
Impact of Exercise Training on Depressive Symptoms in Cancer Patients: A Critical Analysis

 , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Data Extraction
3. Results
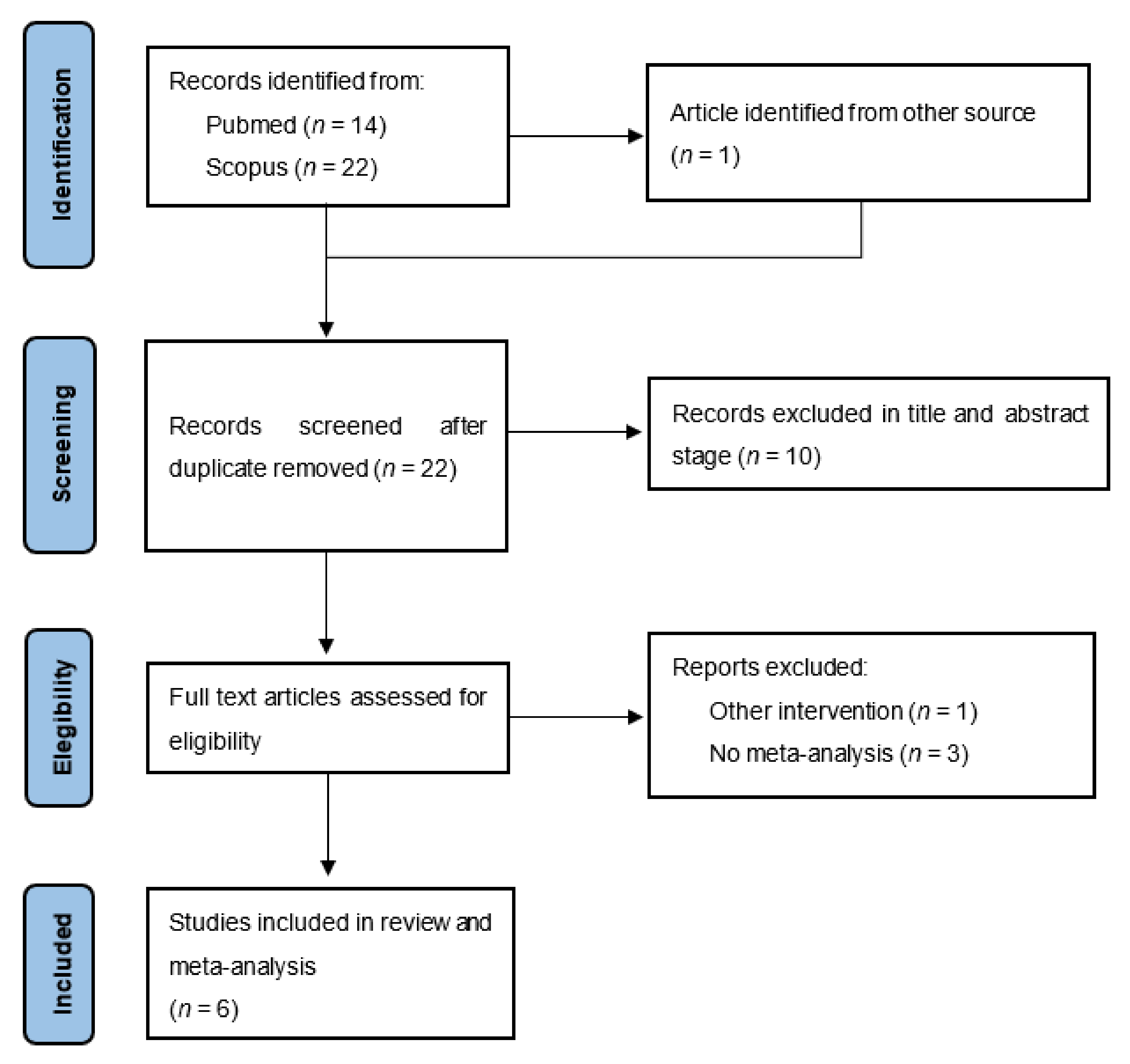
3.1. Literature Search
3.2. Study Characteristics
3.3. Number of RCTs and Participants
3.4. Participants’ Characteristics
3.5. Exercise Intervention Characteristics
3.6. Comparison of Experimental Conditions
3.7. Outcome Measures
3.8. Quality Assessment of Studies
3.9. Quality Assessment
3.10. Synthesis of Results
3.10.1. Main Results
3.10.2. Sensitivity and Subgroup Analyses
4. Discussion
Strengths and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquini, M.; Biondi, M. Depression in cancer patients: A critical review. Clin. Pract. Epidemiol. Ment. Health 2007, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef]
- Naser, A.Y.; Hameed, A.N.; Mustafa, N.; Alwafi, H.; Dahmash, E.Z.; Alyami, H.S. Depression and anxiety in patients with cancer: A cross-sectional study. Front. Psychol. 2021, 12, 585534. [Google Scholar] [CrossRef]
- Caruso, R.; Nanni, M.G.; Riba, M.; Sabato, S.; Mitchell, A.J.; Croce, E.; Grassi, L. Depressive spectrum disorders in cancer: Prevalence, risk factors and screening for depression: A critical review. Acta Oncol. 2017, 56, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Pilevarzadeh, M.; Amirshahi, M.; Afsargharehbagh, R.; Rafiemanesh, H.; Hashemi, S.-M.; Balouchi, A. Global prevalence of depression among breast cancer patients: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2019, 176, 519–533. [Google Scholar] [CrossRef]
- Walker, J.; Holm Hansen, C.; Martin, P.; Sawhney, A.; Thekkumpurath, P.; Beale, C. Prevalence of depression in adults with cancer: A systematic review. Ann. Oncol. 2013, 24, 895–900. [Google Scholar] [CrossRef]
- Ayres, A.; Hoon, P.W.; Franzoni, J.B.; Matheny, K.B.; Cotanch, P.H.; Takayanagi, S. Influence of mood and adjustment to cancer on compliance with chemotherapy among breast cancer patients. J. Psychosom. Res. 1994, 38, 393–402. [Google Scholar] [CrossRef]
- Onitilo, A.A.; Nietert, P.J.; Egede, L.E. Effect of depression on all-cause mortality in adults with cancer and differential effects by cancer site. Gen. Hosp. Psychiatry 2006, 28, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Dwight-Johnson, M.; Ell, K.; Lee, P.J. Can collaborative care address the needs of low-income Latinas with comorbid depression and cancer? Results from a randomised pilot study. Psychosomatics 2005, 46, 224–232. [Google Scholar] [CrossRef]
- Laoutidis, Z.G.; Mathiak, K. Antidepressants in the treatment of depression/depressive symptoms in cancer patients: A systematic review and meta-analysis. BMC Psychiatry 2013, 13, 140. [Google Scholar] [CrossRef] [Green Version]
- Rodin, G.; Katz, M.; Lloyd, N.; Green, E.; Mackay, J.A.; Wong, R.K.S. The treatment of depression in cancer patients: A systematic review. Supportive Care Cancer 2007, 15, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Newton, R.U.; Galvão, D.A. Exercise in prevention and management of cancer. Curr. Treat. Options Oncol. 2008, 9, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Merwin, R.M. The role of exercise in management of mental health disorders: An integrative review. Annu. Rev. Med. 2021, 72, 45–62. [Google Scholar] [CrossRef] [PubMed]
- Yuan, N.; Chen, Y.; Xia, Y.; Dai, J.; Liu, C. Inflammation-related biomarkers in major psychiatric disorders: A cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl. Psychiatry 2019, 9, 233. [Google Scholar] [CrossRef]
- Bower, J.E.; Huedo-Medina, T.B.; Pescatello, L.S.; Ryan, S.M.; Pescatello, S.M.; Moker, E. Fatigue and proinflammatory cytokine activity in breast cancer survivors. Psychosom. Med. 2002, 64, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Motivala, S.J.; Sarfatti, A.; Olmos, L.; Irwin, M.R. Inflammatory markers and sleep disturbance in major depression. Psychosom. Med. 2005, 67, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Fedewa, M.V.; Hathaway, E.D.; Ward-Ritaco, C.; Williams, T.D.; Dobbs, W.C. The effect of chronic exercise training on leptin: A systematic review and meta-analysis of randomized controlled trials. Sports Med. 2018, 48, 1437–1450. [Google Scholar] [CrossRef]
- Moon, H.Y.; Kim, S.H.; Yang, Y.R.; Suh, P.-G. Macrophage migration inhibitory factor mediates the antidepressant actions of voluntary exercise. Proc. Natl. Acad. Sci. USA 2012, 109, 13094–13099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, M.P. The antidepressant effects of physical activity: Mediating self-esteem and self-efficacy mechanisms. Psychol. Health 2008, 23, 279–307. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Huedo-Medina, T.B.; Pescatello, L.S.; Ryan, S.M.; Pescatello, S.M.; Moker, E.; LaCroix, J.M.; Ferrer, R.A.; Johnson, B.T. The efficacy of exercise in reducing depressive symptoms among cancer survivors: A meta-analysis. PLoS ONE 2012, 7, e30955. [Google Scholar] [CrossRef]
- Craft, L.L.; VanIterson, E.H.; Helenowski, I.B.; Rademaker, A.W.; Courneya, K.S. Exercise effects on depressive symptoms in cancer survivors: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2012, 21, 3–19. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.; Pascoe, M.C.; Yang, G.; de Manincor, M.; Grant, S.; Lacey, J.; Firth, J.; Sarris, J. Yoga for depression and anxiety symptoms in people with cancer: A systematic review and meta-analysis. Psychooncology 2021, 30, 1196–1208. [Google Scholar] [CrossRef]
- Patsou, E.D.; Alexias, G.D.; Anagnostopoulos, F.G.; Karamouzis, M.V. Effects of physical activity on depressive symptoms during breast cancer survivorship: A meta-analysis of randomised control trials. ESMO Open 2017, 2, e000271. [Google Scholar] [CrossRef] [Green Version]
- Vashistha, V.; Singh, B.; Kaur, S.; Prokop, L.J.; Kaushik, D. The effects of exercise on fatigue, quality of life, and psychological function for men with prostate cancer: Systematic review and meta-analyses. Eur. Urol. Focus 2016, 2, 284–295. [Google Scholar] [CrossRef]
- Yi, L.J.; Tian, X.; Jin, Y.F.; Luo, M.J.; Jimenez-Herrera, M.F. Effects of yoga on health-related quality, physical health and psychological health in women with breast cancer receiving chemotherapy: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 1961–1975. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Zabora, J.; BrintzenhofeSzoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The prevalence of psychological distress by cancer site. Psychooncology 2001, 10, 19–28. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Vahdaninia, M.; Omidvari, S.; Montazeri, A. What do predict anxiety and depression in breast cancer patients? A follow-up study. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 355–361. [Google Scholar] [CrossRef]
- Ganz, P.A. Psychological and social aspects of breast cancer. Oncology 2008, 22, 642–650, discussion 650. [Google Scholar]
- Baucom, D.H.; Porter, L.S.; Kirby, J.S.; Gremore, T.M.; Keefe, F.J. Psychosocial issues confronting young women with breast cancer. Breast Dis. 2005, 23, 103–113. [Google Scholar] [CrossRef]
- Helms, R.L.; O’Hea, E.L.; Corso, M. Body image issues in women with breast cancer. Psychol. Health Med. 2008, 13, 313–325. [Google Scholar] [CrossRef]
- Snoj, Z.; Akelj, M.P.; Lièina, M.; Pregelj, P. Psychosocial correlates of progesterone receptors in breast cancer. Depress. Anxiety 2009, 26, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Han, J.; Lee, M.Y.; Jang, M.K. The experience of cancer-related fatigue, exercise and exercise adherence among women breast cancer survivors: Insights from focus group interviews. J. Clin. Nurs. 2020, 29, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.P. The effect of a 12-week home-based walking program on reducing fatigue in women with breast cancer undergoing chemotherapy: A randomised controlled study. Int. J. Nurs. Stud. 2019, 99, 103376. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Kok, R.M.; Reynolds, C.F., 3rd. Management of depression in older adults: A review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef]
- Loh, K.P.; Zittel, J.; Kadambi, S.; Pandya, C.; Xu, H.; Flannery, M.; Magnunson, A.; Bautista, J.; McHugh, C.; Mustian, K.; et al. Elucidating the associations between sleep disturbance and depression, fatigue, and pain in older adults with cancer. J. Geriatr. Oncol. 2018, 9, 464–468. [Google Scholar] [CrossRef]
- Loh, K.P.; Kleckner, I.R.; Lin, P.J.; Mohile, S.G.; Canin, B.E.; Flannery, M.A.; Fung, C.; Dunne, R.F.; Bautista, J.; Culakova, E.; et al. Effects of a home-based exercise program on anxiety and mood disturbances in older adults with cancer receiving chemotherapy. J. Am. Geriatr. Soc. 2019, 67, 1005–1011. [Google Scholar] [CrossRef] [Green Version]
- Gultyaeva, V.V.; Zinchenko, M.I.; Uryumtsev, D.Y.; Krivoschekov, S.G.; Aftanas, L.I. Exercise for depression treatment. Physiological mechanisms. Zh. Nevrol. Psikhiatr. SS Korsakova 2019, 119, 112–119. [Google Scholar] [CrossRef]
- Ruddy, K.J.; Stan, D.L.; Bhagra, A.; Jurisson, M.; Cheville, A.L. Alternative exercise traditions in cancer rehabilitation. Phys. Med. Rehabil. 2017, 28, 181–192. [Google Scholar] [CrossRef]
- Scott, J.M.; Zabor, E.C.; Schwitzer, E.; Koelwyn, G.J.; Adams, S.C.; Nilsen, T.S.; Moskowitz, C.S.; Matsoukas, K.; IYengar, N.M.; Dang, C.T.; et al. Efficacy of exercise therapy on cardiorespiratory fitness in patients with cancer: A systematic review and meta-analysis. J. Clin. Oncol. 2018, 36, 2297–2305. [Google Scholar] [CrossRef]
- Gardner, J.R.; Livingston, P.M.; Fraser, S.F. Effects of exercise on treatment-related adverse effects for patients with prostate cancer receiving androgen-deprivation therapy: A systematic review. J. Clin. Oncol. 2014, 32, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.M.; Dobek, J.C.; Bennett, J.A.; Dieckmann, N.F.; Maddalozzo, G.F.; Ryan, C.W.; Beer, T.M. Resistance training reduces disability in prostate cancer survivors on androgen deprivation therapy: Evidence from a randomised controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Courneya, K.S.; Segal, R.J.; Mackey, J.R.; Gelmon, K.; Reid, R.D.; Friedenreich, C.M.; Ladha, A.B.; Proulx, C.; Vallance, J.K.H.; Lane, K.; et al. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomised controlled trial. J. Clin. Oncol. 2007, 25, 4396–4404. [Google Scholar] [CrossRef] [PubMed]
- Kleckner, I.R.; Kamen, C.; Gewandter, J.S.; Mohile, N.A.; Heckler, C.E.; Culakova, E.; Fung, C.; Janlesins, M.C.; Asare, M.; Lin, P.; et al. Effects of exercise during chemotherapy on chemotherapy-induced peripheral neuropathy: A multicenter, randomised controlled trial. Support Care Cancer 2018, 26, 1019–1028. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | No. of RCTs and Participants | Participants Characteristics | Exercise Intervention’s Characteristics | Comparison | Outcomes Measures |
|---|---|---|---|---|---|
| Brown et al. [24] | 37 RCTs; 2929 participants. | Age: mean 51.3 years (range: 39–70); Gender: 87% women; Cancer: breast cancer (24 studies), other types of cancer (13 studies). | Type: walking (16 studies), stationary cycling (5 studies), resistance machines (2 studies), resistance bands (3 studies), yoga (8 studies); Duration/frequency: mean of 13.2 ± 11.7 weeks with 3.0 ± 2.5 sessions/week lasting 49.1 ± 27.1 min/session. | Usual care. | Depressive symptoms (CES-D, POMS, BDI, HADS) and Symptom Assessment Scale. |
| Craft et al. [25] | 15 RCTs; 1371 participants. | Age: mean 51.6 years; Gender: no information about gender; Cancer: breast cancer (60% of the included studies). | Type: aerobic (10 studies), aerobic and resistance (5 studies); Duration/frequency: ranged from 4 to 14 weeks; Supervised, facility-based programs (3 studies), unsupervised home-based programs (6 studies), some exercise programs supervised (4 studies). | Usual care (12 studies); Educational print material (3 studies). | Depression inventory and clinician interview. |
| Gonzalez et al. [26] * | 26 RCTs; 1486 participants. | Age: mean 54.4 years (range 44–68.7 years); Gender: 86.1% women; Cancer: breast cancer (18 studies), mixed cancers (2 studies), other types of cancers (6 studies). | Type: hatha yoga (11 studies), other types of yoga (15 studies); Duration/frequency: mean of 9.3, with 1 to 3 sessions/week lasting 45–120 min/session. | Usual care (19 studies); Psychosocial or educational interventions (6 studies); Other physical activity interventions (2 studies). | Depressive symptoms (HADS, BDI-II, CES-D, POMS, PHQ-2, PHQ-9). |
| Patsou et al. [27] | 14 RCTs; 1701 participants. | Age: mean 52 years; Gender: only women; Cancer: only breast cancer. | Type: aerobic, resistance, aerobic and resistance, yoga; Duration/frequency: no information; | Usual care; Health education intervention; Waitlist; Relaxation and stretching. | Depressive symptoms (POMS, HADS, CES-D). |
| Vashistha et al. [28] ** | 3 RCTs; 192 participants. | Age: mean between 67 and 73 years; Gender: only men; Cancer: only prostate cancer. | Type: qigong (1 study), aerobic and resistance (1 study), aerobic and light resistance (1 study); Duration/frequency: no information; | Usual care; Stretching. | Depressive symptoms (BSI-18, CES-D). |
| Yi et al. [29] *** | 6 RCTs; 446 participants. | Age: mean between 45 and 60 years; Gender: only women; Cancer: only breast cancer. | Type: only yoga; Duration/frequency: no information; | Usual care. | Depressive symptoms (BDI-II, POMS, HADS, CES-D, SDS). |
| AMSTAR 2 Criteria | Brown et al. [24] | Craft et al. [25] | Gonzalez et al. [26] | Patsou et al. [27] | Vashistha et al. [28] | Yi et al. [29] |
|---|---|---|---|---|---|---|
| 1. Did the research questions and inclusion criteria include the components of PICO? | V | V | V | V | V | V |
| 2. Did the review report contain a statement that the review methods were established before the conduct of the review, and did the report justify significant deviations from the protocol? | X | X | V | X | V | X |
| 3. Did the review authors explain their selection of the study designs for inclusion in the review? | V | V | V | V | V | V |
| 4. Did the review authors use a comprehensive literature search strategy? | V | V | V | V | V | V |
| 5. Did the review authors perform study selection in duplicate? | X | V | V | X | V | V |
| 6. Did the review authors perform data extraction in duplicate? | V | V | V | X | V | V |
| 7. Did the review authors provide a list of excluded studies and justify the exclusions? | V | V | V | V | V | V |
| 8. Did the review authors describe the included studies in adequate detail? | V | V | V | V | V | V |
| 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies included in the review? | V | V | V | V | V | V |
| 10. Did the review authors report funding sources for the studies included? | X | X | X | X | X | X |
| 11. If meta-analysis was performed, did the review authors use appropriate methods for the statistical combination of results? | V | V | V | V | V | V |
| 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | V | X | V | V | V | V |
| 13. Did the review authors account for RoB in individual studies when interpreting/discussing the review results? | V | V | V | V | X | V |
| 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the review results? | V | V | V | V | V | V |
| 15. If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the review results? | V | V | V | V | V | X |
| 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | V | V | V | V | V | V |
| Moderate | Moderate | Moderate | Moderate | Low | Moderate |
| Reference | Effect on Depressive Symptoms (95% CI) | I2 (%) | Conclusions |
|---|---|---|---|
| Brown et al. [24] | d = −0.13 (−0.26, −0.01) | 55% | Significant small reduction in depressive symptoms compared to usual care among all types of cancer. |
| Craft et al. [25] | d = −0.22 (−0.43, −0.009) | The test for heterogeneity was significant (p < 0.001). | Significant small reduction in depressive symptoms when comparing exercise interventions to control groups. |
| Gonzalez et al. [26] | g = −0.55 (−0.78, −0.32) | 77% | Significant medium effect size in favour of yoga interventions for reducing depression symptoms in comparison to control conditions. |
| Patsou et al. [27] | g = −0.38 (−0.89, 0.13) | 77% | Non-significant reduction in depressive symptoms for the exercise group. |
| Vashistha et al. [28] | SMD = −3.02 (−7.83, 1.79) | 78% | Non-significant reduction in depressive symptoms for the exercise group. |
| Yi et al. [29] | SMD = −0.56 (−1.05, −0.07) | 84% | Significant improvement in depressive symptoms for yoga interventions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marconcin, P.; Marques, A.; Ferrari, G.; Gouveia, É.R.; Peralta, M.; Ihle, A. Impact of Exercise Training on Depressive Symptoms in Cancer Patients: A Critical Analysis. Biology 2022, 11, 614. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040614
Marconcin P, Marques A, Ferrari G, Gouveia ÉR, Peralta M, Ihle A. Impact of Exercise Training on Depressive Symptoms in Cancer Patients: A Critical Analysis. Biology. 2022; 11(4):614. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040614
Chicago/Turabian StyleMarconcin, Priscila, Adilson Marques, Gerson Ferrari, Élvio R. Gouveia, Miguel Peralta, and Andreas Ihle. 2022. "Impact of Exercise Training on Depressive Symptoms in Cancer Patients: A Critical Analysis" Biology 11, no. 4: 614. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11040614