Scanning Electron Microscopy Analysis and Energy Dispersion X-ray Microanalysis to Evaluate the Effects of Decontamination Chemicals and Heat Sterilization on Implant Surgical Drills: Zirconia vs. Steel

 , ,
, , 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
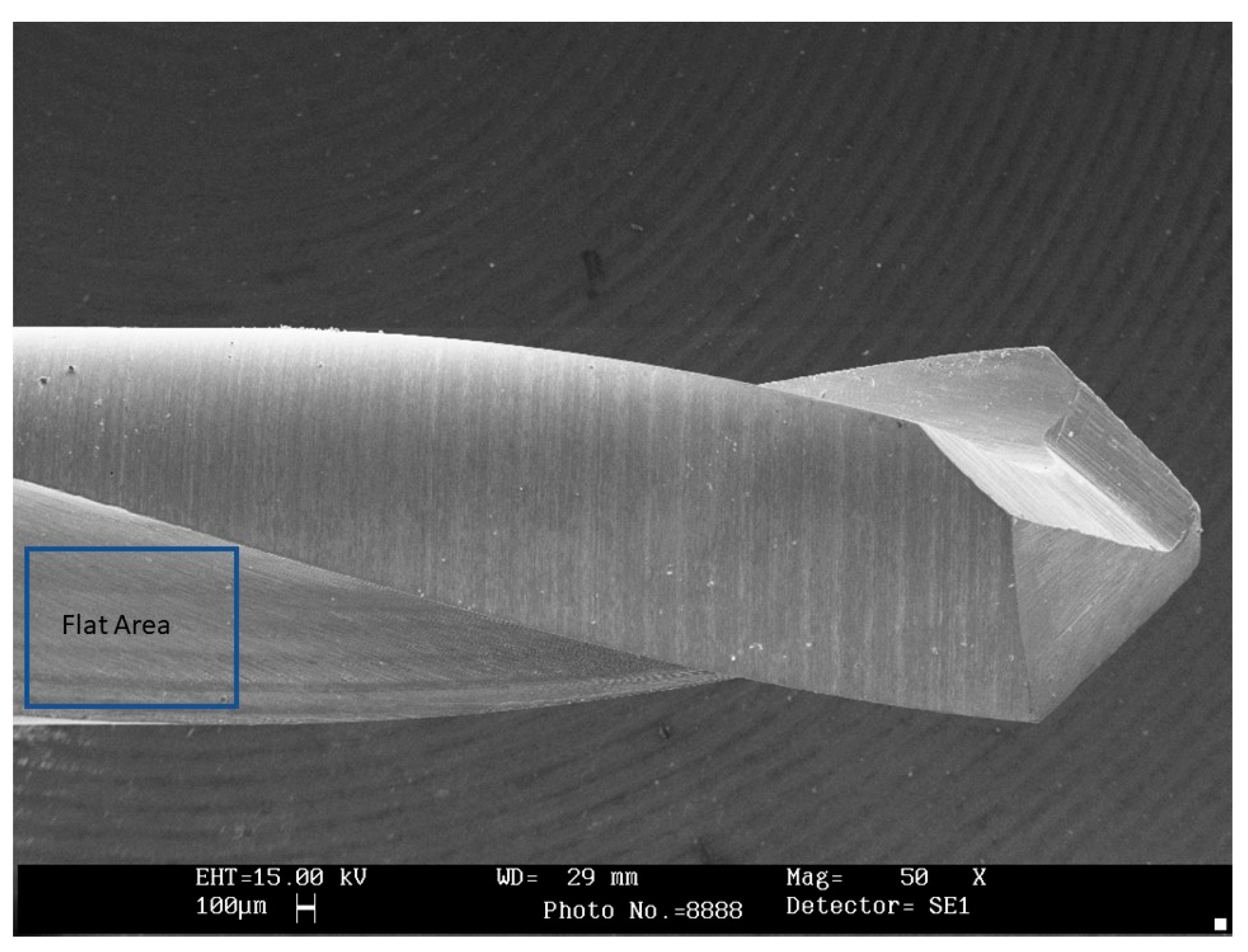
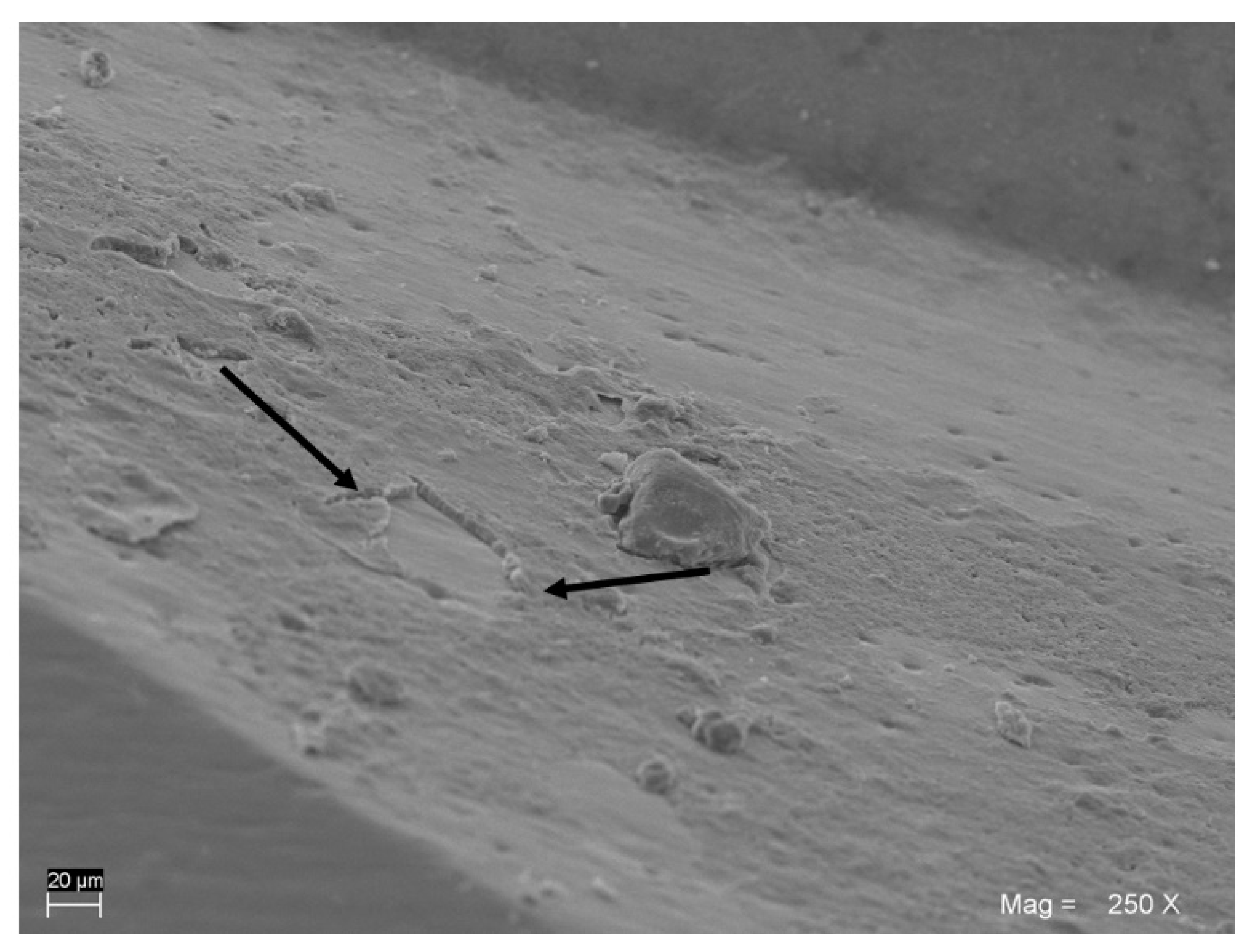
2.1. SEM Observations
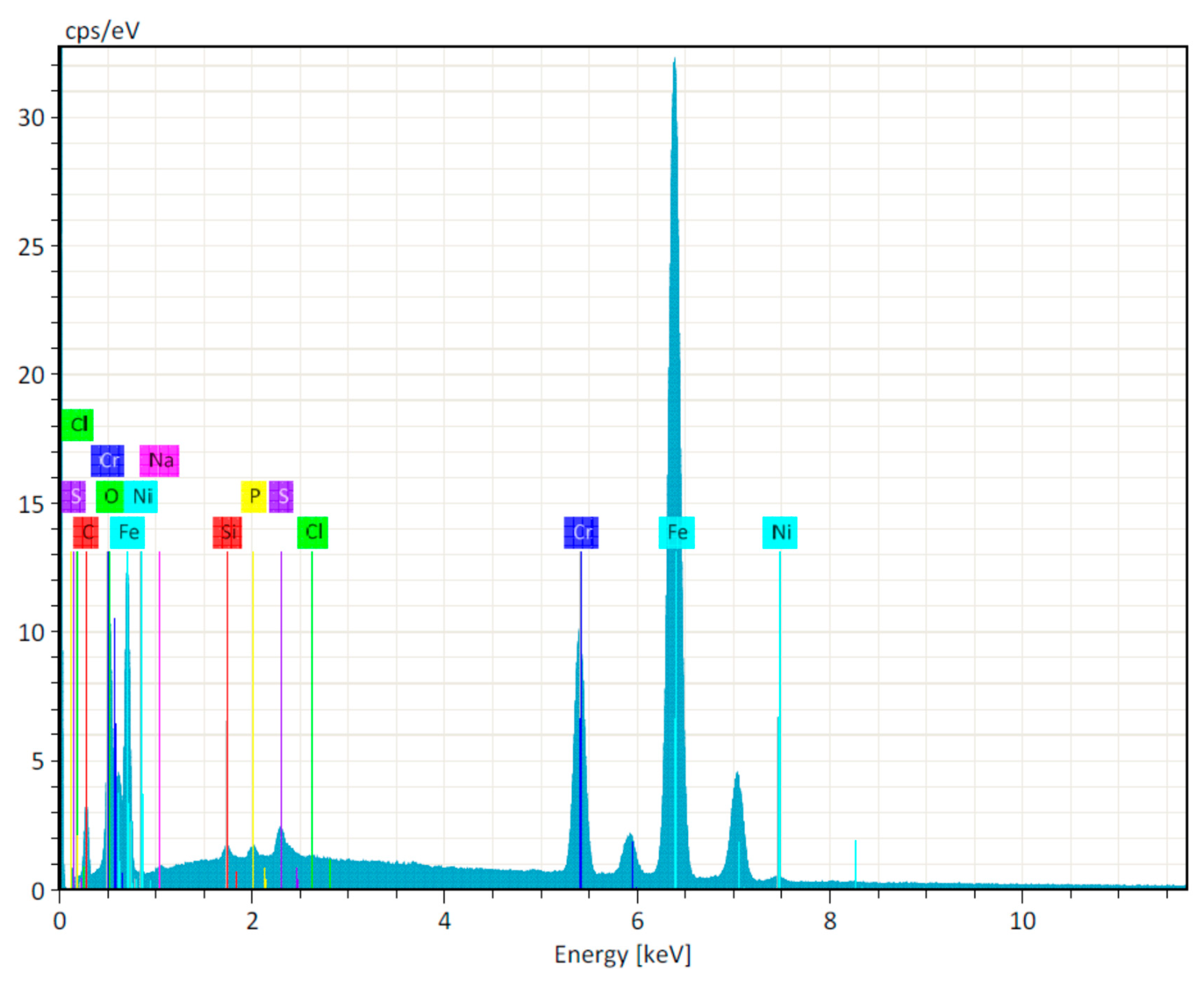
2.2. Energy Dispersive X-ray Spectroscopy (EDX)
2.3. Statistical Evaluation
3. Results
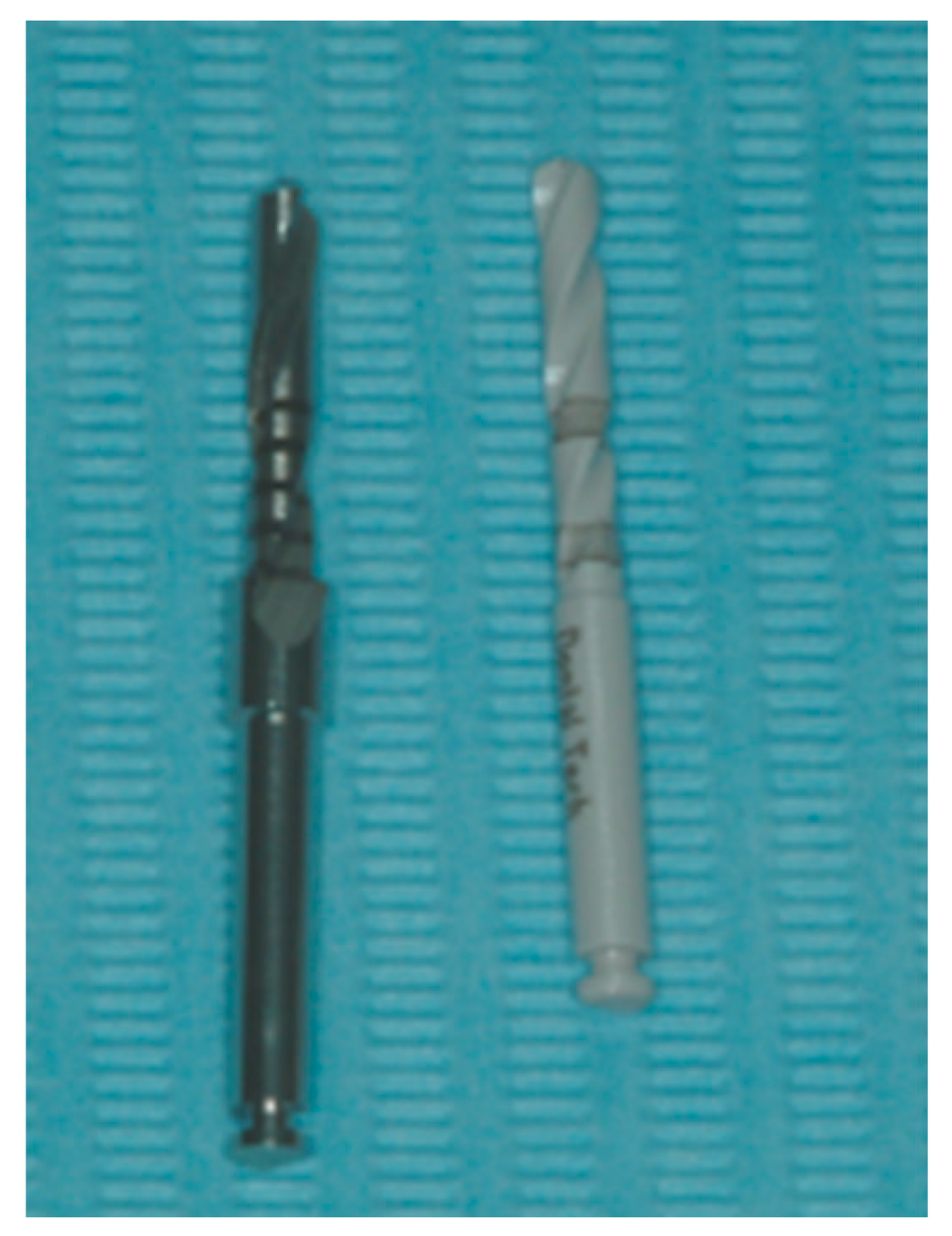
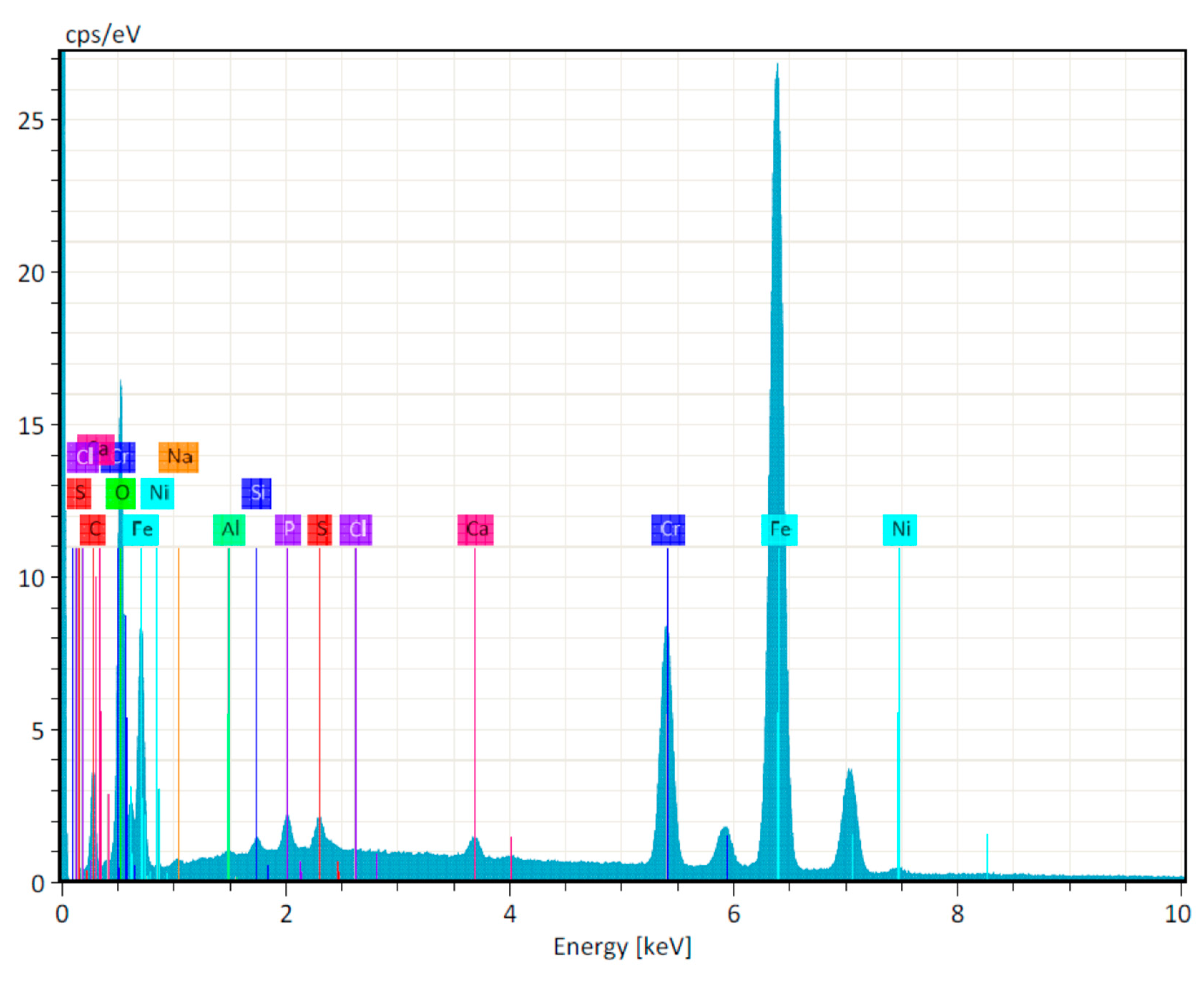
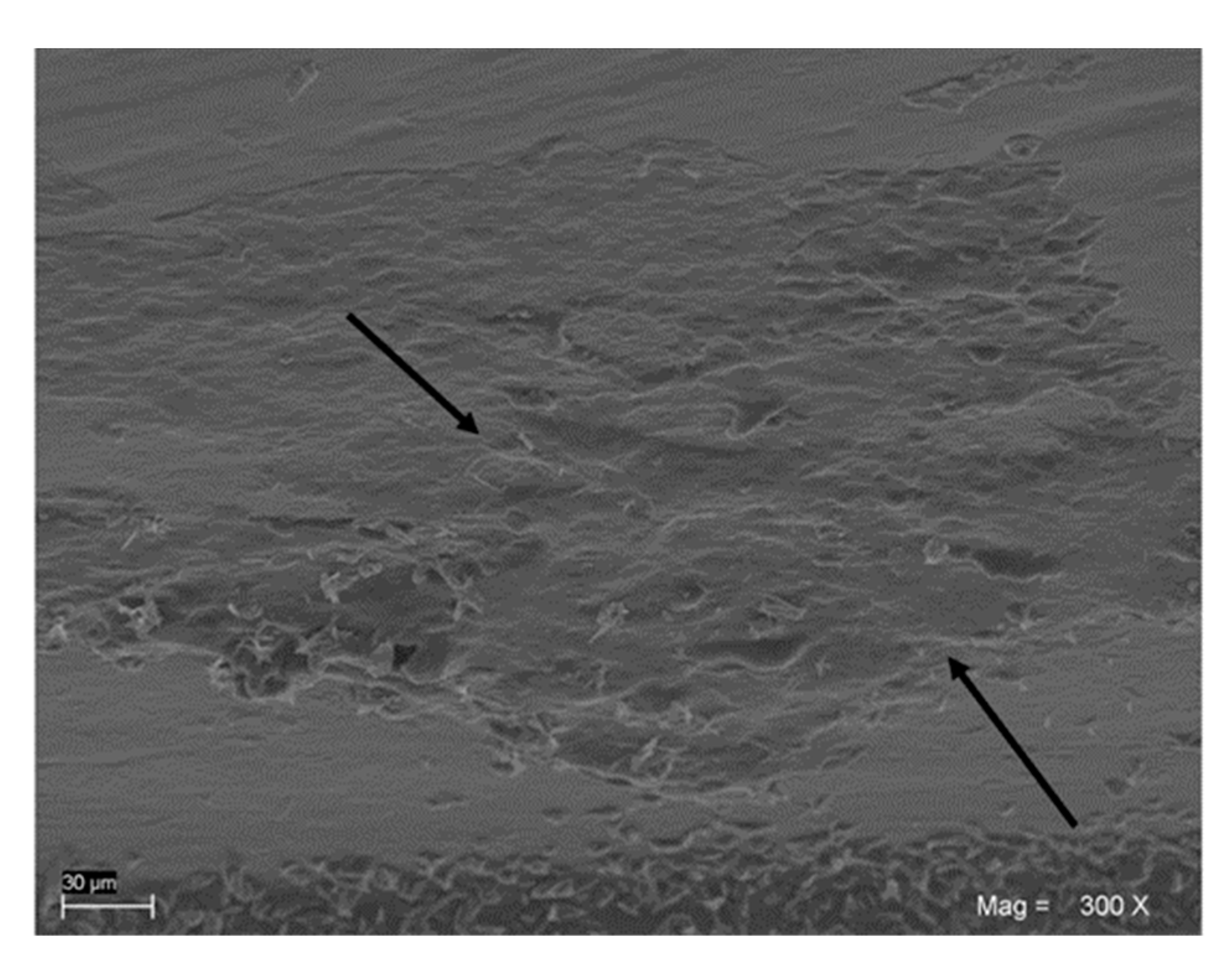
3.1. Steel Drills
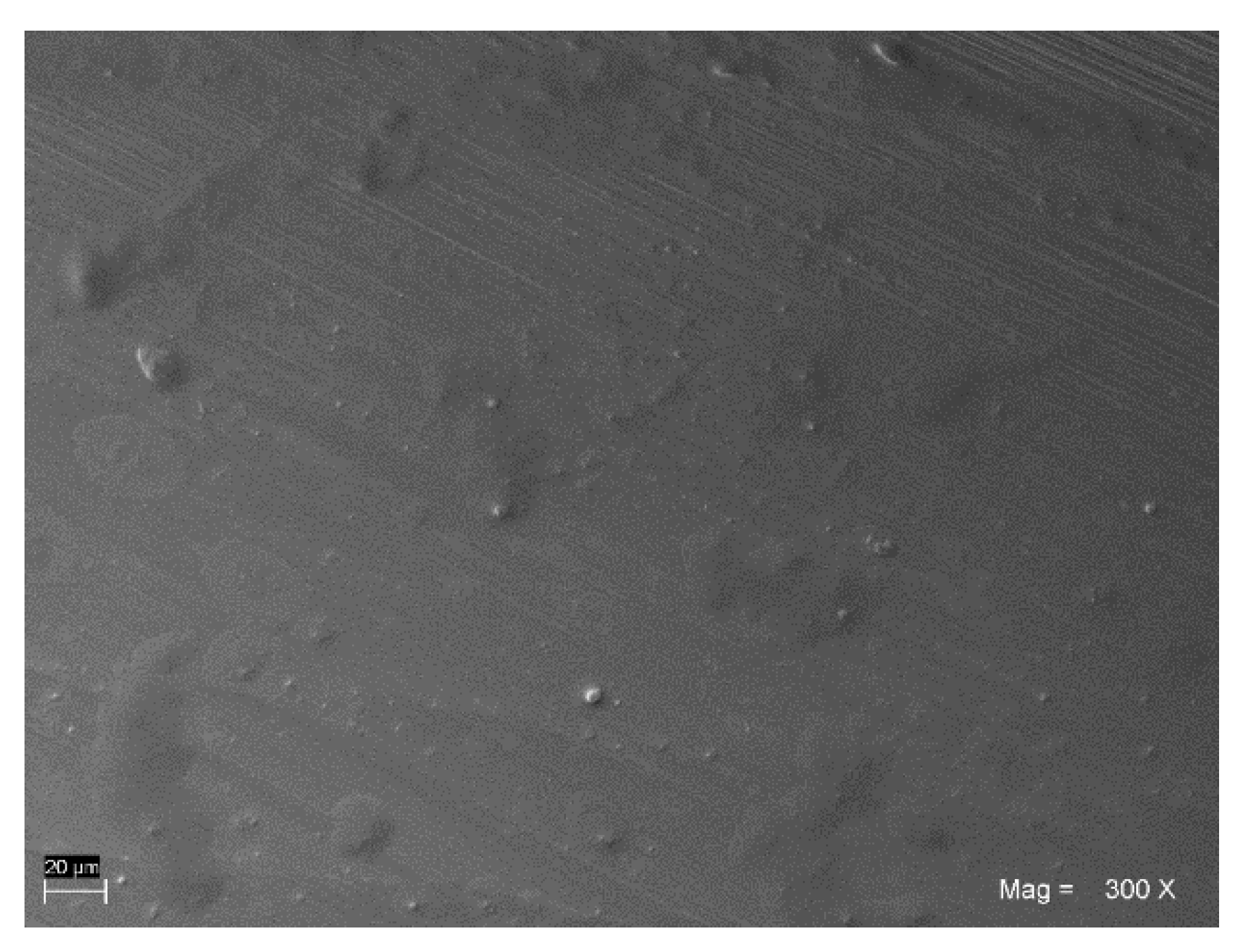
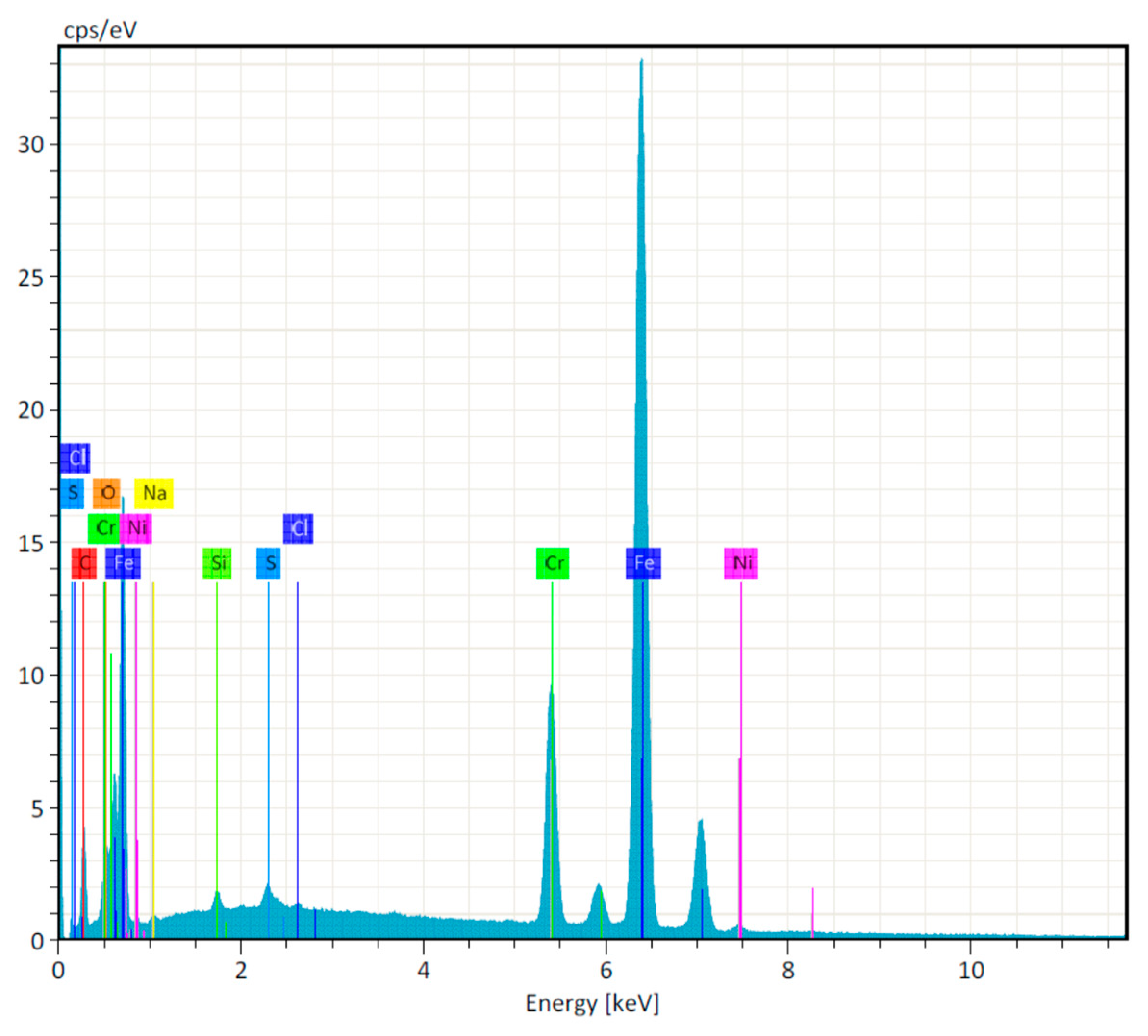
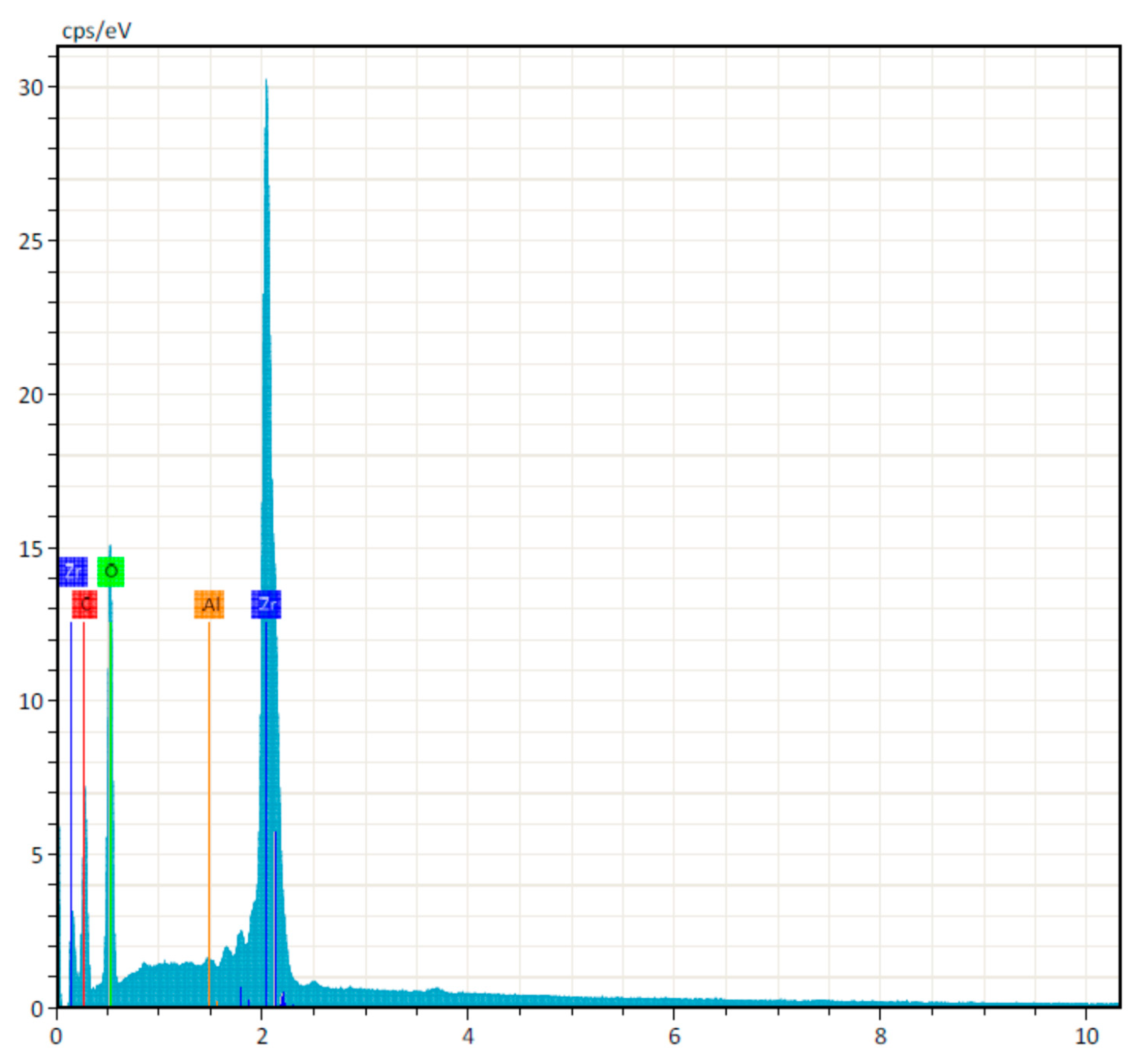
3.2. Zirconia Drills
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scarano, A.; Piattelli, A.; Quaranta, A.; Lorusso, F. Bone Response to Two Dental Implants with Different Sandblasted/Acid-Etched Implant Surfaces: A Histological and Histomorphometrical Study in Rabbits. BioMed Res. Int. 2017, 2017, 8724951. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef]
- Scarano, A.; Carinci, F.; Lorusso, F.; Festa, F.; Bevilacqua, L.; Santos de Oliveira, P.; Maglione, M. Ultrasonic vs Drill Implant Site Preparation: Post-Operative Pain Measurement through VAS, Swelling and Crestal Bone Remodeling: A Randomized Clinical Study. Materials 2018, 11, 2516. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, R.; Adell, R. Temperatures during drilling for the placement of implants using the osseointegration technique. J. Oral Maxillofac. Surg. 1986, 44, 4–7. [Google Scholar] [CrossRef]
- Scarano, A.; Di Carlo, F.; Piattelli, A. Effect of sterilization and cleansing on implantology drills: Zirconia vs steel. Ital. Oral Surg. 2008, 3, 61–72. [Google Scholar]
- Hochscheidt, C.J.; Shimizu, R.H.; Andrighetto, A.R.; Pierezan, R.; Thomé, G.; Salatti, R. Comparative Analysis of Cutting Efficiency and Surface Maintenance between Different Types of Implant Drills: An In Vitro Study. Implant Dent. 2017, 26, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Hein, C.; Inceoglu, S.; Juma, D.; Zuckerman, L. Heat Generation during Bone Drilling: A Comparison between Industrial and Orthopaedic Drill Bits. J. Orthop. Trauma 2017, 31, e55–e59. [Google Scholar] [CrossRef] [PubMed]
- Louropoulou, A.; Slot, D.E.; Van der Weijden, F.A. Titanium surface alterations following the use of different mechanical instruments: A systematic review. Clin. Oral Implant. Res. 2012, 23, 643–658. [Google Scholar] [CrossRef]
- Noumbissi, S.; Scarano, A.; Gupta, S. A Literature Review Study on Atomic Ions Dissolution of Titanium and Its Alloys in Implant Dentistry. Materials 2019, 12, 368. [Google Scholar] [CrossRef]
- Dubruille, J.H.; Viguier, E.; Le Naour, G.; Dubruille, M.T.; Auriol, M.; Le Charpentier, Y. Evaluation of combinations of titanium, zirconia, and alumina implants with 2 bone fillers in the dog. Int. J. Oral Maxillofac. Implant. 1999, 14, 271–277. [Google Scholar]
- Scarano, A.; Di Carlo, F.; Quaranta, M.; Piattelli, A. Bone Response to Zirconia Ceramic Implants: An Experimental Study in Rabbits. J. Oral Implant. 2003, 29, 8–12. [Google Scholar] [CrossRef]
- Jackson, M.C. Restoration of posterior implants using a new ceramic material. J. Dent. Technol. 1999, 16, 19–22. [Google Scholar] [PubMed]
- Spinelli, M.; Maccauro, G.; Graci, C.; Cittadini, A.; Magnani, G.; Sangiorgi, S.; Del Bravo, V.; Manicone, P.; Raffaelli, L.; Muratori, F.; et al. Zirconia Toughened Alumina (ZTA) Powders: Ultrastructural and Histological Analysis. Int. J. Immunopathol. Pharmacol. 2011, 24, 153–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.; Niu, B.; Yi, J.; Deng, Z.; Song, J.; Chen, Q. Toxicity and Metal Corrosion of Glutaraldehyde-Didecyldimethylammonium Bromide as a Disinfectant Agent. BioMed Res. Int. 2018, 2018, 9814209. [Google Scholar] [CrossRef] [PubMed]
- Urayama, S.; Kozarek, R.A.; Sumida, S.; Raltz, S.; Merriam, L.; Pethigal, P. Mycobacteria and glutaraldehyde: Is high-level disinfection of endoscopes possible? Gastrointest. Endosc. 1996, 43, 451–456. [Google Scholar] [CrossRef]
- Chenjiao, W.; HongYan, Z.; Qing, G.; Xiaoqi, Z.; Liying, G.; Ying, F. In-Use Evaluation of Peracetic Acid for High-Level Disinfection of Endoscopes. Gastroenterol. Nurs. 2016, 39, 116–120. [Google Scholar] [PubMed]
- Omidbakhsh, N.; Sattar, S.A. Broad-spectrum microbicidal activity, toxicologic assessment, and materials compatibility of a new generation of accelerated hydrogen peroxide-based environmental surface disinfectant. Am. J. Infect. Control 2006, 34, 251–257. [Google Scholar] [CrossRef]
- Scarano, A.; Carinci, F.; Quaranta, A.; Di Iorio, D.; Assenza, B.; Piattelli, A. Effects of Bur Wear during Implant Site Preparation: An in Vitro Study. Int. J. Immunopathol. Pharmacol. 2007, 20, 23–26. [Google Scholar] [CrossRef]
- Bagg, J.; Smith, A.J.; Hurrell, D.; McHugh, S.; Irvine, G. Pre-sterilisation cleaning of re-usable instruments in general dental practice. Br. Dent. J. 2007, 202, E22. [Google Scholar] [CrossRef]
- Laheij, A.M.G.A.; Kistler, J.O.; Belibasakis, G.N.; Välimaa, H.; de Soet, J.J.; European Oral Microbiology Workshop (EOMW) 2011. Healthcare-associated viral and bacterial infections in dentistry. J. Oral Microbiol. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Dussart, C.; Saliasi, I.; Laforest, L.; Tramini, P.; Carrouel, F. Observance of Sterilization Protocol Guideline Procedures of Critical Instruments for Preventing Iatrogenic Transmission of Creutzfeldt-Jakob Disease in Dental Practice in France, 2017. Int. J. Environ. Res. Public Health 2018, 15, 853. [Google Scholar] [CrossRef] [PubMed]
- Douet, J.Y.; Lacroux, C.; Aron, N.; Head, M.W.; Lugan, S.; Tillier, C.; Huor, A.; Cassard, H.; Arnold, M.; Beringue, V.; et al. Distribution and Quantitative Estimates of Variant Creutzfeldt-Jakob Disease Prions in Tissues of Clinical and Asymptomatic Patients. Emerg. Infect. Dis. 2017, 23, 946–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Assenza, B.; Di Iorio, D.; Quaranta, A. Effect of sterilization and cleansing on implantology drills. Ital. Oral Surg. 2008, 2, 4–13. [Google Scholar]
- Ministero della Sanità. Norme di Protezione dal Contagio Professionale da HIV Nelle Strutture Sanitarie e Assistenziali Pubbliche e Private; Ministero della Sanità: Rome, Italy, 1990.
- Spaulding, E.H. Chemical disinfection and antisepsis in the hospital. J. Hosp. Res. 1972, 9, 5–31. [Google Scholar]
- Tehemar, S.H. Factors affecting heat generation during implant site preparation: A review of biologic observations and future considerations. Int. J. Oral Maxillofac. Implant. 1999, 14, 127–136. [Google Scholar]
- Rutala, W.A.; Weber, D.J. Disinfection, sterilization, and antisepsis: An overview. Am. J. Infect. Control 2016, 44, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, A.; Assenza, B.; Carinci, F.; Di Donato, L.; Romani, G.L.; Merla, A. Infrared thermographic evaluation of temperature modifications induced during implant site preparation with cylindrical versus conical drills. Clin. Implant Dent. Relat. Res. 2011, 13, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Wilson, T.G.; Valderrama, P.; Watkins-Curry, P.; Chan, J.Y.; Rodrigues, D.C. In Vitro Evaluation of Titanium Exfoliation during Simulated Surgical Insertion of Dental Implants. J. Oral Implant. 2016, 42, 34–40. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Polimeni, A.; Di Iorio, D.; Carinci, F. Bacterial Adhesion on Commercially Pure Titanium and Anatase-Coated Titanium Healing Screws: An In Vivo Human Study. J. Periodontol. 2010, 81, 1466–1471. [Google Scholar] [CrossRef]
- Scarano, A.; Cholakis, A.; Piattelli, A. Histologic Evaluation of Sinus Grafting Materials after Peri-implantitis–Induced Failure: A Case Series. Int. J. Oral Maxillofac. Implant. 2017, 32, e36–e75. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
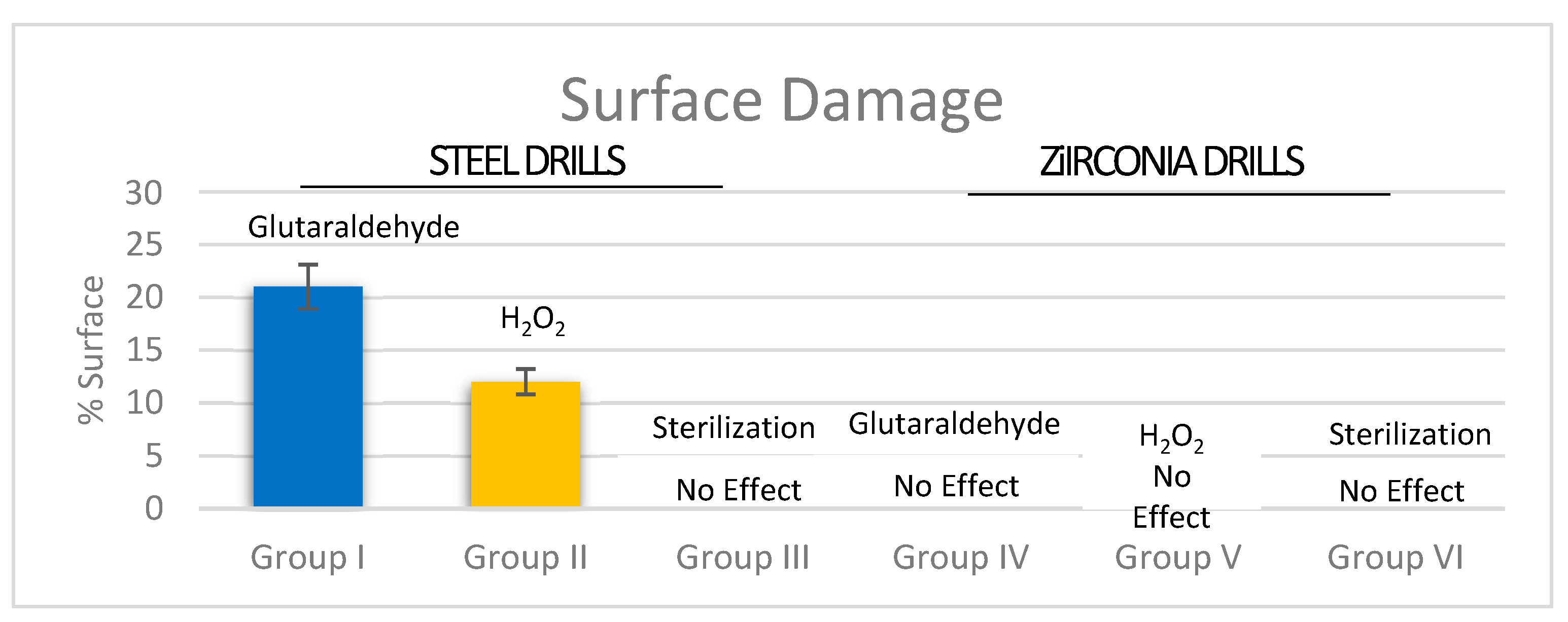
| STEEL DRILLS | ZIRCONIA DRILLS | |||||
|---|---|---|---|---|---|---|
| Group I (6 drills) | Group II (6 drills) | Group III (6 drills) | Group IV (6 drills) | Group V (6 drills) | Group VI (6 drills) | |
| Mean | 21% ** | 12% ** | No Damage ** | No Damage ** | No Damage ** | No Damage ** |
| SD | ±3% | ±2% | − | − | − | − |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Noumbissi, S.; Gupta, S.; Inchingolo, F.; Stilla, P.; Lorusso, F. Scanning Electron Microscopy Analysis and Energy Dispersion X-ray Microanalysis to Evaluate the Effects of Decontamination Chemicals and Heat Sterilization on Implant Surgical Drills: Zirconia vs. Steel. Appl. Sci. 2019, 9, 2837. https://0-doi-org.brum.beds.ac.uk/10.3390/app9142837
Scarano A, Noumbissi S, Gupta S, Inchingolo F, Stilla P, Lorusso F. Scanning Electron Microscopy Analysis and Energy Dispersion X-ray Microanalysis to Evaluate the Effects of Decontamination Chemicals and Heat Sterilization on Implant Surgical Drills: Zirconia vs. Steel. Applied Sciences. 2019; 9(14):2837. https://0-doi-org.brum.beds.ac.uk/10.3390/app9142837
Chicago/Turabian StyleScarano, Antonio, Sammy Noumbissi, Saurabh Gupta, Francesco Inchingolo, Pierbiagio Stilla, and Felice Lorusso. 2019. "Scanning Electron Microscopy Analysis and Energy Dispersion X-ray Microanalysis to Evaluate the Effects of Decontamination Chemicals and Heat Sterilization on Implant Surgical Drills: Zirconia vs. Steel" Applied Sciences 9, no. 14: 2837. https://0-doi-org.brum.beds.ac.uk/10.3390/app9142837