Climatic Factors in Relation to Diarrhoea Hospital Admissions in Rural Limpopo, South Africa

 ,
, 

Abstract
:1. Introduction
2. Methods
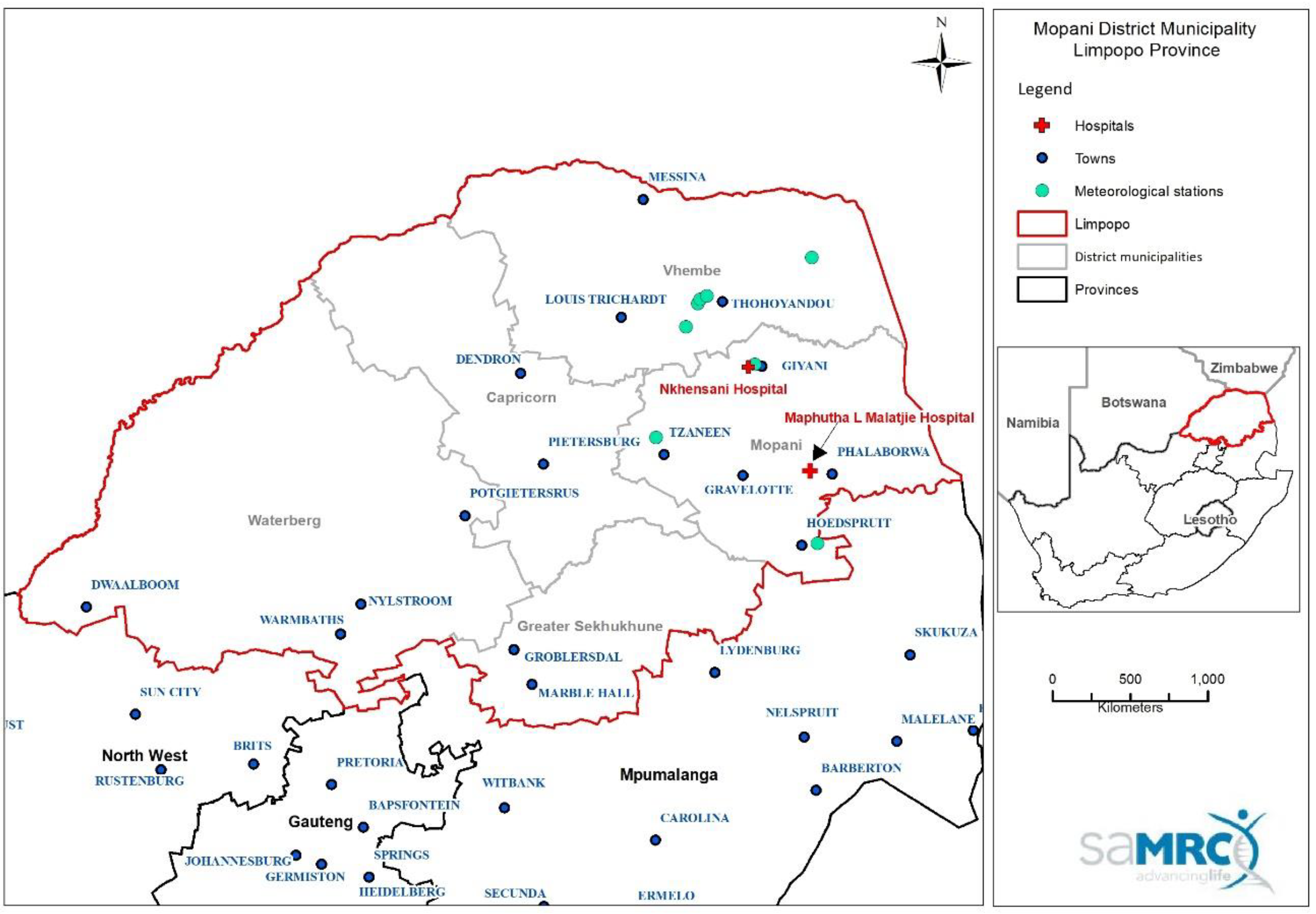
2.1. Study Setting and Data
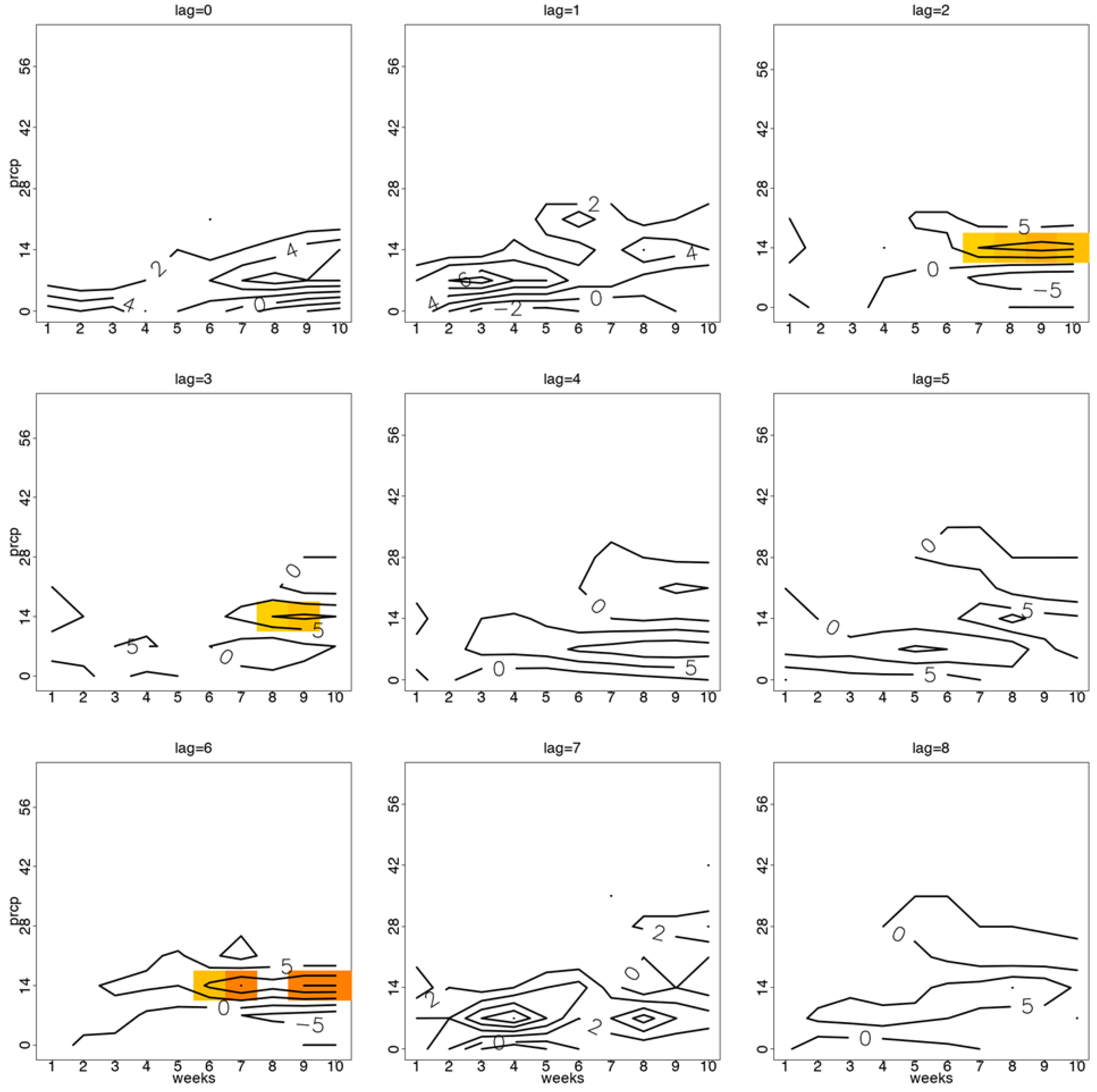
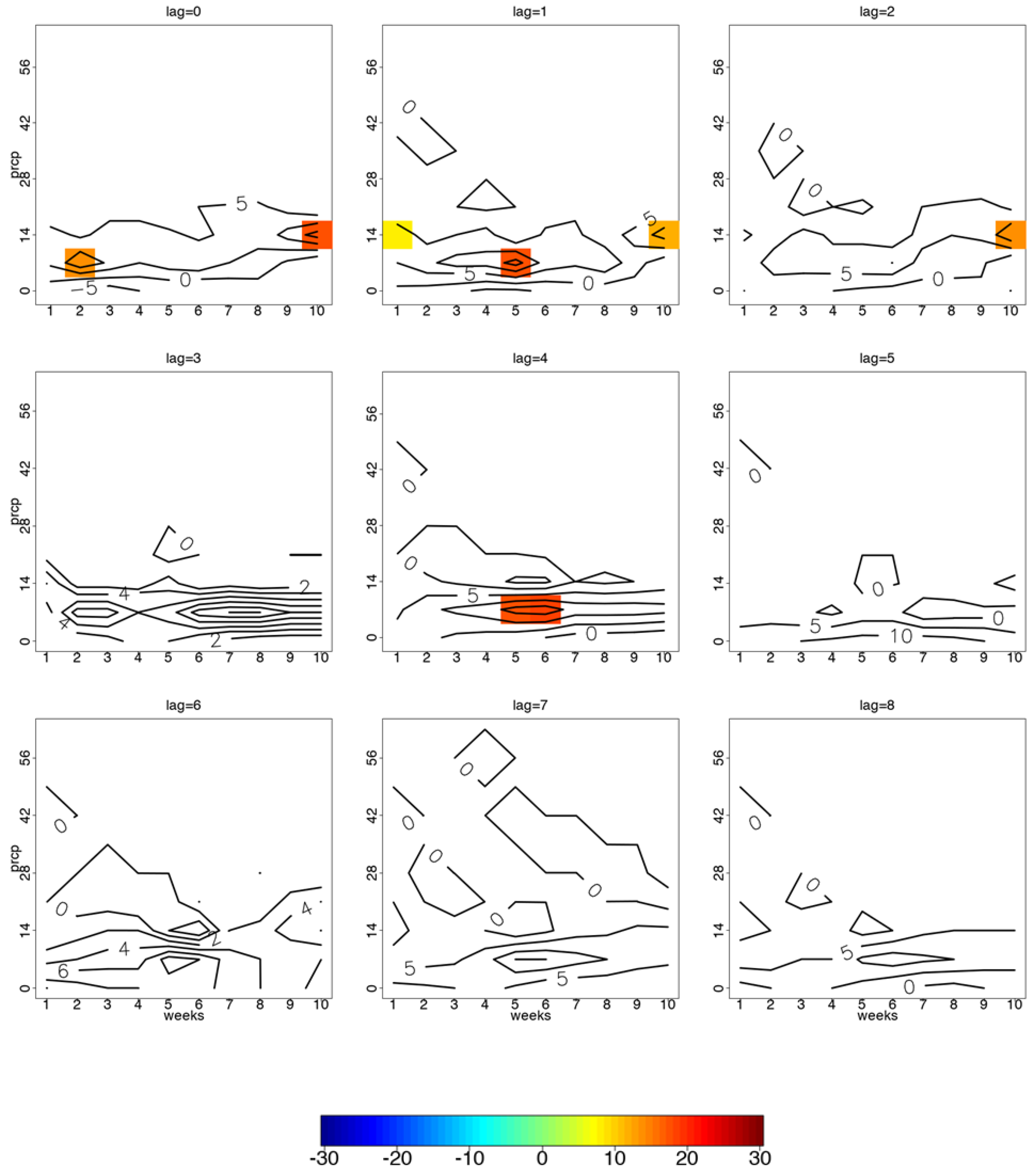
2.2. Contour Analysis
- (i)
- Seasonal patterns that repeated with a fixed period of time (defined according to season with spring: September-October-November (SON); summer: December-January-February (DJF); autumn: March-April-May (MAM); and winter: June-July-August (JJA)) considered on a monthly scale and deemed as the climatological means;
- (ii)
- The underlying trend which could be related to the effort of collecting diarrhoea data, the effect of some community-based intervention or population growth, etc.;
- (iii)
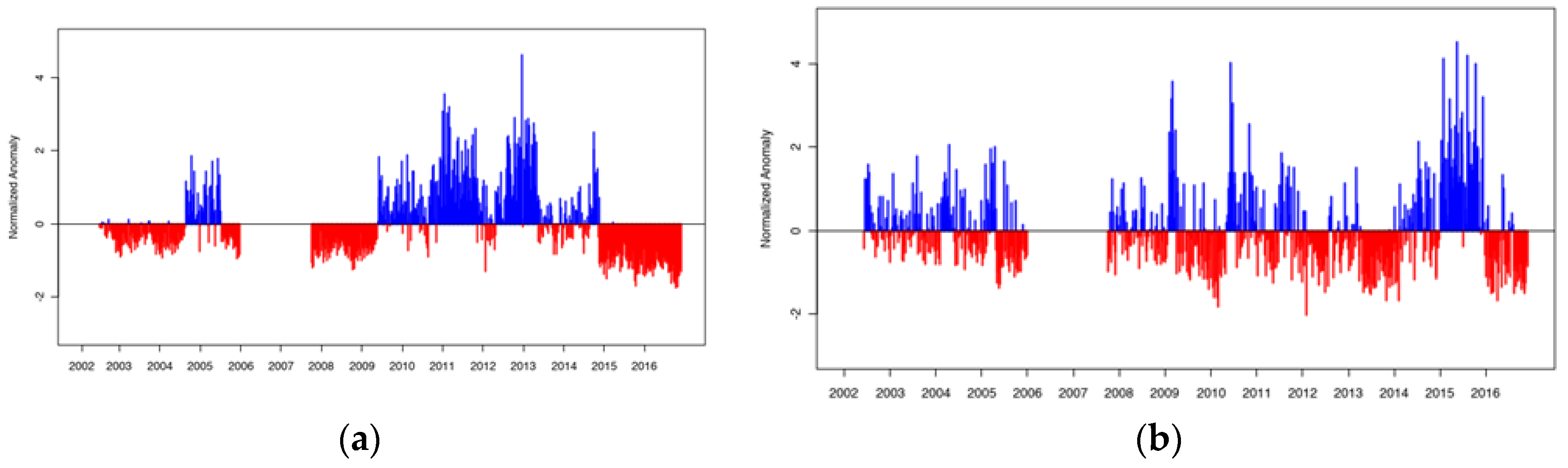
- The residuals of the original time series obtained after the seasonal and trend components were removed, which is thus termed the random component, i.e., the anomalies. Anomalies were calculated according to Equation (1):where A is the anomaly, S is the seasonal component, T is the trend component, and t is time (or week). High weekly anomalies were inferred as ‘higher than normal’ diarrhoea case counts and low anomalies were referred to as ‘lower than normal’. ‘Normal’ refers to the long-term average for the corresponding period/week. In addition, we discarded anomalies that were less than one standard deviation from the mean to retain only anomalously extreme high or extreme low incidence. Then we categorised the high and low incidence (diarrhoea case count anomalies) by season.A(t) = X(t) − S(t) − T(t),
2.3. Ethics Statement
3. Results
3.1. Hospital Admission Counts
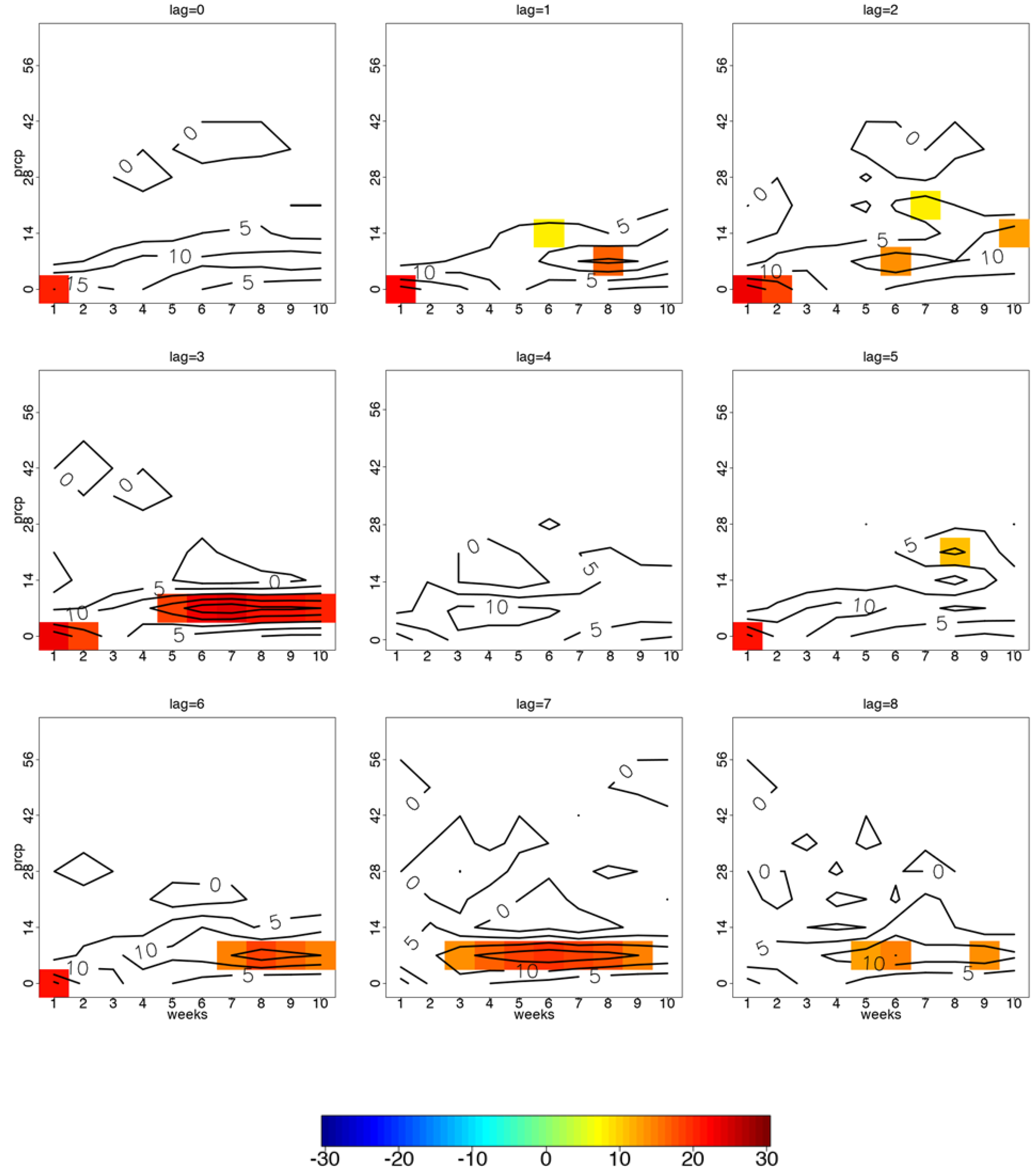
3.2. Precipitation and Diarrhoea Case Counts for Individuals 5 Years and Older
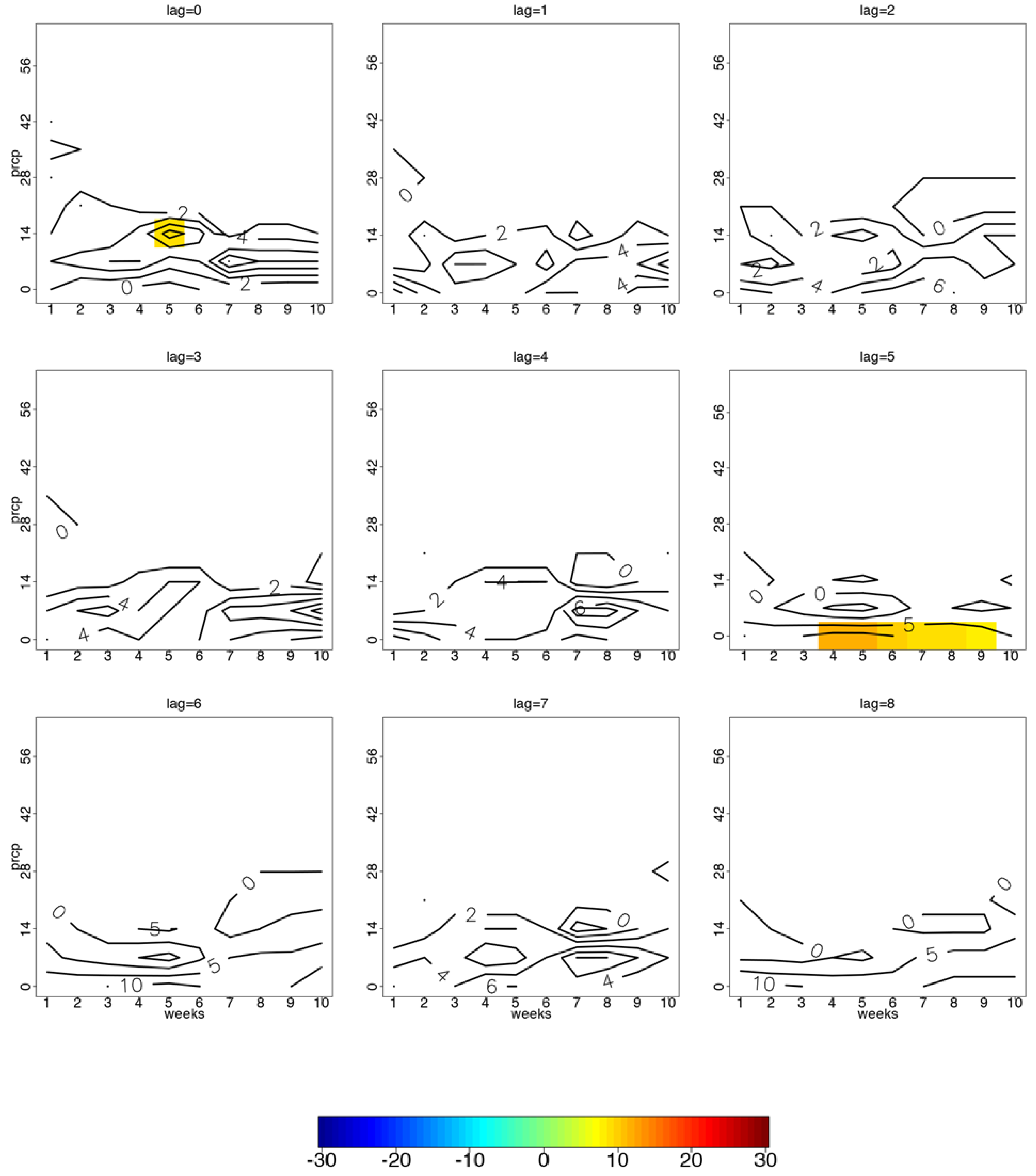
3.3. Precipitation and Diarrhoea Case Counts for Children Under 5 Years of Age
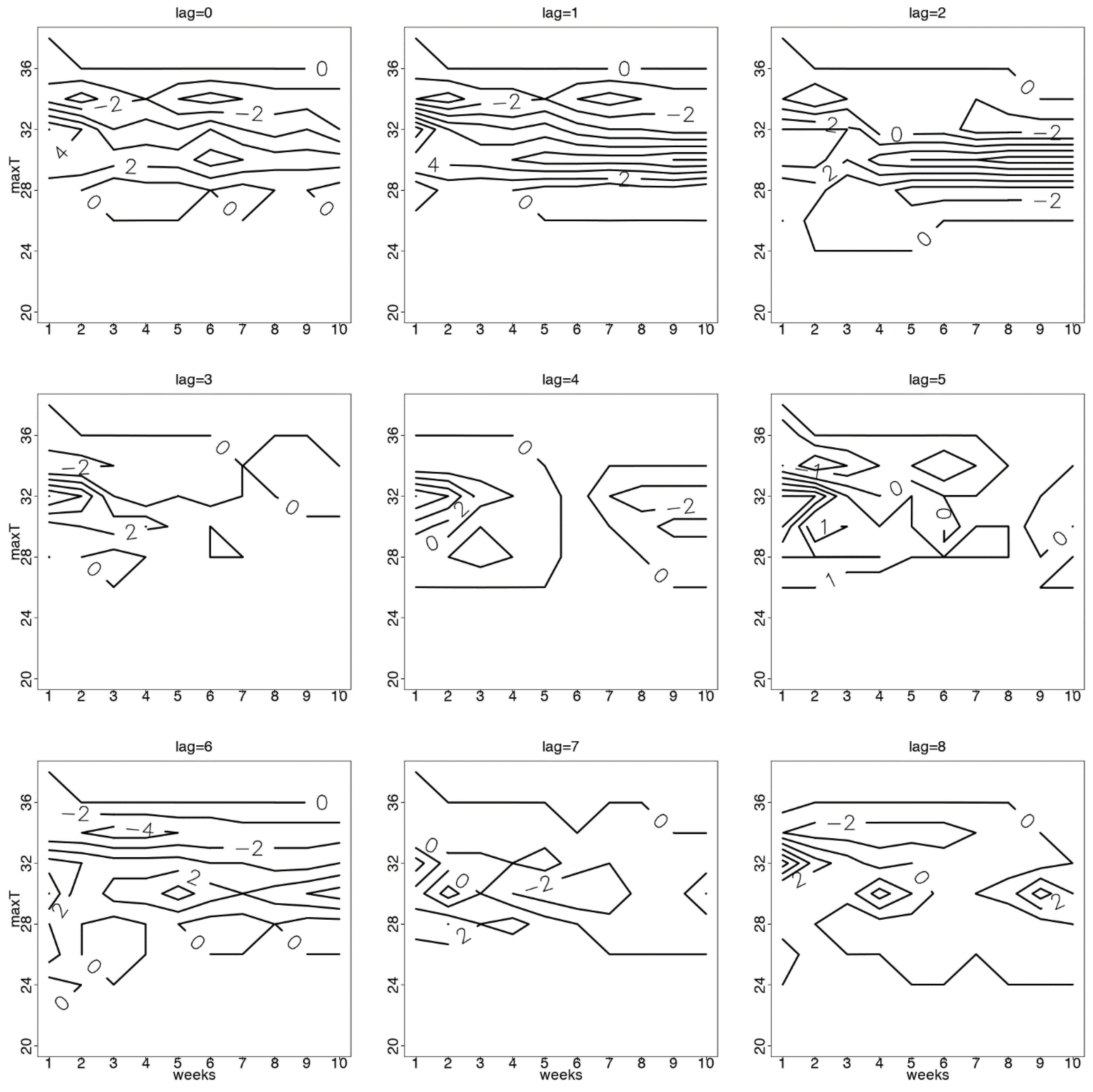
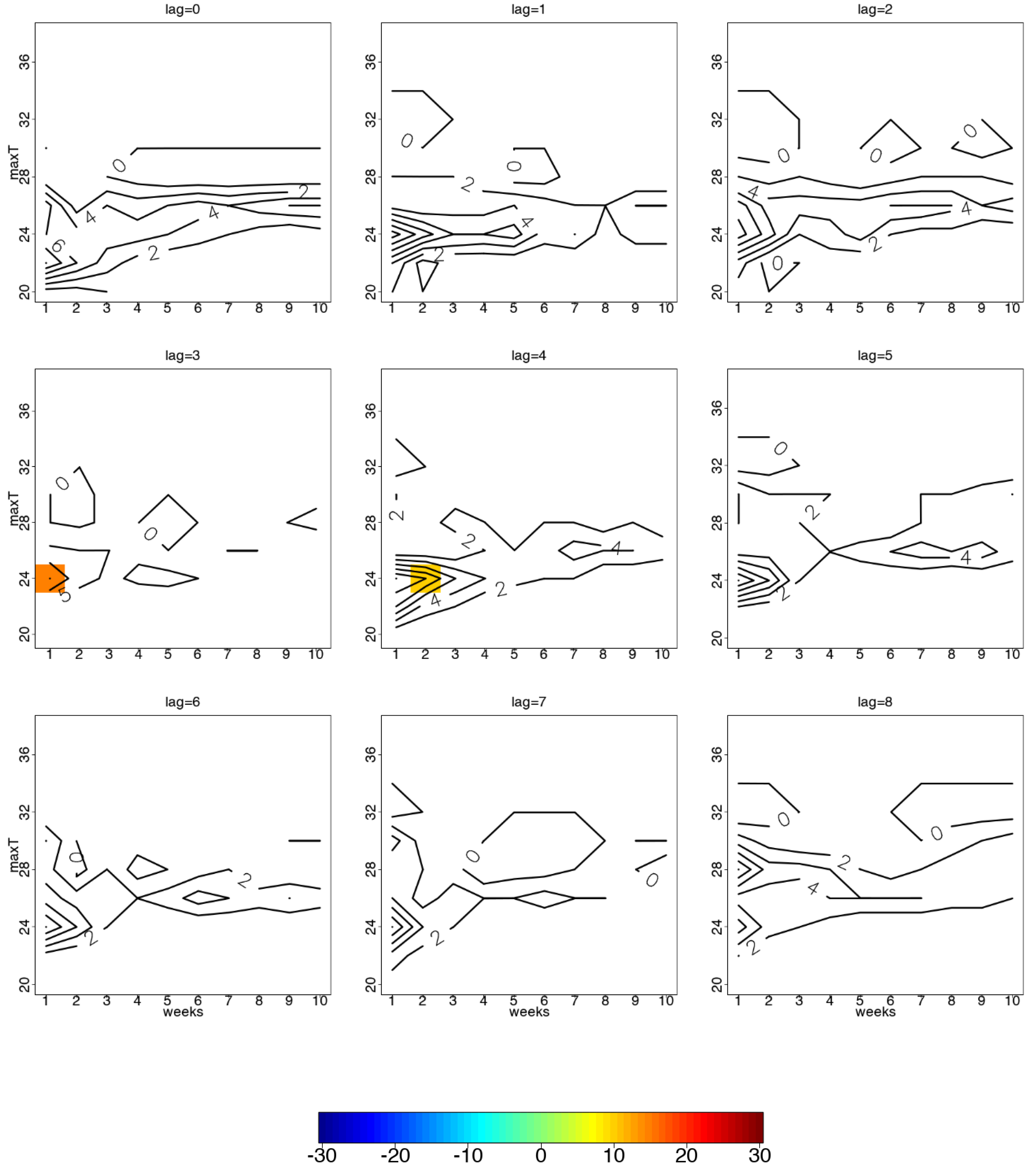
3.4. Temperature and Diarrhoea Case Counts for Individuals Aged 5 Years and Older
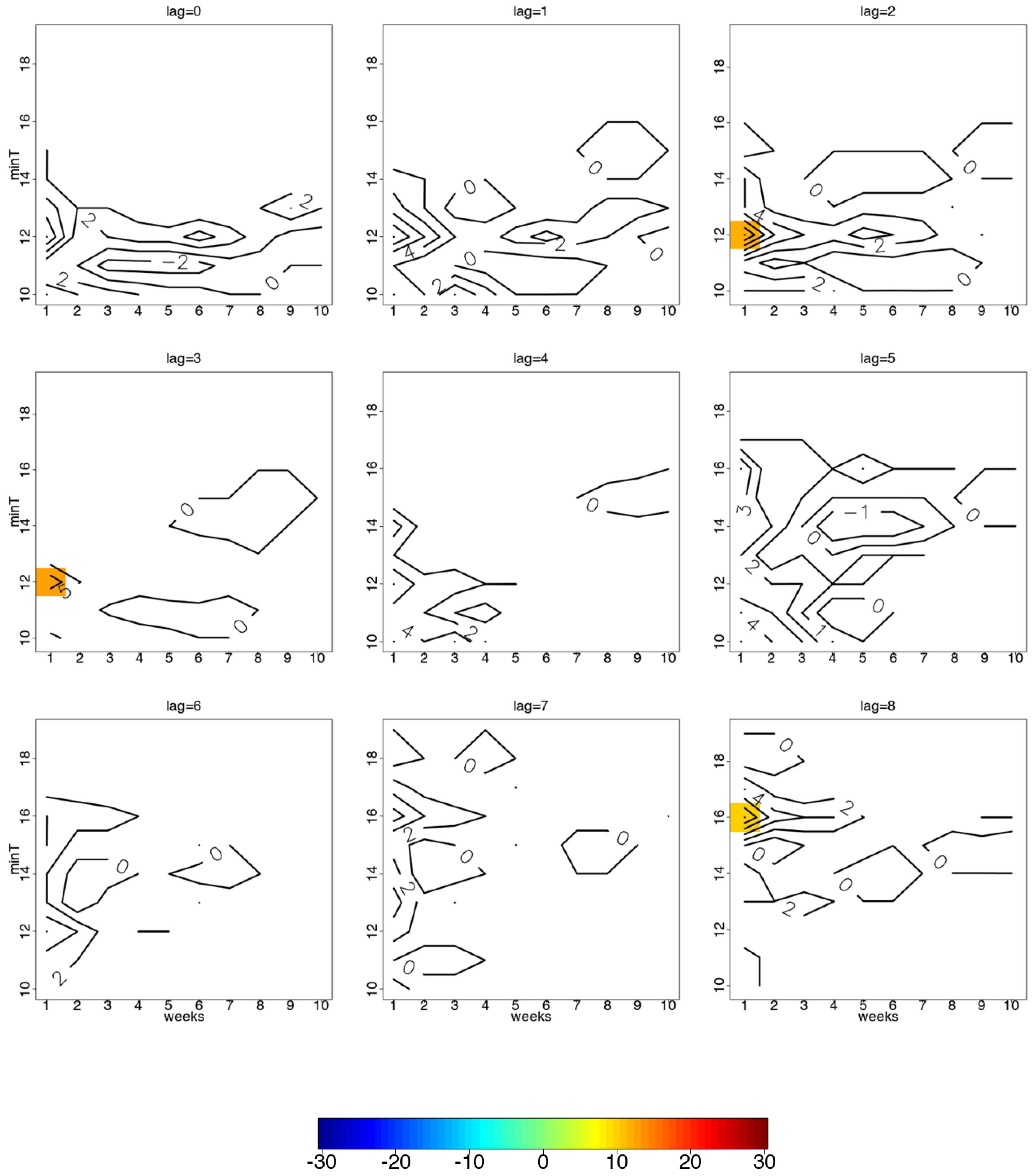
3.5. Temperature and Diarrhoea Case Counts for Children Under 5 Years of Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. 2017 Diarrheal Disease Key Facts. Available online: http://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease (accessed on 8 October 2018).
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrheal disease, as estimated from studies published between 1992 and 2000. Bull. WHO 2003, 81, 197–204. [Google Scholar]
- Awoniton, O.F.; Pillay-van Wky, V.; Dhansay, A.; Day, C.; Bradshaw, D. Diarrhoea in children under five years of age in South Africa (1997–2014). Trop. Med. Int. Health 2016, 21, 1060–1070. [Google Scholar]
- McMichael, A.J.; Woodruff, R.E.; Hales, S. Climate change and human health: Present and future risks. Lancet 2007, 367, 859–869. [Google Scholar] [CrossRef]
- Patz, J.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Haines, A.; Kovats, R.S.; Campbell-Mendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef]
- Levy, K.; Woster, A.P.; Goldstein, R.S.; Carlton, E.J. Untangling the impacts of climate change on waterborne diseases: A systematic review of relationships between diarrheal diseases and temperature, rainfall, flooding, and drought. Environ. Sci. Technol. 2016, 50, 4905–4922. [Google Scholar] [CrossRef]
- WHO. Climate Change and Human Health—Risks and Responses Summary. 2018. Available online: http://www.who.int/globalchange/summary/en/index4.html (accessed on 8 October 2018).
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, A.; Hayashi, T.; Sack, D. Association between climate variability and hospital visits for non-cholera diarrhoea in Bangladesh: Effects and vulnerable groups. Int. J. Epidemiol. 2007, 36, 1030–1037. [Google Scholar] [CrossRef]
- Thiam, S.; Diene, A.N.; Sy, I.; Winkler, M.S.; Schindler, C.; Ndione, J.A.; Faye, O.; Vounatsou, P.; Utzinger, J.; Cissé, G. Association between childhood diarrheal incidence and climatic factors in urban and rural settings in the Health District of Mbour, Senegal. Int. J. Environ. Res. Public Health 2017, 14, 1049. [Google Scholar] [CrossRef]
- Thompson, C.N.; Zelner, J.L.; Nhu Tdo, H.; Phan, M.V.; Hoang Le, P.; Nguyen Thanh, H.; Vu Thuy, D.; Minh Nguyen, N.; Ha Manh, T.; Van Hoang Minh, T.; et al. The impact of environmental and climatic variation on the spatiotemporal trends of hospitalized paediatric diarrhoea in Ho Chi Minh City, Vietnam. Health Place 2015, 35, 147–154. [Google Scholar] [CrossRef]
- Carlton, E.J.; Eisenberg, J.N.S.; Goldstick, J.; Cevallos, W.; Trostel, J.; Levy, K. Heavy rainfall events and diarrhoea incidence: The role of social and environmental factors. Am. J. Epidemiol. 2013, 179, 344–352. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Kanji, S.; Wang, L. The impact of rainfall and temperature variation on diarrheal prevalence in Sub-Saharan Africa. Appl. Geogr. 2012, 33, 63–72. [Google Scholar] [CrossRef]
- Chou, W.C.; Wu, J.L.; Wang, Y.C.; Huang, H.; Sung, F.C.; Chuang, C.Y. Modelling the impact of climate variability on diarrhoea-associated diseases in Taiwan (1996–2007). Sci. Total Environ. 2010, 409, 43–51. [Google Scholar] [CrossRef]
- Ebi, K.L. Adaptation costs for climate change-related cases of diarrheal disease, malnutrition, and malaria in 2030. Glob. Health 2008, 4, 9. [Google Scholar] [CrossRef]
- Haffejee, I.E.; Moosa, A. Rotavirus studies in Indian (Asian) South African infants with acute gastro-enteritis: I. Microbiological and epidemiological aspects. Ann. Trop. Paediatr. 1990, 10, 165–172. [Google Scholar] [CrossRef]
- Mphahlele, M.J.; Steele, A.D. Relative frequency of human rotavirus VP4 (P) genotypes recovered over a ten-year period from South African children with diarrhea. J. Med. Virol. 1995, 47, 1–5. [Google Scholar] [CrossRef]
- Potgieter, N.; de Beer, M.C.; Taylor, M.B.; Steele, A.D. Prevalence and diversity of rotavirus strains in children with acute diarrhoea from rural communities in the Limpopo Province, South Africa, from 1998 to 2000. J. Infect. Dis. 2010, 202 (Suppl. 1), 148–155. [Google Scholar] [CrossRef]
- Lopez-Carr, D.; Pricope, N.G.; Aukema, J.E.; Jankowska, M.M.; Funk, C.; Husak, G.; Michaelson, J. A spatial analysis of population dynamics and climate change in Africa: Potential vulnerability hot spots emerge when precipitation declines and demographic pressures coincide. Popul. Environ. 2014, 35, 323–339. [Google Scholar] [CrossRef]
- Mopani District Municipality. Reviewed Integrated Development Plan 2016–2021 (2017/18 Version 2); Mopani District Municipality: Giyani, South Africa, 2017. Available online: http://www.mopani.gov.za/docs/idp/Mopani%20IDP%202017%202018%20Version%202.pdf (accessed on 17 August 2019).
- Christiansen, T.B.; Lauritsen, J.M. (Eds.) EpiData—Comprehensive Data Management and Basic Statistical Analysis System; EpiData Association: Odense, Denmark, 2010; Available online: http://www.epidata.dk (accessed on 17 August 2019).
- University of Wisconsin-Madison. Contour Analysis. 1997. Available online: http://cimss.ssec.wisc.edu/wxwise/contour/contour1.html (accessed on 8 October 2018).
- Swales, D.; Alexander, M.; Hughes, M. Examining moisture pathways and extreme precipitation in the U.S. Intermountain West using self-organizing maps. Geophys. Res. Lett. 2016, 43, 1727–1735. [Google Scholar] [CrossRef]
- Hope, A.C.A. A simplified Monte Carlo significance test procedure. J. R. Stat. Soc. Ser. B 1968, 30, 582–598. [Google Scholar] [CrossRef]
- Carlton, E.J.; Woster, A.P.; DeWitt, P.; Goldstein, R.S.; Levy, K. A systematic review and meta-analysis of ambient temperature and diarrheal diseases. Int. J. Epidemiol. 2016, 45, 117–130. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016; Available online: https://www.R-project.org/ (accessed on 8 October 2018).
- Purohit, S.G.; Kelkar, S.D.; Simha, V. Time series analysis of patients with rotavirus diarrhoea in Pune, India. J. Diarrheal Dis. Res. 1998, 16, 74–83. [Google Scholar]
- Imai, C.; Hashizume, M. A Systematic review on methodology: Time series regression analysis for environmental factors and infectious diseases. Trop. Med. Health 2015, 43, 1–9. [Google Scholar] [CrossRef]
- Tagbo, B.N.; Mwenda, J.M.; Armah, G.; Obidike, E.O.; Okafor, U.H.; Oguonu, T.; Ozumba, U.C.; Eke, C.B.; Chukwubuike, C.; Edelu, B.O.; et al. Epidemiology of rotavirus diarrhoea among children younger than 5 years in Enugu, South East, Nigeria. Paediatr. Infect. Dis. J. 2014, 33, S19–S22. [Google Scholar] [CrossRef]
- Alexander, K.A.; Carzolio, M.; Goodin, D.; Vance, E. Climate Change is Likely to Worsen the Public Health Threat of Diarrheal Disease in Botswana. Int. J. Environ. Res. Public Health 2013, 10, 1202–1230. [Google Scholar] [CrossRef]
- Singh, R.B.; Hales, S.; De Wet, N.; Raj, R.; Hearnden, M.; Weinstein, P. The influence of climate variation and change on diarrheal disease in the Pacific Islands. Environ. Health Perspect. 2001, 109, 155–159. [Google Scholar] [CrossRef]
- Boithias, L.; Choisy, M.; Souliyaseng, N.; Jourden, M.; Quet, F.; Buisson, Y.; Thammahacksa, C.; Silvera, N.; Latsachack, K.; Sengtaheuanghoung, O.; et al. Hydrological Regime and Water Shortage as Drivers of the Seasonal Incidence of Diarrheal Diseases in a Tropical Montane Environment. PLoS Negl. Trop. Dis. 2016, 10, e0005195. [Google Scholar] [CrossRef]
- Kapwata, T.; Mathee, A.; le Roux, W.; Wright, C.Y. Diarrhoeal disease in relation to possible household risk factors in South African villages. Int. J. Environ. Res. Public Health 2018, 15, 1665. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Climate Variable | Season | |||
|---|---|---|---|---|
| JJA | SON | DJF | MAM | |
| Mean Tmax (°C) (Tmax SE) | 24.0 (0.2) | 28.7 (0.2) | 29.7 (0.2) | 26.9 (0.2) |
| Mean Tmin (°C) (Tmin SE) | 11.1 (0.1) | 16.2 (0.1) | 19.3 (0.1) | 15.6 (0.2) |
| Mean Prcp (mm) (Prcp SE) | 0.6 (0.2) | 7.4 (1.1) | 19.5 (2.6) | 6.9 (1.4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, T.; Kapwata, T.; Behera, S.K.; Minakawa, N.; Hashizume, M.; Sweijd, N.; Mathee, A.; Wright, C.Y. Climatic Factors in Relation to Diarrhoea Hospital Admissions in Rural Limpopo, South Africa. Atmosphere 2019, 10, 522. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090522
Ikeda T, Kapwata T, Behera SK, Minakawa N, Hashizume M, Sweijd N, Mathee A, Wright CY. Climatic Factors in Relation to Diarrhoea Hospital Admissions in Rural Limpopo, South Africa. Atmosphere. 2019; 10(9):522. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090522
Chicago/Turabian StyleIkeda, Takayoshi, Thandi Kapwata, Swadhin K. Behera, Noboru Minakawa, Masahiro Hashizume, Neville Sweijd, Angela Mathee, and Caradee Yael Wright. 2019. "Climatic Factors in Relation to Diarrhoea Hospital Admissions in Rural Limpopo, South Africa" Atmosphere 10, no. 9: 522. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090522