

Cytokines and Obstructive Sleep Apnea in Childhood: Study of a Group of Children

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Polysomnographic Evaluation
2.3. Serum Cortisol Levels
2.4. In Vitro Production of Cytokines by Peripheral Blood Mononuclear Cell Cultures
2.5. Statistical Analysis
3. Results
3.1. Subjects
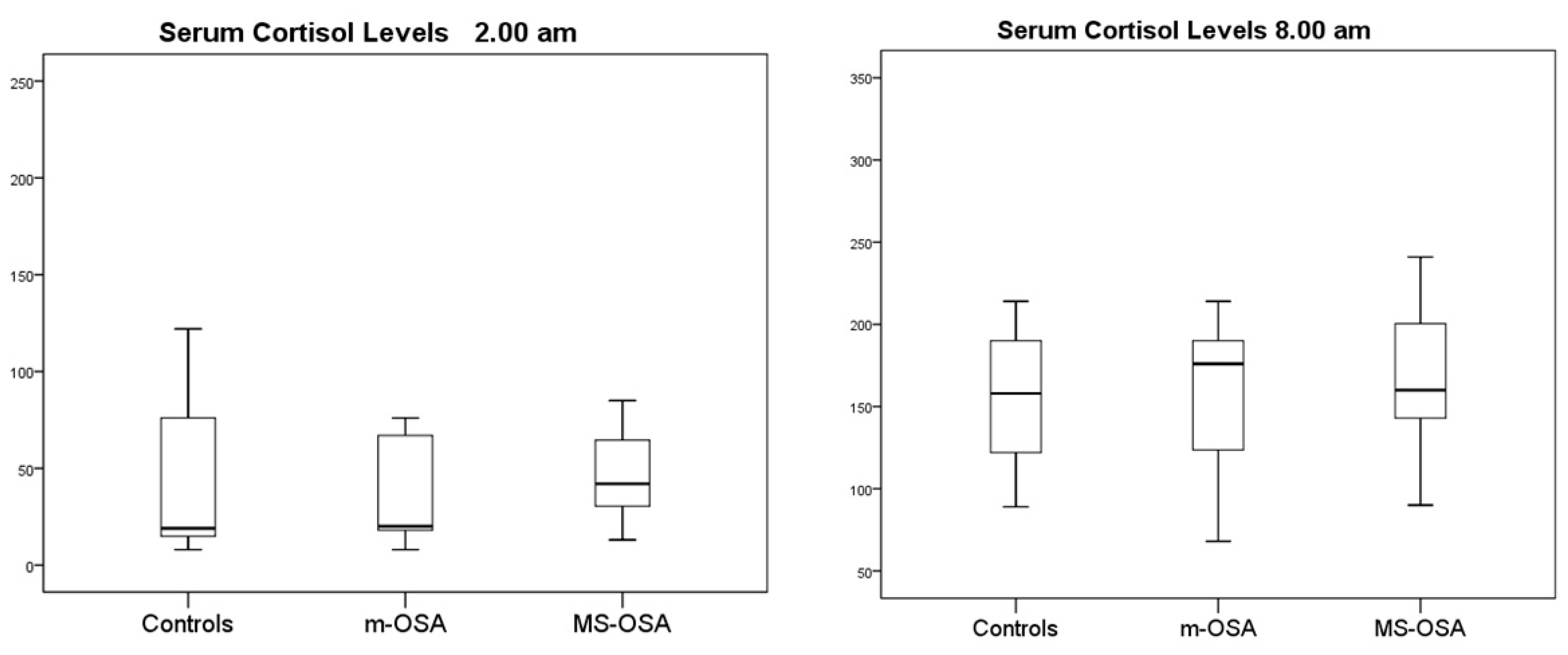
3.2. Serum Cortisol Levels
3.3. In Vitro Cytokine Production by PBMCs
3.3.1. m-OSA vs. MS-OSA
3.3.2. OSA vs. Controls
3.3.3. Controls
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bryant, P.A.; Trinder, J.; Curtis, N. Sick and tired: Does sleep have a vital role in the immune system? Nat. Rev. Immunol. 2004, 4, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.A.; Amin, R.S.; Meltzer, L.J.; Laposky, A.; Fiks, A.G.; Tapia, I.E. Defining and Promoting Pediatric Pulmonary Health: Understanding Sleep and Ventilatory Health. Pediatrics 2023, 152 (Suppl. S2), e2023062292D. [Google Scholar] [CrossRef] [PubMed]
- Verhulst, S. The metabolic consequences of obstructive sleep apnoea in children. Breathe 2009, 6, 111–114. [Google Scholar] [CrossRef]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of Pediatric Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Arens, R.; Muzumdar, H. Childhood obesity and obstructive sleep apnea syndrome. J. Appl. Physiol. 2010, 108, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Davidson Ward, S.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Lehmann, C.; Schechter, M.S.; Sheldon, S.; et al. American Academy of Pediatrics. Obstructive sleep apnea syndrome: Clinical practice guideline for the diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef] [PubMed]
- Dyugovskaya, L.; Lavie, P.; Lavie, L. Increased adhesion molecules expression and production of reactive oxygen species in leukocytes of sleep apnea patients. Am. J. Respir. Crit. Care Med. 2002, 165, 934–939. [Google Scholar] [CrossRef]
- Israel, L.P.; Benharoch, D.; Gopas, J.; Goldbart, A.D. A Pro-Inflammatory Role for Nuclear Factor Kappa B in Childhood Obstructive Sleep Apnea Syndrome. Sleep 2013, 36, 1947–1955. [Google Scholar] [CrossRef]
- Goldbart, A.D.; Gannot, M.; Haddad, H.; Gopas, J. Nuclear factor kappa B activation in cardiomyocytes by serum of children with obstructive sleep apnea syndrome. Sci. Rep. 2020, 10, 22115. [Google Scholar] [CrossRef]
- Regev, D.; Etzion, S.; Haddad, H.; Gopas, J.; Goldbart, A. Obstructive sleep apnea syndrome in vitro model: Controlled intermittent hypoxia stimulation of human stem cells-derived cardiomyocytes. Int. J. Mol. Sci. 2022, 23, 10272. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Sanjabi, A.; Brand, S.; Brühl, A.; Bahmani, D.S. Associations between morning salivary and blood cortisol concentrations in individuals with obstructive sleep apnea syndrome: A Meta-Analysis. Front. Endocrinol. 2021, 11, 568823. [Google Scholar] [CrossRef]
- Kheirandish-Gozal, L.; Gozal, D. Obstructive Sleep Apnea and Inflammation: Proof of Concept Based on Two Illustrative Cytokines. Int. J. Mol. Sci. 2019, 20, 459. [Google Scholar] [CrossRef]
- Balbo, M.; Leproult, R.; Van Cauter, E. Impact of sleep and its disturbances on hypothalamo-pituitary-adrenal axis activity. Int. J. Endocrinol. 2010, 2010, 759234. [Google Scholar] [CrossRef]
- Park, C.S.; Guilleminault, C.; Hwang, S.H.; Jeong, J.H.; Park, D.S.; Maeng, J.H. Correlation of salivary cortisol level with obstructive sleep apnea syndrome in pediatric subjects. Sleep Med. 2013, 14, 978–984. [Google Scholar] [CrossRef]
- Muzumdar, H.; Arens, R. Physiological effects of obstructive sleep apnea syndrome in childhood. Respir. Physiol. Neurobiol. 2013, 188, 370–382. [Google Scholar] [CrossRef]
- Carroll, J. Obstructive sleep-disordered breathing in children: New controversies, new directions. Clin. Chest Med. 2003, 24, 261–282. [Google Scholar] [CrossRef]
- Alexander, N.S.; Schroeder, J.W. Pediatric Obstructive Sleep Apnea Syndrome. Pediatr. Clin. N. Am. 2013, 60, 827–840. [Google Scholar] [CrossRef]
- Brockmann, P.E.; Gozal, D. Review Neurocognitive Consequences in Children with Sleep Disordered Breathing: Who Is at Risk? Children 2022, 9, 1278. [Google Scholar] [CrossRef]
- Liu, X.; Ma, Y.; Ouyang, R.; Zeng, Z.; Zhan, Z.; Lu, H.; Cui, Y.; Dai, Z.; Luo, L.; He, C.; et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J. Neuroinflammation 2020, 17, 229. [Google Scholar] [CrossRef]
- Ryan, S.; Taylor, C.T.; McNicholas, W.T. Selective Activation of Inflammatory Pathways by Intermittent Hypoxia in Obstructive Sleep Apnea Syndrome. Circulation 2005, 112, 2660–2667. [Google Scholar] [CrossRef]
- Smith, D.F.; Hossain, M.; Hura, A.; Huang, G.; McConnell, K.; Ishman, S.L.; Amin, R.S. Inflammatory Milieu and Cardiovascular Homeostasis in Children with Obstructive Sleep Apnea. Sleep 2017, 40, zsx022. [Google Scholar] [CrossRef]
- Gipson, K.; Lu, M.; Kinane, T.G. Sleep-disordered breathing in children. Pediatr. Rev. 2019, 40, 3–13. [Google Scholar] [CrossRef]
- Katz, E.S.; Moore, R.H.; Rosen, C.L.; Mitchell, R.B.; Amin, R.; Arens, R.; Muzumdar, H.; Chervin, R.D.; Marcus, C.L.; Paruthi, S.; et al. Growth after adenotonsillectomy for obstructive apnea: An RCT. Pediatrics 2014, 134, 282–289. [Google Scholar] [CrossRef]
- Kheiradish Gozal, L.; Gileles Hillel, A.; Alonso Alvarez, M.L.; Peris, E.; Bhattacharjee, R.; Terán-Santos, J.; Duran-Cantolla, J.; Gozal, D. Effects of adenotonsillectomy on plasma inflammatory biomarkers in obese children with obstructive sleep apnea: A community-based study. Int. J. Obes. 2015, 39, 1094–1100. [Google Scholar] [CrossRef]
- Lee, C.H.; Hsu, W.C.; Chang, W.H.; Lin, M.T.; Kang, K.T. Polysomnographic finding after adenotonsillectomy for obstructive sleep apnea in obese and non-obese children: A systematic review and meta-analysis. Clin. Otolaryngol. 2016, 41, 498–510. [Google Scholar] [CrossRef]
- Bhattacharyya, N.; Lin, H.W. Changes and consistencies in the epidemiology of pediatric adenotonsillar surgery, 1996–2006. Otolaryngol. Head Neck Surg. 2010, 143, 680–684. [Google Scholar] [CrossRef]
- Weatherly, R.A.; Mai, E.F.; Ruzicka, D.L.; Chervin, R.D. Identification and evaluation of obstructive sleep apnea prior to adenotonsillectomy in children: A survey of practice patterns. Sleep Med. 2003, 4, 297–307. [Google Scholar] [CrossRef]
- Bhattacharjee, R.; Kheirandish-Gozal, L.; Kaditis, A.G.; Verhulst, S.L.; Gozal, D. C-reactive protein as a potential biomarker of residual obstructive sleep apnea following adenotonsillectomy in children. Sleep 2016, 39, 283–291. [Google Scholar] [CrossRef]
- Li, Q.; Zheng, X. Tumor necrosis factor alpha is a promising circulating biomarker for the development of Obstructive Sleep Apnea-syndrome: A meta-analysis. Oncotarget 2017, 8, 27616–27626. [Google Scholar] [CrossRef]
- Martınez-Garcıa, M.A.; Oscullo, G.; Gomez-Olivas, J.D.; Gozal, D. Measuring severity in OSA: The arguments for collaboratively developing a multidimensional score. J. Clin. Sleep Med. 2023, 19, 1705–1707. [Google Scholar] [CrossRef]
- Cortese, R.; Adams, T.S.; Cataldo, K.H.; Hummel, J.; Kaminski, N.; Kheirandish-Gozal, L.; Gozal, D. Single-cell RNA-seq uncovers cellular heterogeneity and provides a signature for paediatric sleep apnoea. Eur. Respir. J. 2023, 61, 2201465. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.E.; Mohamed, A.; Ebrahim, A.; Zahran, M.; Eltonsy, M.; Zewail, A.; Kasem, A.; Abdelaal, K.; Seddeek, M.; Ahmed, Z. Alterations in Inflammatory Markers and Cognitive Ability after Treatment of Pediatric Obstructive Sleep Apnea. Medicina 2023, 59, 204. [Google Scholar] [CrossRef]
- Mohit; Tomar, M.S.; Sharma, D.; Nandan, S.; Pateriya, A.; Shrivastava, A.; Chand, P. Emerging role of metabolomics for biomarker discovery in obstructive sleep apnea. Sleep Breath. 2023, 27, 1247–1254. [Google Scholar] [CrossRef]
- Liao, J.; Gao, X.; Shi, Y.; Li, Y.; Han, D. Evaluation of obstructive sleep apnea: An analysis based on aberrant genes. Sleep Breath. 2023, 27, 1419–1431. [Google Scholar] [CrossRef]
- Sánchez-de-la-Torre, M.; Barbé, F. Cellular heterogeneity insights and molecular signatures in paediatric sleep apnoea. Eur. Respir. J. 2023, 61, 2202316. [Google Scholar] [CrossRef]
- Kohane, I.S.; Valtchinov, V.I. Quantifying the white blood cell transcriptome as an accessible window to the multiorgan transcriptome. Bioinformatics 2012, 28, 538–545. [Google Scholar] [CrossRef]
- Polotsky, V.Y.; Bevans-Fonti, S.; Grigoryev, D.N.; Punjabi, N.M. Intermittent hypoxia alters gene expression in peripheral blood mononuclear cells of healthy volunteers. PLoS ONE 2015, 10, e0144725. [Google Scholar] [CrossRef]
- Lin, S.W.; Tsai, C.N.; Lee, Y.S.; Chu, S.F.; Chen, N.H. Gene expression profiles in peripheral blood mononuclear cells of Asian obstructive sleep apnea patients. Biomed. J. 2014, 37, 60–70. [Google Scholar] [CrossRef]
- Tan, H.-L.; Gozal, D.; Wang, Y.; Bandla, H.P.; Bhattacharjee, R.; Kulkarni, R.; Kheirandish-Gozal, L. Alterations in circulating T-cell lymphocyte populations in children with obstructive sleep apnea. Sleep 2013, 36, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Fiedorczuk, P.; Polecka, A.; Walasek, M.; Olszewska, E. Potential diagnostic and monitoring biomarkers of obstructive sleep apnea-umbrella review of Meta-Analysis. J. Clin. Med. 2022, 12, 60. [Google Scholar] [CrossRef]
- Karaka, Z.; Ismailogullari, S.; Korkmaz, S.; Cakir, I.; Aksu, M.; Baydemir, R.; Tanriverdi, F.; Bayram, F. Obstructive sleep apnea is associated with relative hypocortisolemia and decrease hypothalamo-pituitary-adrenal axis response to 1 and 250 µg ACTH and glucagon stimulation tests. Sleep Med. 2013, 14, 160–164. [Google Scholar] [CrossRef]
- Späth-Schwalbe, E.; Schöller, T.; Kern, W.; Fehma, H.L.; Born, J. Nocturnal adrenocorticotropin and cortisol secretion depends on sleep duration and decreases in association with spontaneous awakening in the morning. J. Clin. Endocrinol. Metab. 1992, 75, 1431–1435. [Google Scholar] [CrossRef]
- Cain, D.W.; Cidlowshi, J.A. Immune regulation by glucocorticoids. Nature Rev. Immunol. 2017, 17, 233–247. [Google Scholar] [CrossRef]
- Meeran, K.; Hattersley, A.; Mould, G.; Bloom, S.R. Venipuncture causes rapid rise in plasma ACTH. Br. J. Clin. Pract. 1993, 47, 246–247. [Google Scholar] [CrossRef] [PubMed]
- Malakasioti, G.; Alexopoulos, E.I.; Varlami, V.; Chaidas, K.; Liakos, N.; Gourgoulianis, K.; Kaditis, A.G. Low morning serum cortisol levels in children with tonsillar hypertrophy and moderate-to-severe OSA. Sleep 2013, 36, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Patacchioli, F.R.; Tabarrini, A.; Ghiciuc, C.M.; Dima-Cozma, L.C.; Prete, A.; Bianchini, C.; Nicoletti, F.; Gozal, D.; Villa, M.P. Salivary Biomarkers of Obstructive Sleep Apnea Syndrome in Children. Pediatr. Pulmonol. 2014, 49, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Tauman, R.; Ivanenko, A.; O’Brien, L.M.; Gozal, D. Plasma C-reactive protein levels among children with sleep-disordered breathing. Pediatrics 2004, 113, e564–e569. [Google Scholar] [CrossRef] [PubMed]
- Gozal, D.; Serpero, L.D.; Kheirandish-Gozal, L.; Capdevila, S.O.; Khalyfa, A.; Tauman, R. Sleep measures and morning plasma TNF-α levels in children with sleep-disordered sleeping. Sleep 2010, 33, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Cofta, S.; Wysocka, E.; Michalak, S.; Piorunek, T.; Batura-Gabryel, H.; Torlinski, L. Endothelium-derived markers and antioxidant status in the blood of obstructive sleep apnea males. Eur. J. Med. Res. 2009, 14 (Suppl. S4), 49–52. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, H.; Weyand, C.M.; Goronzy, J. Generation and durability of immune memory in older adults. J. Allergy Clin. Immunol. 2023, 152, 601–603. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, P.; Dinarello, C.A.; Bianchi, M.; Rosandich, M.E.; Repine, J.E.; White, C.W. Hypoxia increases production of interleukin-1 and tumor necrosis factor by human mononuclear cells. Cytokine 1991, 3, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Entzian, P.; Linnemann, K.; Schlaak, M.; Zabel, P. Obstructive sleep apnea syndrome and circadian rhytms of hormones and cytokines. Am. J. Respir. Crit. Care 1996, 153, 1080–1086. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Controls (n = 6) | m-OSA (n = 20) | MS-OSA (n = 16) | p Value | |
|---|---|---|---|---|
| Sex (F/M) | 3/3 | 12/8 | 9/7 | >0.05 |
| Age (months) | 81.53 ± 40.74 | 86 ± 8 | 78 ± 12 | >0.05 |
| BMI (kg/m2) | 17.05 ± 2.57 | 16.9 ± 0.5 | 17.1 ± 0.8 | >0.05 |
| BMI (percentile) | 48.7 ± 6.7 | 54.7 ± 6.8 | 51.9 ± 7.6 | >0.05 |
| 2 am | 8 am | ||||
|---|---|---|---|---|---|
| Unstimulated | PHA | Unstimulated | PHA | ||
| IL-1β | m-OSA | 87.2 (38.3–330.6) pg/mL | 318.1 (193.4–492) pg/mL | 71.0 (47.2–138.5) pg/mL | 317.4 (245.8–460.8) pg/mL |
| Controls | 49.0 (34.8–135.4) pg/mL | 233.2 (131.1–334.6) pg/mL, | 71.0 (52.5–89.1) pg/mL | 313.9 (217.9–368.3) pg/mL | |
| MS-OSA | 54.9 (41.2–177.3) pg/mL | 189.5 (135.5–276.2) pg/mL | 62.3 (60.1–321.8) pg/mL | 502.9 (231.0–533.3) pg/mL | |
| All patients | 49.0 (34.8–267.2) pg/mL | 276.2 (135.5–344.3) pg/mL | 71.0 (52.5–199.0) pg/mL | 317.4 (197.6–525.7) pg/mL | |
| TNF-a | m-OSA | 44.2 (17.1–105.1) pg/mL | 226.6 (176.1–341.8) pg/mL | 17.9 (10.8–46.0) pg/mL | 276.7 (188.9–344.7) pg/mL |
| Controls | 46.8 (18.0–47.9) pg/mL | 321.4 (182.3–360.6) pg/mL | 16.4 (10.8–17.8) pg/mL | 289.4 (210.8–307.8) pg/mL | |
| MS-OSA | 32.7 (6.7–55.2) pg/mL | 79.7 (70.5–120.2) pg/mL | 17.8 (13.5–25.2) pg/mL | 105.4 (75.2–190.7) pg/mL | |
| All patients | 45.9 (8.4–55.2) pg/mL | 220.5 (82.9–360.6) pg/mL | 16.5 (10.4–25.2) pg/mL | 262.4 (116.6–298.6) pg/mL | |
| Comparison between Conditions (p-Values) | |||||
|---|---|---|---|---|---|
| Unstimulated vs. PHA—2am | Unstimulated vs. PHA—8 am | 2 am vs. 8 am—Unstimulated | 2 am vs. 8 am—PHA | ||
| IL-1β | m-OSA | ↑ (p = 0.028) * | ↑ (p = 0.018) * | ↓ (p = 0.214) | ↓ (p = 0.15) |
| Controls | ↑ (p = 0.043) * | ↑ (p = 0.043) * | ↑ (p = 0.39) | ↑ (p = 0.021) * | |
| MS-OSA | ↑ (p = 0.068) | ↑ (p = 0.08) | ↑ (p = 0.84) | ↑ (p = 0.72) | |
| All Patients | ↑ (p = 0.001) * | ↑ (p < 0.01) * | ↑ (p = 0.4) | ↑ (p = 0.11) | |
| TNF-α | m-OSA | ↑ (p = 0.028) * | ↑ (p = 0.028) * | ↓ (p = 0.073) | ↑ (p = 0.16) |
| Controls | ↑ (p = 0.027) * | ↑ (p = 0.027) * | ↓ (p = 0.058) | ↓ (p = 0.95) | |
| MS-OSA | ↑ (p = 0.046) * | ↑ (p = 0.046) * | ↓ (p = 0.27) | ↑ (p = 0.94) | |
| All Patients | ↑ (p < 0.01) * | ↑ (p < 0.01) * | ↓ (p = 0.01) * | ↑ (p = 0.33) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nosetti, L.M.; Tirelli, C.; Marino, F.; Gaiazzi, M.; Sacchi, L.; De Amici, M.; Barocci, F.; Maio, R.; Cosentino, M.; Nespoli, L. Cytokines and Obstructive Sleep Apnea in Childhood: Study of a Group of Children. Biologics 2024, 4, 44-54. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics4010004
Nosetti LM, Tirelli C, Marino F, Gaiazzi M, Sacchi L, De Amici M, Barocci F, Maio R, Cosentino M, Nespoli L. Cytokines and Obstructive Sleep Apnea in Childhood: Study of a Group of Children. Biologics. 2024; 4(1):44-54. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics4010004
Chicago/Turabian StyleNosetti, Luana Maria, Claudio Tirelli, Franca Marino, Michela Gaiazzi, Lucia Sacchi, Mara De Amici, Fiorella Barocci, Ramona Maio, Marco Cosentino, and Luigi Nespoli. 2024. "Cytokines and Obstructive Sleep Apnea in Childhood: Study of a Group of Children" Biologics 4, no. 1: 44-54. https://0-doi-org.brum.beds.ac.uk/10.3390/biologics4010004