Keeping Doors Closed as One Reason for Fatigue in Teenagers—A Case Study


Department of Air Protection, Silesian University of Technology, 22B Konarskiego St., 44-100 Gliwice, Poland
*
Author to whom correspondence should be addressed.
Appl. Sci. 2019, 9(17), 3533; https://0-doi-org.brum.beds.ac.uk/10.3390/app9173533
Submission received: 9 July 2019
/
Revised: 19 August 2019
/
Accepted: 22 August 2019
/
Published: 28 August 2019
(This article belongs to the Special Issue Indoor Air Quality)
Abstract
:Featured Application
Presented results are only a case study and the authors are not able to relate them to the population of children and teenagers in Poland; however, it is worth underlining the positive effects of opening doors during sleep, since the CO2 concentration decreases 55−64% without a reduction in thermal comfort. This simple action applied by parents can decrease the contribution of low indoor environment quality (IEQIV) in children’s and teenager’s bedrooms to approximately 1% during the night.
Abstract
(1) Background: Healthy teenagers are often sleepy. This can be explained by their physiology and behavioral changes; however, the influence of CO2 concentration above 1000 ppm should not be neglected with respect to sleep dissatisfaction. (2) Methods: CO2 concentrations were measured in two similar bedrooms occupied by girls aged 9 and 13 years old. The scheme of measurements included random opening and closing of the bedroom doors for the night. Additionally, the girls evaluated their sleep satisfaction in a post-sleep questionnaire. (3) Results: During the night, the CO2 concentration varied from 402 to 3320 ppm in the teenager’s bedroom and from 458 to 2176 ppm in the child’s bedroom. When the bedroom doors were open, inadequate indoor air quality (IEQIII and IEQIV categories) was observed in both the teenager’s and child’s bedroom during 11% and 25% of the night, respectively; however, closing the doors increased the contribution of moderate (IEQIII) and low (IEQIV) categories of air to 79% and 86%, respectively. The girls were dissatisfied only when the bedroom door was closed. The satisfied category of sleep was selected only by the younger girl. (4) Conclusions: Opening the bedroom door during the night can decrease the CO2 concentration 55–64% without reducing thermal comfort.
1. Introduction
There is a generally accepted opinion in society that teenagers are sleepy. This notion indicates that sleepiness is a negative issue; however, this particular group of young people has several reasons for being tired. From a physiological perspective, teenagers undergo the processes of puberty and rapid increases in height [1], and, from a psychological aspect, they have problems with low self-esteem, seeking their role in society, and getting easily involved in personal conflicts at school or within the family [1,2]. The duration of sleep varies among individuals, with an average teenager attending school requiring at least 8 h of sleep per night; however, the maturational changes combined with a cell phone or computer use within the hour prior to trying to fall asleep lead to shorter sleeping hours or sleep deprivation [3]. Sleep issues have drawn worldwide attention in recent years. Sleep problems threaten health and quality of life for up to 45% of the world’s population, and 35% of individuals feel that they do not get enough sleep, which has negative effects on both physical and mental health [4]. Rafihi-Ferreira et al. [5] referenced several studies, in which the association between sleep quality and behavioral problems was investigated, demonstrated a relationship between externalizing and internalizing problems and sleep problems in children. This association becomes even more serious when considering that childhood sleep problems may persist and that they constitute a greater risk for other behavioral problems. In comparison with psychological state, body condition, and circadian rhythm, indoor environment quality (IEQ) including thermal conditions and indoor air quality (IAQ) can improve sleep through environmental control. Matricciani et al. [6] in the meta-review underlined that sleep duration is associated with adiposity in children, while sleep quality, timing and variability appear important for children’s health, but further research is needed. Children and teenagers are more adversely affected by indoor air pollution than adults since they breathe a greater volume of air relative to their body weight, which may lead to a greater burden of pollutants on their bodies [7,8]. The quality of the indoor environment not only affects health and comfort, but it may also impair learning ability. Poor IEQ, as a result of inadequate thermal conditions, and IAQ can cause symptoms such as being too hot or too cold as well as feeling restless or sleepy [7].
A powerful remedial to improve IAQ is to increase the outdoor air supply rate; however, in recent years, effort has been focussed on decreasing energy consumption. Within houses, the building airtightness is maximized and the ventilation rates are minimized, leading to a general deterioration in indoor air quality. Consequently, by focussing on optimal indoor thermal comfort, air infiltration and dilution of indoor air pollutants are lowered.
Generally, in passive stack ventilation systems, to create optimal air quality conditions for the maintenance of health and comfort of the occupants, windows should be open slightly. In moderate climate zones such as Poland, this is the best solution from spring to fall seasons; however, during winter, unsealed windows decrease thermal comfort. The Upper Silesia region, in comparison with other Polish regions and European Union countries, is characterized by relatively high particulate matter concentrations. Although the last three decades of economic changes have forced the greatest drop in Polish industrial air pollution by closure of the old steelworks, cookeries, coal mines, and coking plants, emissions from small-scale combustion utilities, such as domestic boilers, together with re-suspension processes from urban surfaces and road traffic, have become particularly dangerous. Investigations performed during the winter season confirm that the hazard of domestic sources originates from the low quality of fuels (coal, biomass, culm, or even refuse) used for heating [9,10]. According to the dominant role of coal combustion in the region, residents are even advised not to open windows during winter, particularly at low wind speed, since it decreases IAQ.
IAQ is a multi-disciplinary phenomenon and is determined by many pathways in which chemical, biological, and physical contaminants eventually become a portion of the total indoor environmental composition. There is spatial and temporal heterogeneity of these contaminants, and the determination of exposure is difficult due to the diversity of time that occupants spend within the space [11,12]. Among indoor air pollutants, carbon dioxide (CO2) is considered a useful and easily measurable indicator of the ventilation and air quality in indoor environments. Although this pollutant itself does not cause serious health issues at lower concentrations and, for short durations, higher concentrations can indicate a lower ventilation level and possible air contamination with other pollutants [13].
In residential non-smoking areas, with the exception of kitchens, occupants are a major source of CO2 through exhalation. Mean concentrations of CO2 during cooking times are significantly higher (p < 0.01) than those during non-cooking times, with no significant differences among fuel types [14]. While the CO2 generation rate per person varies as a function of age, activity, and diet, on average, children aged 6–11 years old produce 448 mg/min/p and adults generate 763 mg/min/p [15]. Persily and de Jonge in [16] presented CO2 generation rates according to age and gender. During sleep, the level of physical activity (MET) is 1.0; thus, the calculated metabolic rate in children aged 6–11 years old is 295 mg/min/p and 271 mg/min/p for boys and girls, respectively, while, for 11–16-year-old males and females, it is 401 mg/min/p and 342 mg/min/p, respectively. Teenagers generate more CO2 according to their higher body weight, and they demand more privacy, therefore keeping their door closed all day and night. The metabolic activity itself influences air quality in bedrooms by reducing the concentration of oxygen and increasing the level of CO2.
For CO2, the exposure limits have been derived exclusively on the basis of health considerations. The Exposure Guidelines for Residential Indoor Air Quality [17] suggest that CO2 concentrations above 1800 mg/m3 (1000 ppm) are indicative of an inadequate supply of fresh air, although complaints have been documented at concentrations as low as 1100 mg/m3 (600 ppm) [17]. Assumptions regarding these levels are in accordance with ASHRAE standards, which previously (62-1989) considered 1000 ppm as the highest acceptable concentration for a minimum sanitary requirement and 8 l/p/s as the minimum ventilation rate. More recent standards (ASHRAE 62-1999, 62-2001, and 62-2004) recommend that the indoor-outdoor differential concentration should not exceed 700 ppm [15]. Generally, a sufficient margin to protect against undesirable changes in the acid-base balance and subsequent adaptive changes such as the release of calcium from bones is a level of 6300 mg/m3 (3500 ppm) [17]. However, a higher maximum exposure concentration is recommended for direct physiological effects of exposure to CO2 as opposed to subjective symptoms. Subjective symptoms such as fatigue, headaches, and an increased perception of warmth and unpleasant odors have been associated with CO2 levels of 900–5800 mg/m3 (500–3200 ppm) [17].
Polish legal acts do not specify permissible concentrations of CO2 in ambient air or in rooms intended for the permanent residence of individuals, i.e., apartments and houses. The regulations of the Ministry of Family, Work, and Social Policy define the highest permissible concentrations and intensities of agents harmful to health in the work environment [18]. The highest permissible CO2 concentration is 9000 mg/m3. Thus far, the Polish Committee for Standardisation followed general guidelines concerning the quality of air inside non-residential buildings (PN-EN 13779 standard [19]), but, in May 2019, the Polish Committee for Standardisation accepted EN-16798-1 (in English) [20] as a national standard and in CEN/TR 16798-2 Technical Report [21] including recommended criteria for the CO2 calculation for demand-controlled ventilation in occupied living rooms and bedrooms. Design ΔCO2 concentration for bedrooms (ppm above outdoors) are within the limits of ≤380 ppm (IEQI), 380–550 ppm (IEQII), 550–950 ppm (IEQIII), and ≥950 ppm (IEQIV) corresponding to high (I), medium (II), moderate (III), and low (IV) indoor environment quality, respectively.
IEQ evaluation based on CO2 concentration and possible effects on occupants comfort has been examined [11,22,23,24,25,26,27]. Polish research on CO2 levels and possible occupant fatigue includes a few publications [9,28,29,30,31]; however, no research regarding IEQ in the bedrooms of Polish children and teenagers have been performed. Such studies can help to better define how behavioral patterns influence the possible exposure levels of air pollutants and occupant fatigue. The present paper presents the results of the measurement of CO2 levels and the corresponding IAQ linked to the possible tiredness and lethargy of a teenager as compared with a child.
2. Materials and Methods
The concentration of CO2 was continuously measured in two bedrooms: one occupied by a teenage girl aged 13 and a second by a younger girl aged 9. The choice of girls instead of boys was intentional since, among children and teenagers, more males than females exhibit excessive nightly use of computer games and consequent sleep disturbances [1]. Moreover, Karjalainen [32] suggested that female occupants should primarily be used as subjects when examining indoor thermal comfort requirements, since, if women are satisfied, then it is highly probable that men are also satisfied. Participation in the present study was voluntary. Prior to starting the measurements, the participants’ parents gave informed consent.
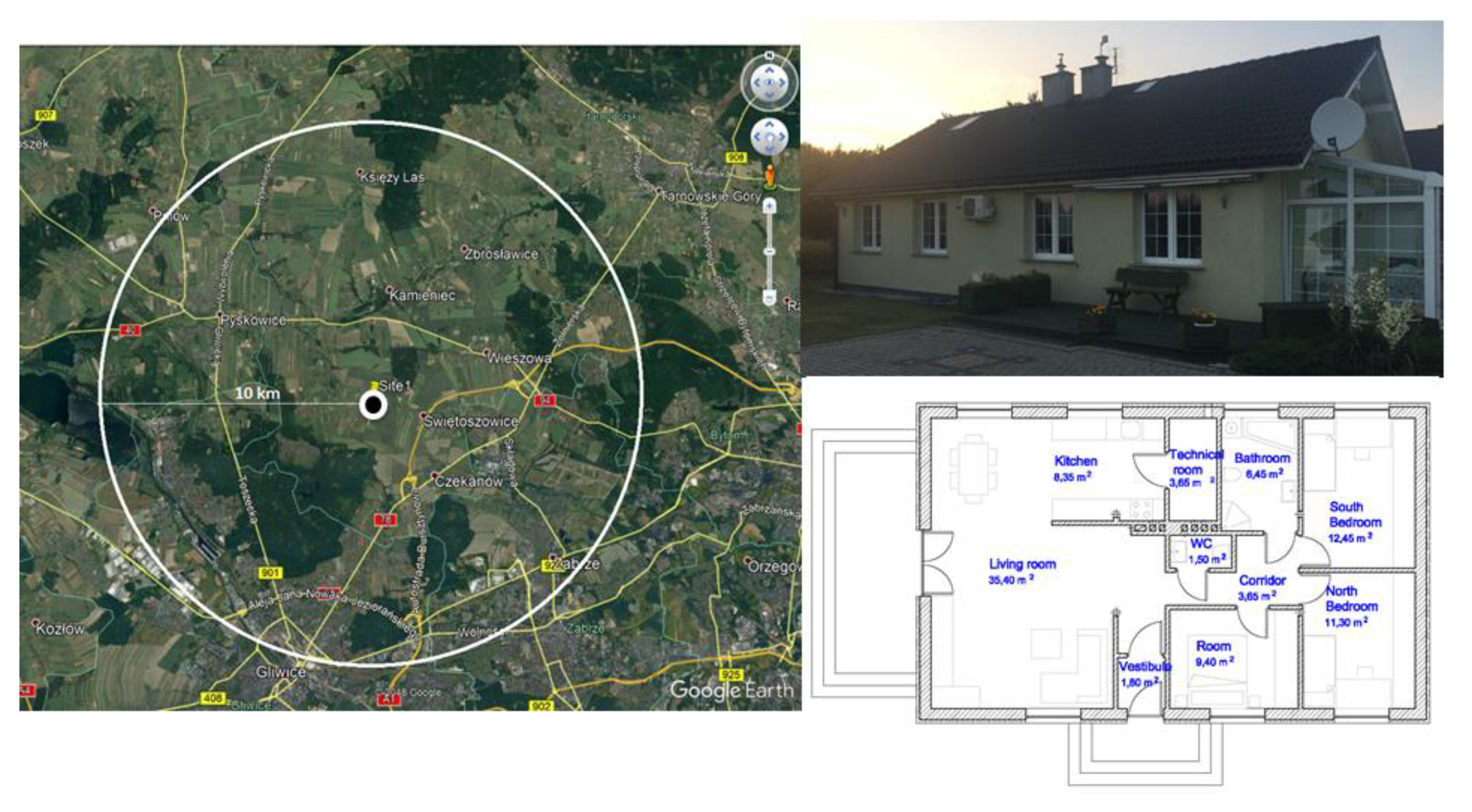
The home of the girls was located in the suburbs of the western part of the Upper Silesia region. The distance from the urban area was approximately 10 km (Figure 1). The house was built in 2008 and was located in the third row of buildings, 100 m from the local street. It was a detached house (Figure 1) with an attic and no basement. The house area was 98 m2 with a glass terrace of 12 m2. The measurements were performed in the South and North bedrooms, which each had an area of approx. 12 m2 and were occupied by the older and younger girl, respectively; detailed information has been added in Supplementary Materials Table S1.
The sampling strategy for CO2 included indoor CO2 concentration, measurement, and questionnaires. Precautions necessary to avoid measurements in air directly exhaled by building occupants were performed as described in [33]. One automatic portable monitor (model 77535, Az Instruments International Ltd., Hong Kong, China) connected to a PC with RS232 software installed was used in the present study. According to Mahyuddin et al. [34], one CO2 sensor in a room with <100 m2 floor area had significant p-value relationships, and the breathing zone within the occupied space was considered to be between 1.0 and 1.2 m in the middle of a zone as a representative location. The monitor was equipped with a non-dispersive infrared sensor. The precision of measurements ranged between +0 and +10,000 ppm CO2: ±100 ppm CO2 or ±3% at a concentration below 100 ppm. The monitor also displayed and recorded in real-time the measurements of air temperature and relative humidity in the bedroom, allowing for logged data to be downloaded for analysis. The selected sampling interval was 60 s.
To estimate the parameters influencing CO2 concentrations in the bedrooms during the measurements, parents were asked to note whether each daughter left the room for a longer period during the night. They provided a diary in which it was specified whether the windows and doors were closed, ajar, or fully open during the monitored days and nights. Additionally, the girls were asked to evaluate their sleep satisfaction as categorized into five levels [4]: very dissatisfied (1), dissatisfied (2), moderate (3), satisfied (4), and very satisfied (5). However, for the analysis, three levels were used: very dissatisfied and dissatisfied, defined as dissatisfied; moderately satisfied, defined as moderate; and satisfied and very satisfied, defined as satisfied. The evaluations of sleep quality were included in the post-sleep questionnaire. In total, 137 questionnaires were acquired, with 121 being valid.
During the study, the family was asked to maintain their regular routine regarding the opening of doors and windows. It should be underlined that, during daylight hours, the bedroom windows were fully open only twice for cleaning and ajar for a maximum of 1 h less than 10 times. The measurements were performed between 16 September 2018 and 2 March 2019. For the final analysis, 102 nights from 9:00 p.m. to 7:00 a.m. (51 nights per room) were included.
3. Results
As mentioned above, proper ventilation controls IAQ. Among the techniques adopted to evaluate ventilation rates, the one based on the measurement and analysis of the indoor CO2 concentration and trends is the most common approach; however, it could be improved by the integration of an electronic nose for odor detection [35]. Acceptable ventilation conditions can be easily achieved in mechanically ventilated rooms, but it is not equally simple to maintain CO2 and odor levels under control in indoor environments that are naturally ventilated [35]. Natural ventilation is typical for detached buildings in Poland, where the ventilation and the IAQ are controlled only by means of air infiltration through cracks and openings. The IAQ gets worse during the winter season when the desire for thermal comfort and acceptable IAQ are in conflict. For the characterization of IAQ by measuring CO2 concentration, several indicators and criteria can be used [25]. We selected the average CO2 concentration and a time fraction over a limit of ΔCO2 values spent during the night according to the PN-EN 16798 standards [20,21].
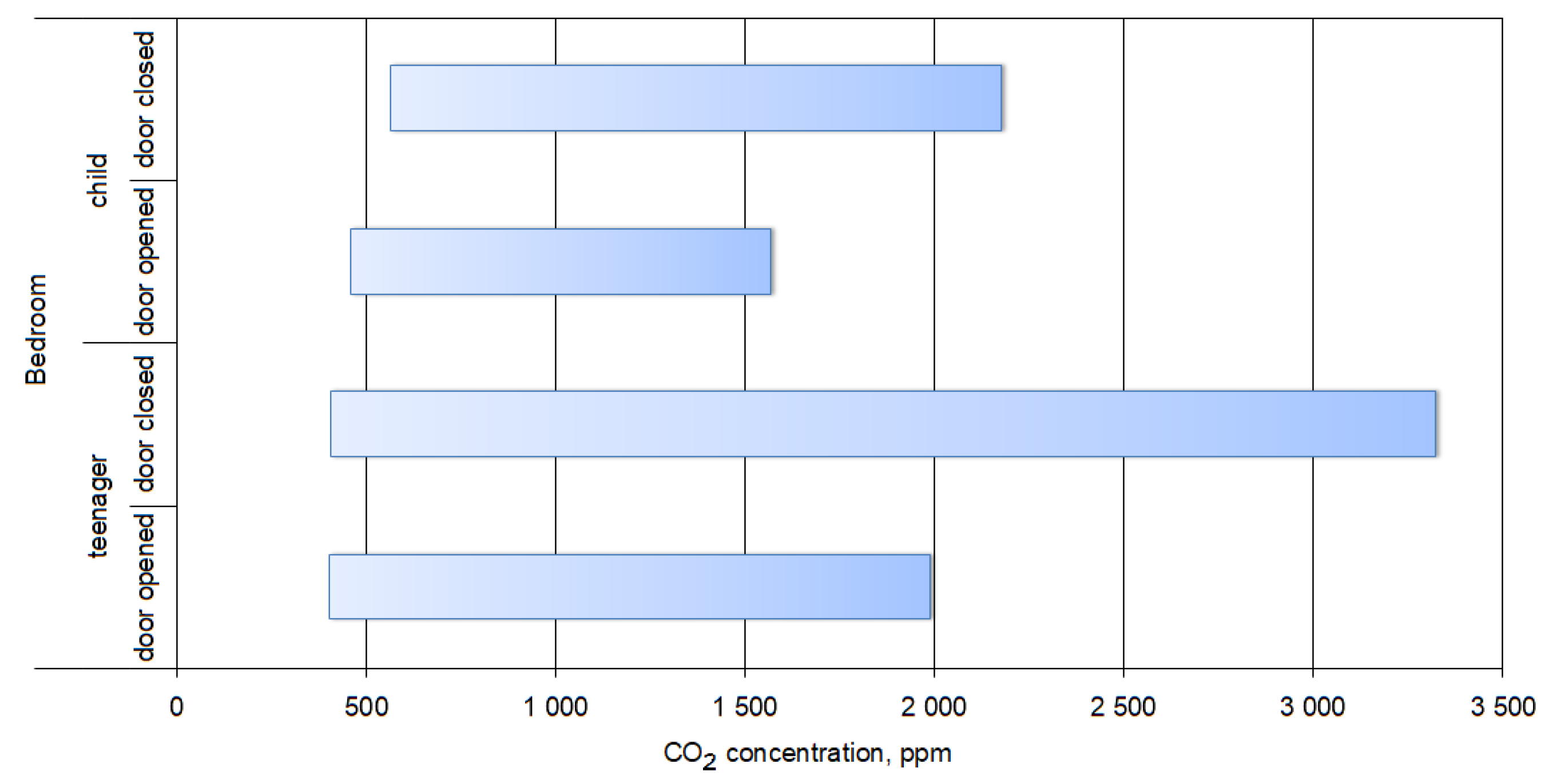
Figure 2 shows the field measurements in the teenager’s and child’s bedrooms, including the CO2 concentration range, when the doors were open and closed.
During the night, the short-term (60 s average) concentrations varied from 402 to 3320 ppm in the teenager’s bedroom and from 458 to 2176 ppm in the child’s bedroom. Thus, the highest concentrations exceeded the limits characteristic of subjective symptoms such as fatigue, headaches, and an increased perception of warmth and unpleasant odors [14]. If we compare the data separately by day of the week (Table 1), it is clear that, despite similar average concentrations, the maximum concentrations were significantly higher in the teenager’s bedroom.
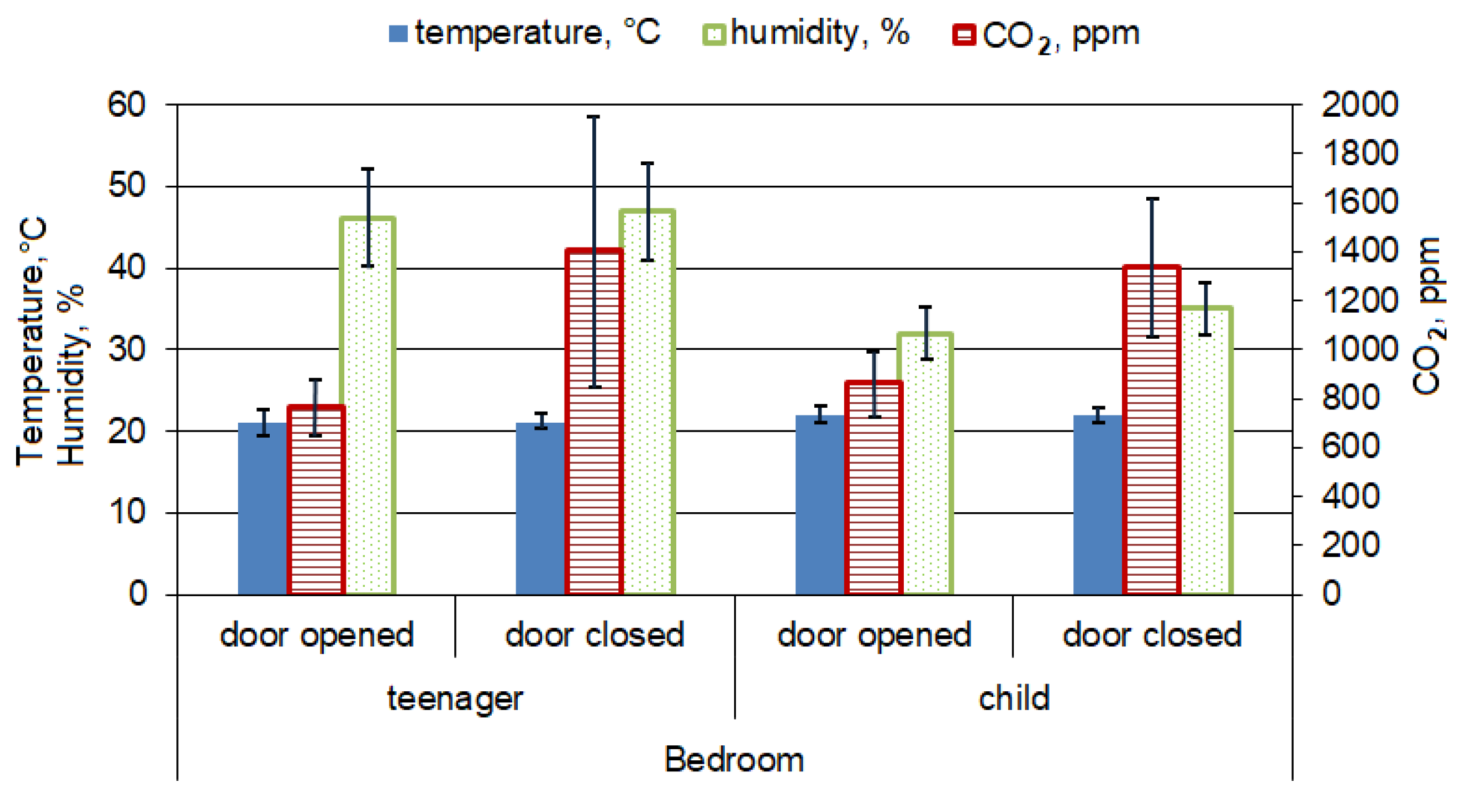
Distinguishing between open and closed doors in the teenager’s and child’s bedrooms, the average nightly concentrations were not significantly different (p = 0.76; 1077 and 1103 ppm, respectively); however, there was a statistically significant difference in CO2 concentration between bedrooms with open and closed doors (Figure 3). In the teenager’s bedroom, opening the doors during the night decreased the average CO2 concentration by 55%, and in the child’s bedroom, the observed decrease was 64%.
Moreover, room temperature and humidity are important factors that may influence perceived environment quality. They both affect the thermal balance of the human body through effects on the skin and respiratory organs. Changes in air temperature trigger a sympathetic reflex via the skin that strengthens with lower air temperature. High temperatures and humidity require the human body to respond by increasing heat loss through the skin surface via blood circulation. The relation between indoor temperature and humidity depends on the season and indoor conditions [36]. In our study in the younger girl bedroom, the temperature and humidity correlation coefficient were −0.10 and −0.08 (p < 0.05) with opened or closed doors, respectively. In the older girl bedroom, the temperature and humidity were weakly positively correlated in the case of opened doors 0.26 and negatively correlated −0.33 in the case of closed doors. The mean room temperature differed between the teenager’s and child’s bedrooms significantly (p < 0.01). The mean temperature in the teenager’s bedroom (21.1 ± 1.11 °C) was lower than that in the child’s bedroom (22.05 ± 0.59 °C); however, the influence of opening and closing the doors to each bedroom during the night was not statistically significant (p > 0.05). The mean nightly temperature in the teenager’s bedroom was 21.07 ± 1.39 °C and 21.01 ± 0.76 °C with open and closed doors, respectively, while, in the child’s bedroom, the mean nightly temperature was 22.06 ± 0.62 °C and 22.03 ± 0.57 °C, respectively. In the case of humidity, a significant difference (p < 0.01) between the teenager’s and child’s bedrooms was also observed (46.46 ± 5.79% and 33.39 ± 3.41%, respectively). In the teenager’s bedroom, the humidity did not differ between nights with respect to open and closed doors (46.04 ± 5.97% and 46.89 ± 5.68%, respectively), while, in child’s bedroom, this difference was statistically significant (p < 0.01; 31.83 ± 3.20% and 34.88 ± 2.95%, respectively).
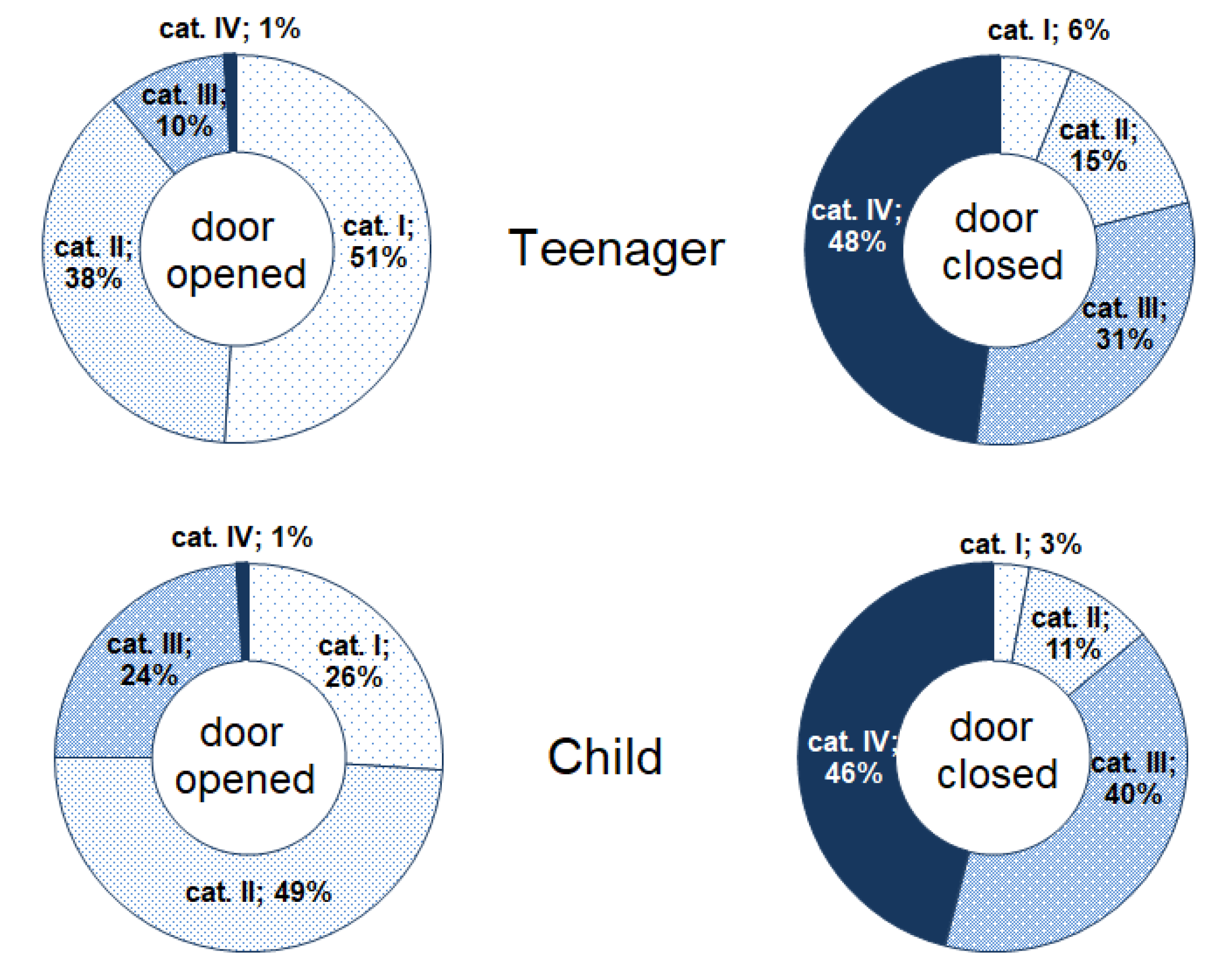
Based on WHO regulations [37] and the PN-EN 16798-1 and CEN/TR 16798-2 standards [20,21], the increase in CO2 concentration in relation to that of outdoor air (ΔCO2) was measured in both bedrooms. During the night, the general IEQ in the bedrooms included 32% in the high category (I), 28% in the medium category (II), 19% in the moderate category (III), and 21% in the low category (IV) in the older girl’s bedroom and 14%, 29%, 32%, and 24%, respectively, in the younger girl’s bedroom. This indicates that, for 10 h of rest at night, the teenager spent approximately 3 h in proper air quality, while the child spent only approximately 1.5 h. The indoor concentrations of CO2 showed a higher contribution of inadequate air quality in the III and IV categories, corresponding to moderate and low IEQ, in the younger girl’s bedroom. When the bedroom doors were open, inadequate IEQ was observed in the teenager’s and child’s bedrooms for 11% and 25% of the night, respectively (Figure 4); however, closing the doors increased the contribution of the moderate (III) and low (IV) categories to 79% and 86%, respectively.
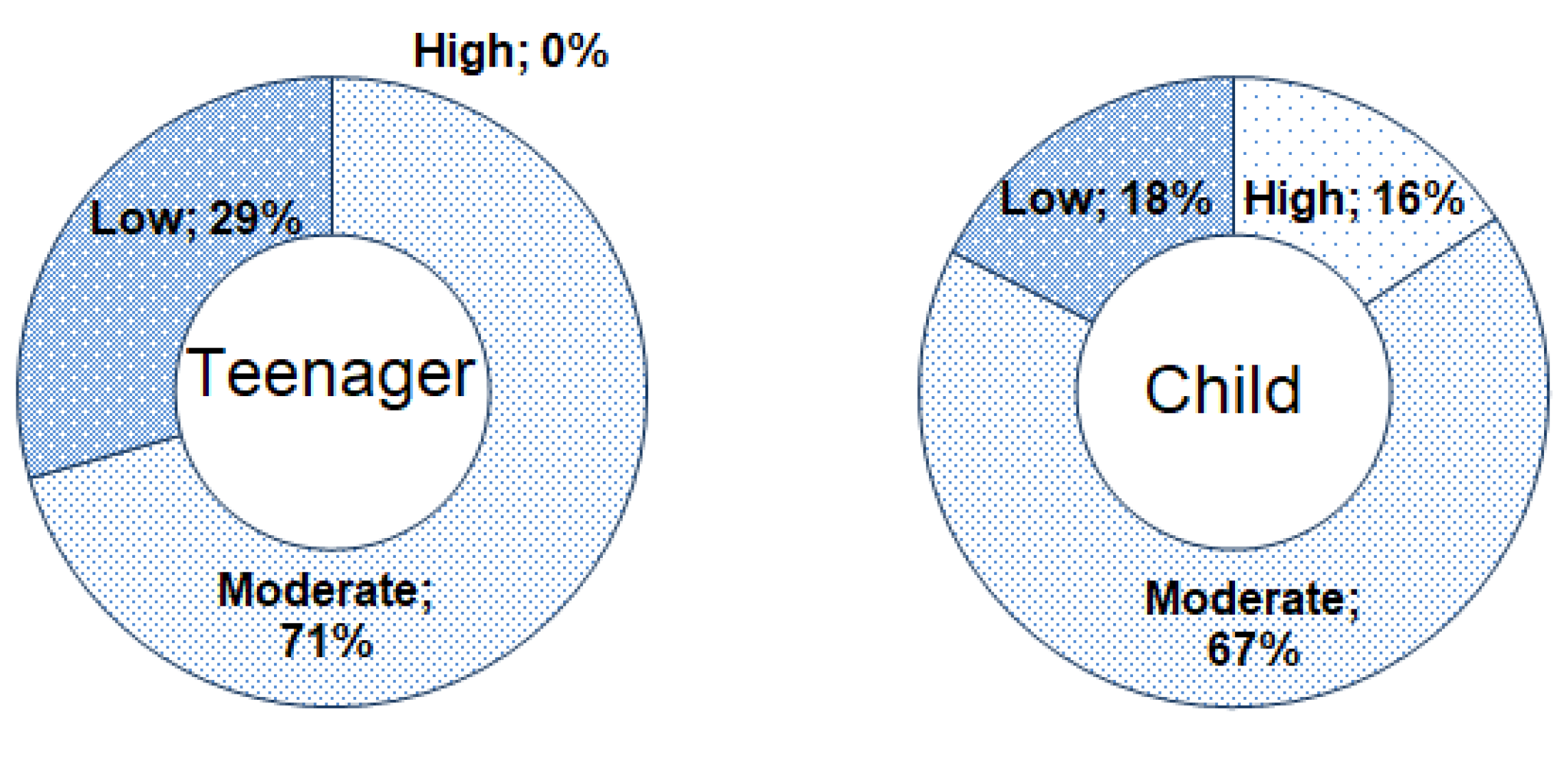
Despite the fact that the teenage girl spent an extra 1.5 h in the high and medium quality environment (IEQI and IEQII), this did not correspond to sleep satisfaction. In the older girl’s opinion, her sleep during study was never satisfying. During 51 nights of measurement, the teenage girl evaluated her sleep as moderate (3) for 36 nights, 13 nights as dissatisfied (2), and only two nights as very dissatisfied (1). The younger girl made a more positive assessment, evaluating seven nights as satisfied (4) and one night as very satisfied (5), eight nights categorized as dissatisfied (2), while one night as very dissatisfied (1), and 34 nights as moderate (3). Following the small contribution of very dissatisfied (1) and very satisfied (5) categories, we gathered categories (1) and (2) into one group defined as low sleep satisfaction, in addition to categories (4) and (5) in one group defined as high sleep satisfaction, as presented in Figure 5.
Deeper analysis reveals that the girls were dissatisfied only when the bedroom door was closed. It is interesting that the average CO2 concentration during the nights evaluated as dissatisfied had a similar average value of 1691 ppm and 1623 ppm in the older and younger girl’s bedroom, respectively. Moreover, the average concentration ranges were not statistically different (1070 ppm and 1079 ppm to 2308 ppm and 1878 ppm) in the teenager’s and child’s bedroom, respectively. The moderate category was selected during the nights with open as well as closed doors. The average concentration of CO2 during nights defined as moderate with open doors was 766 ppm and 903 ppm in the teenager’s and the child’s bedroom, respectively, while, during nights with closed doors, the CO2 concentration was 968 ppm and 1185 ppm, respectively. The satisfied category of sleep was selected only by the younger girl during nights with open doors, corresponding to an average CO2 concentration of 769 ppm.
4. Discussion
To ensure that the CO2 concentration is at a lower level, it is necessary to supply an adequate amount of fresh air instead of used air. Bekö et al. [38] summarised that the most influential variables on the air change rate (ACR) are room volume, number of individuals sleeping in the bedroom, average window and door opening habits, location of the measured room (ground or higher floor), and year of building construction. The authors underlined that more door opening results in a higher air change rate. Our study was performed in two similar bedrooms occupied by girls aged 13 and 9 years old. Due to a low IAQ outside the building, the window opening was very limited; thus, we focussed on door opening and compared it with subjective evaluation of sleep satisfaction. Research by Bekö et al. [38] revealed that, when the bedroom doors are ajar or fully open instead of closed, the ACR increases from 0.48 to 0.55 (14%) and 0.71 (48%). Although we did not calculate the ACH, the observed decrease in CO2 concentration while keeping the bedroom doors open during the night was 55% and 64% in the teenager’s and the child’s bedroom, respectively.
Generally, adults appear to be additional immune to the consequences of sleep deprivation, whereas children, teenagers and particularly young children tend to be a vulnerable subpopulation as they spend the majority of their time indoors at home while their respiratory and other systems are under development [8]. When an individual does not get enough sleep to feel awake and alert, they begin to experience symptoms of sleep deprivation such as yawning, irritability, fatigue, inability to concentrate, moodiness, forgetfulness, lack of motivation, depression, and poor perspective on life [3]. In our study, the average concentration during the night was similar in both bedrooms, at 1077 ppm (teenager) and 1103 ppm (child), which is comparable with the average CO2 concentration in unoccupied bedrooms (999 ppm and 1236 ppm in South and North bedrooms, respectively) as reported by Bouvier et al. [25]. In occupied bedrooms, the authors in [25] reported higher (1585 ppm and 1760 ppm in South and North bedrooms, respectively) than our average concentration of CO2, which was 766 ppm and 860 ppm with open doors and 1402 ppm and 1337 ppm with closed doors, in the teenager’s and the child’s bedroom, respectively (Figure 3). However, it is similar to the average CO2 concentration of 716 ppm measured in 13 bedrooms located in Athens’ residences [39].
During the night with the doors closed, in the teenager’s and the child’s bedroom, 48% and 43% of CO2 concentration measurements were higher than 950 ppm above outdoor CO2 concentration (398 ppm), which corresponds to category IV–low indoor environment quality (IEQIV), and, when open, it was < 1% in both bedrooms. The PN-EN 16798-1 standard [20] underlines that a lower level will not provide any health risk but may decrease comfort. At the same time, the categories are related to the levels of expectations. A normal level would be medium, but, for occupants with special needs (children, elderly, persons with disabilities, etc.), a higher level might be selected. During the research with opened doors, a high IEQ prevailed during 51% of the night in the teenager’s bedroom, and during 26% of the night in the younger girl’s bedroom. In comparison, the authors in [25] reported that time spent by an occupant in a CO2 concentration over 1500 ppm in a mechanically ventilated detached house was approximately 30% of an entire day; thus, the IEQ in researched bedrooms could be satisfying with the door open; however, only the younger girl evaluated sleep satisfaction as high (16%). The subjective assessment of sleep satisfaction points to a lower IEQ in the case of the older girl’s bedroom, which can be supported by a greater CO2 concentration range (Figure 2) in the teenager’s bedroom. Nevertheless, the sharing of categories of environment calculated based on the PN-EN 16798-1 standard [20] does not explain the lower sleep satisfaction in the older girl’s assessment. The reason can be seen in Table 1, which presents average CO2 concentrations and ranges depending on the day of the week. In the teenager’s bedroom, the maximum CO2 concentrations were >3000 ppm on four days of the week (Mondays, Fridays, Saturdays, and Sundays), while, in the younger girl’s bedroom, the maximum CO2 concentration exceeded 2000 ppm only on Saturday nights. These results indicate the important role of short-term high concentrations in sleep satisfaction assessment.
Increasing the effectiveness of the building ventilation system is to decrease the number of exceedances of CO2 concentration in naturally ventilated buildings. A cheap and simple solution is the application of ventilation grills to the window frames [40]. We would recommend simple passive grilles, where the airflow is due to the pressure drop between the indoor and the outdoor environment in addition to the typical pressure drop of the grille itself. Humidity-sensitive grills might not be very effective in this case because of lower humidity values (29.7–50.4%) in the bedrooms during the heating season (Supplementary Materials Table S1).
5. Conclusions
We investigated the variability of CO2 concentration in naturally ventilated bedrooms occupied by a teenage girl and a female child according to their sleep satisfaction. Despite the fact that the average CO2 concentration was 1077 ppm in the teenager’s bedroom and 1103 ppm in the child’s bedroom, the concentration ranges were much wider, from 402 to 3320 ppm and 458 to 2176 ppm, respectively. The average concentration during the night with the doors closed was 1402 ppm and 1336 ppm, respectively; however, the simple action of door opening decreased the CO2 concentration by 55% and 64% in the older and younger girl’s bedroom, respectively.
In the studied period of heating season (from 16 September 2018 to 2 March 2019) during the night (9:00 p.m. to 7:00 a.m.), the time spent by the teenage and younger girls at a concentration over 1348 ppm (IV—low IEQ category) was generally 21% and 24%, respectively. With the doors open, the low IEQ contributed to <1% of the time in both bedrooms; however, keeping the doors closed increased the contribution of low IEQ to 48% and 46% in the teenager’s and the girl’s bedroom, respectively. This highlights the strong influence of simple door opening during children’s sleep.
The evaluation of sleep satisfaction highlights that the teenage girl was more dissatisfied in the mornings than was the younger girl, indicating the important role of short-term CO2 concentrations >3000 ppm in sleep satisfaction assessment.
There are several limitations to this work. This study was limited by small sample size and was confined to one house. The suburban site where the house was located may be different from the general population of children and teenagers in Poland with respect to socioeconomic status, education, and other risk factors for adverse health outcomes, all of which may affect the level of IEQ of the home. The relationships presented here cannot be directly linked to other groups of children, and may not be applicable to other regions due to community differences and the air quality in the area. In Poland, during winter, suburban and rural areas according to individual coal heating systems tend to be more polluted than urban areas connected to collective heating systems, which influences the air quality in the area. Finally, these results apply to residential indoor exposure and may not apply to indoor exposure experienced in settings such as multi-family buildings. Of two bedroom IEQ measures during nights, we found that the parent’s approval of children’s and teenager’s privacy by keeping the doors closed increased airtightness in the bedrooms, favoring low ventilation rates and poor indoor environment quality (IEQ). Caution should be taken regarding the fact that the measurement results may not be able to be interpreted as a human exposure level under regularly ventilated conditions since the data were obtained after the windows were closed. However, it could be useful for predicting exposure of CO2 in children and teenagers during the night, since it is not only in Poland where occupants tend to close the windows and doors while sleeping. Examination of these relationships in other buildings, over a longer period of time, as well as involving wilder groups of participants, could help to explain what parameters affect indoor environment and sleep quality, which has effects on both physical and mental health.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/2076-3417/9/17/3533/s1, Table S1: General characteristic of studied bedrooms as well as the distribution of nightly average indoor temperature and humidity in each studied bedroom depending on door opening.
Author Contributions
Conceptualization, A.M.; Methodology, A.M.; Investigation, A.M.; Data curation, A.M.; Writing—original draft preparation, A.M.; Writing—review and editing, E.Z.-Z.; Visualization, A.M.; Project administration, E.Z.-Z.
Funding
This research was funded by the Faculty of Energy and Environmental Engineering, Silesian University of Technology (statutory research).
Acknowledgments
We would like to thank our colleague Walter Mucha for drawing the scheme of the building.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Landtblom, A.M.; Engström, M. The sleepy teenager-diagnostic challenges. Front. Neurol. 2014, 5, 1–5. [Google Scholar] [CrossRef]
- Herrmann, J.; Koeppen, K.; Kessels, U. Do girls take school too seriously? Investigating gender differences in school burnout from a self-worth perspective. Learn. Individ. Differ. 2019, 69, 150–161. [Google Scholar] [CrossRef]
- Preety, R.; Devi, R.G.; Priya, A.J. Sleep deprivation and cell phone usage among teenagers. Drug Invent. Today 2018, 10, 2073–2075. [Google Scholar]
- Zhang, N.; Cao, B.; Zhu, Y. Indoor environment and sleep quality: A research based on online survey and field study. Build. Environ. 2018, 137, 198–207. [Google Scholar] [CrossRef]
- Rafihi-Ferreira, R.E.; Laura, M.; Pires, N.; Ferreira, E.; Silvares, M. Behavioral intervention for sleep problems in childhood: A Brazilian randomized controlled trial. Psicol. Reflexão Crítica 2019, 32, 1–13. [Google Scholar] [CrossRef]
- Matricciani, L.; Paquet, C.; Galland, B.; Short, M.; Olds, T. Children’s sleep and health: A meta-review. Sleep Med. Rev. 2019, 46, 136–150. [Google Scholar] [CrossRef]
- Hall, R.; Hardin, T.; Ellis, R. School indoor air quality best management practices manual. 2003. Available online: https://www.doh.wa.gov/portals/1/Documents/Pubs/333-044.pdf (accessed on 26 August 2019).
- Stamatelopoulou, A.; Saraga, D.; Asimakopoulos, D.; Vasilakos, C.; Maggos, T. The link between residential air quality and children’s health. Fresenius Environ. Bull. 2017, 26, 162–176. [Google Scholar]
- Mainka, A.; Zajusz-Zubek, E. Indoor air quality in urban and rural preschools in Upper Silesia, Poland: Particulate patter and carbon dioxide. Int. J. Environ. Res. Public Health 2015, 12, 7697–7711. [Google Scholar] [CrossRef]
- Mainka, A.; Zubek, E.Z.; Kaczmarek, K. PM10 composition in urban and rural nursery schools in Upper Silesia, Poland: A trace elements analysis. Int. J. Environ. Pollut. 2017, 61, 98. [Google Scholar] [CrossRef]
- Tham, K.W. Indoor air quality and its effects on humans—A review of challenges and developments in the last 30 years. Energy Build. 2016, 130, 637–650. [Google Scholar] [CrossRef]
- Monn, C. Exposure assessment of air pollutants: A review on spatial heterogeneity and indoor/outdoor/personal exposure to suspended particulate matter, nitrogen dioxide and ozone. Atmos. Environ. 2001, 35, 1–32. [Google Scholar] [CrossRef]
- Pathirana, S.M.; Sheranie, M.D.M.; Halwatura, R.U. Indoor thermal comfort and carbon dioxide concentration: A comparative study of air conditioned and naturally ventilated houses in Sri Lanka. In Proceedings of the Moratuwa Engineering Research Conference (MERCon), Moratuwa, Sri Lanka, 29–31 May 2017; pp. 401–406. [Google Scholar]
- Khalequzzaman, M.; Kamijima, M.; Sakai, K.; Chowdhury, N.A.; Hamajima, N.; Nakajima, T. Indoor air pollution and its impact on children under five years old in Bangladesh. Indoor Air 2007, 17, 297–304. [Google Scholar] [CrossRef]
- Santamouris, M.; Synnefa, A.; Asssimakopoulos, M.; Livada, I.; Pavlou, K.; Papaglastra, M.; Gaitani, N.; Kolokotsa, D.; Assimakopoulos, V. Experimental investigation of the air flow and indoor carbon dioxide concentration in classrooms with intermittent natural ventilation. Energy Build. 2008, 40, 1833–1843. [Google Scholar] [CrossRef]
- Persily, A.; de Jonge, L. Carbon dioxide generation rates for building occupants. Indoor Air 2017, 27, 868–879. [Google Scholar] [CrossRef]
- Government of Canada: Health Canada Exposure Guidelines for Residential Indoor Air Quality. Available online: http://publications.gc.ca/collections/Collection/H46-2-90-156E.pdf (accessed on 26 August 2019).
- Regulation of the Minister of Family, Labor and Social Policy Regarding the Highest Permissible Concentrations and Intensities of Harmful Factors in the Work Environment. Available online: http://www.ilo.org/dyn/natlex/natlex4.detail?p_lang=en&p_isn=99664 (accessed on 26 August 2019).
- PN-EN13779. Ventilation for Non-Residential Buildings. Performance Requirements for Ventilation and Room-Conditioning Systems. Available online: http://www.cres.gr/greenbuilding/PDF/prend/set4/WI_25_Pre-FV_version_prEN_13779_Ventilation_for_non-resitential_buildings.pdf (accessed on 26 August 2019).
- PN-EN 16798-1: 2019. Indoor environmental input parameters for design and assessment of energy performance of buildings addressing indoor air quality, thermal environment, lighting and acoustics. Available online: http://sklep.pkn.pl/pn-en-16798-1-2019-06e.html (accessed on 27 August 2019).
- CEN/TR 16798-2. Technical Report: Energy Performance of Buildings-Ventilation for Buildings-Part 2: Interpretation of the Requirements in EN 16798-1-Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor. Available online: https://epb.center/documents/centr-16798-2/ (accessed on 26 August 2019).
- Bekö, G.; Lund, T.; Nors, F.; Toftum, J.; Clausen, G. Ventilation rates in the bedrooms of 500 Danish children. Build. Environ. 2010, 45, 2289–2295. [Google Scholar] [CrossRef]
- Satish, U.; Mendell, M.J.; Shekhar, K.; Hotchi, T.; Sullivan, D. Is CO2 an indoor pollutant? Direct effects of low-to-moderate CO2 concentrations on human decision-making performance. Environ. Health Perspect. 2012, 120, 1671–1678. [Google Scholar] [CrossRef]
- Norbäck, D.; Nordström, K.; Zhao, Z.; Nordstro, K.; Norba, D. Carbon dioxide (CO2) demand-controlled ventilation in university computer classrooms and possible effects on headache, fatigue and perceived indoor environment: An intervention study. Int. Arch. Occup. Environ. Health 2013, 86, 199–209. [Google Scholar] [CrossRef]
- Bouvier, J.L.; Bontemps, S.; Mora, L. Uncertainty and sensitivity analyses applied to a dynamic simulation of the carbon dioxide concentration in a detached house. Int. J. Energy Environ. Eng. 2019, 10, 47–65. [Google Scholar] [CrossRef]
- Belmonte, J.F.; Barbosa, R.; Almeida, M.G. CO2 concentrations in a multifamily building in Porto, Portugal: Occupants’ exposure and differential performance of mechanical ventilation control strategies. J. Build. Eng. 2019, 23, 114–126. [Google Scholar] [CrossRef]
- Bakó-Biró, Z.; Clements-Croome, D.J.; Kochhar, N.; Awbi, H.B.; Williams, M.J. Ventilation rates in schools and pupils’ performance. Build. Environ. 2012, 48, 215–223. [Google Scholar] [CrossRef]
- Telejko, M.; Zander-Świercz, E. Attempt to improve indoor air quality in kindergartens. Procedia Eng. 2016, 161, 1704–1709. [Google Scholar] [CrossRef]
- Zender-Swiercz, E.; Telejko, M. Indoor air quality in kindergartens in Poland. In Proceedings of the IOP Conference Series: Materials Science and Engineering, 3rd World Multidisciplinary Civil Engineering, Architecture, Urban Planning Symposium (WMCAUS 2018), Prague, Czech Republic, 18–22 June 2018; Volume 471. [Google Scholar]
- Krawczyk, D.A.; Rodero, A.; Gładyszewska-Fiedoruk, K.; Gajewski, A. CO2 concentration in naturally ventilated classrooms located in different climates—Measurements and simulations. Energy Build. 2016, 129, 491–498. [Google Scholar] [CrossRef]
- Mainka, A.; Zajusz-Zubek, E.; Kozielska, B.; Brągoszewska, E. Investigation of air pollutants in rural nursery school–a case study. In Proceedings of the E3S Web of Conferences, X-th Scientific Conference Air Protection in Theory and Practice, Zakopane, Poland, 18–21 October 2017; Volume 28, pp. 1–8. [Google Scholar]
- Karjalainen, S. Thermal comfort and gender: A literature review. Indoor Air 2012, 22, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Seppanen, O.A.; Fisk, W.J.; Mendell, M.J. Association of ventilation rates and CO2 concentrations with health and other responses. Indoor Air 1999, 9, 226–252. [Google Scholar] [CrossRef] [PubMed]
- Mahyuddin, N.; Awbi, H.B. A Review of CO2 measurement procedures in ventilation research. Int. J. Vent. 2012, 10, 353–370. [Google Scholar] [CrossRef]
- Eusebio, L.; Derudi, M.; Capelli, L.; Nano, G.; Sironi, S. Assessment of the indoor odour impact in a naturally ventilated room. Sensors 2017, 17, 778. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.L.; Schwartz, J.; Dockery, D.W. The relationship between indoor and outdoor temperature, apparent temperature, relative humidity, and absolute humidity. Indoor Air 2014, 24, 103–112. [Google Scholar] [CrossRef]
- WHO. WHO Air Quality Guidelines for Europe; WHO: Copenhagen, Denmark, 2000. [Google Scholar]
- Bekö, G.; Toftum, J.; Clausen, G. Modeling ventilation rates in bedrooms based on building characteristics and occupant behavior. Build. Environ. 2011, 46, 2230–2237. [Google Scholar] [CrossRef]
- Stamatelopoulou, A.; Asimakopoulos, D.N.; Maggos, T. Effects of PM, TVOCs and comfort parameters on indoor air quality of residences with young children. Build. Environ. 2019, 150, 233–244. [Google Scholar] [CrossRef]
- D’Ambrosio Alfano, F.R.; Ficco, G.; Palella, B.I.; Riccio, G.; Ranesi, A. An experimental investigation on the air permeability of passive ventilation grilles. Energy Procedia 2015, 78, 2869–2874. [Google Scholar] [CrossRef]
Figure 1.
Location, south view and ground floor plan of the house.

Figure 2.
CO2 concentration inside the teenager’s and child’s bedrooms during the night.

Figure 3.
Mean temperature, relative air humidity, and CO2 concentration inside the teenager’s and child’s bedrooms during the night.
Figure 3.
Mean temperature, relative air humidity, and CO2 concentration inside the teenager’s and child’s bedrooms during the night.

Figure 4.
Categories of the indoor environment inside the teenager’s and child’s bedrooms during the night.
Figure 4.
Categories of the indoor environment inside the teenager’s and child’s bedrooms during the night.

Figure 5.
Low, moderate, and high sleep satisfaction of the teenager and child corresponding to categories: Very dissatisfied and dissatisfied (1) + (2); moderate (3), as well as satisfied and very satisfied (4) + (5).
Figure 5.
Low, moderate, and high sleep satisfaction of the teenager and child corresponding to categories: Very dissatisfied and dissatisfied (1) + (2); moderate (3), as well as satisfied and very satisfied (4) + (5).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Average, minimum, and maximum CO2 concentrations according to the day of the week.
| Parameters | CO2 Concentrations, ppm | |||||
|---|---|---|---|---|---|---|
| Teenager’s Bedroom | Child’s Bedroom | |||||
| Average | Minimum | Maximum | Average | Minimum | Maximum | |
| Monday | 1127 | 402 | 3102 | 1828 | 1828 | 1828 |
| Tuesday | 998 | 597 | 2336 | 1114 | 554 | 1855 |
| Wednesday | 1088 | 452 | 2897 | 1144 | 458 | 1855 |
| Thursday | 1199 | 411 | 2695 | 1118 | 688 | 1778 |
| Friday | 1195 | 479 | 3320 | 1076 | 563 | 1757 |
| Saturday | 3061 | 3061 | 3061 | 1262 | 599 | 2176 |
| Sunday | 1191 | 405 | 3188 | 1993 | 1993 | 1993 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mainka, A.; Zajusz-Zubek, E. Keeping Doors Closed as One Reason for Fatigue in Teenagers—A Case Study. Appl. Sci. 2019, 9, 3533. https://0-doi-org.brum.beds.ac.uk/10.3390/app9173533
AMA Style
Mainka A, Zajusz-Zubek E. Keeping Doors Closed as One Reason for Fatigue in Teenagers—A Case Study. Applied Sciences. 2019; 9(17):3533. https://0-doi-org.brum.beds.ac.uk/10.3390/app9173533
Chicago/Turabian StyleMainka, Anna, and Elwira Zajusz-Zubek. 2019. "Keeping Doors Closed as One Reason for Fatigue in Teenagers—A Case Study" Applied Sciences 9, no. 17: 3533. https://0-doi-org.brum.beds.ac.uk/10.3390/app9173533
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.