of gene expression during the inflammation and endochondral bone formation stages of rat femur fracture repair. Bone 2006, 38, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.A.; Gugliandolo, P.; Favaloro, A.; Vermiglio, G.; Centofanti, A.; Bruschetta, D.; Rizzo, G. Morpho-structural alterations of sub-chondral bone tissue in patients with osteoarthritis: A scanning electron microscopy study. Ital. J. Anat. Embryol. 2015, 120, 71–81. [Google Scholar] [PubMed]
- Anastasi, G.; Cutroneo, G.; Rizzo, G.; Favaloro, A. Sarcoglycan subcomplex in normal and pathological human muscle fibers. Eur. J. Histochem. 2007, 51 (Suppl. 1), 29–33. [Google Scholar] [PubMed]
- Romeo, U.; del Vecchio, A.; Palaia, G.; Tenore, G.; Visca, P.; Maggiore, C. Bone damage induced by different cutting instruments—An in vitro study. Braz. Dent. J. 2009, 20, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Di Mauro, D.; Gaeta, R.; Arco, A.; Milardi, D.; Lentini, S.; Runci, M.; Rizzo, G.; Magaudda, L. Distribution of costameric proteins in normal human ventricular and atrial cardiac muscle. Folia Histochem. Cytobiol. 2009, 47, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Stefan, U.; Michael, B.; Werner, S. Effects of three different preservation methods on the mechanical properties of human and bovine cortical bone. Bone 2010, 47, 1048–1053. [Google Scholar] [CrossRef]
- Bitar, D.; Parvizi, J. Biological response to prosthetic debris. World J. Orthop. 2015, 6, 172–189. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, M.; Facco, G.; Barberis, F.; Signorini, G.; Capurro, M.; Rebaudi, A.; Sammartino, G. Bone characteristics following osteotomy surgery: An in vitro SEM study comparing traditional Lindemann drill with sonic and ultrasonic instruments. POSEIDO 2013, 1, 187–194. [Google Scholar]
- Moest, T.; Wehrhan, F.; Lutz, R.; Schmitt, C.M.; Neukam, F.W.; Schlegel, K.A. Extra-oral defect augmentation using autologous; bovine and equine bone blocks: A preclinical histomorphometrical comparative study. J. Cranio-Maxillofac. Surg. 2015, 43, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Pantaleo, G.; Lo Giudice, R.; Sammartino, G.; Ilardi, G.; Russo, D. Hybrid Tumor with Presence of Liesengang Rings: Histology; Surgery; and Clinical Management. J. Craniofac. Surg. 2017, 28, 580–581. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Cicciù, M.; Eftimie, L.F.; Miller, M.; Signorino, F.; Famà, F.; Cervino, G.; Lo Giudice, G.; Bramanti, E.; Lauritano, F.; et al. rhBMP-2 applied as support of distraction osteogenesis: A split-mouth histological study over nonhuman primates mandibles. Int. J. Clin. Exp. Med. 2016, 9, 17187–17194. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Burs/Tips | Groups | Observational Parameters | |||
|---|---|---|---|---|---|
| Sharpness (0–3) | Depth (0–3) | Carbonization (0–3) | Bone Debris (0–3) | ||
| Stainless steel diamond | A | 1.38 ± 0.8 | 0.79 ± 0.4 | 0.33 ± 0.4 | 1.79 ± 0.8 |
| Round tungsten carbide | B | 0.10 ± 0.3 | 2.50 ± 0.8 | 1.40 ± 0.5 | 3.00 ± 0 |
| Lindemann stainless steel | C | 0.84 ± 0.5 | 1.96 ± 0.4 | 0.62 ± 0.6 | 2.15 ± 0.5 |
| Piezoelectric OT12S | D | 1.63 ± 0.6 | 1.00 ± 0.9 | 0.38 ± 0.5 | 1.31 ± 0.6 |
| Sonic SFS 101 | E | 1.38 ± 0.5 | 1.50 ± 0.5 | 1.00 ± 0.6 | 1.56 ± 0.5 |
| Control | F | 0.58 ± 0.8 | 0.58 ± 0.5 | 0.17 ± 0.4 | 0.75 ± 0.4 |
| Device | Frequency (kHz) | Insert Tip | Thickness (mm) | Oscillation Amplitude (mm) |
|---|---|---|---|---|
| Piezosurgery Touch | 24 < x < 36 | OT12S | 0.25 | 20 < x < 60 |
| Sonosurgery | 5 < x < 6.5 | SFS101 | 0.25 | 240 |
| Observational Parameters | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Sharpness | Impossible to identify anatomical structure | Low preservation of anatomical structure | Moderate preservation of anatomical structure | High preservation of anatomical structure |
| Depth | Very low incision depth | Low incision depth | Moderate incision depth | High incision depth |
| Carbonization | Absence of carbonization | Low presence of carbonization areas | Moderate presence of carbonization areas | High presence of carbonization areas |
| Bone Fragments | Absence of bone fragments | Low presence of bone fragments | Moderate presence of fragments | High presence of bone fragments |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Giudice, R.; Puleio, F.; Rizzo, D.; Alibrandi, A.; Lo Giudice, G.; Centofanti, A.; Fiorillo, L.; Di Mauro, D.; Nicita, F. Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis. Appl. Sci. 2019, 9, 351. https://0-doi-org.brum.beds.ac.uk/10.3390/app9020351
Lo Giudice R, Puleio F, Rizzo D, Alibrandi A, Lo Giudice G, Centofanti A, Fiorillo L, Di Mauro D, Nicita F. Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis. Applied Sciences. 2019; 9(2):351. https://0-doi-org.brum.beds.ac.uk/10.3390/app9020351
Chicago/Turabian StyleLo Giudice, Roberto, Francesco Puleio, David Rizzo, Angela Alibrandi, Giorgio Lo Giudice, Antonio Centofanti, Luca Fiorillo, Debora Di Mauro, and Fabiana Nicita. 2019. "Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis" Applied Sciences 9, no. 2: 351. https://0-doi-org.brum.beds.ac.uk/10.3390/app9020351