
Peracetic Acid: A Practical Alternative to Formalin for Disinfection of Extracted Human Teeth

 and
and
Abstract
:1. Introduction
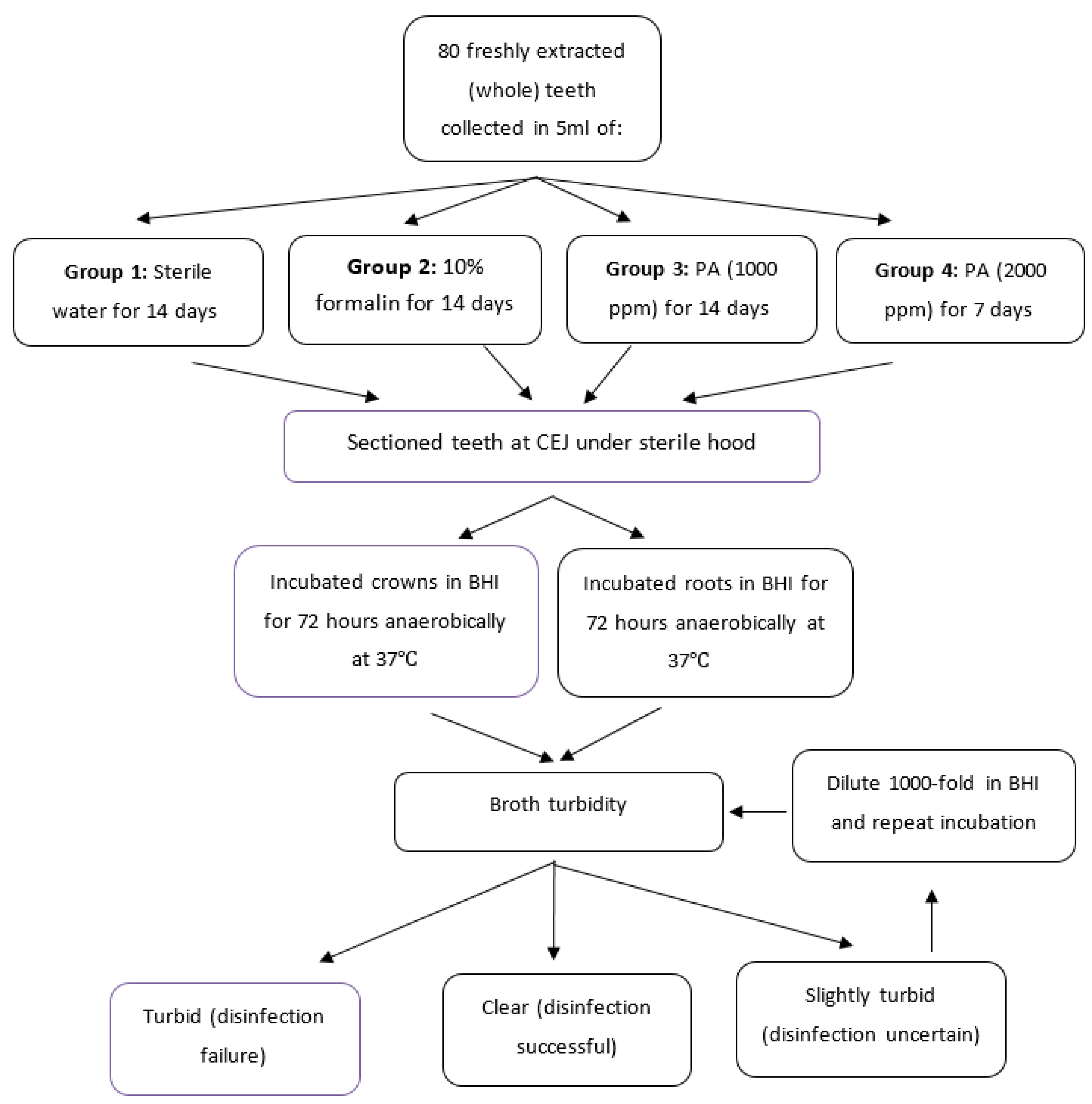
2. Materials and Methods
2.1. Extraction of Infected Teeth
2.2. Preparation of PA Solution
2.3. Transfer of Extracted Teeth into Test and Control Solutions
2.4. Sectioning of Teeth
2.5. Culture Conditions
2.6. Evaluation of Disinfection Effectiveness
2.7. Sample Size Calculation
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Decurcio, D.A.; Lim, E.; Chaves, G.S.; Nagendrababu, V.; Estrela, C.; Rossi-Fedele, G. Pre-clinical endodontic education outcomes between artificial versus extracted natural teeth: A systematic review. Int. Endod. J. 2019, 52, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitter, K.; Gruner, D.; Wolf, O.; Schwendicke, F. Artificial Versus Natural Teeth for Preclinical Endodontic Training: A Randomized Controlled Trial. J. Endod. 2016, 42, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Al-Sudani, D.I.; Basudan, S. Students’ perceptions of pre-clinical endodontic training with artificial teeth compared to extracted human teeth. Eur. J. Dent. Educ. 2017, 21, e72–e75. [Google Scholar] [CrossRef]
- Tchorz, J.P.; Brandl, M.; Ganter, P.A.; Karygianni, L.; Polydorou, O.; Vach, K.; Hellwig, E.; Altenburger, M.J. Pre-clinical endodontic training with artificial instead of extracted human teeth: Does the type of exercise have an influence on clinical endodontic outcomes? Int. Endod. J. 2015, 48, 888–893. [Google Scholar] [CrossRef]
- Lynch, C. Vital guide to Adhesive dentistry. Vital 2006, 3, 21–24. [Google Scholar] [CrossRef] [Green Version]
- CDC. Guidelines for infection control in dental health-care settings—003. MMWR 2003, 52, RR-17. [Google Scholar]
- Pagniano, R.P.; Scheid, R.C.; Rosen, S.; Beck, F.M. Airborne microorganisms collected in a preclinical dental laboratory. J. Dent. Educ. 1985, 49, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Nettey-Marbell, A.; Cook, A., Jr.; Pimenta, L.A.; Leonard, R.; Ritter, A.V. Using extracted teeth for research: The effect of storage medium and sterilization on dentin bond strengths. J. Am. Dent. Assoc. 2007, 138, 1599–1603. [Google Scholar] [CrossRef]
- Milani-Salem, A.; Zand, V.; Jafarabadi-Asghari, M.; Zakeri-Milani, P.; Banifatemeh, A.; Salem-Milani, A.; Asghari-Jafarabadi, M. The effect of protocol for disinfection of extracted teeth recommended by center for disease control (CDC) on microhardness of enamel and dentin. J. Clin. Exp. Dent. 2015, 7, e552–e556. [Google Scholar] [CrossRef] [Green Version]
- Jiang, R.; Xu, Y.; Lin, H. Effects of two disinfection/sterilization methods for dentin specimens on dentin permeability. Clin. Oral Investig. 2019, 23, 899–904. [Google Scholar] [CrossRef]
- Toxicological Profile for Formaldehyde. Report of U.S. Department of Health and Human Services Public Health Service Agency for Toxic Substances and Disease Registry. July 1999. Available online: https://www.atsdr.cdc.gov/ToxProfiles/tp111.pdf (accessed on 15 June 2021).
- Pinkerton, L.E.; Hein, M.J.; Stayner, L.T. Mortality among a cohort of garment workers exposed to formaldehyde: An update. Occup. Environ. Med. 2004, 61, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neghab, M.; Soltanzadeh, A.; Choobineh, A. Respiratory morbidity induced by occupational inhalation exposure to formaldehyde. Ind. Health 2011, 49, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Hope, C.K.; Griffiths, D.A.; Prior, D.M. Finding an alternative to formalin for sterilization of extracted teeth for teaching purposes. J. Dent. Educ. 2013, 77, 68–71. [Google Scholar] [CrossRef] [PubMed]
- FDA. Cleared Sterilants and High-Level Disinfectants with General Claims for Processing Reusable Medical and Dental Devices—March 2015. Available online: https://www.fda.gov/medical-devices/reprocessingreusable-medical-devices-information-manufacturers/ (accessed on 15 June 2021).
- Yoganarasimha, S.; Trahan, W.R.; Best, A.M.; Bowlin, G.L.; Kitten, T.O.; Moon, P.C.; Madurantakam, P.A. Peracetic acid: A practical agent for sterilizing heat-labile polymeric tissue-engineering scaffolds. Tissue Eng. Part C Methods 2014, 20, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Parsell, D.E.; Stewart, B.M.; Barker, J.R.; Nick, T.G.; Karns, L.; Johnson, R.B. The effect of steam sterilization on the physical properties and perceived cutting characteristics of extracted teeth. J. Dent. Educ. 1998, 62, 260–263. [Google Scholar] [CrossRef]
- Soares, L.E.S.; Junior, A.B.; Zanin, F.A.A.; Santo, A.M.E.; Martin, A.A. Effects of heating by steam autoclaving and Er:YAG laser etching on dentin components. Lasers Med. Sci. 2011, 26, 605–613. [Google Scholar] [CrossRef]
- Tate, W.H.; White, R.R. Disinfection of human teeth for educational purposes. J. Dent. Educ. 1991, 55, 583–585. [Google Scholar] [CrossRef] [PubMed]
- Pantera, E.A., Jr.; Schuster, G.S. Sterilization of extracted human teeth. J. Dent. Educ. 1990, 54, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Dominici, J.T.; Eleazer, P.D.; Clark, S.J.; Staat, R.H.; Scheetz, J.P. Disinfection/Sterilization of Extracted Teeth for Dental Student Use. J. Dent. Educ. 2001, 65, 1278–1281. [Google Scholar] [CrossRef] [PubMed]
- White, R.R.; Hays, G.L. Failure of ethylene oxide to sterilize extracted human teeth. Dent. Mater. 1995, 11, 231–233. [Google Scholar] [CrossRef]
- White, J.; Goodis, H.; Marshall, S.; Marshall, G.W. Sterilization of Teeth by Gamma Radiation. J. Dent. Res. 1994, 73, 1560–1567. [Google Scholar] [CrossRef]
- Smitha, D.; Kasetty, S.; Kallianpur, S.; Gupta, S.; Amith, H.; Tijare, M. Vinegar as a disinfectant of extracted human teeth for dental educational use. J. Oral Maxillofac. Pathol. 2014, 18, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Pashley, E.L.; Tao, L.; Pashley, D.H. Sterilization of human teeth: Its effect on permeability and bond strength. Am. J. Dent. 1993, 6, 189–191. [Google Scholar] [PubMed]
- Nawrocka, A.; Kukomska-Szymańska, M. Extracted human teeth and their utility in dental research. Recommendations on proper preservation: A literature review. Dent. Med. Probl. 2019, 56, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeWald, J.P. The use of extracted teeth for in vitro bonding studies: A review of infection control considerations. Dent. Mater. 1997, 13, 74–81. [Google Scholar] [CrossRef]
- Belizário, L.G.; Kuga, M.C.; Castro-Núñez, G.M.; Escalante-Otárola, W.G.; Só, M.V.R.; Pereira, J.R. Effects of different peracetic acid formulations on post space radicular dentin. J. Prosthet. Dent. 2018, 120, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Belizário, L.G.; Kuga, M.C.; Hungaro Duarte, M.A.; Só, M.V.R.; Keine, K.C.; Pereira, J.R. Effect of fiber post space irrigation with different peracetic acid formulations on the bond strength and penetration into the dentinal tubules of self-etching resin cement. J. Prosthet. Dent. 2019, 122, 46.e1–46.e7. [Google Scholar] [CrossRef]
- Keine, K.C.; Kuga, M.C.; Tormin, F.B.C.; Venção, A.C.; Duarte, M.A.H.; Chávez-Andrade, G.M.; Faria, G. Effect of peracetic acid used as single irrigant on the smear layer, adhesion, and penetrability of AH Plus. Braz. Oral Res. 2019, 33, e057. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Treatment | Proportion of Tubes with Turbidity | ||
|---|---|---|---|
| Sterilant | Time | Crown | Root |
| None (sterile H2O) | 14 d | 20/20 | 20/20 |
| Formalin | 14 d | 0/20 * | 0/20 * |
| PA 1000 ppm | 14 d | 0/20 * | 0/20 * |
| PA 2000 ppm | 7 d | 0/20 * | 0/20 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, R.; Bartholomew, J.; Coffey, R.; Carrico, C.; Kitten, T.; Madurantakam, P. Peracetic Acid: A Practical Alternative to Formalin for Disinfection of Extracted Human Teeth. Bioengineering 2021, 8, 217. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120217
Ali R, Bartholomew J, Coffey R, Carrico C, Kitten T, Madurantakam P. Peracetic Acid: A Practical Alternative to Formalin for Disinfection of Extracted Human Teeth. Bioengineering. 2021; 8(12):217. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120217
Chicago/Turabian StyleAli, Riaz, Justin Bartholomew, Randolph Coffey, Caroline Carrico, Todd Kitten, and Parthasarathy Madurantakam. 2021. "Peracetic Acid: A Practical Alternative to Formalin for Disinfection of Extracted Human Teeth" Bioengineering 8, no. 12: 217. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120217